
Differences in the On- and Off-Tumor Microbiota between Right- and Left-Sided Colorectal Cancer

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Sample Collection
2.2. DNA Extraction and 16S Ribosomal RNA Amplicon Sequencing
2.3. Statistical Analysis
3. Results
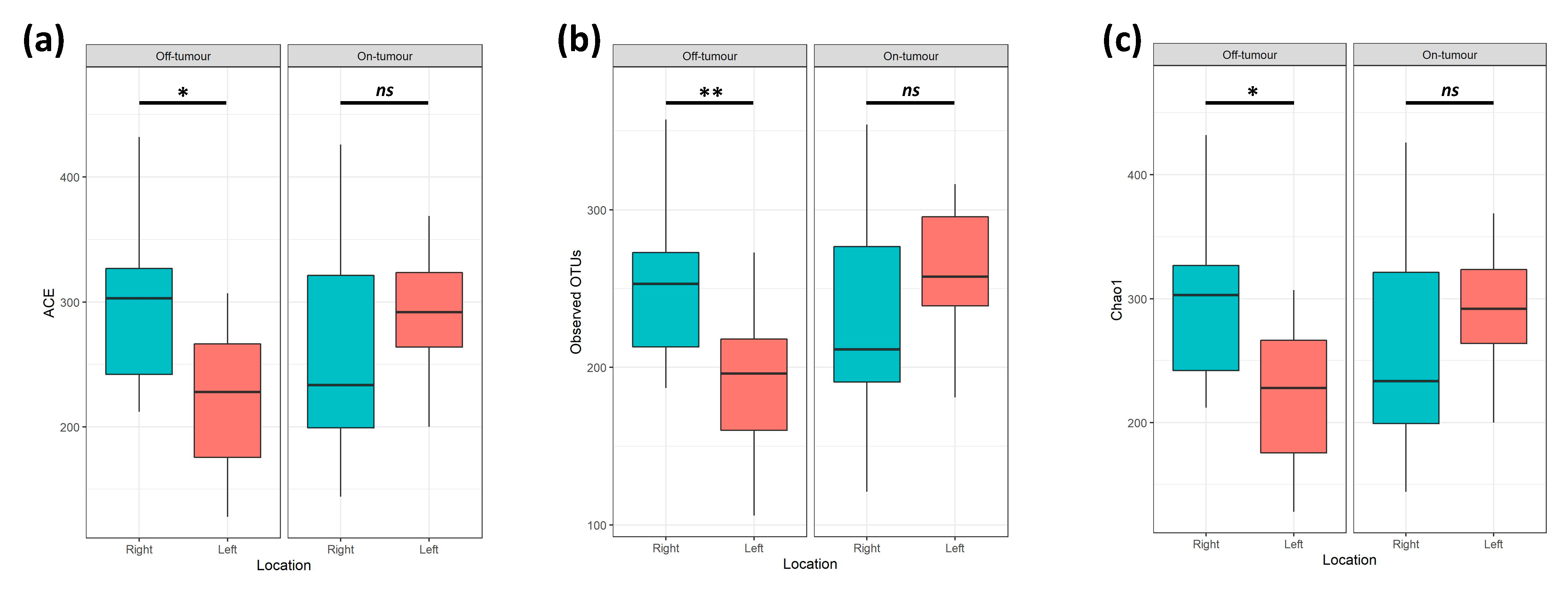
3.1. On- and Off-Tumor Bacterial Diversity between the Right and Left Colon
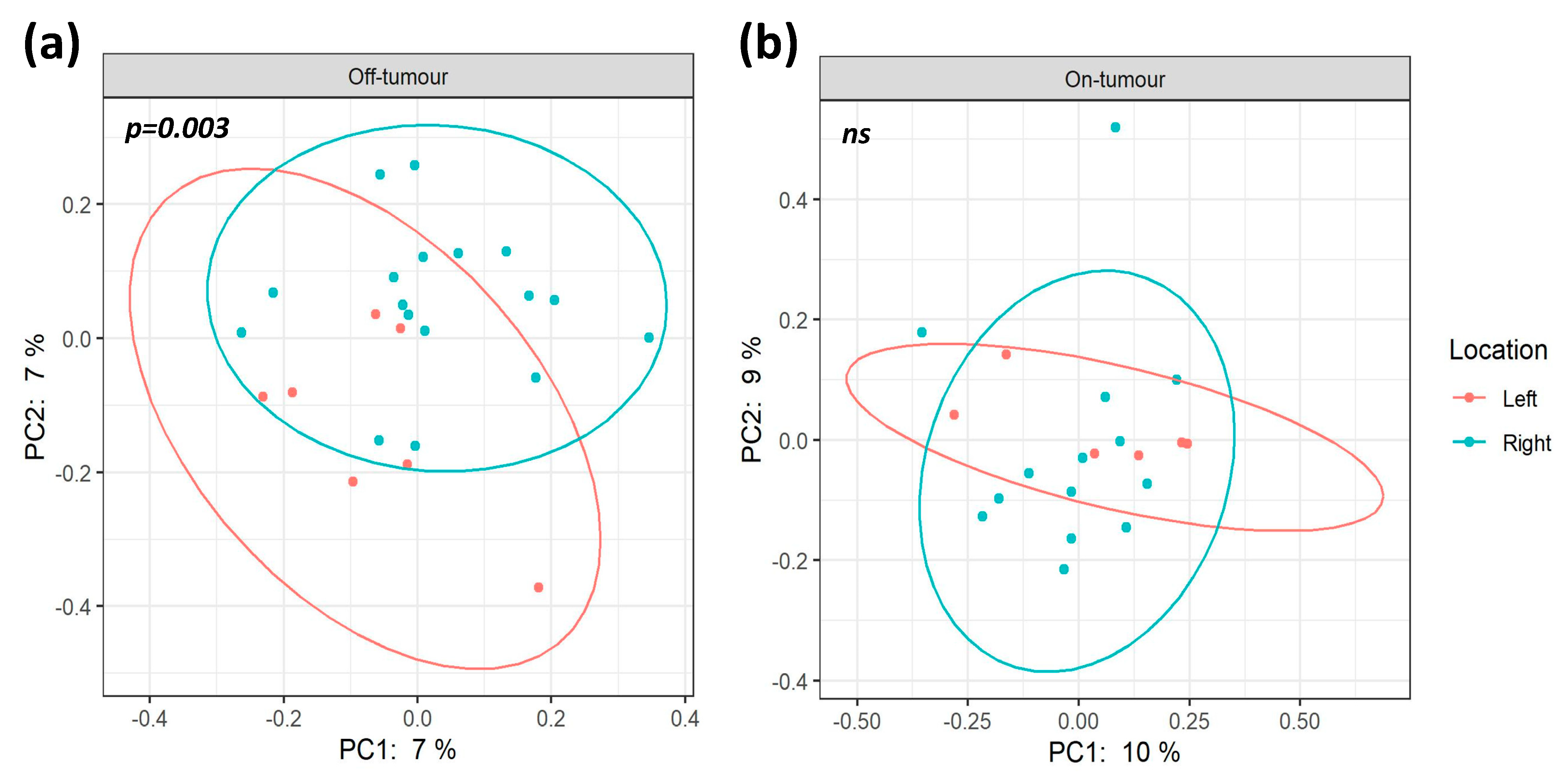
3.2. Gut Phylogenetic Profiles between Right- and Left-Sided Colorectal Cancer Patients
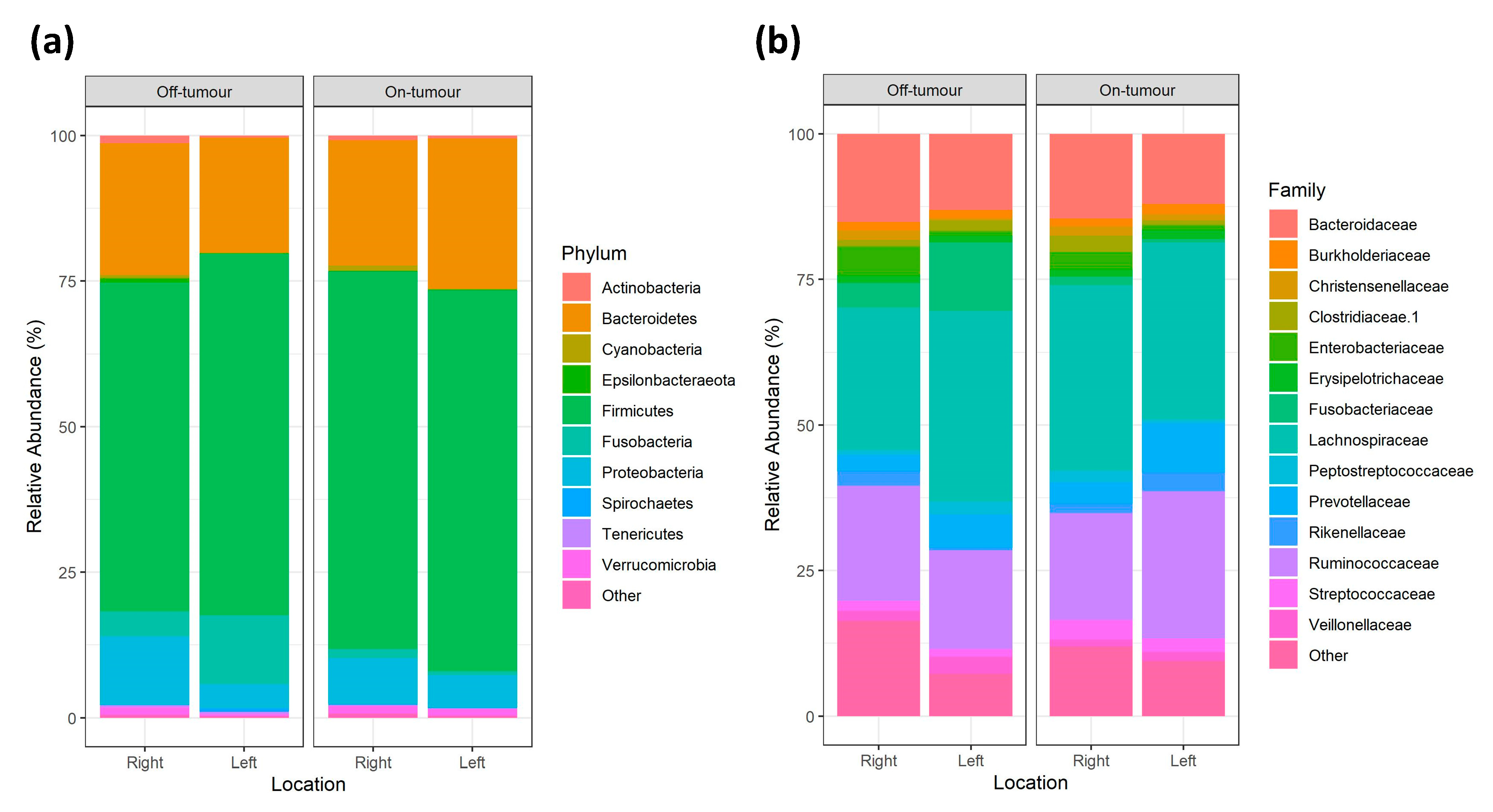
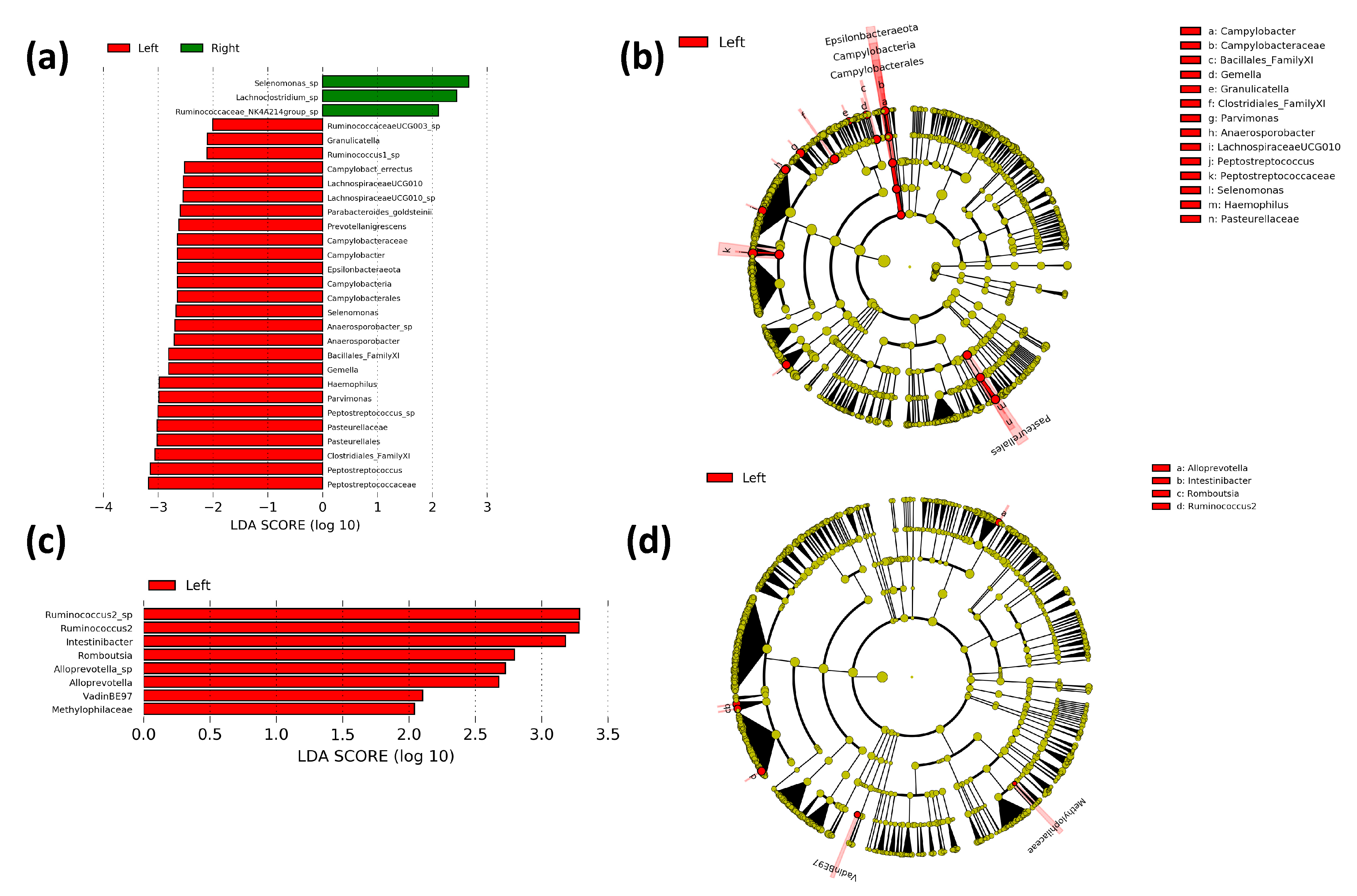
3.3. Comparison of Bacterial Taxa between the Right and Left Colon
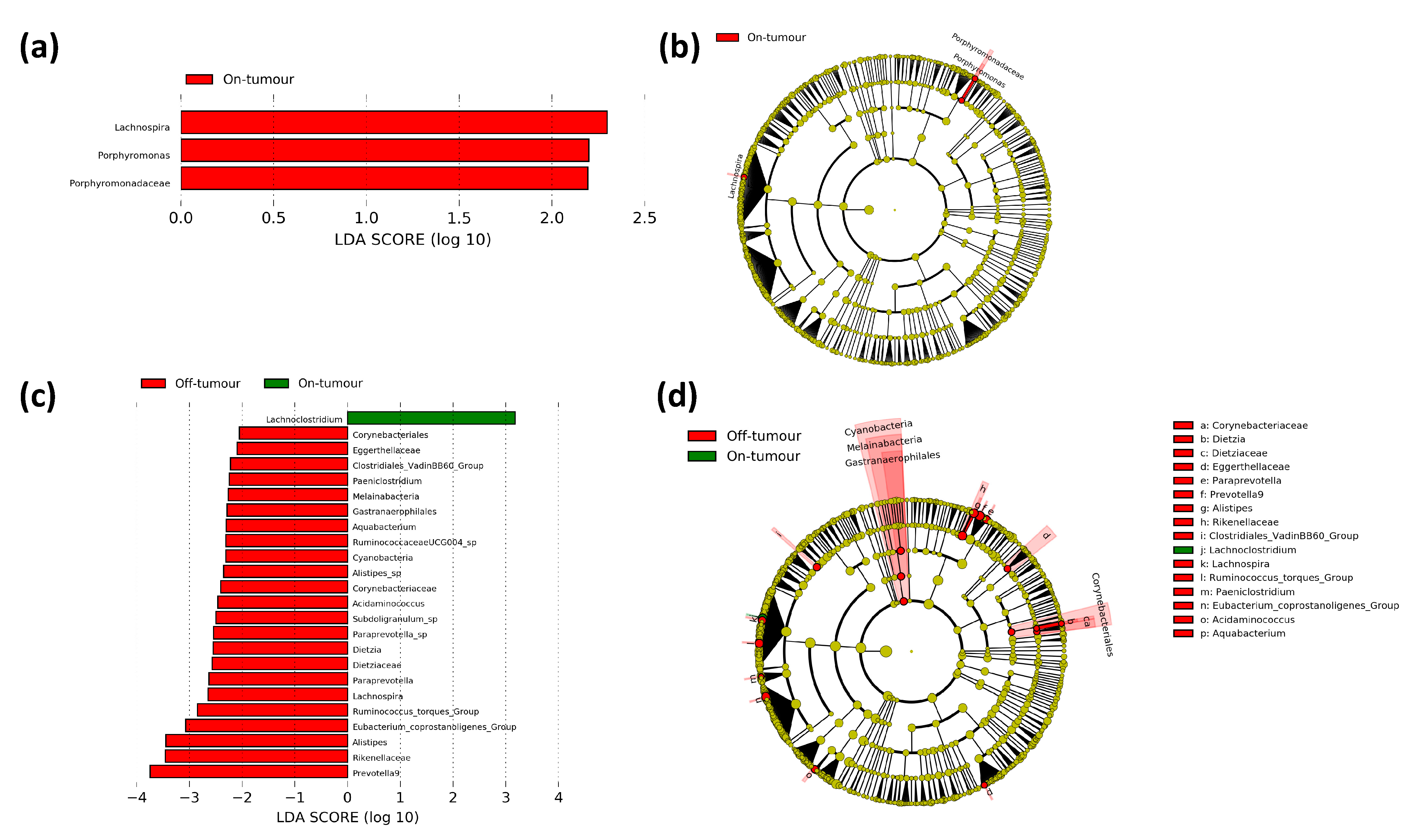
3.4. Difference in Paired On- and Off-Tumor Bacterial Taxa in Right- and Left-Sided Colorectal Cancer Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baran, B.; Ozupek, N.M.; Tetik, N.Y.; Acar, E.; Bekcioglu, O.; Baskin, Y. Difference Between Left-Sided and Right-Sided Colorectal Cancer: A Focused Review of Literature. Gastroenterol. Res. 2018, 11, 264–273. [Google Scholar] [CrossRef] [Green Version]
- Mukund, K.; Syulyukina, N.; Ramamoorthy, S.; Subramaniam, S. Right and left-sided colon cancers—Specificity of molecular mechanisms in tumorigenesis and progression. BMC Cancer 2020, 20, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Kwak, H.D.; Ju, J.K.; Lee, S.Y.; Kim, C.H.; Kim, Y.J.; Kim, H.R. Comparison of Right-side and Left-side Colon Cancers Following Laparoscopic Radical Lymphadenectomy. J. Investig. Surg. 2021, 34, 142–147. [Google Scholar] [CrossRef]
- Manyama, M.; Malyango, A.; Raoof, A.; Mligiliche, N.L.; Msuya, C.; Nassir, N.; Mtui, E. A variant source of arterial supply to the ascending, transverse and descending colon. Surg. Radiol. Anat. 2019, 41, 1383–1386. [Google Scholar] [CrossRef] [Green Version]
- De Renzi, G.; Gaballo, G.; Gazzaniga, P.; Nicolazzo, C. Molecular Biomarkers according to Primary Tumor Location in Colorectal Cancer: Current Standard and New Insights. Oncology 2020, 99, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Balchen, V.; Simon, K. Colorectal cancer development and advances in screening. Clin. Interv. Aging 2016, 11, 967–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhinai, E.A.; Walton, G.E.; Commane, D.M. The Role of the Gut Microbiota in Colorectal Cancer Causation. Int. J. Mol. Sci. 2019, 20, 5295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flemer, B.; Warren, R.D.; Barrett, M.P.; Cisek, K.; Das, A.; Jeffery, I.B.; Hurley, E.; O’Riordain, M.; Shanahan, F.; O’Toole, P.W. The oral microbiota in colorectal cancer is distinctive and predictive. Gut 2017, 67, 1454–1463. [Google Scholar] [CrossRef] [Green Version]
- Flemer, B.; Herlihy, M.; O’Riordain, M.; Shanahan, F.; O’Toole, P.W. Tumour-associated and non-tumour-associated microbiota: Addendum. Gut Microbes 2018, 9, 1–5. [Google Scholar] [CrossRef]
- Flemer, B.; Lynch, D.B.; Brown, J.M.R.; Jeffery, I.B.; Ryan, F.J.; Claesson, M.J.; O’Riordain, M.; Shanahan, F.; O’Toole, P.W. Tumour-associated and non-tumour-associated microbiota in colorectal cancer. Gut 2017, 66, 633–643. [Google Scholar] [CrossRef]
- Gao, Z.; Guo, B.; Gao, R.; Zhu, Q.; Qin, H. Microbiota Disbiosis is Associated with Colorectal Cancer. Front. Microbiol. 2015, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Al-Hassi, H.O.; Ng, O.; Brookes, M. Tumour-associated and non-tumour-associated microbiota in colorectal cancer. Gut 2018, 67, 395. [Google Scholar] [CrossRef] [PubMed]
- Phipps, O.; Al-Hassi, H.; Quraishi, M.; Dickson, E.; Segal, J.; Steed, H.; Kumar, A.; Acheson, A.; Beggs, A.; Brookes, M. Oral and Intravenous Iron Therapy Differentially Alter the On- and Off-Tumor Microbiota in Anemic Colorectal Cancer Patients. Cancers 2021, 13, 1341. [Google Scholar] [CrossRef] [PubMed]
- Phipps, O.; Al-Hassi, H.O.; Quraishi, M.N.; Kumar, A.; Brookes, M.J. Influence of Iron on the Gut Microbiota in Colorectal Cancer. Nutrients 2020, 12, 2512. [Google Scholar] [CrossRef] [PubMed]
- Weersma, R.K.; Zhernakova, A.; Fu, J. Interaction between drugs and the gut microbiome. Gut 2020, 69, 1510–1519. [Google Scholar] [CrossRef]
- Lee, T.; Clavel, T.; Smirnov, K.; Schmidt, A.; Lagkouvardos, I.; Walker, A.; Lucio, M.; Michalke, B.; Schmitt-Kopplin, P.; Fedorak, R.; et al. Oral versus intravenous iron replacement therapy distinctly alters the gut microbiota and metabolome in patients with IBD. Gut 2016, 66, 863–871. [Google Scholar] [CrossRef]
- Keeler, B.D.; Simpson, J.A.; Ng, O.; Padmanabhan, H.; Brookes, M.J.; Acheson, A.G.; Banerjea, A.; Walter, C.; Maxwell-Armstrong, C.; Williams, J.; et al. Randomized clinical trial of preoperative oral versus intravenous iron in anaemic patients with colorectal cancer. J. Br. Surg. 2017, 104, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Earth Microbiome Project. Illumina 16s PCR Protocols. 2020. Available online: https://www.earthmicrobiome.org/protocols-and-standards/16s/ (accessed on 29 June 2020).
- Bolyen, E.; Rideout, J.R.; Dillon, M.R.; Bokulich, N.A.; Abnet, C.C.; Al-Ghalith, G.A.; Alexander, H.; Alm, E.J.; Arumugam, M.; Asnicar, F.; et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. 2019, 37, 852–857. [Google Scholar] [CrossRef]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glöckner, F.O. The SILVA Ribosomal RNA Gene Database Project: Improved Data Processing and Web-Based Tools. Nucleic Acids Res. 2013, 41, D590–D596. [Google Scholar] [CrossRef] [PubMed]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Segata, N.; Izard, J.; Waldron, L.; Gevers, D.; Miropolsky, L.; Garrett, W.S.; Huttenhower, C. Metagenomic biomarker discovery and explanation. Genome Biol. 2011, 12, R60. [Google Scholar] [CrossRef] [Green Version]
- Lyra, A.; Forssten, S.; Rolny, P.; Wettergren, Y.; Lahtinen, S.J.; Salli, K.; Cedgård, L.; Odin, E.; Gustavsson, B.; Ouwehand, A.C. Comparison of Bacterial Quantities in Left and Right Colon Biopsies and Faeces. World J. Gastroenterol. WJG 2012, 18, 4404–4411. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Kato, I. Gut Microbiota, Inflammation and Colorectal Cancer. Genes Dis. 2016, 3, 130–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, A.M.; Jesus, E.C.; Lopes, A.; Aguiar, J.S.; Begnami, M.D.; Rocha, R.M.; Carpinetti, P.A.; Camargo, A.A.; Hoffmann, C.; Freitas, H.C.; et al. Tissue-Associated Bacterial Alterations in Rectal Carcinoma Patients Revealed by 16S rRNA Community Profiling. Front. Cell. Infect. Microbiol. 2016, 6, 179. [Google Scholar] [CrossRef] [Green Version]
- Acher, P.L.; Al-Mishlab, T.; Rahman, M.; Bates, T. Iron-deficiency anaemia and delay in the diagnosis of colorectal cancer. Color. Dis. 2003, 5, 145–148. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Right-Sided Colorectal Cancer (n = 17) | Left-Sided Colorectal Cancer (n = 7) |
|---|---|---|
| Age | 75.3 [7.5] | 74 [7.7] |
| Male | 9 (53%) | 7 (100%) |
| Female | 8 (47%) | 0 (0%) |
| Height, m | 1.67 [0.08] | 1.77 [0.08] |
| Weight, kg | 75.6 [12.8] | 88.5 [24.0] |
| Inclusion Hb, g/L | 97.1 [14.1] | 102.9 [10.0] |
| Recruitment ferritin, μg/L * | 25 [15–55] | 10 [8–49] |
| Recruitment transferrin saturation, % * | 2.6 [2.3–3.6] | 2.8 [2.6–3.3] |
| Duration of iron treatment, days * | 21 [15–35] | 28 [15–43] |
| Tumor Stage | ||
| T ≤ 2 | 1 (6%) | 0 (0%) |
| T3 | 3 (18%) | 5 (71%) |
| T4 | 13 (76%) | 2 (29%) |
| Preoperative Risk Assessment | ||
| ASA fitness status classification | ||
| I–II | 7 (41%) | 2 (29%) |
| III–IV | 10 (59%) | 5 (71%) |
| CR-POSSUM mortality score, % * | 3.5 [2.5–9.3] | 3.5 [2.6–6.6] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phipps, O.; Quraishi, M.N.; Dickson, E.A.; Steed, H.; Kumar, A.; Acheson, A.G.; Beggs, A.D.; Brookes, M.J.; Al-Hassi, H.O. Differences in the On- and Off-Tumor Microbiota between Right- and Left-Sided Colorectal Cancer. Microorganisms 2021, 9, 1108. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9051108
Phipps O, Quraishi MN, Dickson EA, Steed H, Kumar A, Acheson AG, Beggs AD, Brookes MJ, Al-Hassi HO. Differences in the On- and Off-Tumor Microbiota between Right- and Left-Sided Colorectal Cancer. Microorganisms. 2021; 9(5):1108. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9051108
Chicago/Turabian StylePhipps, Oliver, Mohammed N. Quraishi, Edward A. Dickson, Helen Steed, Aditi Kumar, Austin G. Acheson, Andrew D. Beggs, Matthew J. Brookes, and Hafid Omar Al-Hassi. 2021. "Differences in the On- and Off-Tumor Microbiota between Right- and Left-Sided Colorectal Cancer" Microorganisms 9, no. 5: 1108. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9051108