
Development and Clinical Evaluation of Serum and Urine-Based Lateral Flow Tests for Diagnosis of Human Visceral Leishmaniasis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Antigen Preparation
2.3. Preparation and Assembly of the LFA Device
2.4. Principle of the Test
2.5. Result Interpretation
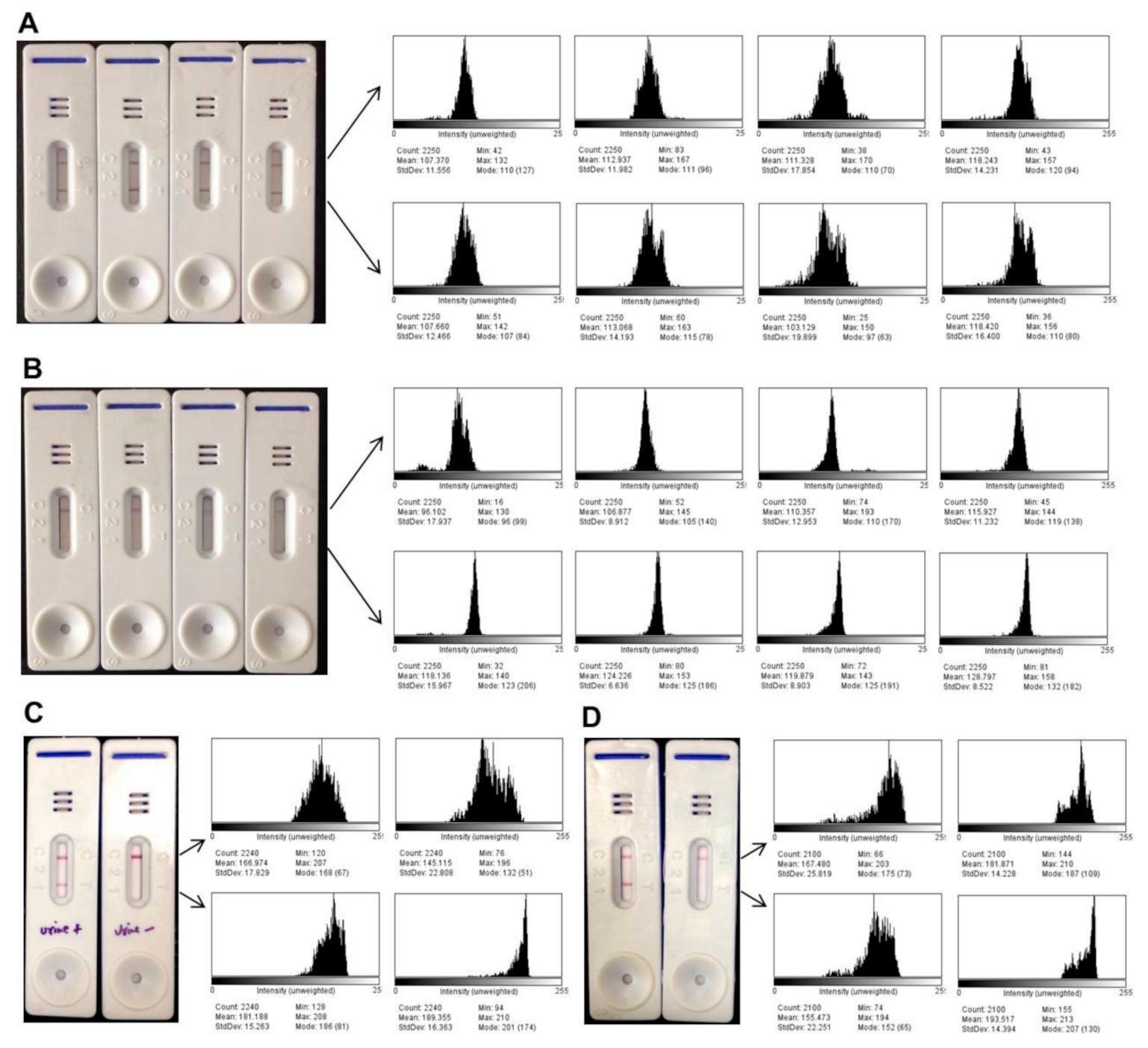
2.6. Quantitative Band Intensity Analysis
3. Results
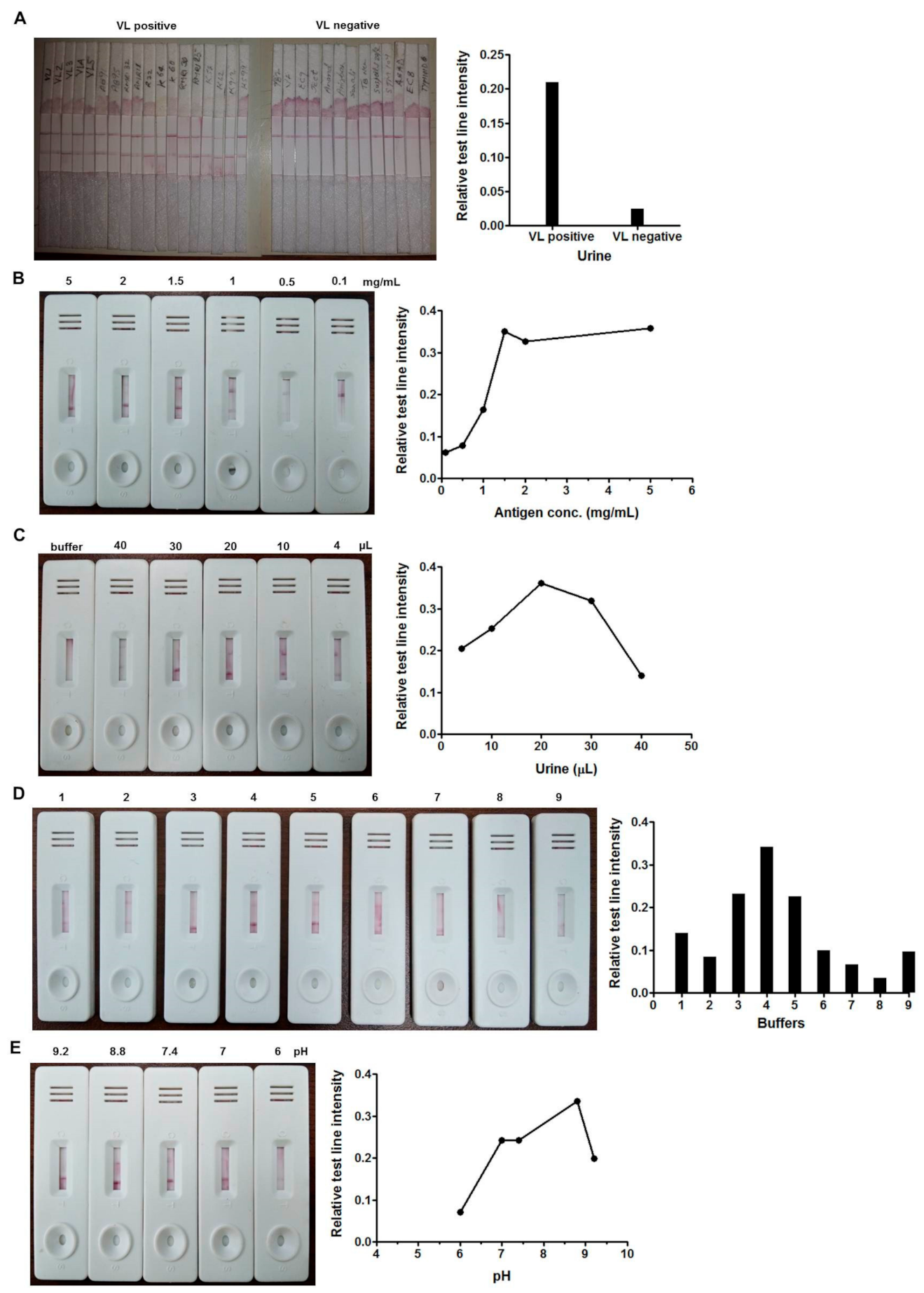
3.1. Optimization of Serum-Based Lateral Flow Assay
3.2. Optimization of Urine-Based Lateral Flow Assay
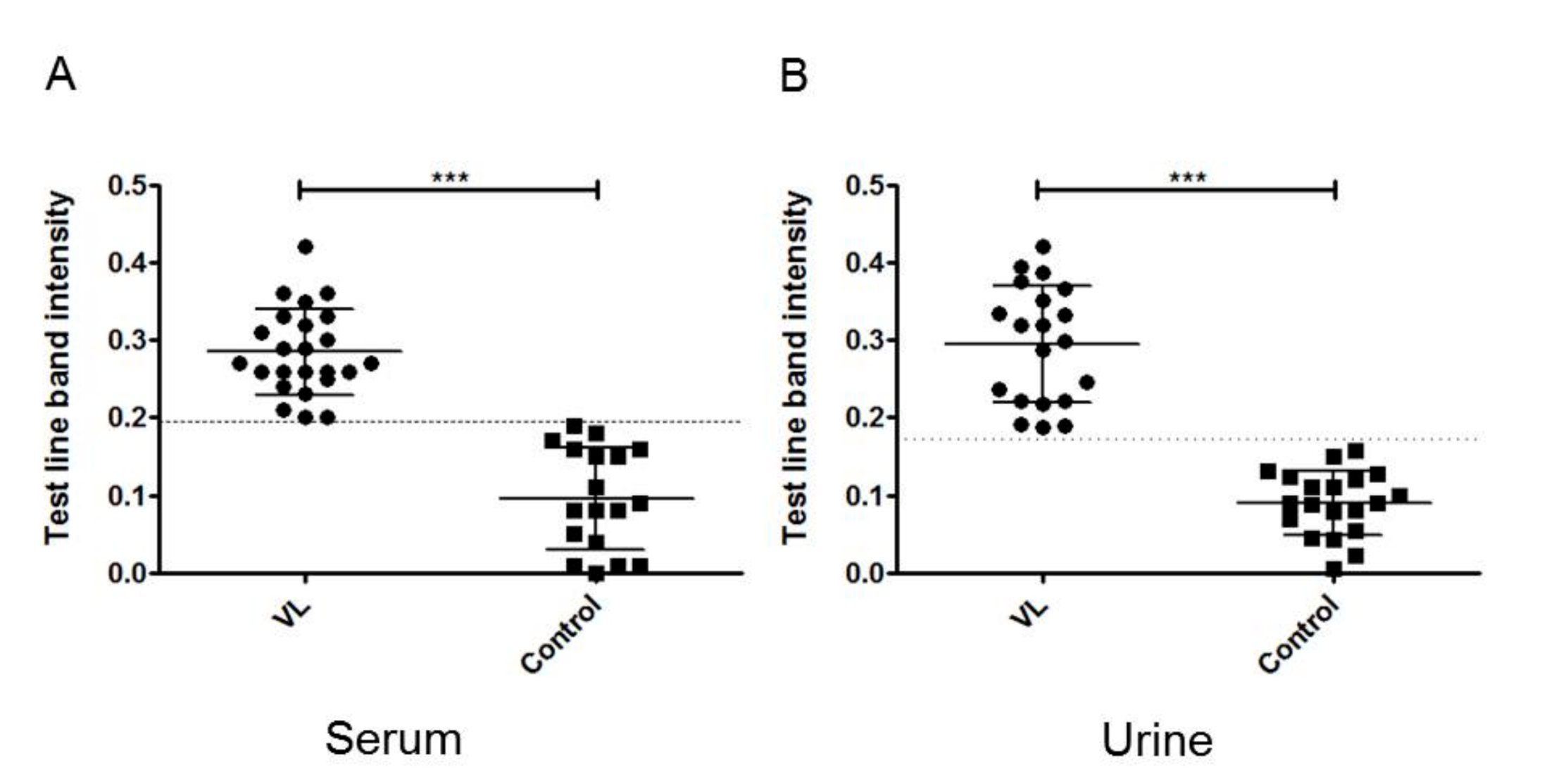
3.3. Performance of LFA with Human Sera
3.4. Performance of LFA with Human Urine Samples
3.5. Quantitative Detection of Band Intensity
3.6. Stability and Reproducibility
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Selvapandiyanid, A.; Croft, S.L.; Rijal, S.; Nakhasiid, H.L.; Ganguly, N.K. Innovations for the elimination and control of visceral leishmaniasis. PLoS Negl. Trop. Dis. 2019, 13, e0007616. [Google Scholar] [CrossRef]
- Zijlstra, E.E. Biomarkers in Post-kala-azar Dermal Leishmaniasis. Front. Cell. Infect. Microbiol. 2019, 9, 228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anfossi, L.; Di Nardo, F.; Profiti, M.; Nogarol, C.; Cavalera, S.; Baggiani, C.; Giovannoli, C.; Spano, G.; Ferroglio, E.; Mignone, W.; et al. A versatile and sensitive lateral flow immunoassay for the rapid diagnosis of visceral leishmaniasis. Anal. Bioanal. Chem. 2018, 410, 4123–4134. [Google Scholar] [CrossRef]
- Ibarra-Meneses, A.V.; Moreno, J.; Carrillo, E. New Strategies and Biomarkers for the Control of Visceral Leishmaniasis. Trends Parasitol. 2020, 36, 29–38. [Google Scholar] [CrossRef]
- Kumar, A.; Pandey, S.C.; Samant, M. A spotlight on the diagnostic methods of a fatal disease Visceral Leishmaniasis. Parasite Immunol. 2020, 42, e12727. [Google Scholar] [CrossRef] [PubMed]
- Kühne, V.; Rezaei, Z.; Pitzinger, P.; Büscher, P. Systematic review on antigens for serodiagnosis of visceral leishmaniasis, with a focus on East Africa. PLoS Negl. Trop. Dis. 2019, 13, e0007658. [Google Scholar] [CrossRef]
- Lévêque, M.F.; Lachaud, L.; Simon, L.; Battery, E.; Marty, P.; Pomares, C. Place of Serology in the Diagnosis of Zoonotic Leishmaniases With a Focus on Visceral Leishmaniasis Due to Leishmania infantum. Front. Cell. Infect. Microbiol. 2020, 10, 67. [Google Scholar] [CrossRef]
- Burza, S.; Croft, S.L.; Boelaert, M. Leishmaniasis. Lancet 2018, 392, 951–970. [Google Scholar] [CrossRef]
- Posthuma-Trumpie, G.A.; Korf, J.; Van Amerongen, A. Lateral flow (immuno)assay: Its strengths, weaknesses, opportunities and threats. A literature survey. Anal. Bioanal. Chem. 2009, 393, 569–582. [Google Scholar] [CrossRef] [Green Version]
- O’Farrell, B. Lateral Flow Immunoassay Systems: Evolution from the Current State of the Art to the Next Generation of Highly Sensitive, Quantitative Rapid Assays. In The Immunoassay Handbook; Elsevier Science: Amsterdam, The Netherlands, 2013; pp. 89–107. ISBN 9780080970370. [Google Scholar]
- Sarkari, B.; Rezaei, Z.; Mohebali, M. Immunodiagnosis of visceral leishmaniasis: Current status and challenges: A review article. Iran. J. Parasitol. 2018, 13, 331–341. [Google Scholar]
- Sundar, S.; Singh, O.P.; Chakravarty, J. Visceral leishmaniasis elimination targets in India, strategies for preventing resurgence. Expert Rev. Anti-Infect. Ther. 2018, 16, 805–812. [Google Scholar] [CrossRef] [PubMed]
- Ejazi, S.A.; Bhattacharya, P.; Bakhteyar, M.A.K.; Mumtaz, A.A.; Pandey, K.; Das, V.N.R.; Das, P.; Rahaman, M.; Goswami, R.P.; Ali, N. Noninvasive Diagnosis of Visceral Leishmaniasis: Development and Evaluation of Two Urine-Based Immunoassays for Detection of Leishmania donovani Infection in India. PLoS Negl. Trop. Dis. 2016, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ejazi, S.A.; Bhattacharyya, A.; Choudhury, S.T.; Ghosh, S.; Sabur, A.; Pandey, K.; Das, V.N.R.; Das, P.; Rahaman, M.; Goswami, R.P.; et al. Immunoproteomic Identification and Characterization of Leishmania Membrane Proteins as Non-Invasive Diagnostic Candidates for Clinical Visceral Leishmaniasis. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Sereno, D.; Akhoundi, M.; Sayehmri, K.; Mirzaei, A.; Holzmuller, P.; Lejon, V.; Waleckx, E. Noninvasive biological samples to detect and diagnose infections due to trypanosomatidae parasites: A systematic review and meta-analysis. Int. J. Mol. Sci. 2020, 21, 1684. [Google Scholar] [CrossRef] [Green Version]
- Manna, L.; Reale, S.; Picillo, E.; Vitale, F.; Gravino, A.E. Urine sampling for real-time polymerase chain reaction-based diagnosis of canine leishmaniasis. J. Vet. Diagn. Investig. 2008, 20, 64–67. [Google Scholar] [CrossRef] [Green Version]
- Abeijon, C.; Campos-Neto, A. Potential Non-invasive Urine-Based Antigen (Protein) Detection Assay to Diagnose Active Visceral Leishmaniasis. PLoS Negl. Trop. Dis. 2013, 7, e2161. [Google Scholar] [CrossRef] [Green Version]
- Vallur, A.C.; Tutterrow, Y.L.; Mohamath, R.; Pattabhi, S.; Hailu, A.; Abdoun, A.O.; Ahmed, A.E.; Mukhtar, M.; Salam, M.A.; Almeida, M.L.; et al. Development and comparative evaluation of two antigen detection tests for Visceral Leishmaniasis. BMC Infect. Dis. 2015, 15, 384. [Google Scholar] [CrossRef] [Green Version]
- Ejazi, S.A.; Ghosh, S.; Saha, S.; Choudhury, S.T.; Bhattacharyya, A.; Chatterjee, M.; Pandey, K.; Das, V.N.R.; Das, P.; Rahaman, M.; et al. A multicentric evaluation of dipstick test for serodiagnosis of visceral leishmaniasis in India, Nepal, Sri Lanka, Brazil, Ethiopia and Spain. Sci. Rep. 2019, 9. [Google Scholar] [CrossRef]
- Saha, S.; Goswami, R.; Pramanik, N.; Guha, S.K.; Saha, B.; Rahman, M.; Mallick, S.; Modak, D.; Silva, F.O.; Mendonca, I.L.; et al. Easy test for visceral leishmaniasis and post-kala-azar dermal leishmaniasis. Emerg. Infect. Dis. 2011, 17, 1304–1306. [Google Scholar] [CrossRef]
- Sivakumar, R.; Dey, A.; Sharma, P.; Singh, S. Expression and characterization of a recombinant kinesin antigen from an old Indian strain (DD8) of Leishmania donovani and comparing it with a commercially available antigen from a newly isolated (KE16) strain of L. donovani. Infect. Genet. Evol. 2008, 8, 313–322. [Google Scholar] [CrossRef]
- Pattabhi, S.; Whittle, J.; Mohamath, R.; El-Safi, S.; Moulton, G.G.; Guderian, J.A.; Colombara, D.; Abdoon, A.O.; Mukhtar, M.M.; Mondal, D.; et al. Design, development and evaluation of rK28-based point-of-care tests for improving rapid diagnosis of visceral leishmaniasis. PLoS Negl. Trop. Dis. 2010, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abass, E.; Bollig, N.; Reinhard, K.; Camara, B.; Mansour, D.; Visekruna, A.; Lohoff, M.; Steinhoff, U. rKLO8, a Novel Leishmania donovani—Derived Recombinant Immunodominant Protein for Sensitive Detection of Visceral Leishmaniasis in Sudan. PLoS Negl. Trop. Dis. 2013, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Griensven, J.; Diro, E. Visceral Leishmaniasis: Recent Advances in Diagnostics and Treatment Regimens. Infect. Dis. Clin. N. Am. 2019, 33, 79–99. [Google Scholar] [CrossRef] [PubMed]
- Ejazi, S.A.; Ghosh, S.; Bhattacharyya, A.; Kamran, M.; Das, S.; Bhowmick, S.; Rahaman, M.; Goswami, R.P.; Ali, N. Investigation of the antigenicity and protective efficacy of Leishmania promastigote membrane antigens in search of potential diagnostic and vaccine candidates against visceral leishmaniasis. Parasites Vectors 2020, 13. [Google Scholar] [CrossRef]
- do Vale, I.N.P.C.; Saliba, J.W.; Fonseca, G.S.F.; Peruhype-Magalhães, V.; de Araújo, F.F.; Pascoal-Xavier, M.A.; Teixeira-Carvalho, A.; Campos, F.M.F.; Andrade, M.C.; Lula, J.F.; et al. Laboratorial algorithm for serological diagnosis of visceral leishmaniasis using rK39-ICT, DAT-LPC and FC-Simplex IgG1. J. Immunol. Methods 2020, 480. [Google Scholar] [CrossRef]
- Sanchez, M.C.A.; Celeste, B.J.; Lindoso, J.A.L.; Fujimori, M.; De Almeida, R.P.; Fortaleza, C.M.C.B.; Druzian, A.F.; Lemos, A.P.F.; De Melo, V.C.A.; Paniago, A.M.M.; et al. Performance of rK39-based immunochromatographic rapid diagnostic test for serodiagnosis of visceral leishmaniasis using whole blood, serum and oral fluid. PLoS ONE 2020, 15. [Google Scholar] [CrossRef]
- Didwania, N.; Ejazi, S.A.; Chhajer, R.; Sabur, A.; Mazumder, S.; Kamran, M.; Kar, R.; Pandey, K.; Das, V.N.R.; Das, P.; et al. Evaluation of cysteine protease c of Leishmania donovani in comparison with glycoprotein 63 and elongation factor 1α for diagnosis of human visceral leishmaniasis and for posttreatment follow-up response. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Country | Sensitivity to Active VL Patients in % (n/N) | Specificity to Non-Endemic Healthy Controls in % (n’/N) | Specificity to Endemic Healthy Controls in % (n’/N) | Specificity to Other Diseases in % (n’/N) | Total Specificity |
|---|---|---|---|---|---|---|
| Serum | India | 96.49 (110/114) | 100 (32/32) | 75 (6/8) | 95 (19/20) | 95 (57/60) |
| Brazil | 88.57 (31/35) | 94.73 (18/19) | - | - | 94.73 (18/19) | |
| Urine | India | 95.12 (39/41) | 100 (25/25) | 100 (12/12) | 88.88 (16/18) | 96.36 (53/55) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ejazi, S.A.; Choudhury, S.T.; Bhattacharyya, A.; Kamran, M.; Pandey, K.; Das, V.N.R.; Das, P.; da Silva, F.O.; Costa, D.L.; Costa, C.H.N.; et al. Development and Clinical Evaluation of Serum and Urine-Based Lateral Flow Tests for Diagnosis of Human Visceral Leishmaniasis. Microorganisms 2021, 9, 1369. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071369
Ejazi SA, Choudhury ST, Bhattacharyya A, Kamran M, Pandey K, Das VNR, Das P, da Silva FO, Costa DL, Costa CHN, et al. Development and Clinical Evaluation of Serum and Urine-Based Lateral Flow Tests for Diagnosis of Human Visceral Leishmaniasis. Microorganisms. 2021; 9(7):1369. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071369
Chicago/Turabian StyleEjazi, Sarfaraz Ahmad, Somsubhra Thakur Choudhury, Anirban Bhattacharyya, Mohd Kamran, Krishna Pandey, Vidya Nand Ravi Das, Pradeep Das, Fernando Oliveira da Silva, Dorcas Lamounier Costa, Carlos Henrique Nery Costa, and et al. 2021. "Development and Clinical Evaluation of Serum and Urine-Based Lateral Flow Tests for Diagnosis of Human Visceral Leishmaniasis" Microorganisms 9, no. 7: 1369. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071369