
Recovery of Innate Immune Cells and Persisting Alterations in Adaptive Immunity in the Peripheral Blood of Convalescent Plasma Donors at Eight Months Post SARS-CoV-2 Infection

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Participants
2.2. Flow Cytometry Analysis
2.3. Statistical Analysis
3. Results
3.1. Characteristics of CP Donors
3.2. The Immune Profiling at Eight Months Post SARS-CoV-2 Infection Does Not Correlate With the Clinical Characteristics of CP Donors
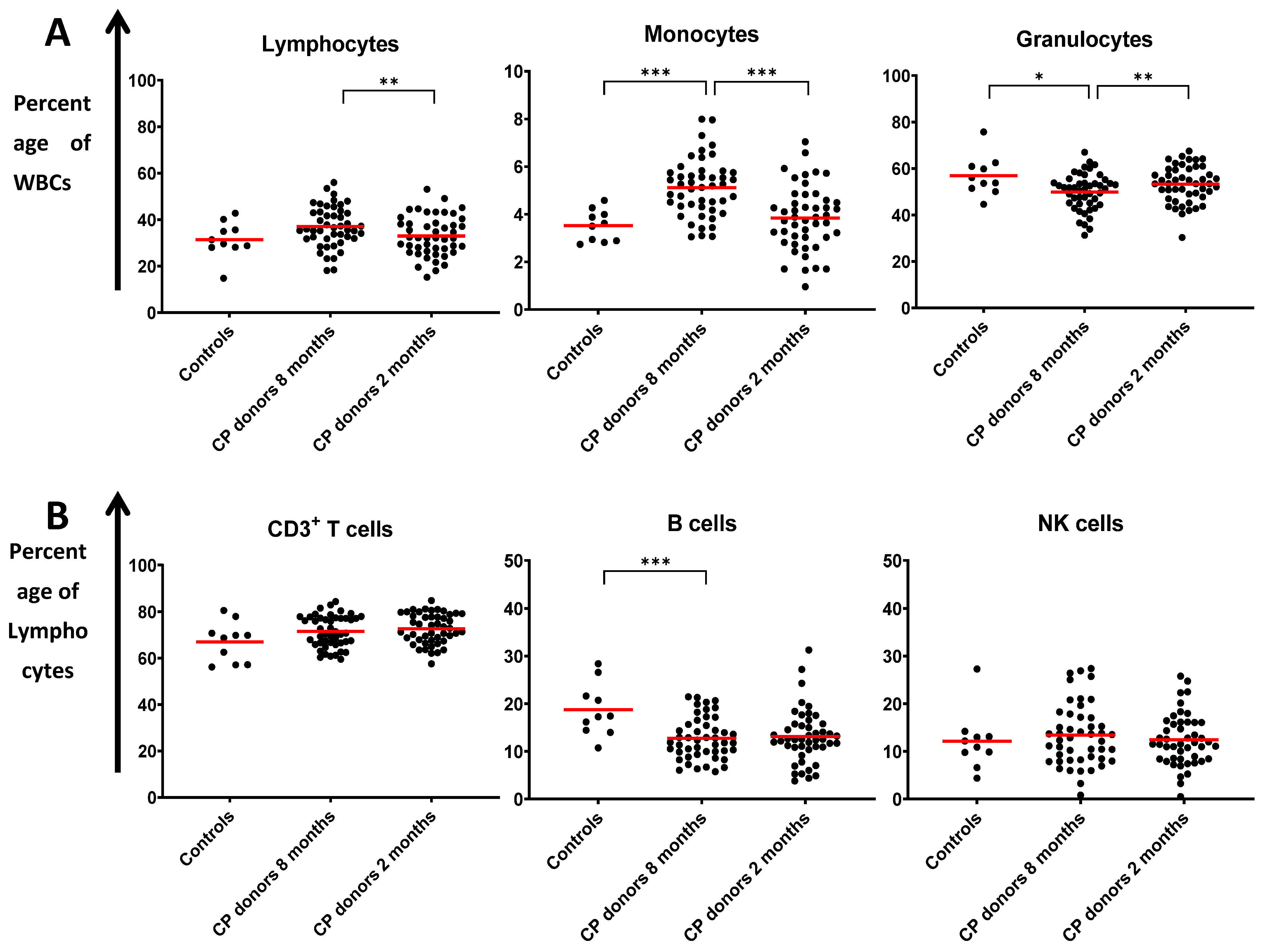
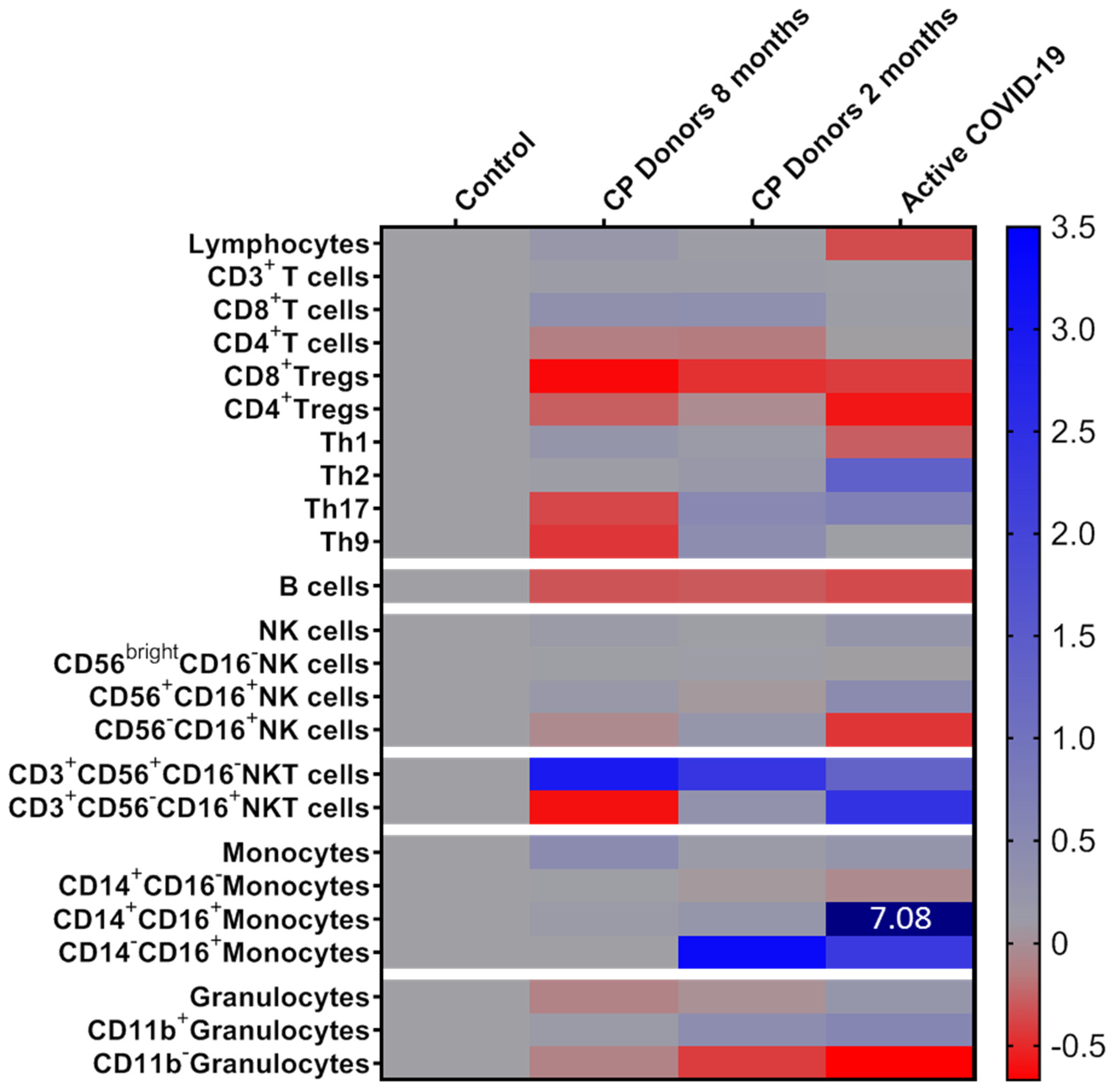
3.3. Innate Immunity Recovery at Eight Months Post COVID-19
3.4. Alterations in Adaptive Immunity Persist at Eight Months Post Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsitsilonis, O.E.; Paraskevis, D.; Lianidou, E.; Pierros, V.; Akalestos, A.; Kastritis, E.; Moutsatsou, P.; Scorilas, A.; Sphicopoulos, T.; Terpos, E.; et al. Seroprevalence of Antibodies against SARS-CoV-2 among the Personnel and Students of the National and Kapodistrian University of Athens, Greece: A Preliminary Report. Life 2020, 10, 214. [Google Scholar] [CrossRef]
- Gavriatopoulou, M.; Korompoki, E.; Fotiou, D.; Ntanasis-Stathopoulos, I.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Organ-specific manifestations of COVID-19 infection. Clin. Exp. Med. 2020, 20, 493–506. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, Y.; Shao, C.; Huang, J.; Gan, J.; Huang, X.; Bucci, E.; Piacentini, M.; Ippolito, G.; Melino, G. COVID-19 infection: The perspectives on immune responses. Cell Death Differ. 2020, 27, 1451–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, X. COVID-19: Immunopathology and its implications for therapy. Nat. Rev. Immunol. 2020, 20, 269–270. [Google Scholar] [CrossRef] [Green Version]
- Jamilloux, Y.; Henry, T.; Belot, A.; Viel, S.; Fauter, M.; El Jammal, T.; Walzer, T.; Francois, B.; Seve, P. Should we stimulate or suppress immune responses in COVID-19? Cytokine and anti-cytokine interventions. Autoimmun. Rev. 2020, 19, 102567. [Google Scholar] [CrossRef] [PubMed]
- Hagg, S.; Jylhava, J.; Wang, Y.; Xu, H.; Metzner, C.; Annetorp, M.; Garcia-Ptacek, S.; Khedri, M.; Bostrom, A.M.; Kadir, A.; et al. Age, Frailty, and Comorbidity as Prognostic Factors for Short-Term Outcomes in Patients With Coronavirus Disease 2019 in Geriatric Care. J. Am. Med. Dir. Assoc. 2020, 21, 1555–1559.e2. [Google Scholar] [CrossRef] [PubMed]
- Wendel Garcia, P.D.; Fumeaux, T.; Guerci, P.; Heuberger, D.M.; Montomoli, J.; Roche-Campo, F.; Schuepbach, R.A.; Hilty, M.P.; Investigators, R.-I. Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: Initial report of the international RISC-19-ICU prospective observational cohort. EClinicalMedicine 2020, 25, 100449. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Ren, L.; Zhang, L.; Zhong, J.; Xiao, Y.; Jia, Z.; Guo, L.; Yang, J.; Wang, C.; Jiang, S.; et al. Heightened Innate Immune Responses in the Respiratory Tract of COVID-19 Patients. Cell Host Microbe 2020, 27, 883–890.e2. [Google Scholar] [CrossRef]
- Sette, A.; Crotty, S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]
- Breton, G.; Mendoza, P.; Hagglof, T.; Oliveira, T.Y.; Schaefer-Babajew, D.; Gaebler, C.; Turroja, M.; Hurley, A.; Caskey, M.; Nussenzweig, M.C. Persistent cellular immunity to SARS-CoV-2 infection. J. Exp. Med. 2021, 218, e20202515. [Google Scholar] [CrossRef]
- Neeland, M.R.; Bannister, S.; Clifford, V.; Dohle, K.; Mulholland, K.; Sutton, P.; Curtis, N.; Steer, A.C.; Burgner, D.P.; Crawford, N.W.; et al. Innate cell profiles during the acute and convalescent phase of SARS-CoV-2 infection in children. Nat. Commun. 2021, 12, 1084. [Google Scholar] [CrossRef]
- Orologas-Stavrou, N.; Politou, M.; Rousakis, P.; Kostopoulos, I.V.; Ntanasis-Stathopoulos, I.; Jahaj, E.; Tsiligkeridou, E.; Gavriatopoulou, M.; Kastritis, E.; Kotanidou, A.; et al. Peripheral Blood Immune Profiling of Convalescent Plasma Donors Reveals Alterations in Specific Immune Subpopulations Even at 2 Months Post SARS-CoV-2 Infection. Viruses 2020, 13, 26. [Google Scholar] [CrossRef]
- Terpos, E.; Politou, M.; Sergentanis, T.N.; Mentis, A.; Rosati, M.; Stellas, D.; Bear, J.; Hu, X.; Felber, B.K.; Pappa, V.; et al. Anti-SARS-CoV-2 Antibody Responses in Convalescent Plasma Donors Are Increased in Hospitalized Patients; Subanalyses of a Phase 2 Clinical Study. Microorganisms 2020, 8, 1885. [Google Scholar] [CrossRef]
- Rezaei, M.; Marjani, M.; Mahmoudi, S.; Mortaz, E.; Mansouri, D. Dynamic Changes of Lymphocyte Subsets in the Course of COVID-19. Int. Arch. Allergy Immunol. 2021, 182, 254–262. [Google Scholar] [CrossRef]
- Zhang, D.; Guo, R.; Lei, L.; Liu, H.; Wang, Y.; Wang, Y.; Qian, H.; Dai, T.; Zhang, T.; Lai, Y.; et al. COVID-19 infection induces readily detectable morphologic and inflammation-related phenotypic changes in peripheral blood monocytes. J. Leukoc. Biol. 2021, 109, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Laing, A.G.; Lorenc, A.; Del Molino Del Barrio, I.; Das, A.; Fish, M.; Monin, L.; Muñoz-Ruiz, M.; McKenzie, D.R.; Hayday, T.S.; Francos-Quijorna, I.; et al. A consensus Covid-19 immune signature combines immuno-protection with discrete sepsis-like traits associated with poor prognosis. medRxiv 2020. [Google Scholar] [CrossRef]
- Kwissa, M.; Nakaya, H.I.; Onlamoon, N.; Wrammert, J.; Villinger, F.; Perng, G.C.; Yoksan, S.; Pattanapanyasat, K.; Chokephaibulkit, K.; Ahmed, R.; et al. Dengue virus infection induces expansion of a CD14(+)CD16(+) monocyte population that stimulates plasmablast differentiation. Cell Host Microbe 2014, 16, 115–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merad, M.; Martin, J.C. Pathological inflammation in patients with COVID-19: A key role for monocytes and macrophages. Nat. Rev. Immunol. 2020, 20, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Sampath, P.; Moideen, K.; Ranganathan, U.D.; Bethunaickan, R. Monocyte Subsets: Phenotypes and Function in Tuberculosis Infection. Front. Immunol. 2018, 9, 1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Fu, B.; Zheng, X.; Wang, D.; Zhao, C.; Qi, Y.; Sun, R.; Tian, Z.; Xu, X.; Wei, H. Pathogenic T-cells and inflammatory monocytes incite inflammatory storms in severe COVID-19 patients. Natl. Sci. Rev. 2020, 7, 998–1002. [Google Scholar] [CrossRef] [Green Version]
- Narasimhan, P.B.; Marcovecchio, P.; Hamers, A.A.J.; Hedrick, C.C. Nonclassical Monocytes in Health and Disease. Annu. Rev. Immunol. 2019, 37, 439–456. [Google Scholar] [CrossRef]
- Olingy, C.E.; San Emeterio, C.L.; Ogle, M.E.; Krieger, J.R.; Bruce, A.C.; Pfau, D.D.; Jordan, B.T.; Peirce, S.M.; Botchwey, E.A. Non-classical monocytes are biased progenitors of wound healing macrophages during soft tissue injury. Sci. Rep. 2017, 7, 447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, M.; Steinfort, D.P.; Smallwood, D.; Hew, M.; Chen, W.; Ernst, M.; Irving, L.B.; Anderson, G.P.; Hibbs, M.L. CD11b immunophenotyping identifies inflammatory profiles in the mouse and human lungs. Mucosal. Immunol. 2016, 9, 550–563. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R.; Gant, V.A.; Williams, B.; Enver, T. Increased Complement Receptor-3 levels in monocytes and granulocytes distinguish COVID-19 patients with pneumonia from those with mild symptoms. Int. J. Infect. Dis. 2020, 99, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Mentis, A.; Dimopoulos, M.A. Loss of Anti-SARS-CoV-2 Antibodies in Mild Covid-19. N. Engl. J. Med. 2020, 383, 1695. [Google Scholar] [CrossRef]
- Afrin, L.B.; Weinstock, L.B.; Molderings, G.J. Covid-19 hyperinflammation and post-Covid-19 illness may be rooted in mast cell activation syndrome. Int. J. Infect. Dis. 2020, 100, 327–332. [Google Scholar] [CrossRef]
- Della Chiesa, M.; Pesce, S.; Muccio, L.; Carlomagno, S.; Sivori, S.; Moretta, A.; Marcenaro, E. Features of Memory-Like and PD-1(+) Human NK Cell Subsets. Front. Immunol. 2016, 7, 351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Bruin, A.M.; Voermans, C.; Nolte, M.A. Impact of interferon-gamma on hematopoiesis. Blood 2014, 124, 2479–2486. [Google Scholar] [CrossRef] [Green Version]
- Peng, Y.; Mentzer, A.J.; Liu, G.; Yao, X.; Yin, Z.; Dong, D.; Dejnirattisai, W.; Rostron, T.; Supasa, P.; Liu, C.; et al. Broad and strong memory CD4(+) and CD8(+) T cells induced by SARS-CoV-2 in UK convalescent individuals following COVID-19. Nat. Immunol. 2020, 21, 1336–1345. [Google Scholar] [CrossRef]
- Schulien, I.; Kemming, J.; Oberhardt, V.; Wild, K.; Seidel, L.M.; Killmer, S.; Daul, F.; Lago, M.S.; Decker, A.; Luxenburger, H.; et al. Characterization of pre-existing and induced SARS-CoV-2-specific CD8(+) T cells. Nat. Med. 2021, 27, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Fujii, S.I.; Yamasaki, S.; Sato, Y.; Shimizu, K. Vaccine Designs Utilizing Invariant NKT-Licensed Antigen-Presenting Cells Provide NKT or T Cell Help for B Cell Responses. Front. Immunol. 2018, 9, 1267. [Google Scholar] [CrossRef]
- Tyznik, A.J.; Verma, S.; Wang, Q.; Kronenberg, M.; Benedict, C.A. Distinct requirements for activation of NKT and NK cells during viral infection. J. Immunol. 2014, 192, 3676–3685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.Y.; Wang, X.M.; Xing, X.; Xu, Z.; Zhang, C.; Song, J.W.; Fan, X.; Xia, P.; Fu, J.L.; Wang, S.Y.; et al. Single-cell landscape of immunological responses in patients with COVID-19. Nat. Immunol. 2020, 21, 1107–1118. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Characteristics | CP Donors (n = 47) |
|---|---|
| Male gender (N/percentage) | 27 (57.4%) |
| Age in years, median (range) | 49 (37–72) |
| Symptoms (N/percentage) | |
| Fever | 12 (25.5%) |
| Fatigue | 15 (31.9%) |
| Headache | 27 (57.4%) |
| Cough | 26 (55.3%) |
| Breathlessness | 35 (74.5%) |
| Diarrhea | 34 (72.3%) |
| Anosmia | 22 (46.8%) |
| Ageusia | 25 (53.2%) |
| Anti-S1 IgG, median OD (IQR) | 5.14 (6.23) |
| Immune Subset | Controls N = 10 | CP Donors Eight Months N = 47 | CP Donors Two Months N = 47 | p Value ** | p Value *** |
|---|---|---|---|---|---|
| Lymphocytes (% of WBCs) | 31.41 ± 7.78 * | 36.95 ± 8.74 | 32.96 ± 8.57 | ns | 0.002 |
| CD3+ T Cells (% of Lymphocytes) | 67.07 ± 8.61 | 71.51 ± 6.80 | 72.70 ± 6.50 | ns | ns |
| CD8+ T Cells (% of CD3+ T Cells) | 24.38 ± 8.51 | 32.65 ± 9.37 | 33.38 ± 10.38 | 0.013 | ns |
| CD4+ T Cells (% of CD3+ T Cells) | 71.36 ± 11.28 | 61.40 ± 10.12 | 60.43 ± 10.82 | 0.008 | ns |
| CD8+ Tregs (% of CD8+ T Cells) | 7.29 ± 8.24 | 2.67 ± 3.74 | 3.86 ± 4.95 | 0.011 | ns |
| CD4+ Tregs (% of CD4+ T Cells) | 2.04 ± 0.90 | 1.48 ± 0.90 | 1.87 ± 1.28 | ns | <0.001 |
| Th1 (% of CD4+ T Cells) | 26.77 ± 7.96 | 32.71 ± 10.35 | 29.25 ± 10.32 | ns | 0.022 |
| Th2 (% of CD4+ T Cells) | 7.67 ± 3.60 | 8.13 ± 9.11 | 8.86 ± 14.71 | ns | ns |
| Th17 (% of CD4+ T Cells) | 1.73 ± 0.96 | 1.09 ± 1.79 | 2.61 ± 6.63 | ns | ns |
| Th9 (% of CD4+ T Cells) | 11.57 ± 4.10 | 6.45 ± 6.01 | 16.15 ± 16.74 | 0.013 | <0.001 |
| B Cells (% of Lymphocytes) | 18.74 ± 5.60 | 12.74 ± 4.39 | 13.13 ± 5.59 | <0.001 | ns |
| NK Cells (% of Lymphocytes) | 12.14 ± 6.13 | 13.41 ± 6.43 | 12.43 ± 5.42 | ns | ns |
| Immature NK Cells (% of NK Cells) | 0.69 ± 0.32 | 0.71 ± 0.63 | 0.72 ± 0.63 | ns | ns |
| Mature NK Cells (% of NK Cells) | 8.84 ± 5.05 | 10.33 ± 5.53 | 8.55 ± 4.84 | ns | 0.001 |
| Memory-like NK Cells (% of NK Cells) | 2.61 ± 1.20 | 2.37 ± 1.48 | 3.16 ± 1.81 | ns | 0.007 |
| CD3+CD56−CD16+ NKT Cells (% of CD3+ Cells) | 0.19 ± 0.13 | 0.07 ± 0.15 | 0.25 ± 0.47 | 0.029 | 0.014 |
| CD3+CD56+CD16− NKT Cells (% of CD3+ Cells) | 1.80 ± 2.05 | 7.07 ± 6.13 | 6.00 ± 5.29 | 0.010 | 0.002 |
| Monocytes (% of WBCs) | 3.52 ± 0.66 | 5.11 ± 1.20 | 3.84 ± 1.34 | <0.001 | <0.001 |
| Classical Monocytes (% of Monocytes) | 95.04 ± 3.14 | 97.57 ± 2.13 | 91.95 ± 12.22 | 0.003 | <0.001 |
| Intermediate Monocytes (% of Monocytes) | 0.81 ± 0.64 | 0.89 ± 1.14 | 0.99 ± 1.21 | ns | ns |
| Non-classical Monocytes (% of Monocytes) | 0.27 ± 0.24 | 0.27 ± 0.54 | 1.16 ± 2.45 | ns | 0.012 |
| Granulocytes (% of WBCs) | 56.84 ± 8.56 | 49.86 ± 7.80 | 53.20 ± 7.88 | 0.014 | 0.002 |
| CD11b+ Granulocytes (% of Granulocytes) | 46.12 ± 34.14 | 50.94 ± 23.16 | 64.52 ± 25.10 | ns | 0.001 |
| CD11b− Granulocytes (% of Granulocytes) | 47.29 ± 27.52 | 41.43 ± 18.13 | 27.38 ± 18.47 | ns | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostopoulos, I.V.; Orologas-Stavrou, N.; Rousakis, P.; Panteli, C.; Ntanasis-Stathopoulos, I.; Charitaki, I.; Korompoki, E.; Gavriatopoulou, M.; Kastritis, E.; Trougakos, I.P.; et al. Recovery of Innate Immune Cells and Persisting Alterations in Adaptive Immunity in the Peripheral Blood of Convalescent Plasma Donors at Eight Months Post SARS-CoV-2 Infection. Microorganisms 2021, 9, 546. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9030546
Kostopoulos IV, Orologas-Stavrou N, Rousakis P, Panteli C, Ntanasis-Stathopoulos I, Charitaki I, Korompoki E, Gavriatopoulou M, Kastritis E, Trougakos IP, et al. Recovery of Innate Immune Cells and Persisting Alterations in Adaptive Immunity in the Peripheral Blood of Convalescent Plasma Donors at Eight Months Post SARS-CoV-2 Infection. Microorganisms. 2021; 9(3):546. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9030546
Chicago/Turabian StyleKostopoulos, Ioannis V., Nikolaos Orologas-Stavrou, Pantelis Rousakis, Chrysanthi Panteli, Ioannis Ntanasis-Stathopoulos, Ioanna Charitaki, Eleni Korompoki, Maria Gavriatopoulou, Efstathios Kastritis, Ioannis P. Trougakos, and et al. 2021. "Recovery of Innate Immune Cells and Persisting Alterations in Adaptive Immunity in the Peripheral Blood of Convalescent Plasma Donors at Eight Months Post SARS-CoV-2 Infection" Microorganisms 9, no. 3: 546. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9030546