
Update on Coagulase-Negative Staphylococci—What the Clinician Should Know


Institute of Medical Microbiology and Hygiene, Saarland University, 66424 Homburg, Germany
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Microorganisms 2021, 9(4), 830; https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9040830
Submission received: 8 March 2021
/
Revised: 3 April 2021
/
Accepted: 6 April 2021
/
Published: 14 April 2021
(This article belongs to the Special Issue Human Skin Microbiota)
Abstract
:Coagulase-negative staphylococci (CoNS) are among the most frequently recovered bacteria in routine clinical care. Their incidence has steadily increased over the past decades in parallel to the advancement in medicine, especially in regard to the utilization of foreign body devices. Many new species have been described within the past years, while clinical information to most of those species is still sparse. In addition, interspecies differences that render some species more virulent than others have to be taken into account. The distinct populations in which CoNS infections play a prominent role are preterm neonates, patients with implanted medical devices, immunodeficient patients, and those with other relevant comorbidities. Due to the property of CoNS to colonize the human skin, contamination of blood cultures or other samples occurs frequently. Hence, the main diagnostic hurdle is to correctly identify the cases in which CoNS are causative agents rather than contaminants. However, neither phenotypic nor genetic tools have been able to provide a satisfying solution to this problem. Another dilemma of CoNS in clinical practice pertains to their extensive antimicrobial resistance profile, especially in healthcare settings. Therefore, true infections caused by CoNS most often necessitate the use of second-line antimicrobial drugs.
1. Introduction
Coagulase-negative staphylococci (CoNS) form a large group of Gram-positive cocci united by their mutual lack of the virulence factor coagulase [1]. Many species belong to this group, the latest one, Staphylococcus borealis, being described as recent as 2020 [2]. In daily clinical practice, CoNS are commonly regarded as less pathogenic than Staphylococcus (S.) aureus and other members of the S. aureus complex [3,4,5], which in contrast possess coagulase. There is a huge discrepancy in published literature, with publications pertinent to S. aureus outnumbering literature on CoNS by far. This discrepancy is indicative of the relative lack of CoNS’ scientific appraisal during the past years and decades. Many CoNS infections are associated with foreign bodies (e.g., catheters) that facilitate biofilm formation, which contributes to CoNS pathogenicity. Importantly, the virulence factors of CoNS vary considerably, with some species (e.g., S. lugdunensis) being capable of significant adverse impacts on patients [6,7,8]. A probable explanation to why CoNS-related infections are overlooked so often is the fact that they are frequent commensal members of the skin microbiota [9]. As a consequence, they are often classified as contaminants rather than the causative agent of infection. The distinction between infection and contamination is not always straightforward, and most attempts thus far to identify one or more distinctive marker(s) have been unsuccessful. In this review, we will focus on the increasing clinical impact of CoNS-associated infections, the challenges in diagnostics, and the current therapeutic options.
2. Increasing Clinical Impact of CoNS
CoNS have been increasingly recovered in clinically relevant samples, e.g., blood cultures or otherwise primarily sterile samples, in parallel to the advancement in all medical specialties [10]. These medical advancements include not only sophisticated immunosuppressive or -modulatory treatment regimens in oncology, but also the increased use of implantable foreign bodies, such as central venous access devices, total joint replacements, and vascular grafts.
Newborns and preterm neonates are a particularly vulnerable patient group, in whom infections caused by microorganisms with low pathogenicity can occur at a higher rate than in otherwise healthy children or adults [11,12,13]. Neonatal sepsis contributes heavily to the high morbidity and mortality, and CoNS have been reported to be one of the main causes of neonatal sepsis in neonatal intensive care units (NICU) [14]. However, bloodstream infections (BSI) caused by CoNS are one of the most prevalent nosocomial infections among all age groups. CoNS represented 31% among all cases of nosocomial BSI within a period of 7 years in a total of 49 US hospitals [15]. This finding was confirmed in several other cohorts of different geographical backgrounds over the past years [16]. For example, an observational study from Germany, which examined the prevalence of nosocomial infections in a University hospital, identified CoNS as the second most common cause of nosocomial infections [17]. More recent studies revealed the relationship between CoNS and the increased use of implanted medical devices like cardiac valves or joint replacements [18].
Several CoNS form a biofilm that enables the bacteria to adhere to medical devices and, as a result, to protect them against antibiotics [19]. Furthermore, especially elderly people with significant comorbidities, premature neonates or immunocompromised patients are at high risk for CoNS-associated BSIs, skin and soft tissue infections, and both native and prosthetic valve endocarditis. Additionally, CoNS-associated infections can occur in young and healthy individuals as well. S. saprophyticus, for example, is a cause for urinary tract infections, especially in young women.
Moreover, CoNS are being increasingly studied within veterinary medicine, while their role as disease-causing pathogens in animals is still regarded as small. Although the relevance for human disease is not fully established, it has been shown that CoNS-inhabiting animals can display a wide range of antimicrobial resistances, and thus may potentially serve as a reservoir of resistance genes [20].
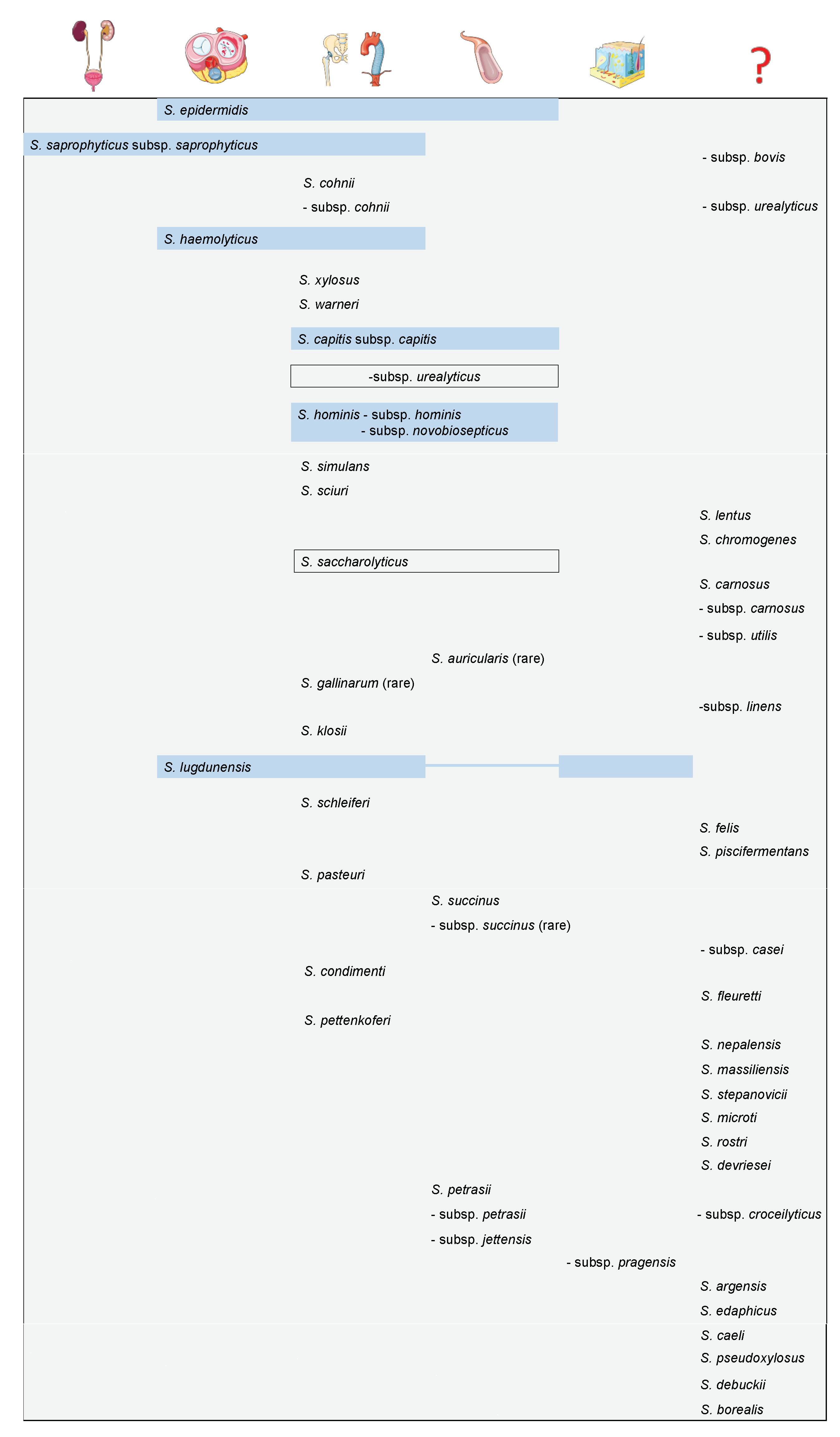
Currently, more than 50 different CoNS species have been described. Figure 1 displays an overview of CoNS known thus far, their attributable clinical relevance, frequency, and the associated infectious syndrome. In total, six species are believed to be associated with a higher clinical significance, namely S. epidermidis, S. saprophyticus, S. haemolyticus, S. capitis, S. hominis, and S. lugdunensis. Some species, including S. lugdunensis, are known to cause severe clinical disease. Antibiotic resistance has become an increasing problem with S. lugdunensis, which has some mutual features with S. aureus and has been reported as a cause of infective endocarditis [6,8].
Besides sporadic case reports, only limited clinical data is available about the most recently discovered CoNS species. Six species were discovered between 2015–2020, one of which is S. argensis [22]. Up until now, this strain has only been isolated from an aquatic environment, precisely from the river, Argen, in Southern Germany. S. edaphicus was also isolated from a natural environment. Scientists first isolated S. edaphicus from stone fragments and sandy soil in James Ross Island, Antarctica [23]. It is notable that S. edaphicus possesses mobile genetic elements that carry antimicrobial resistance genes, thereby rendering it a resistance reservoir that potentially spreads resistance-associated genes. Three further species were described for the first time in 2019, i.e., S. caeli, S. pseudoxylosus, and S. debuckii [24,25,26]. All three were isolated from various animal environments (S. caeli from air sampling in a rabbit holding, S. pseudoxylosus from bovine mastitis and S. debuckii from bovine milk), and their clinical relevance for humans remains to be established. The most recently discovered species, S. borealis, was obtained from four isolates of the human skin, as well as from one blood culture, indicating this species’ ability to colonize human skin and potentially penetrate into the blood stream [2]. Due to lack of data, it has not been possible yet to link the newer CoNS species to specific infectious syndromes or define their impacts on humans. However, one existing problem is that even species that have been known for a longer time can be difficult to assign to a specific infectious syndrome. In order to give an exemplary overview into a selection of CoNS and the wide range of associated infections, three species and their characteristics of clinical cases reported thus far are listed in Table 1. For S. saccharolyticus—of note, the only anaerobic CoNS—more than a dozen clinical cases have been reported. Several of these cases were foreign body-related infections, but also cases without any indwelling medical devices have been documented [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. Only single case reports for the more recently described species S. massiliensis, S. petrasii subsp. petrasii, and S. petrasii subsp. croceilyticus are existing [43,44]. However, this does not necessarily translate into a reduced clinical significance. It was pointed out by the authors of the case report that a variety of CoNS species were found in the clinical samples, which made it impossible to undoubtedly identify the species that caused the infection and thus determine the clinical significance of a species. This has been a recurring problem in the diagnosis of CoNS.
3. The Diagnostic Complexities—How to Distinguish between Infection and Contamination
The main challenge in diagnosis is the correct adjudication of whether or not the detected organism, i.e., a CoNS member, is the causative pathogen of the patient’s infection. It can be assumed that the complexity of a diagnosis leads to potentially disregarded CoNS infections, consequently leading to undertreatment (i.e., delayed or withheld antibiotics) in some cases and thereby contributing to morbidity and mortality [45]. On the other hand, antibiotic overtreatment is associated with the development of antimicrobial resistance, severe adverse events, and higher costs, mainly due to the need for in-patient therapy [46]. Ultimately, an unnecessarily prolonged hospitalization does not only cause a loss in quality-adjusted life-years, but hospital bed occupancy exposes another factor of this complexity, which becomes particularly immanent during times of hospital capacity shortage, especially during pandemics, such as COVID-19 [47].
Another diagnostic challenge is the correct identification on a species level. In some laboratories, matrix-assisted laser desorption/ionization time of flight mass spectrometry (MALDI-TOF MS) may not be as readily available as in others, even though this method has been considered the gold standard since its introduction into microbiological diagnostics more than a decade ago [48,49,50]. As described above, significant interspecies differences in clinical relevance, pathogenicity, and even antimicrobial susceptibility exist [50,51]. Therefore, identification to the species level can be regarded as fundamental. Yet, taxonomic categorizations are ongoing. Some previously described species have been partially re-classified, and some newly described CoNS may not yet be deposited in the relevant MALDI-TOF MS databases [52]. An additional problem that can complicate the microbiological identification is the fastidious and slow growth of some species, for example of S. saccharolyticus [38].
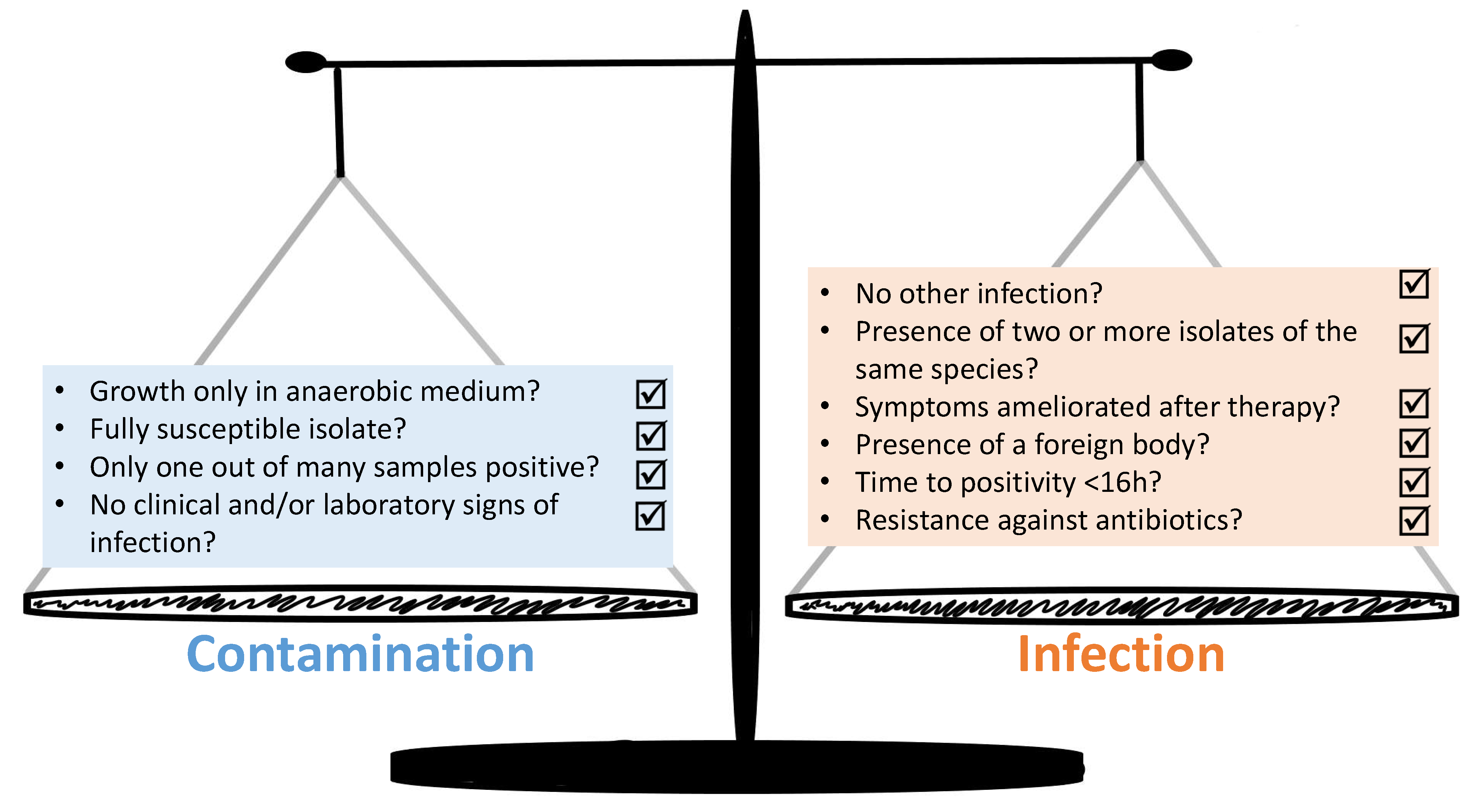
The group of CoNS is a heterogenous group constituted by a variety of different species, each with a unique set of traits. These microbiological properties have previously been described in detail [53]. Nevertheless, many studies have the tendency to compile all CoNS into one group. Not only do the phenotypic traits differ, but the niches which they tend to colonize vary widely. For example, S. capitis is found preferably on the scalp, while S. cohnii is isolated from feet, and S. saccharolyticus from back skin [40,54]. Considering the CoNS trait to colonize the human skin as commensals, it is not surprising that they can result in contaminated samples. Currently it remains a challenge to find valid and universally applicable tools that make it possible to decide whether the clinical case is an infection caused by CoNS or if the detection of a CoNS species indicates just a contamination with the same respective microorganism. Figure 2 summarizes a proposed set of criteria for the distinction between contamination and infection derived from the literature.
Beekmann and colleagues proposed that in order to prevent misclassification of CoNS as a cause of infection, at least two independent blood cultures must be positive for CoNS within 5 days. Alternatively, one positive blood culture suffices if the clinical symptoms are suggestive of an infection [55]. Other research groups have similarly reasoned that one single positive blood culture may be clinically significant, especially in the context of clinical syndromes with high mortality, e.g., sepsis [56]. García-Vázquez proposed an algorithm including a Charlson score ≥ 3, Pitt score ≥ 1, neutropenia, the presence of central venous catheter, identification of S. epidermidis, and time to positivity < 16 h, which yielded a positive predictive value of 83% [57]. Apart from this, additional criteria can be considered. For example, Hitzenbichler and colleagues performed a single-center retrospective analysis of 252 patients with blood cultures positive for CoNS other than S. epidermidis [54]. They considered an infection as “likely” when all of the following criteria where met: absence of another likely infection at the time of blood culture withdrawal; ≥ 2 blood cultures were positive with the same species or one of the findings was a relevant clinical specimen; and if the symptoms or markers of inflammation improved after therapy. To account for cases with only one positive blood culture, they designated these as “possible” infections, if in addition a foreign body was in situ. Additionally, according to the authors, the time to positivity, the resistance profile, and the sole growth in anaerobic blood cultures should also be examined for their potential do distinguish between infection and contamination. Leveraging sequencing or genotyping data to characterize the pathogenic potential of CoNS constitutes another approach that has been applied recently [58]. Aiming to find a genotype-phenotype correlation, Shelburne and colleagues showed with whole-genome sequencing that certain sequence types of S. epidermidis predominate among patients with complicated BSI [59]. Sánchez and colleagues sought to find a genetic marker to distinguish between commensal and infecting strains of S. epidermidis in prosthetic joint infections [60]. While some differences between the strains were noted, especially pertaining to antibiotic resistance and genes linked with increased pathogenicity, properties like biofilm formation were equally distributed. They concluded that despite some differences, no single distinction marker, which would be sensitive and specific enough, could be found.
In conclusion, it can be summarized that several distinguishing features exist, but a general and reliable method remains elusive. Another, yet different approach would entail taking the host response into account. This can be achieved by either measuring novel biomarkers or sets thereof [61], or by exploiting transcriptomics to measure differential gene expression [62]. Several research groups have developed transcriptomic tools utilizing different gene sets, while the feasibility on a large-scale and in point-of-care settings remains to be established [63,64]. We hypothesize that future steps could combine both modern microbiological methods with probing the host response. However, clinical data employing this dual approach are currently very scarce [65,66].

{kind=link}
{kind=link}
Table 1.
Detailed clinical information on the cases reported thus far with S. saccharolyticus, S. massiliensis, and the different S. petrasii subspecies.
Table 1.
Detailed clinical information on the cases reported thus far with S. saccharolyticus, S. massiliensis, and the different S. petrasii subspecies.
| Species | Main Source | Case Reports | References |
|---|---|---|---|
| S. saccharolyticus | Human skin (especially back skin), animal skin (gorilla), contaminated platelet concentrates | 13 Anaerobic endocarditis, prosthetic valve endocarditis, bacteremia, discitis and vertebral osteomyelitis, pneumonia, lung infections in cystic fibrosis patients, infection of the shoulder joint, bone marrow infection, pyomyositis, heart valve disease, spondylodiscitis, empyema. | [27,28,29,30,31,32,33,35,36,37,39,41,42] |
| S. massiliensis | Human skin | 1 Brain abscess. | [43,67,68] |
| S. petrasii | |||
| subsp. petrasii | Human skin and ear canal | 1 Cerebral hemorrhage. | [44] |
| subsp. croceilyticus | Human skin and ear canal | 1 Acute otitis externa. | [44] |
| subsp. jettensis | not documented | / Strains were isolated from human clinical samples which were expected to be sterile (catheters, biopsies, cerebrospinal fluid, blood and deep swabs). Moreover, they were found in mixtures with other CoNS, which made it difficult to assess their clinical significance. | [69,70] |
| subsp. pragensis | not documented | 6 Prostatitis, hand wound infection, appendicitis, pancreatitis, sepsis, phlegmona. | [71] |
4. Therapy and Prevention—Many Old Bugs, Little New Drugs
4.1. General Remarks
As opposed to strains acquired in community settings, nosocomial or healthcare-associated CoNS usually display a wider range of resistance patterns. Most notable are the higher resistance rates to beta-lactam antibiotics, including penicillin, oxacillin/methicillin, but also gentamicin, clindamycin, ciprofloxacin, and erythromycin. Hence, CoNS can be considered as relatively “difficult to treat”, which is somewhat in stark contrast to the aforementioned low pathogenicity compared to S. aureus or others. Moreover, CoNS have the ability to rapidly acquire and modify resistance genes. This ability subsequently promotes the transmission of these genes into different staphylococcal species or even other bacterial genera [72,73]. While methicillin-susceptible strains can and should be treated like methicillin-susceptible S. aureus infections, i.e., with an anti-staphylococcal penicillin e.g., (flucl-)oxacillin (or alternatively, cefazolin), the majority of CoNS in health-care settings require the use of second-line antibiotics such as vancomycin, daptomycin, or linezolid. Specific therapy recommendations depend on the affected organ system; on the presence of foreign bodies, the contingency to remove those; and patient characteristics, such as age, immune status, and comorbidities.
4.2. Glycopeptides
Vancomycin, the oldest glycopeptide antibiotic, offers a broad Gram-positive coverage through inhibiting cell wall synthesis [74]. Initially, its use was propagated for the treatment of penicillin-resistant Staphylococcus aureus, but with the advent of penicillinase-stable beta-lactam antibiotics, it soon became a reserve substance, e.g., for patients allergic to beta-lactams, and the drug of choice for infections caused by methicillin-resistant S. aureus (MRSA). Although the increasing prevalence of vancomycin-resistant enterococci (VRE) has limited its empiric use in settings with high VRE prevalence, the rate of vancomycin-resistance among staphylococci has remained steadily low [75]. Therapeutic drug monitoring (TDM) is recommended to ensure target attainment and to minimize drug toxicity, mainly nephrotoxicity. The so-called “red man syndrome” has been associated with rapid infusion. A recently revised guideline of the Infectious Disease Society of America (IDSA) has proposed a more sophisticated approach to TDM in the context of MRSA. It propagates computing the target area under the curve over 24 h to minimum inhibitory concentration (AUC/MIC) of 400–600 mg/L/hour on the basis of two or more measurements [76], while the more traditional approach relied on target trough levels as a surrogate marker [77].
Teicoplanin was discovered a few decades later [78], but with a similar mode of action, with clinically relevant differences pertaining to the MIC variability in some CoNS. In a French study, as much as one third of CoNS isolates were found to have an MIC of >4 µg/mL, and thus were non-susceptible to teicoplanin [79].
4.3. Lipoglycopeptides
Telavancin, dalbavancin, and oritavancin belong to the newly developed semisynthetic group of glycopeptides. Hence, the spectrum of antimicrobial activity resembles those of vancomycin and teicoplanin [80,81,82]. Their main indications per approval are acute bacterial skin and skin structure infections; in addition, telavancin can be used in pneumonia caused by MRSA as well. Intriguingly, dalbavancin offers the possibility of once-a-week dosing, owing to its long half-life of 8.5 days. Side effects of note are renal impairment (telavancin); gastrointestinal symptoms and liver enzyme elevation (dalbavancin); and infusion reaction and potential drug–drug interactions (oritavancin). Experience from extended clinical use is still relatively limited.
4.4. Daptomycin
Daptomycin is a cyclic lipopeptide that was discovered in the 1980s; however, its approval in the US and in Europe followed decades later in 2003 and 2006, respectively. This substance targets the cell membrane of Gram-positive bacteria. Its spectrum of activity is similar to that of glycopeptides. A low rate of resistance among CoNS has recently been reported [83]. Examples for its clinical use include prosthetic joint infections by oxacillin-resistant staphylococci with either non-susceptibility or reported allergy to vancomycin [84] and bacteremia by S. aureus, including right-sided endocarditis. Initially, this substance was approved primarily for acute bacterial skin and skin structure infections caused by Gram-positive cocci. It has also been proposed as an alternative to linezolid in the treatment of VRE infections, albeit with a higher than approved dose, i.e., 8–12 mg/kg per day [85]. Relevant adverse effects are a reversible muscle toxicity, which was especially prevalent during the early years when daptomycin was given twice daily, and eosinophilic pneumonia [86].
4.5. Oxazolidinones
Linezolid is the most widely used oxazolidinone, a group of bacteriostatic drugs that inhibit protein synthesis. The main role of linezolid has been as a therapeutic option for VRE infections. Currently, only limited data is available to recommend its use in CoNS as a first-line treatment. Still, there have been increasing reports on linezolid use in the past years [87,88]. In a large study on the feasibility of early oral step-down therapy in endocarditis, linezolid was among the antibiotics that were used, and was largely used in combination with other antibiotics [89]. The study which rightfully gained a lot of attention by showing the non-inferiority of early oral step-down therapy to the conventional intravenous therapy, was however underpowered to assess individual antibiotic combinations and their comparison among each other. Nevertheless, the continuing trend to shorten intravenous therapies in favor of an early step-down is likely to keep linezolid relevant, due to its oral formulation with high bioavailability. However, imprudent use of linezolid has been linked to the emergence of linezolid-resistant strains [90], in particular linezolid-resistant S. epidermidis [91,92,93]. CoNS have a higher and easier ability to acquire and develop linezolid-resistance factors following exposure to the drug. The incidence of linezolid resistance in CoNS is currently higher than in S. aureus. It is believed that linezolid resistance originally emerged in CoNS, and then transmitted to S. aureus [94]. Another concern is severe and partially irreversible side effects, such as bone marrow toxicity, lactic acidosis, and neuropathies. The risk for adverse events steeply increases after 2 weeks. Another limitation is the restriction of approval for a maximum of 28 days, which hampers its longer-term use in, e.g., bone and joint infections [95].
4.6. Alternatives and Biofilm-Active Substances
Alternative substances that are of importance, especially in non-critical, localized infections, such as skin and soft tissue infections or bone and joint infections, are e.g., co-trimoxazole, clindamycin, and doxycycline. All of these possess a high oral bioavailability [96]. In foreign body-related infections, the additive use of a biofilm-active substance has been propagated by relevant guidelines and experts [84,97,98]. For CoNS, these are largely rifampicin and, to a lesser extent, fosfomycin [99].
5. Conclusions
In conclusion, CoNS form a large group of skin microbiota that play an increasingly important role, especially in health-care associated infections. The advent of MALDI-TOF MS in routine microbiology diagnostics and the increasing feasibility of whole-genome sequencing will bring even more CoNS species to life, while also helping to better characterize their pathogenicity and resistance profiles. The main challenge in routine diagnostics remains to correctly assign the causative role of CoNS recovered from primarily sterile materials, as no single or composite diagnostic tool with a sufficiently high sensitivity and specificity exists to allow for a reliable diagnosis. Future studies aiming to leverage both modern pathogen detection methods and assessment of the host response could help shed light on the clinical utility on such a combined approach. Moreover, clinical data are highly needed especially for the rarer and newly described CoNS.
Author Contributions
Conceptualization, R.M. and C.P.; methodology, R.M. and K.L.; writing—original draft preparation, R.M. and K.L.; writing—review and editing, R.M., K.L., S.L.B., and C.P.; visualization, R.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
We are thankful to Alexa N. Lauer for the proofreading of this manuscript. We acknowledge support by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) and Saarland University within the funding programme Open Access Publishing.
Conflicts of Interest
C.P. reports receiving a research grant from MeMed Diagnostics. All other authors declare no conflict of interest.
References
- Becker, K.; Both, A.; Weißelberg, S.; Heilmann, C.; Rohde, H. Emergence of coagulase-negative staphylococci. Expert. Rev. Anti. Infect. Ther. 2020, 18, 349–366. [Google Scholar] [CrossRef] [PubMed]
- Pain, M.; Wolden, R.; Jaén-Luchoro, D.; Salvà-Serra, F.; Iglesias, B.P.; Karlsson, R.; Klingenberg, C.; Cavanagh, J.P. Staphylococcus borealis sp. nov., isolated from human skin and blood. Int. J. Syst. Evol. Microbiol. 2020, 70. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Schaumburg, F.; Kearns, A.; Larsen, A.R.; Lindsay, J.A.; Skov, R.L.; Westh, H. Implications of identifying the recently defined members of the Staphylococcus aureus complex S. argenteus and S. schweitzeri: A position paper of members of the ESCMID Study Group for Staphylococci and Staphylococcal Diseases (ESGS). Clin. Microbiol. Infect. 2019, 25, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Alhussein, F.; Fürstenberg, J.; Gaupp, R.; Eisenbeis, J.; Last, K.; Becker, S.L.; Papan, C. Human infections caused by Staphylococcus argenteus in Germany: Genetic characterisation and clinical implications of novel species designation. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 2461–2465. [Google Scholar] [CrossRef]
- Nurjadi, D.; Last, K.; Klein, S.; Boutin, S.; Schmack, B.; Mueller, F.; Heeg, K.; Ruhparwar, A.; Heininger, A.; Zanger, P. Nasal colonization with Staphylococcus aureus is a risk factor for ventricular assist device infection in the first year after implantation: A prospective, single-centre, cohort study. J. Infect. 2020, 80, 511–518. [Google Scholar] [CrossRef]
- Aldman, M.H.; Rasmussen, M.; Olaison, L.; Påhlman, L.I. Endocarditis due to Staphylococcus lugdunensis—A retrospective national registry-based study. Eur. J. Clin. Microbiol. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Hussain, M.; Kohler, C.; Becker, K. Role of SrtA in Pathogenicity of Staphylococcus lugdunensis. Microorganisms 2020, 8, 1975. [Google Scholar] [CrossRef] [PubMed]
- Taha, L.; Stegger, M.; Söderquist, B. Staphylococcus lugdunensis: Antimicrobial susceptibility and optimal treatment options. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1449–1455. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, S.; Fong, S.S. Computational Modeling of the Human Microbiome. Microorganisms 2020, 8, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvani, A.P.; Parpia, A.S.; Foster, E.M.; Singer, B.H.; Fitzpatrick, M.C. Improving the prognosis of health care in the USA. Lancet 2020, 395, 524–533. [Google Scholar] [CrossRef]
- Papan, C.; Förster, K.; Herterich, R.; Schulze, A.; Schubert, S.; Flemmer, A.W. Identification and Containment of a Cluster of Two Bacillus cereus Infections in a Neonatal Intensive Care Unit. Can. J. Infect. Dis. Med. Microbiol. 2019, 2019, 1506583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eichel, V.; Papan, C.; Mutters, N.T. Update Hygiene: Prevention of Vascular Catheter-Associated Infections in Premature and Newborn Infants. Klinische Padiatrie 2019, 231, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Papan, C.; Karremann, M.; Weis, M.; Petzold, A.; Zahn, K.; Schroten, H.; Weichert, S.; Tenenbaum, T. A 28-Day-Old Boy with Multifocal Osteomyelitis Mimicking Non-Accidental Injury. Klinische Padiatrie 2021, 233, 91–93. [Google Scholar] [CrossRef]
- Escalante, M.J.; Ceriani-Cernadas, J.M.; D’Apremont, I.; Bancalari, A.; Webb, V.; Genes, L.; Villarroel, L.; Munoz, E.; Tapia, J.L. Late Onset Sepsis in Very Low Birth Weight Infants in the South American NEOCOSUR Network. Pediatr. Infect. Dis. J. 2018, 37, 1022–1027. [Google Scholar] [CrossRef]
- Wisplinghoff, H.; Bischoff, T.; Tallent, S.M.; Seifert, H.; Wenzel, R.P.; Edmond, M.B. Nosocomial bloodstream infections in US hospitals: Analysis of 24,179 cases from a prospective nationwide surveillance study. Clin. Infect. Dis. 2004, 39, 309–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenthal, V.D.; Chaparro, G.J.; Servolo-Medeiros, E.A.; Souza-Fram, D.; Escudero, D.; Gualtero-Trujillo, S.M.; Morfin-Otero, R.; Gonzalez-Diaz, E.; Rodriguez-Noriega, E.; Altuzar-Figueroa, M.A.; et al. An eight-year multicenter study on short-term peripheral intravenous catheter-related bloodstream infection rates in 100 intensive care units of 9 countries in Latin America: Argentina, Brazil, Colombia, Costa Rica, Dominican Republic, Ecuador, Mexico, Panama, and Venezuela. Findings of the International Nosocomial Infection Control Consortium (INICC). Infect. Control Hosp. Epidemiol. 2021, 1–7. [Google Scholar] [CrossRef]
- Ott, E.; Saathoff, S.; Graf, K.; Schwab, F.; Chaberny, I.F. The prevalence of nosocomial and community acquired infections in a university hospital: An observational study. Dtsch. Aerzteblatt Int. 2013, 110, 533–540. [Google Scholar] [CrossRef] [Green Version]
- Noshak, M.A.; Rezaee, M.A.; Hasani, A.; Mirzaii, M. The Role of the Coagulase-negative Staphylococci (CoNS) in Infective Endocarditis; A Narrative Review from 2000 to 2020. Curr Pharm Biotechnol. 2020, 21, 1140–1153. [Google Scholar] [CrossRef]
- Kranjec, C.; Morales Angeles, D.; Torrissen Mårli, M.; Fernández, L.; García, P.; Kjos, M.; Diep, D.B. Staphylococcal Biofilms: Challenges and Novel Therapeutic Perspectives. Antibiotics 2021, 10, 131. [Google Scholar] [CrossRef]
- Ruiz-Ripa, L.; Gómez, P.; Alonso, C.A.; Camacho, M.C.; Ramiro, Y.; de la Puente, J.; Fernández-Fernández, R.; Quevedo, M.Á.; Blanco, J.M.; Báguena, G.; et al. Frequency and Characterization of Antimicrobial Resistance and Virulence Genes of Coagulase-Negative Staphylococci from Wild Birds in Spain. Detection of tst-Carrying, S. sciuri Isolates. Microorganisms 2020, 8, 1317. [Google Scholar] [CrossRef]
- Servier Medical Art. Available online: https://smart.servier.com (accessed on 1 March 2021).
- Heß, S.; Gallert, C. Staphylococcus argensis sp. nov., a novel staphylococcal species isolated from an aquatic environment. Int. J. Syst. Evol. Microbiol. 2015, 65, 2661–2665. [Google Scholar] [CrossRef] [Green Version]
- Pantůček, R.; Sedláček, I.; Indráková, A.; Vrbovská, V.; Mašlaňová, I.; Kovařovic, V.; Švec, P.; Králová, S.; Krištofová, L.; Kekláková, J.; et al. Staphylococcus edaphicus sp. nov., Isolated in Antarctica, Harbors the mecC Gene and Genomic Islands with a Suspected Role in Adaptation to Extreme Environments. Appl. Environ. Microbiol. 2018, 84. [Google Scholar] [CrossRef] [Green Version]
- MacFadyen, A.C.; Drigo, I.; Harrison, E.M.; Parkhill, J.; Holmes, M.A.; Paterson, G.K. Staphylococcus caeli sp. nov., isolated from air sampling in an industrial rabbit holding. Int. J. Syst. Evol. Microbiol. 2019, 69, 82–86. [Google Scholar] [CrossRef]
- MacFadyen, A.C.; Leroy, S.; Harrison, E.M.; Parkhill, J.; Holmes, M.A.; Paterson, G.K. Staphylococcus pseudoxylosus sp. nov., isolated from bovine mastitis. Int. J. Syst. Evol. Microbiol. 2019, 69, 2208–2213. [Google Scholar] [CrossRef] [PubMed]
- Naushad, S.; Kanevets, U.; Nobrega, D.; Carson, D.; Dufour, S.; Roy, J.P.; Lewis, P.J.; Barkema, H.W. Staphylococcus debuckii sp. nov., a coagulase-negative species from bovine milk. Int. J. Syst. Evol. Microbiol. 2019, 69, 2239–2249. [Google Scholar] [CrossRef] [PubMed]
- Westblom, T.U.; Gorse, G.J.; Milligan, T.W.; Schindzielorz, A.H. Anaerobic endocarditis caused by Staphylococcus saccharolyticus. J. Clin. Microbiol. 1990, 28, 2818–2819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnan, S.; Haglund, L.; Ashfaq, A.; Leist, P.; Roat, T. Prosthetic valve endocarditis due to Staphylococcus saccharolyticus. Clin. Infect. Dis. 1996, 22, 722–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinbrueckner, B.; Singh, S.; Freney, J.; Kuhnert, P.; Pelz, K.; Aufenanger, J. Facing a mysterious hospital outbreak of bacteraemia due to Staphylococcus saccharolyticus. J. Hosp. Infect. 2001, 49, 305–307. [Google Scholar] [CrossRef]
- Godreuil, S.; Jean-Pierre, H.; Morel, J.; Darbas, H.; Jumas-Bilak, E.; Bañuls, A.L.; Marchandin, H. Unusual case of spondylodiscitis due to Staphylococcus saccharolyticus. Joint Bone Spine 2005, 72, 91–93. [Google Scholar] [CrossRef]
- Mikhael, M.M.; Bach, H.G.; Huddleston, P.M.; Maus, T.P.; Berbari, E.F. Multilevel diskitis and vertebral osteomyelitis after diskography. Orthopedics 2009, 32, 60. [Google Scholar] [CrossRef]
- Worlitzsch, D.; Rintelen, C.; Böhm, K.; Wollschläger, B.; Merkel, N.; Borneff-Lipp, M.; Döring, G. Antibiotic-resistant obligate anaerobes during exacerbations of cystic fibrosis patients. Clin. Microbiol. Infect. 2009, 15, 454–460. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Yu, C.; Wang, X. A case of Staphylococcus saccharolyticus pneumonia. Int. J. Infect. Dis. 2009, 13, e43–e46. [Google Scholar] [CrossRef] [Green Version]
- Ali, H.; Rood, I.G.; de Korte, D.; Ramírez-Arcos, S. Strict anaerobic Staphylococcus saccharolyticus isolates recovered from contaminated platelet concentrates fail to multiply during platelet storage. Transfusion 2012, 52, 916–917. [Google Scholar] [CrossRef]
- Schneeberger, A.G.; Yian, E.; Steens, W. Injection-induced low-grade infection of the shoulder joint: Preliminary results. Arch. Orthop. Trauma Surg. 2012, 132, 1387–1392. [Google Scholar] [CrossRef]
- Liu, C.J.; Sun, B.; Guo, J.; He, J.L.; Feng, B.; Wang, H.G.; Cao, K.-K.; Liu, T.; Shen, D.-X. A case of bone marrow infection by Staphylococcus saccharolyticus. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 1161–1163. [Google Scholar]
- Young, N.; Bhally, H. Bilateral Neck Pyomyositis Caused by Staphylococcus capitis and Staphylococcus saccharolyticus in a Diabetic Adult. Case Rep. Infect. Dis. 2017, 2017, 3713212. [Google Scholar] [CrossRef] [Green Version]
- Brüggemann, H.; Poehlein, A.; Brzuszkiewicz, E.; Scavenius, C.; Enghild, J.J.; Al-Zeer, M.A.; Brinkmann, V.; Jensen, A.; Söderquist, B. Staphylococcus saccharolyticus Isolated From Blood Cultures and Prosthetic Joint Infections Exhibits Excessive Genome Decay. Front. Microbiol. 2019, 10, 478. [Google Scholar] [CrossRef]
- Oberbach, A.; Friedrich, M.; Lehmann, S.; Schlichting, N.; Kullnick, Y.; Gräber, S.; Buschmann, T.; Hagl, C.; Bagaev, E.; Gruhle, M.; et al. Bacterial infiltration in structural heart valve disease. J. Thorac Cardiovasc. Surg. 2019. [Google Scholar] [CrossRef] [Green Version]
- Ahle, C.M.; Stødkilde, K.; Afshar, M.; Poehlein, A.; Ogilvie, L.A.; Söderquist, B.; Hüpeden, J.; Brüggemann, H. Staphylococcus saccharolyticus: An Overlooked Human Skin Colonizer. Microorganisms 2020, 8, 1105. [Google Scholar] [CrossRef]
- Trojani, M.C.; Lamy, B.; Ruimy, R.; Amoretti, N.; Risso, K.; Roux, C. An unusual Staphylococcus saccharolyticus spondylodiscitis post kyphoplasty: A case report. BMC Infect. Dis. 2020, 20, 539. [Google Scholar] [CrossRef]
- Wang, P.; Liu, Y.; Xu, Y.; Xu, Z. Staphylococcus saccharolyticus infection: Case series with a PRISMA-compliant systemic review. Medicine 2020, 99, e20686. [Google Scholar] [CrossRef]
- Al Masalma, M.; Raoult, D.; Roux, V. Staphylococcus massiliensis sp. nov., isolated from a human brain abscess. Int. J. Syst. Evol. Microbiol. 2010, 60, 1066–1072. [Google Scholar] [CrossRef]
- Pantůček, R.; Švec, P.; Dajcs, J.J.; Machová, I.; Černohlávková, J.; Šedo, O.; Gelbíčová, T.; Mašlaňová, I.; Doškař, J.; Zdráhal, Z.; et al. Staphylococcus petrasii sp. nov. including S. petrasii subsp. petrasii subsp. nov. and S. petrasii subsp. croceilyticus subsp. nov., isolated from human clinical specimens and human ear infections. Syst. Appl. Microbiol. 2013, 36, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.P.; Anderson, W.E.; Beam, K.; Taylor, B.; Ellerman, J.; Kowalkowski, M.A. The Association Between Antibiotic Delay Intervals and Hospital Mortality Among Patients Treated in the Emergency Department for Suspected Sepsis. Crit. Care Med. 2021. [Google Scholar] [CrossRef]
- Papan, C.; Willersinn, M.; Weiß, C.; Karremann, M.; Schroten, H.; Tenenbaum, T. Antibiotic utilization in hospitalized children under 2 years of age with influenza or respiratory syncytial virus infection—A comparative, retrospective analysis. BMC Infect. Dis. 2020, 20, 606. [Google Scholar] [CrossRef] [PubMed]
- Meyer, S.; Papan, C.; Last, K. A global health perspective on SARS-CoV-2-hazards, disaster and hope. Wien Med. Wochenschr. 2020, 170, 357–358. [Google Scholar] [CrossRef]
- Troncoso, C.; Pavez, M.; Cerda, A.; Oporto, M.; Villarroel, D.; Hofmann, E.; Rios, E.; Sierralta, A.; Copelli, L.; Barrientos, L. MALDI-TOF MS and 16S RNA Identification of Culturable Gastric Microbiota: Variability Associated with the Presence of Helicobacter pylori. Microorganisms 2020, 8, 1763. [Google Scholar] [CrossRef]
- Sy, I.; Margardt, L.; Ngbede, E.O.; Adah, M.I.; Yusuf, S.T.; Keiser, J.; Rehner, J.; Utzinger, J.; Poppert, S.; Becker, S.L. Identification of Adult Fasciola spp. Using Matrix-Assisted Laser/Desorption Ionization Time-of-Flight (MALDI-TOF) Mass Spectrometry. Microorganisms 2020, 9, 82. [Google Scholar] [CrossRef] [PubMed]
- Chiu, K.H.Y.; Lam, R.P.K.; Chan, E.; Lau, S.K.P.; Woo, P.C.Y. Emergence of Staphylococcus lugdunensis as a Cause of Urinary Tract Infection: Results of the Routine Use of MALDI-TOF MS. Microorganisms 2020, 8, 381. [Google Scholar] [CrossRef] [Green Version]
- Lavecchia, A.; Chiara, M.; De Virgilio, C.; Manzari, C.; Monno, R.; De Carlo, A.; Pazzani, C.; Horner, D.; Pesole, G.; Placido, A. Staphylococcus arlettae Genomics: Novel Insights on Candidate Antibiotic Resistance and Virulence Genes in an Emerging Opportunistic Pathogen. Microorganisms 2019, 7, 580. [Google Scholar] [CrossRef] [Green Version]
- Lavecchia, A.; Chiara, M.; De Virgilio, C.; Manzari, C.; Pazzani, C.; Horner, D.; Pesole, G.; Placido, A. Comparative genomics suggests a taxonomic revision of the Staphylococcus cohnii species complex. Genome Biol. Evol. 2021. [Google Scholar] [CrossRef]
- Becker, K.; Heilmann, C.; Peters, G. Coagulase-negative staphylococci. Clin. Microbiol. Rev. 2014, 27, 870–926. [Google Scholar] [CrossRef] [Green Version]
- Hitzenbichler, F.; Simon, M.; Salzberger, B.; Hanses, F. Clinical significance of coagulase-negative staphylococci other than S. epidermidis blood stream isolates at a tertiary care hospital. Infection 2017, 45, 179–186. [Google Scholar] [CrossRef]
- Beekmann, S.E.; Diekema, D.J.; Doern, G.V. Determining the clinical significance of coagulase-negative staphylococci isolated from blood cultures. Infect. Control Hosp. Epidemiol. 2005, 26, 559–566. [Google Scholar] [CrossRef]
- Favre, B.; Hugonnet, S.; Correa, L.; Sax, H.; Rohner, P.; Pittet, D. Nosocomial bacteremia: Clinical significance of a single blood culture positive for coagulase-negative staphylococci. Infect. Control. Hosp. Epidemiol. 2005, 26, 697–702. [Google Scholar] [CrossRef] [PubMed]
- García-Vázquez, E.; Fernández-Rufete, A.; Hernández-Torres, A.; Canteras, M.; Ruiz, J.; Gómez, J. When is coagulase-negative Staphylococcus bacteraemia clinically significant? Scand. J. Infect. Dis. 2013, 45, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Méric, G.; Mageiros, L.; Pensar, J.; Laabei, M.; Yahara, K.; Pascoe, B.; Kittiwan, N.; Tadee, P.; Post, V.; Lamble, S.; et al. Disease-associated genotypes of the commensal skin bacterium Staphylococcus epidermidis. Nat. Commun. 2018, 9, 5034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shelburne, S.A.; Dib, R.W.; Endres, B.T.; Reitzel, R.; Li, X.; Kalia, A.; Sahasrabhojane, P.; Chaftari, A.-M.; Hachem, R.; Vargas-Cruz, N.S.; et al. Whole-genome sequencing of Staphylococcus epidermidis bloodstream isolates from a prospective clinical trial reveals that complicated bacteraemia is caused by a limited number of closely related sequence types. Clin. Microbiol. Infect. 2020, 26, e1–e8. [Google Scholar] [CrossRef]
- Sánchez, A.; Benito, N.; Rivera, A.; García, L.; Miró, E.; Mur, I.; González, Y.; Gutiérrez, C.; Horcajada, J.P.; Espinal, P.; et al. Pathogenesis of Staphylococcus epidermidis in prosthetic joint infections: Can identification of virulence genes differentiate between infecting and commensal strains? J. Hosp. Infect. 2020, 105. [Google Scholar] [CrossRef]
- Ashkenazi-Hoffnung, L.; Oved, K.; Navon, R.; Friedman, T.; Boico, O.; Paz, M.; Kronenfeld, G.; Etshtein, L.; Cohen, A.; Gottlieb, T.M.; et al. A host-protein signature is superior to other biomarkers for differentiating between bacterial and viral disease in patients with respiratory infection and fever without source: A prospective observational study. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1361–1371. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, T.E. Hunting for Genes Linked to Risk of, Not From, Bloodstream Infection. Crit. Care Med. 2020, 48, 1696–1697. [Google Scholar] [CrossRef]
- Mahajan, P.; Kuppermann, N.; Mejias, A.; Suarez, N.; Chaussabel, D.; Casper, T.C.; Smith, B.; Alpern, E.R.; Anders, J.; Atabaki, S.M.; et al. Association of RNA Biosignatures With Bacterial Infections in Febrile Infants Aged 60 Days or Younger. JAMA 2016, 316, 846–857. [Google Scholar] [CrossRef]
- Mayhew, M.B.; Buturovic, L.; Luethy, R.; Midic, U.; Moore, A.R.; Roque, J.A.; Shaller, B.D.; Asuni, T.; Rawling, D.; Remmel, M.; et al. A generalizable 29-mRNA neural-network classifier for acute bacterial and viral infections. Nat. Commun. 2020, 11, 1177. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.C.; Chang, J.C.; Mao, X.W.; Hsu, W.T.; Chen, S.Y.; Chen, Y.C.; How, C.-K. Combining Procalcitonin and Rapid Multiplex Respiratory Virus Testing for Antibiotic Stewardship in Older Adult Patients With Severe Acute Respiratory Infection. J. Am. Med. Dir. Assoc. 2020, 21, 62–67. [Google Scholar] [CrossRef]
- Moradi, T.; Bennett, N.; Shemanski, S.; Kennedy, K.; Schlachter, A.; Boyd, S. Use of Procalcitonin and a Respiratory Polymerase Chain Reaction Panel to Reduce Antibiotic Use via an Electronic Medical Record Alert. Clin. Infect. Dis. 2020, 71, 1684–1689. [Google Scholar] [CrossRef]
- Srivastav, R.; Singh, A.; Jangir, P.K.; Kumari, C.; Muduli, S.; Sharma, R. Genome Sequence of Staphylococcus massiliensis Strain S46, Isolated from the Surface of Healthy Human Skin. Genome Announc. 2013, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zong, Z. The newly-recognized species Staphylococcus massiliensis is likely to be part of the human skin microflora. Antonie Van Leeuwenhoek 2012, 101, 449–451. [Google Scholar] [CrossRef]
- De Bel, A.; Van Hoorde, K.; Wybo, I.; Vandoorslaer, K.; Echahidi, F.; De Brandt, E.; Schumann, P.; Ieven, M.; Soetens, O.; Piérard, D.; et al. Staphylococcus jettensis sp. nov., a coagulase-negative staphylococcal species isolated from human clinical specimens. Int. J. Syst. Evol. Microbiol. 2013, 63, 3250–3256. [Google Scholar] [CrossRef]
- De Bel, A.; Švec, P.; Petráš, P.; Sedláček, I.; Pantůček, R.; Echahidi, F.; Piérard, D.; Vandamme, P. Reclassification of Staphylococcus jettensis De Bel et al. 2013 as Staphylococcus petrasii subsp. jettensis subsp. nov. and emended description of Staphylococcus petrasii Pantucek et al. 2013. Int. J. Syst. Evol. Microbiol. 2014, 64, 4198–4201. [Google Scholar] [CrossRef]
- Švec, P.; Bel, A.; Sedláček, I.; Petráš, P.; Gelbíčová, T.; Černohlávková, J.; Mašlanová, I.; Cnockaert, M.; Varbanovová, I.; Echahidi, F.; et al. Staphylococcus petrasii subsp. pragensis subsp. nov., occurring in human clinical material. Int. J. Syst. Evol. Microbiol. 2015, 65, 2071–2077. [Google Scholar] [CrossRef] [PubMed]
- Moawad, A.A.; Hotzel, H.; Awad, O.; Roesler, U.; Hafez, H.M.; Tomaso, H.; Neubauer, H.; El-Adawy, H. Evolution of Antibiotic Resistance of Coagulase-Negative Staphylococci Isolated from Healthy Turkeys in Egypt: First Report of Linezolid Resistance. Microorganisms 2019, 7, 476. [Google Scholar] [CrossRef] [Green Version]
- Otto, M. Coagulase-negative staphylococci as reservoirs of genes facilitating MRSA infection: Staphylococcal commensal species such as Staphylococcus epidermidis are being recognized as important sources of genes promoting MRSA colonization and virulence. Bioessays 2013, 35, 4–11. [Google Scholar] [CrossRef] [Green Version]
- McCormick, M.H.; McGuire, J.M.; Pittenger, G.E.; Pittenger, R.C.; Stark, W.M. Vancomycin, a new antibiotic. I. Chemical and biologic properties. Antibiot. Annu. 1955, 3, 606–611. [Google Scholar]
- Da Costa, T.M.; Cuba, G.T.; Morgado, P.G.M.; Nicolau, D.P.; Nouér, S.A.; Dos Santos, K.R.N.; Kiffer, C.B.V. Pharmacodynamic comparison of different antimicrobial regimens against Staphylococcus aureus bloodstream infections with elevated vancomycin minimum inhibitory concentration. BMC Infect. Dis. 2020, 20, 74. [Google Scholar] [CrossRef] [Green Version]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic Monitoring of Vancomycin for Serious Methicillin-resistant Staphylococcus aureus Infections: A Revised Consensus Guideline and Review by the American Society of Health-system Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Clin. Infect. Dis. 2020, 71, 1361–1364. [Google Scholar] [CrossRef]
- Rybak, M.J.; Lomaestro, B.M.; Rotschafer, J.C.; Moellering, R.C.; Craig, W.A.; Billeter, M.; Dalovisio, J.R.; Levine, D.P. Vancomycin therapeutic guidelines: A summary of consensus recommendations from the infectious diseases Society of America, the American Society of Health-System Pharmacists, and the Society of Infectious Diseases Pharmacists. Clin. Infect. Dis. 2009, 49, 325–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cynamon, M.H.; Granato, P.A. Comparison of the in vitro activities of teichomycin A2 and vancomycin against staphylococci and enterococci. Antimicrob. Agents Chemother. 1982, 21, 504–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Decousser, J.W.; Desroches, M.; Bourgeois-Nicolaos, N.; Potier, J.; Jehl, F.; Lina, G.; Cattoir, V.; Vandenesh, F.; Doucet-Populaire, F. Susceptibility trends including emergence of linezolid resistance among coagulase-negative staphylococci and meticillin-resistant Staphylococcus aureus from invasive infections. Int. J. Antimicrob. Agents 2015, 46, 622–630. [Google Scholar] [CrossRef]
- Berti, A.D.; Harven, L.T.; Bingley, V. Distinct Effectiveness of Oritavancin against Tolerance-Induced Staphylococcus aureus. Antibiotics 2020, 9, 789. [Google Scholar] [CrossRef]
- Saravolatz, L.D.; Cleveland, K.O.; Rikabi, K.; Hassoun, A.; Reilly, J.; Johnson, L.B.; Spak, C.; Valenti, S.; Szpunar, S. Real-world use of telavancin in the treatment of osteomyelitis. Diagn. Microbiol. Infect. Dis. 2019, 95, 185–190. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Mendes, R.E.; Duncan, L.R.; Flamm, R.K.; Sader, H.S. Activity of dalbavancin and comparator agents against Gram-positive cocci from clinical infections in the USA and Europe 2015–16. J. Antimicrob. Chemother. 2018, 73, 2748–2756. [Google Scholar] [CrossRef] [PubMed]
- Shariati, A.; Dadashi, M.; Chegini, Z.; van Belkum, A.; Mirzaii, M.; Khoramrooz, S.S.; Darban-Sarokhalil, D. The global prevalence of Daptomycin, Tigecycline, Quinupristin/Dalfopristin, and Linezolid-resistant Staphylococcus aureus and coagulase-negative staphylococci strains: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control. 2020, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satlin, M.J.; Nicolau, D.P.; Humphries, R.M.; Kuti, J.L.; Campeau, S.A.; Lewis, J.S.; Weinstein, M.P.; Jorgensen, J.H. Development of Daptomycin Susceptibility Breakpoints for Enterococcus faecium and Revision of the Breakpoints for Other Enterococcal Species by the Clinical and Laboratory Standards Institute. Clin. Infect. Dis. 2020, 70, 1240–1246. [Google Scholar] [CrossRef]
- Gray, D.A.; Wenzel, M. More Than a Pore: A Current Perspective on the In Vivo Mode of Action of the Lipopeptide Antibiotic Daptomycin. Antibiotics 2020, 9, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matrat, L.; Plaisant, F.; Barreto, C.; Claris, O.; Butin, M. Increasing use of linezolid in a tertiary NICU during a 10-year period: Reasons and concerns for the future. Antimicrob. Resist. Infect. Control. 2020, 9, 156. [Google Scholar] [CrossRef]
- Kramer, T.S.; Schwab, F.; Behnke, M.; Hansen, S.; Gastmeier, P.; Aghdassi, S.J.S. Linezolid use in German acute care hospitals: Results from two consecutive national point prevalence surveys. Antimicrob. Resist. Infect. Control. 2019, 8, 159. [Google Scholar] [CrossRef] [Green Version]
- Iversen, K.; Ihlemann, N.; Gill, S.U.; Madsen, T.; Elming, H.; Jensen, K.T.; Bruun, N.E.; Høfsten, D.E.; Fursted, K.; Christensen, J.J.; et al. Partial Oral versus Intravenous Antibiotic Treatment of Endocarditis. N. Engl. J. Med. 2019, 380, 415–424. [Google Scholar] [CrossRef]
- Kerschner, H.; Cabal, A.; Hartl, R.; Machherndl-Spandl, S.; Allerberger, F.; Ruppitsch, W.; Apfalter, P. Hospital outbreak caused by linezolid resistant Enterococcus faecium in Upper Austria. Antimicrob. Resist. Infect. Control. 2019, 8, 150. [Google Scholar] [CrossRef] [Green Version]
- Bouiller, K.; Ilic, D.; Wicky, P.H.; Cholley, P.; Chirouze, C.; Bertrand, X. Spread of clonal linezolid-resistant Staphylococcus epidermidis in an intensive care unit associated with linezolid exposure. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39. [Google Scholar] [CrossRef]
- Kosecka-Strojek, M.; Sadowy, E.; Gawryszewska, I.; Klepacka, J.; Tomasik, T.; Michalik, M.; Hryniewicz, W.; Miedzobrodzki, J. Emergence of linezolid-resistant Staphylococcus epidermidis in the tertiary children’s hospital in Cracow, Poland. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39. [Google Scholar] [CrossRef]
- Maarouf, L.; Omar, H.; El-Nakeeb, M.; Abouelfetouh, A. Prevalence and mechanisms of linezolid resistance among staphylococcal clinical isolates from Egypt. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 40. [Google Scholar] [CrossRef]
- Gu, B.; Kelesidis, T.; Tsiodras, S.; Hindler, J.; Humphries, R.M. The emerging problem of linezolid-resistant Staphylococcus. J. Antimicrob. Chemother. 2013, 68, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Theil, C.; Schmidt-Braekling, T.; Gosheger, G.; Schwarze, J.; Dieckmann, R.; Schneider, K.N.; Möllenbeck, B. Clinical use of linezolid in periprosthetic joint infections—A systematic review. J. Bone Jt. Infect. 2020, 6, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Shortridge, D.; Flamm, R.K. Comparative In Vitro Activities of New Antibiotics for the Treatment of Skin Infections. Clin. Infect. Dis. 2019, 68 (Suppl. 3), S200–S205. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- Høiby, N.; Bjarnsholt, T.; Moser, C.; Bassi, G.L.; Coenye, T.; Donelli, G.; Hall-Stoodley, L.; Holá, V.; Imbert, C.; Kirketerp-Møller, K.; et al. ESCMID guideline for the diagnosis and treatment of biofilm infections 2014. Clin. Microbiol. Infect. 2015, 21 (Suppl. 1), S1–S25. [Google Scholar] [CrossRef] [Green Version]
- Antonello, R.M.; Principe, L.; Maraolo, A.E.; Viaggi, V.; Pol, R.; Fabbiani, M.; Montagnani, F.; Lovecchio, A.; Luzzati, R.; Di Bella, S. Fosfomycin as Partner Drug for Systemic Infection Management. A Systematic Review of Its Synergistic Properties from In Vitro and In Vivo Studies. Antibiotics 2020, 9, 500. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Overview of CoNS, according to the predominantly affected organ site or infectious syndrome, from left to right: urinary tract; cardiac valves; prosthetic joints and vascular grafts; bloodstream infections; skin and soft tissue infections; the question mark designates species of unknown clinical relevance. Most prevalent and relevant species are highlighted in blue; species are depicted in accordance with their first description, from top to bottom. Pictograms were taken with permission from Servier Medical Art [21].
Figure 1.
Overview of CoNS, according to the predominantly affected organ site or infectious syndrome, from left to right: urinary tract; cardiac valves; prosthetic joints and vascular grafts; bloodstream infections; skin and soft tissue infections; the question mark designates species of unknown clinical relevance. Most prevalent and relevant species are highlighted in blue; species are depicted in accordance with their first description, from top to bottom. Pictograms were taken with permission from Servier Medical Art [21].

Figure 2.
Model for differentiation between contamination and infection pertaining to the finding of CoNS in a primary sterile material; BC: blood culture.
Figure 2.
Model for differentiation between contamination and infection pertaining to the finding of CoNS in a primary sterile material; BC: blood culture.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Michels, R.; Last, K.; Becker, S.L.; Papan, C. Update on Coagulase-Negative Staphylococci—What the Clinician Should Know. Microorganisms 2021, 9, 830. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9040830
AMA Style
Michels R, Last K, Becker SL, Papan C. Update on Coagulase-Negative Staphylococci—What the Clinician Should Know. Microorganisms. 2021; 9(4):830. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9040830
Chicago/Turabian StyleMichels, Ricarda, Katharina Last, Sören L. Becker, and Cihan Papan. 2021. "Update on Coagulase-Negative Staphylococci—What the Clinician Should Know" Microorganisms 9, no. 4: 830. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9040830
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.