
Helicobacter pylori-Related Metabolic Parameters and Premalignant Gastric Mucosa Histological Lesions in Swiss Bariatric Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Considerations
2.3. Inclusion and Exclusion Criteria
2.4. Data Collection and Extraction
2.5. Statistical Analysis
3. Results
4. Discussion
- (a)
- High-salt diet, a known risk factor for arterial hypertension, which favors Hp colonization [45];
- (b)
- (c)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doulberis, M.; Papaefthymiou, A.; Polyzos, S.A.S.A.; Katsinelos, P.; Grigoriadis, N.; Srivastava, D.S.D.S.; Kountouras, J. Rodent models of obesity. Minerva Endocrinol. 2020, 47, 243–263. [Google Scholar] [CrossRef]
- Doulberis, M.; Polyzos, S.A.; Papaefthymiou, A.; Katsinelos, P.; Kiosses, C.; Kountouras, J. Treatment of nonalcoholic fatty liver disease: From adult trials to perspectives in the management of children and adolescents. Expert Opin. Pharmacother. 2020, 21, 247–251. [Google Scholar] [CrossRef]
- Kountouras, J.; Polyzos, S.A.; Katsinelos, P.; Zeglinas, C.; Artemaki, F.; Tzivras, D.; Vardaka, E.; Gavalas, E.; Romiopoulos, I.; Simeonidou, C.; et al. Cardio-cerebrovascular disease and Helicobacter pylori-related metabolic syndrome: We consider eradication therapy as a potential cardio-cerebrovascular prevention strategy. Int. J. Cardiol. 2017, 229, 17–18. [Google Scholar] [CrossRef]
- Komaei, I.; Currò, G.; Mento, F.; Cassaro, G.; Lazzara, C.; Barbera, A.; Ammendola, M.; Alibrandi, A.; Navarra, G. Gastric Histopathologic Findings in South Italian Morbidly Obese Patients Undergoing Laparoscopic Sleeve Gastrectomy: Is Histopathologic Examination of All Resected Gastric Specimens Necessary? Obes. Surg. 2020, 30, 1339–1346. [Google Scholar] [CrossRef]
- Tay, S.W.; Li, J.W.; Fock, K.M. Diet and cancer of the esophagus and stomach. Curr. Opin. Gastroenterol. 2021, 37, 158–163. [Google Scholar] [CrossRef]
- Doulberis, M.; Papaefthymiou, A.; Polyzos, S.A.; Kotronis, G.; Gialamprinou, D.; Tzitiridou-Chatzopoulou, M.; Touloumtzi, M.; Kountouras, J. Helicobacter pylori, Sleeve Gastrectomy, and Gastroesophageal Reflux Disease: Is There a Relation? Obes. Surg. 2020, 31, 1839–1840. [Google Scholar] [CrossRef]
- Kountouras, J.; Doulberis, M.; Papaefthymiou, A.; Polyzos, S.A.S.A.; Vardaka, E.; Tzivras, D.; Dardiotis, E.; Deretzi, G.; Giartza-Taxidou, E.; Grigoriadis, S.; et al. A perspective on risk factors for esophageal adenocarcinoma: Emphasis on Helicobacter pylori infection. Ann. N. Y. Acad. Sci. 2019, 1452, 12–17. [Google Scholar] [CrossRef]
- Schistosomes, liver flukes and Helicobacter pylori. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Lyon, 7–14 June 1994. IARC Monogr. Eval. Carcinog. Risks Hum. 1994, 61, 1–241.
- Correa, P. Human gastric carcinogenesis: A multistep and multifactorial process--First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention. Cancer Res. 1992, 52, 6735–6740. [Google Scholar]
- Graham, D.Y. The only good Helicobacter pylori is a dead Helicobacter pylori. Lancet 1997, 350, 70–71. [Google Scholar] [CrossRef]
- Asombang, A.W.; Kelly, P. Gastric cancer in Africa: What do we know about incidence and risk factors? Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 69–74. [Google Scholar] [CrossRef]
- Park, Y.H.; Kim, N. Review of Atrophic Gastritis and Intestinal Metaplasia as a Premalignant Lesion of Gastric Cancer. J. Cancer Prev. 2015, 20, 25–40. [Google Scholar] [CrossRef]
- De Vries, A.C.; van Grieken, N.C.T.; Looman, C.W.N.; Casparie, M.K.; de Vries, E.; Meijer, G.A.; Kuipers, E.J. Gastric Cancer Risk in Patients With Premalignant Gastric Lesions: A Nationwide Cohort Study in the Netherlands. Gastroenterology 2008, 134, 945–952. [Google Scholar] [CrossRef]
- Doulberis, M.; Srivastava, S.; Polyzos, S.A.; Kountouras, J.; Papaefthymiou, A.; Klukowska-Rötzler, J.; Blank, A.; Exadaktylos, A.K.; Srivastava, D.S. Active Helicobacter pylori Infection is Independently Associated with Nonalcoholic Steatohepatitis in Morbidly Obese Patients. J. Clin. Med. 2020, 9, 215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doulberis, M.; Papaefthymiou, A.; Srivastava, D.S.; Exadaktylos, A.K.; Katsinelos, P.; Kountouras, J.; Polyzos, S.A. Update on the association between non-alcoholic fatty liver disease and Helicobacter pylori infection. Int. J. Clin. Pract. 2020. [Google Scholar] [CrossRef]
- Doulberis, M.; Kotronis, G.; Gialamprinou, D.; Kountouras, J.; Katsinelos, P. Non-alcoholic fatty liver disease: An update with special focus on the role of gut microbiota. Metabolism 2017, 71, 182–197. [Google Scholar] [CrossRef]
- Dogan, U.; Suren, D.; Oruc, M.T.; Gokay, A.A.; Mayir, B.; Cakir, T.; Aslaner, A.; Oner, O.Z.; Bulbuller, N. Spectrum of gastric histopathologies in morbidly obese Turkish patients undergoing laparoscopic sleeve gastrectomy. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 5430–5436. [Google Scholar] [CrossRef]
- Sabbah, N.A.; Saoud, C.Z.; Deeb, M.; Nasser, S.M. Helicobacter pylori Prevalence in Laparoscopic Sleeve Gastrectomy Specimen. Gastroenterol. Res. Pract. 2020, 2020, 5–9. [Google Scholar] [CrossRef]
- Anand, S.; Kalayarasan, R.; Chandrasekar, S.; Mohan, P.; Pottakkat, B.; Gnanasekaran, S. Is histopathological examination of sleeve gastrectomy specimens necessary in areas endemic for gastric cancer? Natl. Med. J. India 2019, 32, 83–85. [Google Scholar] [CrossRef]
- Saafan, T.; El Ansari, W.; Bashah, M. Compared to What? Is BMI Associated with Histopathological Changes in Laparoscopic Sleeve Gastrectomy Specimens? Obes. Surg. 2019, 29, 2166–2173. [Google Scholar] [CrossRef] [Green Version]
- Ge, L.; Moon, R.C.; Nguyen, H.; de Quadros, L.G.; Teixeira, A.F.; Jawad, M.A. Pathologic findings of the removed stomach during sleeve gastrectomy. Surg. Endosc. 2019, 33, 4003–4007. [Google Scholar] [CrossRef]
- Almazeedi, S.; Al-Sabah, S.; Al-Mulla, A.; Al-Murad, A.; Al-Mossawi, A.; Al-Enezi, K.; Jumaa, T.; Bastaki, W. Gastric histopathologies in patients undergoing laparoscopic sleeve gastrectomies. Obes. Surg. 2013, 23, 314–319. [Google Scholar] [CrossRef]
- Rath-Wolfson, L.; Varona, R.; Bubis, G.; Tatarov, A.; Koren, R.; Ram, E. Gastritis in patients undergoing sleeve gastrectomy. Medicine 2017, 96, e6602. [Google Scholar] [CrossRef]
- Turan, G.; Kocaöz, S. Helicobacter Pylori Infection Prevalence and Histopathologic Findings in Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2019, 29, 3674–3679. [Google Scholar] [CrossRef]
- Canil, A.M.; Iossa, A.; Termine, P.; Caporilli, D.; Petrozza, V.; Silecchia, G. Histopathology Findings in Patients Undergoing Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2018, 28, 1760–1765. [Google Scholar] [CrossRef]
- Rossetti, G.; Moccia, F.; Marra, T.; Buonomo, M.; Pascotto, B.; Pezzullo, A.; Napolitano, V.; Schettino, P.; Avellino, M.; Conzo, G.; et al. Does helicobacter pylori infection have influence on outcome of laparoscopic sleeve gastrectomy for morbid obesity? Int. J. Surg. 2014, 12, S68–S71. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [PubMed] [Green Version]
- Guideline for Good Clinical Practice E6. Available online: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e-6-r2-guideline-good-clinical-practice-step-5_en.pdf (accessed on 25 April 2020).
- Wang, Y.-K.; Kuo, F.-C.; Liu, C.-J.; Wu, M.-C.; Shih, H.-Y.; Wang, S.S.W.; Wu, J.-Y.; Kuo, C.-H.; Huang, Y.-K.; Wu, D.-C. Diagnosis of Helicobacter pylori infection: Current options and developments. World J. Gastroenterol. 2015, 21, 11221–11235. [Google Scholar] [CrossRef] [PubMed]
- Kountouras, J.; Gavalas, E.; Zavos, C.; Stergiopoulos, C.; Chatzopoulos, D.; Kapetanakis, N.; Gisakis, D. Alzheimer’s disease and Helicobacter pylori infection: Defective immune regulation and apoptosis as proposed common links. Med. Hypotheses 2007, 68, 378–388. [Google Scholar] [CrossRef] [PubMed]
- Composition of Macro Geographical (Continental) Regions, Geographical Sub-Regions, and Selected Economic and Other Groupings Web Site. Available online: https://unstats.un.org/unsd/methodology/m49/ (accessed on 15 May 2021).
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2005, 28 (Suppl. 1), S37–S42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Hooi, J.K.Y.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.S.; Wu, J.C.Y.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [Green Version]
- Metzger, J.; Styger, S.; Sieber, C.; Von Fliie, M.; Vogelbach, P.; Harder, F. Prevalence of Helicobacter pylori infection in peptic ulcer perforations. Swiss Med. Wkly. 2001, 131, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Heuberger, F.; Pantoflickova, D.; Gassner, M.; Oneta, C.; Grehn, M.; Blum, A.L.; Dorta, G. Helicobacter pylori infection in Swiss adolescents. Eur. J. Gastroenterol. Hepatol. 2003, 15, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Emile, S.H.; Elshobaky, A.; Elbanna, H.G.; Elkashef, W.; Abdel-Razik, M.A. Helicobacter pylori, Sleeve Gastrectomy, and Gastroesophageal Reflux Disease; Is there a Relation? Obes. Surg. 2020, 30, 3037–3045. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A. Exposure-wide epidemiology: Revisiting Bradford Hill. Stat. Med. 2016, 35, 1749–1762. [Google Scholar] [CrossRef]
- Nasrat, S.A.M.; Nasrat, A.M. An Alternative Approach for the Rising Challenge of Hypertensive Illness via Helicobacter pylori Eradication. Cardiol. Res. 2015, 6, 221–225. [Google Scholar] [CrossRef] [Green Version]
- Migneco, A.; Ojetti, V.; Specchia, L.; Franceschi, F.; Candelli, M.; Mettimano, M.; Montebelli, R.; Savi, L.; Gasbarrini, G. Eradication of Helicobacter pylori infection improves blood pressure values in patients affected by hypertension. Helicobacter 2003, 8, 585–589. [Google Scholar] [CrossRef]
- Wan, Z.; Hu, L.; Hu, M.; Lei, X.; Huang, Y.; Lv, Y. Helicobacter pylori infection and prevalence of high blood pressure among Chinese adults. J. Hum. Hypertens. 2018, 32, 158–164. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.M.; Kim, J.-H.; Baik, S.J.; Chun, J.; Youn, Y.H.; Park, H. Sarcopenia and Sarcopenic Obesity as Novel Risk Factors for Gastric Carcinogenesis: A Health Checkup Cohort Study. Front. Oncol. 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.F.; Kurtz, R.C.; Sun, M.; Karpeh, M.; Yu, G.P.; Gargon, N.; Fein, J.S.; Georgopoulos, S.K.; Harlap, S. Adenocarcinomas of the esophagus and gastric cardia: Medical conditions, tobacco, alcohol, and socioeconomic factors. Cancer Epidemiol. Biomark. Prev. 1996, 5, 761–768. [Google Scholar]
- Li, F.; Du, H.; Li, S.; Liu, J. The Association between Metabolic Syndrome and Gastric Cancer in Chinese. Front. Oncol. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Kato, S.; Tsukamoto, T.; Mizoshita, T.; Tanaka, H.; Kumagai, T.; Ota, H.; Katsuyama, T.; Asaka, M.; Tatematsu, M. High salt diets dose-dependently promote gastric chemical carcinogenesis inHelicobacter pylori-infected Mongolian gerbils associated with a shift in mucin production from glandular to surface mucous cells. Int. J. Cancer 2006, 119, 1558–1566. [Google Scholar] [CrossRef] [PubMed]
- Boziki, M.; Grigoriadis, N.; Doulberis, M.; Papaefthymiou, A.; Polyzos, S.A.; Kountouras, J. Potential impact of Helicobacter pylori-related Galectin-3 on chronic kidney, cardiovascular and brain disorders in decompensated cirrhosis. Dig. Liver Dis. 2020, 52, 121–123. [Google Scholar] [CrossRef]
- Kountouras, J.; Polyzos, S.A.; Katsinelos, P.; Zeglinas, C.; Artemaki, F.; Tzivras, D.; Vardaka, E.; Gavalas, E.; Romiopoulos, I.; Simeonidou, C.; et al. Helicobacter pylori eradication to prevent cardio-cerebrovascular disease: Are current data useful for clinical practice? Int. J. Cardiol. 2017, 233, 92. [Google Scholar] [CrossRef] [PubMed]
- Kountouras, J.; Polyzos, S.A.; Doulberis, M.; Zeglinas, C.; Artemaki, F.; Vardaka, E.; Deretzi, G.; Giartza-Taxidou, E.; Tzivras, D.; Vlachaki, E.; et al. Potential impact of Helicobacter pylori-related metabolic syndrome on upper and lower gastrointestinal tract oncogenesis. Metabolism 2018, 87, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Ferrannini, E.; Buzzigoli, G.; Bonadonna, R.; Giorico, M.A.; Oleggini, M.; Graziadei, L.; Pedrinelli, R.; Brandi, L.; Bevilacqua, S. Insulin Resistance in Essential Hypertension. N. Engl. J. Med. 1987, 317, 350–357. [Google Scholar] [CrossRef]
- Gupta, R.; Alcantara, R.; Popli, T.; Tariq, U.; Sood, A.; Mahajan, S.; Ayele, H.; Rajeswaran, Y.; Vyas, A.V. Firibastat: A Novel Brain Aminopeptidase Inhibitor—A New Era of Antihypertensive therapy. Curr. Probl. Cardiol. 2021, 100859. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.; Bitton-Worms, K.; LeRoith, D. The Link between the Metabolic Syndrome and Cancer. Int. J. Biol. Sci. 2011, 7, 1003–1015. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Kountouras, J.; Zavos, C.; Deretzi, G. The association between Helicobacter pylori infection and insulin resistance: A systematic review. Helicobacter 2011, 16, 79–88. [Google Scholar] [CrossRef]
- Rustgi, V.K.; Li, Y.; Gupta, K.; Minacapelli, C.D.; Bhurwal, A.; Catalano, C.; Elsaid, M.I. Bariatric Surgery Reduces Cancer Risk in Adults With Nonalcoholic Fatty Liver Disease and Severe Obesity. Gastroenterology 2021. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, S.A.; Kountouras, J. Novel Advances in the Association between Helicobacter pylori Infection, Metabolic Syndrome, and Related Morbidity. Helicobacter 2015, 20, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, S.A.; Kountouras, J.; Papatheodorou, A.; Patsiaoura, K.; Katsiki, E.; Zafeiriadou, E.; Zavos, C.; Anastasiadou, K.; Terpos, E. Helicobacter pylori infection in patients with nonalcoholic fatty liver disease. Metabolism 2013, 62, 121–126. [Google Scholar] [CrossRef]
- Chen, L.-W.; Chien, C.-Y.; Yang, K.-J.; Kuo, S.-F.; Chen, C.-H.; Chien, R.-N. Helicobacter pylori Infection Increases Insulin Resistance and Metabolic Syndrome in Residents Younger than 50 Years Old: A Community-Based Study. PLoS ONE 2015, 10, e0128671. [Google Scholar] [CrossRef] [PubMed]
- Polyzos, S.A.; Papaefthymiou, A.; Doulberis, M.; Mavridoglou, G.; Kountouras, J. Helicobacter pylori infection and diabetes mellitus. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 845–846. [Google Scholar] [CrossRef]
- Boachie, J.; Adaikalakoteswari, A.; Samavat, J.; Saravanan, P. Low Vitamin B12 and Lipid Metabolism: Evidence from Pre-Clinical and Clinical Studies. Nutrients 2020, 12, 1925. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Cai, C.; Jin, Q.; Chen, X.; Yu, C. The efficacy of Helicobacter pylori eradication in diabetics and its effect on glycemic control: A systematic review and meta-analysis. Helicobacter 2021, 26. [Google Scholar] [CrossRef]
- Lin, Y.; Ness-Jensen, E.; Hveem, K.; Lagergren, J.; Lu, Y. Metabolic syndrome and esophageal and gastric cancer. Cancer Causes Control 2015, 26, 1825–1834. [Google Scholar] [CrossRef]
- Giovannucci, E.; Harlan, D.M.; Archer, M.C.; Bergenstal, R.M.; Gapstur, S.M.; Habel, L.A.; Pollak, M.; Regensteiner, J.G.; Yee, D. Diabetes and Cancer: A consensus report. Diabetes Care 2010, 33, 1674–1685. [Google Scholar] [CrossRef] [Green Version]
- Ogihara, S.; Yamada, M.; Saito, T.; Shono, M.; Rokutan, K. Insulin potentiates mitogenic effect of epidermal growth factor on cultured guinea pig gastric mucous cells. Am. J. Physiol. Liver Physiol. 1996, 271, G104–G112. [Google Scholar] [CrossRef]
- Makino, T.; Noguchi, Y.; Yoshikawa, T.; Doi, C.; Nomura, K. Circulating interleukin 6 concentrations and insulin resistance in patients with cancer. Br. J. Surg. 2003, 85, 1658–1662. [Google Scholar] [CrossRef] [PubMed]
- Ravindranathan, D.; Master, V.A.; Bilen, M.A. Inflammatory Markers in Cancer Immunotherapy. Biology 2021, 10, 325. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, L.; Alinezhad, F.; Kharazi, U.; Badalzadeh, R. The Association of Type 2 Diabetes and Site-Specific Cancers: Linking Mechanisms. Crit. Rev. Oncog. 2019, 24, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.-J.; Wu, C.-T.; Ou, H.-Y.; Lin, C.-H.; Cheng, H.-C.; Chang, W.-L.; Chen, W.-Y.; Yang, H.-B.; Lu, C.-C.; Sheu, B.-S. Male non-insulin users with type 2 diabetes mellitus are predisposed to gastric corpus-predominant inflammation after H. pylori infection. J. Biomed. Sci. 2017, 24, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dandona, P.; Thusu, K.; Cook, S.; Snyder, B.; Makowski, J.; Armstrong, D.; Nicotera, T. Oxidative damage to DNA in diabetes mellitus. Lancet 1996, 347, 444–445. [Google Scholar] [CrossRef]
- Correa, P.; Piazuelo, M.B. The gastric precancerous cascade. J. Dig. Dis. 2012, 13, 2–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikeda, F.; Doi, Y.; Yonemoto, K.; Ninomiya, T.; Kubo, M.; Shikata, K.; Hata, J.; Tanizaki, Y.; Matsumoto, T.; Iida, M.; et al. Hyperglycemia Increases Risk of Gastric Cancer Posed by Helicobacter pylori Infection: A Population-Based Cohort Study. Gastroenterology 2009, 136, 1234–1241. [Google Scholar] [CrossRef] [PubMed]
- Fox, J.G.; Wang, T.C. Inflammation, atrophy, and gastric cancer. J. Clin. Investig. 2007, 117, 60–69. [Google Scholar] [CrossRef]
- Yang, H.-J.; Kang, D.; Chang, Y.; Ahn, J.; Ryu, S.; Cho, J.; Guallar, E.; Sohn, C., II. Diabetes mellitus is associated with an increased risk of gastric cancer: A cohort study. Gastric Cancer 2020, 23, 382–390. [Google Scholar] [CrossRef]
- Lorenzi, M.; Montisano, D.F.; Toledo, S.; Barrieux, A. High glucose induces DNA damage in cultured human endothelial cells. J. Clin. Investig. 1986, 77, 322–325. [Google Scholar] [CrossRef] [Green Version]
- Yi, H.; Hwang, P.; Yang, D.-H.; Kang, C.-W.; Lee, D.-Y. Expression of the insulin-like growth factors (IGFs) and the IGF-binding proteins (IGFBPs) in human gastric cancer cells. Eur. J. Cancer 2001, 37, 2257–2263. [Google Scholar] [CrossRef]
- Zhuang, S.; Jian, Y.-M.; Sun, Y.-N. Inhibition of N-methyl-N-nitrosourea-induced gastric tumorigenesis by Liuwei Dihuang Pill in db/db mice. World J. Gastroenterol. 2017, 23, 4233. [Google Scholar] [CrossRef] [PubMed]
- Stroh, C.; Weiner, R.; Wolff, S.; Knoll, C.; Manger, T. Influences of Gender on Complication Rate and Outcome after Roux-en-Y Gastric Bypass: Data Analysis of More Than 10,000 Operations from the German Bariatric Surgery Registry. Obes. Surg. 2014, 24, 1625–1633. [Google Scholar] [CrossRef]
- Zizza, C.A.; Herring, A.H.; Stevens, J.; Carey, T.S. Bariatric surgeries in North Carolina, 1990 to 2001: A gender comparison. Obes. Res. 2003, 11, 1519–1525. [Google Scholar] [CrossRef] [Green Version]
- Agah, S.; Khedmat, H.; Ghamar-Chehred, M.E.; Hadi, R.; Aghaei, A. Female gender and Helicobacter pylori infection, the most important predisposition factors in a cohort of gastric cancer: A longitudinal study. Casp. J. Intern. Med. 2016, 7, 136–141. [Google Scholar]
- Seo, K., II; Heo, J.J.; Kim, S.E.; Park, S.J.; Park, M.I.; Moon, W.; Kim, J.H.; Jung, K.; Cho, D.H. Sex differences between Helicobacter pylori infection and cholesterol levels in an adult health checkup program. Helicobacter 2020, 25, 1–8. [Google Scholar] [CrossRef] [PubMed]
- De Martel, C.; Parsonnet, J. Helicobacter pylori infection and gender: A meta-analysis of population-based prevalence surveys. Dig. Dis. Sci. 2006, 51, 2292–2301. [Google Scholar] [CrossRef]
- Saqui-Salces, M.; Rocha-Gutierrez, B.L.; Barrios-Payan, J.A.; Ruiz-Palacios, G.; Camacho-Arroyo, I.; Gamboa-Dominguez, A. Effects of Estradiol and Progesterone on Gastric Mucosal Response to Early Helicobacter pylori Infection in Female Gerbils. Helicobacter 2006, 11, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.; Margalit, I.; Goldberg, E.; Krause, I. Gender as an independent risk factor for the components of metabolic syndrome among individuals within the normal range of body mass index. Metab. Syndr. Relat. Disord. 2018, 16, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.-P.; Hung, H.-F.; Chen, M.-K.; Lai, H.-H.; Hsu, W.-F.; Huang, K.-C.; Yang, K.-C. Helicobacter Pylori Infection is Positively Associated with Metabolic Syndrome in Taiwanese Adults: A Cross-Sectional Study. Helicobacter 2015, 20, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Moshkowitz, M. Gender-associated differences in urea breath test for Helicobacter pylori infection referrals and results among dyspeptic patients. World J. Gastrointest. Pathophysiol. 2012, 3, 80. [Google Scholar] [CrossRef]
- Lindkvist, B.; Almquist, M.; Bjørge, T.; Stocks, T.; Borena, W.; Johansen, D.; Hallmans, G.; Engeland, A.; Nagel, G.; Jonsson, H.; et al. Prospective cohort study of metabolic risk factors and gastric adenocarcinoma risk in the Metabolic Syndrome and Cancer Project (Me-Can). Cancer Causes Control 2013, 24, 107–116. [Google Scholar] [CrossRef]
- Moayyedi; Feltbower; Crocombe; Mason; Atha; Brown; Dowell; Richards; Axon The effectiveness of omeprazole, clarithromycin and tinidazole in eradicating Helicobacter pylori in a community screen and treat programme. Aliment. Pharmacol. Ther. 2000, 14, 719–728. [CrossRef]
- Hashimoto, Y.; Hamaguchi, M.; Obora, A.; Kojima, T.; Fukui, M. Impact of metabolically healthy obesity on the risk of incident gastric cancer: A population-based cohort study. BMC Endocr. Disord. 2020, 20, 11. [Google Scholar] [CrossRef] [Green Version]
- Ansari, S.; Yamaoka, Y. Helicobacter pylori virulence factors exploiting gastric colonization and its pathogenicity. Toxins 2019, 11, 677. [Google Scholar] [CrossRef] [Green Version]
- Chew, Y.; Chung, H.Y.; Lin, P.Y.; Wu, D.C.; Huang, S.K.; Kao, M.C. Outer membrane vesicle production by helicobacter pylori represents an approach for the delivery of virulence factors caga, vaca and urea into human gastric adenocarcinoma (Ags) cells. Int. J. Mol. Sci. 2021, 22, 3942. [Google Scholar] [CrossRef]
- Nejati, S.; Karkhah, A.; Darvish, H.; Validi, M.; Ebarhimpour, S.; Nouri, H.R. Influence of Helicobacter pylori virulence factors CagA and VacA on pathogenesis of gastrointestinal disorders. Microb. Pathog. 2018, 117, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Jamkhande, P.G.; Gattani, S.G.; Farhat, S.A. Helicobacter pylori and cardiovascular complications: A mechanism based review on role of Helicobacter pylori in cardiovascular diseases. Integr. Med. Res. 2016, 5, 244–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Blaser, M.J. Association between gastric helicobacter pylori colonization and glycated hemoglobin levels. J. Infect. Dis. 2012, 205, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Shu, L.; Zheng, P.F.; Zhang, X.Y.; Feng, Y.L. Dietary patterns and Helicobacter pylori infection in a group of Chinese adults ages between 45 and 59 years old: An observational study. Medicine 2019, 98, e14113. [Google Scholar] [CrossRef]
- Xue, K.; Liu, Y.; Iversen, K.N.; Mazidi, M.; Qu, Z.; Dong, C.; Jin, T.; Hallmans, G.; Åman, P.; Johansson, A.; et al. Impact of a Fermented High-Fiber Rye Diet on Helicobacter pylori and Cardio-Metabolic Risk Factors: A Randomized Controlled Trial Among Helicobacter pylori-Positive Chinese Adults. Front. Nutr. 2021, 7, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Meng, G.; Zhang, Q.; Liu, L.; Wu, H.; Shi, H.; Bao, X.; Su, Q.; Gu, Y.; Fang, L.; et al. Dietary Patterns are Associated with Helicobacter Pylori Infection in Chinese Adults: A Cross-Sectional Study. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Parameter | Minimum | Maximum | Mean | SD |
|---|---|---|---|---|
| Age (years) | 24 | 75 | 48.66 | 12.55 |
| BMI (kg/m2) | 30.7 | 76 | 54.10 | 8.68 |
| HOMA-IR | 0.2 | 30 | 5.41 | 4.58 |
| Hba1c (%) | 4.2 | 10.8 | 5.97 | 1.12 |
| Parameter | Value | Number | Percentage | |
| Gender | Female | 77 | 66.4% | |
| Male | 39 | 33.6% | ||
| Origin | South America | 3 | 2.6% | |
| Southern Asia | 1 | 0.9% | ||
| Southern Europe | 12 | 10.3% | ||
| Western Asia | 4 | 3.4% | ||
| Eastern Europe | 6 | 5.2% | ||
| Northern Europe | 3 | 2.6% | ||
| Western Europe | 87 | 75% | ||
| Hp Status | positive | 28 | 24.1% | |
| negative | 88 | 75.9% | ||
| Dyslipidemia | present | 62 | 54.4% | |
| absent | 52 | 45.6% | ||
| Triglycerides | present | 32 | 31.1% | |
| absent | 71 | 68.9% | ||
| (Pre)diabetes | present | 61 | 52.6% | |
| absent | 55 | 47.4% | ||
| Arterial hypertension | present | 58 | 50% | |
| absent | 58 | 50% | ||
| Active smoker | positive | 22 | 20.4% | |
| negative | 86 | 79.6% | ||
| Intestinal metaplasia | present | 17 | 14.7% | |
| absent | 99 | 85.3% | ||
| Gastric atrophy | present | 10 | 8.6% | |
| absent | 106 | 91.4% |
| Variable | OR (95% CI) | p-Value | Description |
|---|---|---|---|
| Gender | 1.13 (0.45;2.72) | 0.788 | Man/women |
| Swiss Nationality | 0.58 (0.24;1.44) | 0.23 | Swiss vs. other Nation |
| Western Europe | 0.45 (0.18; 1.14) | 0.088 | Western EU vs. other |
| Balkans | 1.67 (0.42; 5.79) | 0.436 | Balkans vs. other |
| Dyslipidemia | 1.59 (0.66; 3.96) | 0.308 | Yes/no |
| Age | 1.002 (0.99; 1.008) | 0.509 | Continuous |
| Diabetes | 0.966 (0.995; 1.008) | 0.93 | (Pre)diabetes vs. normal |
| Triglycerides | 1.058 (0.386; 2.735) | 0.908 | High/normal |
| Active smoker | 0.521 (0.114; 1.733) | 0.332 | Yes/no |
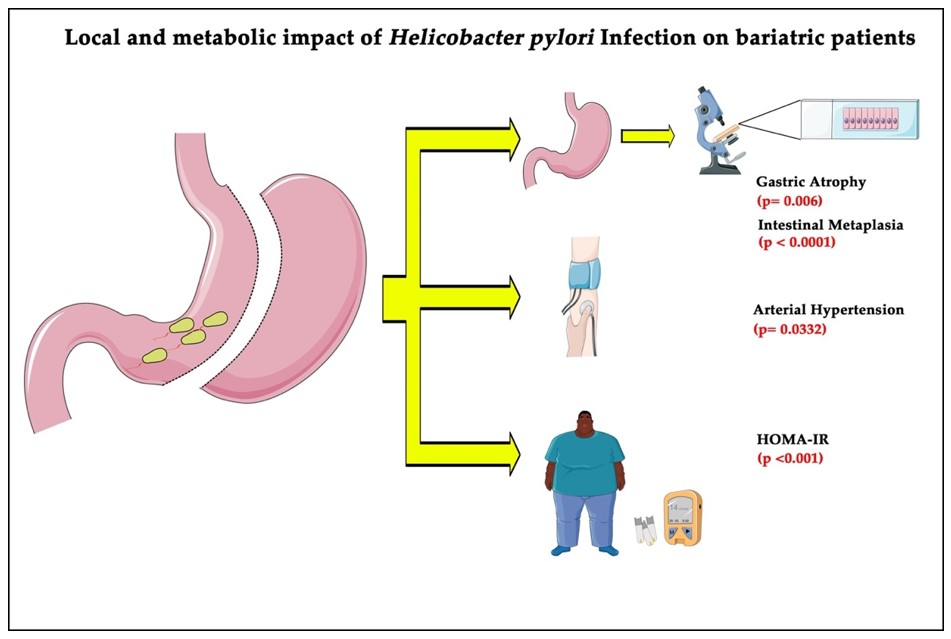
| Arterial hypertension | 2.65 (1.105; 6.766) | 0.0332 * | Yes/no |
| Intestinal metaplasia | 28.3 (8.07; 135.0) | <0.0001 * | Yes/no |
| Gastric atrophy | 17.2 (3.95; 119.9) | <0.001 * | Yes/no |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doulberis, M.; Pierre, N.T.; Manzini, G.; Papaefthymiou, A.; Kountouras, J.; Klukowska-Rötzler, J.; Polyzos, S.A.; Srivastava, S.; Exadaktylos, A.K.; Knuchel, J.; et al. Helicobacter pylori-Related Metabolic Parameters and Premalignant Gastric Mucosa Histological Lesions in Swiss Bariatric Patients. Microorganisms 2021, 9, 1361. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071361
Doulberis M, Pierre NT, Manzini G, Papaefthymiou A, Kountouras J, Klukowska-Rötzler J, Polyzos SA, Srivastava S, Exadaktylos AK, Knuchel J, et al. Helicobacter pylori-Related Metabolic Parameters and Premalignant Gastric Mucosa Histological Lesions in Swiss Bariatric Patients. Microorganisms. 2021; 9(7):1361. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071361
Chicago/Turabian StyleDoulberis, Michael, Noah Thierry Pierre, Giulia Manzini, Apostolis Papaefthymiou, Jannis Kountouras, Jolanta Klukowska-Rötzler, Stergios A. Polyzos, Simone Srivastava, Aristomenis K. Exadaktylos, Jürg Knuchel, and et al. 2021. "Helicobacter pylori-Related Metabolic Parameters and Premalignant Gastric Mucosa Histological Lesions in Swiss Bariatric Patients" Microorganisms 9, no. 7: 1361. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071361