
Multisystem Inflammatory Syndrome in an Adult (MIS-A) Successfully Treated with Anakinra and Glucocorticoids

 , , ,
, , , {kind=link}
{kind=link}
Abstract
:1. Introduction
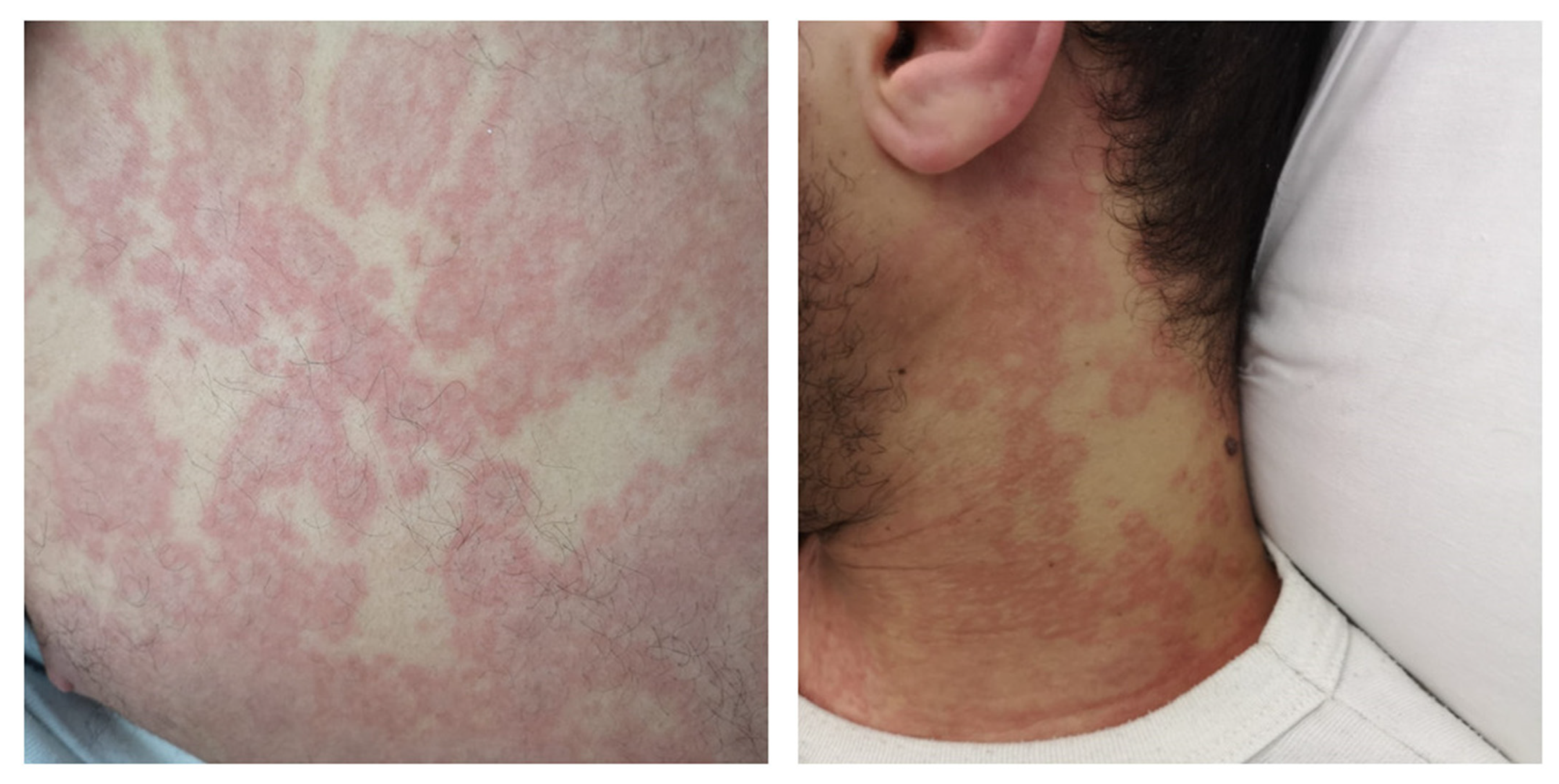
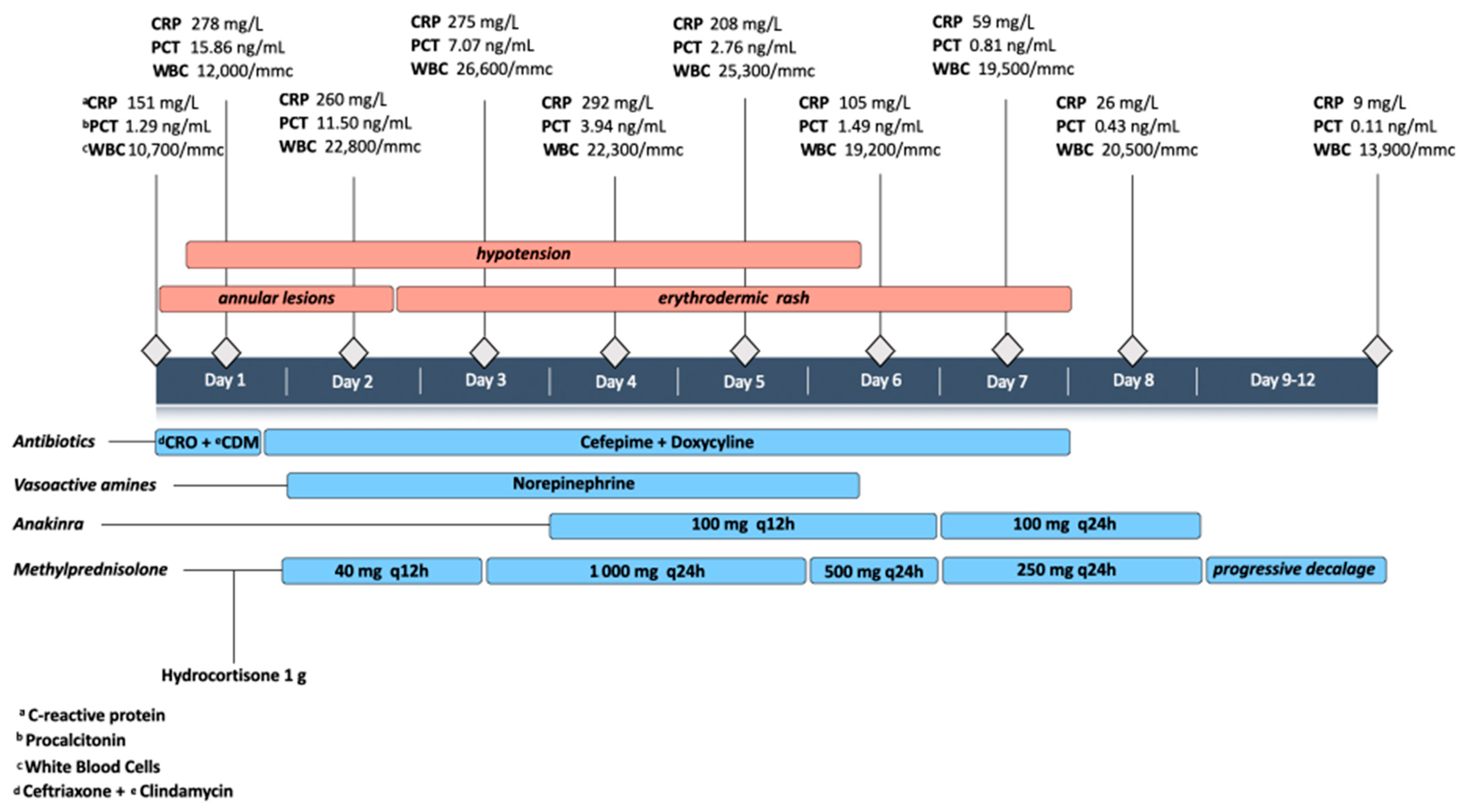
2. Case Presentation
3. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vogel, T.P.; Top, K.A.; Karatzios, C.; Hilmers, D.C.; Tapia, L.I.; Moceri, P.; Giovannini-Chami, L.; Wood, N.; Chandler, R.E.; Klein, N.P.; et al. Multisystem inflammatory syndrome in children and adults (MIS-C/A): Case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 2021, 39, 3037–3049. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.B.; Schwartz, N.G.; Patel, P.; Abbo, L.; Beauchamps, L.; Balan, S.; Lee, E.H.; Paneth-Pollak, R.; Geevarughese, A.; Lash, M.K.; et al. Case Series of Multisystem Inflammatory Syndrome in Adults Associated with SARS-CoV-2 Infection—United Kingdom and United States, March–August 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1450–1456. [Google Scholar] [CrossRef] [PubMed]
- Sokolovsky, S.; Soni, P.; Hoffman, T.; Kahn, P.; Scheers-Masters, J. COVID-19 associated Kawasaki-like multisystem inflammatory disease in an adult. Am. J. Emerg. Med. 2021, 39, 253.e1–253.e2. [Google Scholar] [CrossRef] [PubMed]
- Shaigany, S.; Gnirke, M.; Guttmann, A.; Chong, H.; Meehan, S.; Raabe, V.; Louie, E.; Solitar, B.; Femia, A. An adult with Kawasaki-like multisystem inflammatory syndrome associated with COVID-19. Lancet 2020, 396, e8–e10. [Google Scholar] [CrossRef]
- Kofman, A.D.; Sizemore, E.K.; Detelich, J.F.; Albrecht, B.; Piantadosi, A.L. A young adult with COVID-19 and multisystem inflammatory syndrome in children (MIS-C)-like illness: A case report. BMC Infect. Dis. 2020, 20, 716. [Google Scholar] [CrossRef]
- Moghadam, P.; Blum, L.; Ahouach, B.; Radjou, A.; Lambert, C.; Scanvic, A.; Martres, P.; Decalf, V.; Bégon, E.; Bachmeyer, C. Multisystem Inflammatory Syndrome With Particular Cutaneous Lesions Related to COVID-19 in a Young Adult. Am. J. Med. 2021, 134, e36–e37. [Google Scholar] [CrossRef] [PubMed]
- Hékimian, G.; Kerneis, M.; Zeitouni, M.; Cohen-Aubart, F.; Chommeloux, J.; Bréchot, N.; Mathian, A.; Lebreton, G.; Schmidt, M.; Hié, M.; et al. Coronavirus Disease 2019 Acute Myocarditis and Multisystem Inflammatory Syndrome in Adult Intensive and Cardiac Care Units. Chest 2021, 159, 657–662. [Google Scholar] [CrossRef]
- Weatherhead, J.E.; Clark, E.H.; Vogel, T.P.; Atmar, R.L.; Kulkarni, P.A. Inflammatory syndromes associated with SARS-CoV-2 infection: Dysregulation of the immune response across the age spectrum. J. Clin. Investig. 2020, 130, 6194–6197. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Tang, K.; Levin, M.; Irfan, O.; Morris, S.K.; Wilson, K.; Klein, J.D.; Bhutta, Z.A. COVID-19 and multisystem inflammatory syndrome in children and adolescents. Lancet Infect. Dis. 2020, 20, e276–e288. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, 6529. [Google Scholar] [CrossRef] [PubMed]
- Marot, S.; Malet, I.; Leducq, V.; Zafilaza, K.; Sterlin, D.; Planas, D.; Gothland, A.; Jary, A.; Dorgham, K.; Bruel, T.; et al. Rapid decline of neutralizing antibodies against SARS-CoV-2 among infected healthcare workers. Nat. Commun. 2021, 12, 844. [Google Scholar] [CrossRef] [PubMed]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021, 591, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Aomar-Millán, I.F.; Salvatierra, J.; Torres-Parejo, Ú.; Faro-Miguez, N.; Callejas-Rubio, J.L.; Ceballos-Torres, Á.; Cruces-Moreno, M.T.; Gómez-Jiménez, F.J.; Hernández-Quero, J.; Anguita-Santos, F. Anakinra after treatment with corticosteroids alone or with tocilizumab in patients with severe COVID-19 pneumonia and moderate hyperinflammation. A retrospective cohort study. Intern. Emerg. Med. 2021, 16, 843–852. [Google Scholar] [CrossRef]
- Tharaux, P.-L.; Pialoux, G.; Pavot, A.; Mariette, X.; Hermine, O.; Resche-Rigon, M.; Porcher, R.; Ravaud, P.; Bureau, S.; Dougados, M.; et al. Effect of anakinra versus usual care in adults in hospital with COVID-19 and mild-to-moderate pneumonia (CORIMUNO-ANA-1): A randomised controlled trial. Lancet Respir. Med. 2021, 9, 295–304. [Google Scholar] [CrossRef]
- Kyriazopoulou, E.; Panagopoulos, P.; Metallidis, S.; Dalekos, G.N.; Poulakou, G.; Gatselis, N.; Karakike, E.; Saridaki, M.; Loli, G.; Stefos, A.; et al. An open label trial of anakinra to prevent respiratory failure in COVID-19. eLife 2021, 10, e66125. [Google Scholar] [CrossRef]
- Fouriki, A.; Fougère, Y.; De Camaret, C.; Rohner, G.B.; Grazioli, S.; Wagner, N.; Relly, C.; Schmid, J.P.; Trück, J.; Kottanatu, L.; et al. Case Report: Case Series of Children With Multisystem Inflammatory Syndrome Following SARS-CoV-2 Infection in Switzerland. Front. Pediatr. 2021, 8, 594127. [Google Scholar] [CrossRef]
- Della Paolera, S.; Valencic, E.; Piscianz, E.; Moressa, V.; Tommasini, A.; Sagredini, R.; Kiren, V.; Comar, M.; Taddio, A. Case Report: Use of Anakinra in Multisystem Inflammatory Syndrome During COVID-19 Pandemic. Front. Pediatr. 2020, 8, 624248. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cattaneo, P.; Volpe, A.; Cardellino, C.S.; Riccardi, N.; Bertoli, G.; Ursini, T.; Ustalli, A.; Lodi, G.; Daroui, I.; Angheben, A. Multisystem Inflammatory Syndrome in an Adult (MIS-A) Successfully Treated with Anakinra and Glucocorticoids. Microorganisms 2021, 9, 1393. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071393
Cattaneo P, Volpe A, Cardellino CS, Riccardi N, Bertoli G, Ursini T, Ustalli A, Lodi G, Daroui I, Angheben A. Multisystem Inflammatory Syndrome in an Adult (MIS-A) Successfully Treated with Anakinra and Glucocorticoids. Microorganisms. 2021; 9(7):1393. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071393
Chicago/Turabian StyleCattaneo, Paolo, Alessandro Volpe, Chiara Simona Cardellino, Niccolò Riccardi, Giulia Bertoli, Tamara Ursini, Arjola Ustalli, Giovanni Lodi, Ivan Daroui, and Andrea Angheben. 2021. "Multisystem Inflammatory Syndrome in an Adult (MIS-A) Successfully Treated with Anakinra and Glucocorticoids" Microorganisms 9, no. 7: 1393. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9071393