
Chagas Disease-Related Mortality in Spain, 1997 to 2018

 ,
,  ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Base and Extractionn of Variables
2.2. Statistics Analysis
2.3. Ethical Aspects
3. Results
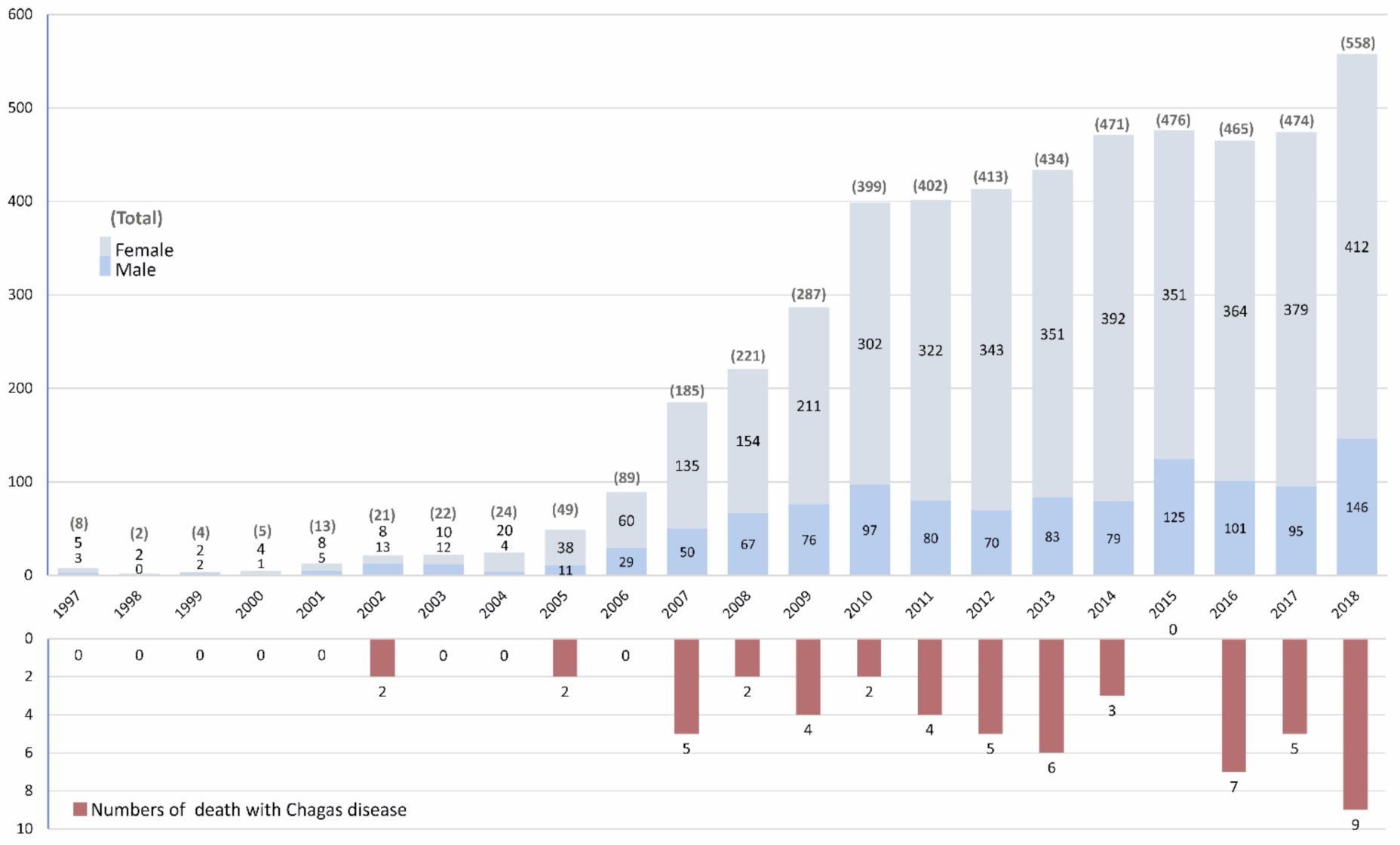
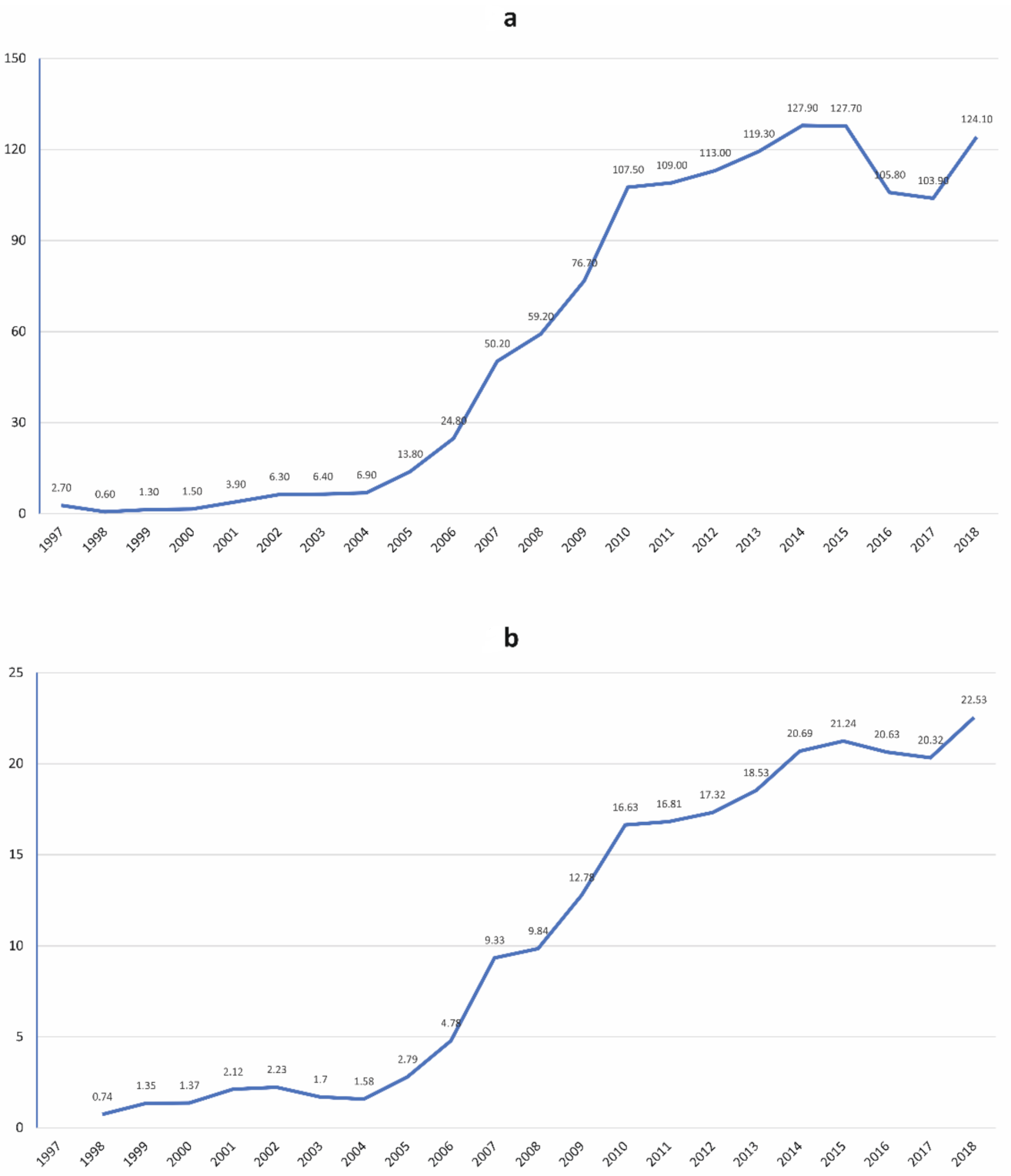
3.1. CD Hospitalization and Incidence Rate
3.2. Fatality and Case Fatality Rate
3.3. Risk Factorrelated with Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Chagas disease. (American trypanosomiasis). In Chagas Disease Fact Sheets; World Health Organization (WHO): Geneva, Switzerland, 2020. [Google Scholar]
- Pérez-Molina, J.A.; Molina, I. Chagas disease. Lancet 2018, 391, 82–94. [Google Scholar] [CrossRef]
- Requena-Méndez, A.; Aldasoro, E.; de Lazzari, E.; Sicuri, E.; Brown, M.; Moore, D.A.J.; Gascon, J.; Muñoz, J. Prevalence of Chagas disease in Latin-American migrants living in Europe: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2015, 9, e0003540. [Google Scholar] [CrossRef] [PubMed]
- Prata, A. Clinical and epidemiological aspects of Chagas disease. Lancet Infect. Dis. 2001, 1, 92–100. [Google Scholar] [CrossRef]
- Cunha-Neto, E.; Chevillard, C. Chagas Disease Cardiomyopathy: Immunopathology and Genetics. Mediat. Inflamm. 2014, 2014, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Bestetti, R.B.; Muccillo, G. Clinical course of Chagas’ heart disease: A comparison with dilated cardiomyopathy. Int. J. Cardiol. 1997, 60, 187–193. [Google Scholar] [CrossRef]
- Sabino, E.C.; Ribeiro, A.; Salemi, V.; Oliveira, C.D.L.; Antunes, A.P.; Menezes, M.M.; Ianni, B.M.; Nastari, L.; Fernandes, F.; Patavino, G.M.; et al. Ten-Year Incidence of Chagas Cardiomyopathy Among Asymptomatic Trypanosoma cruzi—Seropositive Former Blood Donors. Circulation 2013, 127, 1105–1115. [Google Scholar] [CrossRef] [Green Version]
- Carod-Artal, F.J.; Vargas, A.P.; Horan, T.A.; Nunes, L.G.N. Chagasic cardiomyopathy is independently associated with ischemic stroke in Chagas disease. Stroke 2005, 36, 965–970. [Google Scholar] [CrossRef] [Green Version]
- Hotez, P.J.; Alvarado, M.; Basáñez, M.-G.; Bolliger, I.; Bourne, R.; Boussinesq, M.; Brooker, S.J.; Brown, A.S.; Buckle, G.; Budke, C.M.; et al. The global burden of disease study 2010: Interpretation and implications for the neglected tropical diseases. PLoS Negl. Trop. Dis. 2014, 8, e2865. [Google Scholar] [CrossRef] [Green Version]
- Capuani, L.; Bierrenbach, A.L.; Alencar, A.P.; Mendrone, A.; Ferreira, J.E.; Custer, B.; Ribeiro, A.L.P.; Sabino, E.C. Mortality among blood donors seropositive and seronegative for Chagas disease (1996–2000) in São Paulo, Brazil: A death certificate linkage study. PLoS Negl. Trop. Dis. 2017, 11, e0005542. [Google Scholar] [CrossRef] [Green Version]
- Cucunubá, Z.M.; Okuwoga, O.; Basáñez, M.-G.; Nouvellet, P. Increased mortality attributed to Chagas disease: A systematic review and meta-analysis. Parasites Vectors 2016, 9, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Velasco, M.; Gimeno-Feliú, L.A.; Molina, I.; Salas-Coronas, J.; Solà, I.; Monge-Maillo, B.; Torrús-Tendero, D.; Caylà, J.; de Guzmán, E.P.N.; Arellano, J.P.; et al. Screening for Trypanosoma cruzi infection in immigrants and refugees: Systematic review and recommendations from the Spanish Society of Infectious Diseases and Clinical Microbiology. Eurosurveillance 2020, 25, 1900393. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Ayala, A.; Perez-Molina, J.A.; Norman, F.; Navarro, M.; Monge-Maillo, B.; Díaz-Menéndez, M.; Peris-García, J.; Flores-Chavez, M.; Cañavate, C.; López-Vélez, R. Chagas disease in Latin American migrants: A Spanish challenge. Clin. Microbiol. Infect. 2011, 17, 1108–1113. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, J.; Prat, J.G.; Gállego, M.; Gimeno, F.; Treviño, B.; López-Chejade, P.; Ribera, O.; Molina, L.; Sanz, S.; Pinazo, M.J.; et al. Clinical profile of Trypanosoma cruzi infection in a non-endemic setting: Immigration and Chagas disease in Barcelona (Spain). Acta Trop. 2009, 111, 51–55. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Real Decreto 69/2015, de 6 de febrero, por el que se regula el Registro de Actividad de Atención Sanitaria Especializada. Boletín Estado 2015, 35, 1078–1080. Available online: https://www.boe.es/eli/es/rd/2015/02/06/69/con (accessed on 10 August 2021).
- Ministerio de Sanidad y Consumo. Metodología de Análisis de la hospitalización en el Sistema Nacional De Salud. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/docs/metod_modelo_cmbd_pub.pdf (accessed on 10 August 2021).
- Belhassen-García, M.; Alonso-Sardón, M.; Martinez-Perez, A.; Soler, C.; Carranza-Rodriguez, C.; Pérez-Arellano, J.L.; Muro, A.; Salvador, F.; on behalf of The Soil-Transmitted Helminths Study Group of the SEMTSI. Surveillance of strongyloidiasis in Spanish in-patients (1998–2014). PLoS ONE 2017, 12, e0189449. [Google Scholar] [CrossRef] [Green Version]
- Gil-Prieto, R.; Walter, S.; Alvar, J.; Gil De Miguel, A. Epidemiology of Leishmaniasis in Spain Based on Hospitalization Records (1997–2008). Am. J. Trop. Med. Hyg. 2011, 85, 820–825. [Google Scholar] [CrossRef]
- Herrador, Z.; Gherasim, A.; Jiménez, B.C.; Granados, M.D.S.; Martín, J.V.S.; Aparicio, P. Correction: Epidemiological Changes in Leishmaniasis in Spain According to Hospitalization-Based Records, 1997–2011: Raising Awareness towards Leishmaniasis in Non-HIV Patients. PLoS Negl. Trop. Dis. 2016, 10, e0004379. [Google Scholar] [CrossRef]
- Herrador, Z.; Rivas, E.; Gherasim, A.; Gómez-Barroso, D.; García, J.; Benito, A.; Aparicio, P. Using hospital discharge database to characterize chagas disease evolution in Spain: There is a need for a systematic approach towards disease detection and control. PLoS Negl. Trop. Dis. 2015, 9, e0003710. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Salud. Subdirección General de Coordinación Administrativa, Conjunto Mínimo Básico de Datos Hospitales del INSALUD. 2001. Available online: http://www.ingesa.mscbs.gob.es/estadEstudios/documPublica/pdf/CMBD-2001.pdf (accessed on 10 August 2021).
- Olivera, M.J.; Porras-Villamil, J.F.; Villar, J.C.; Herrera, E.V.; Buitrago, G. Chagas disease-related mortality in Colombia from 1979 to 2018: Temporal and spatial trends. Rev. Soc. Bras. Med. Trop. 2021, 54, e07682020. [Google Scholar] [CrossRef]
- Spanish Statistical Institute. Available online: https://www.ine.es/en/index.htm (accessed on 10 August 2021).
- Olivera, M.; Palencia-Sánchez, F.; Riaño-Casallas, M. The Cost of Lost Productivity Due to Premature Chagas Disease-Related Mortality: Lessons from Colombia (2010–2017). Trop. Med. Infect. Dis. 2021, 6, 17. [Google Scholar] [CrossRef]
- Sousa, G.J.B.; Farias, M.S.; Cestari, V.R.F.; Garces, T.S.; Maranhão, T.A.; Moreira, T.M.M.; Silva, L.F.; Sales, J.T.L.; Florêncio, R.S.; Pereira, M.L.D. Spatiotemporal trends of Chagas disease-related mortality in the Northeast of Brazil, 2007–2017. Parasitology 2020, 147, 1552–1558. [Google Scholar] [CrossRef] [PubMed]
- Góes, J.A.P.; Andrade, L.A.; Carvalho, M.S.; Araújo, D.D.C.; Santos, M.B.; Tanajura, D.M.; De Menezes, A.F.; De Araújo, K.C.G.M.; Dos Santos, A.D. Spatial patterns and temporal tendency of mortality related to Chagas disease in an endemic area of northeastern Brazil. Trop. Med. Int. Health 2020, 25, 1298–1305. [Google Scholar] [CrossRef] [PubMed]
- Paola Nieves, S.R. Epidemiología de la enfermedad de Chagas: Alta mortalidad y tasa de incidencia, Región de Coquimbo. Rev. Chil. Infectol. 2020, 37, 402–412. [Google Scholar] [CrossRef]
- Núñez-González, S.; Gault, C.; Simancas-Racines, D. Spatial analysis of dengue, cysticercosis and Chagas disease mortality in Ecuador, 2011–2016. Trans. R. Soc. Trop. Med. Hyg. 2018, 113, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Simões, T.C.; Borges, L.F.; de Assis, A.C.P.; Silva, M.V.; dos Santos, J.; Meira, K.C. Chagas disease mortality in Brazil: A Bayesian analysis of age-period-cohort effects and forecasts for two decades. PLoS Negl. Trop. Dis. 2018, 12, e0006798. [Google Scholar] [CrossRef] [PubMed]
- Moraes, D.N.; Nascimento, B.R.; Beaton, A.Z.; Soliman, E.Z.; Lima-Costa, M.F.; Reis, R.; Ribeiro, A.L.P. Value of the Electrocardiographic (P Wave, T Wave, QRS) Axis as a Predictor of Mortality in 14 Years in a Population with a High Prevalence of Chagas Disease from the Bambuí Cohort Study of Aging. Am. J. Cardiol. 2018, 121, 364–369. [Google Scholar] [CrossRef]
- Gali, W.L.; Sarabanda, A.V.; Baggio, J.M.; Silva, E.F.; Gomes, G.G.; Junqueira, L.F. Predictors of mortality and heart transplantation in patients with Chagas’ cardiomyopathy and ventricular tachycardia treated with implantable cardioverter-defibrillators. Europace 2019, 21, 1070–1078. [Google Scholar] [CrossRef]
- Sherbuk, J.E.; Okamoto, E.E.; Marks, M.A.; Fortuny, E.; Clark, E.H.; Galdos-Cardenas, G.; Vasquez-Villar, A.; Fernandez, A.B.; Crawford, T.C.; Do, R.Q.; et al. Biomarkers and Mortality in Severe Chagas Cardiomyopathy. Glob. Heart 2015, 10, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Nadruz, W.; Gioli-Pereira, L.; Bernardez-Pereira, S.; Marcondes-Braga, F.G.; Fernandes-Silva, M.M.; Silvestre, O.M.; Sposito, A.C.; Ribeiro, A.L.; Bacal, F.; Fernandes, F.; et al. Temporal trends in the contribution of Chagas cardiomyopathy to mortality among patients with heart failure. Heart 2018, 104, 1522–1528. [Google Scholar] [CrossRef]
- Oliveira-Filho, J.; Viana, L.C.; Vieira-De-Melo, R.M.; Faiçal, F.; Torreão, J.A.; Villar, F.A.; Reis, F.J. Chagas disease is an independent risk factor for stroke. Stroke 2005, 36, 2015–2017. [Google Scholar] [CrossRef] [Green Version]
- Montanaro, V.V.A.; Hora, T.F.; da Silva, C.M.; Santos, C.V.D.V.; Lima, M.I.R.; Negrão, E.M.; Ribeiro, D.S.M.; Oliveira, E.M.D.J.; de Freitas, G.R. Mortality and Stroke recurrence in a rehabilitation cohort of patients with cerebral infarcts and Chagas disease. Eur. Neurol. 2018, 79, 177–184. [Google Scholar] [CrossRef]
- Santo, A.H. Tendência da mortalidade relacionada à doença de Chagas, Estado de São Paulo, Brasil, 1985 a 2006: Estudo usando causas múltiplas de morte. Rev. Panam. Salud Pública 2009, 26, 299–309. [Google Scholar] [CrossRef] [Green Version]
- De Almeida, E.A.; Júnior, A.N.R.; Correia, D.; Yasuda, M.S. Co-infection Trypanosoma cruzi/HIV: Systematic review (1980–2010). Rev. Soc. Bras. Med. Trop. 2011, 44, 762–770. [Google Scholar] [CrossRef] [Green Version]
- Martins-Melo, F.R.; Ramos, A.N.; Alencar, C.H.; Heukelbach, J. Mortality related to chagas disease and HIV/AIDS coinfection in Brazil. J. Trop. Med. 2012, 2012, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llenas-García, J.; Hernando, A.; Fiorante, S.; Maseda, D.; Matarranz, M.; Salto, E.; Rubio, R.; Pulido, F. Chagas disease screening among HIV-positive Latin American immigrants: An emerging problem. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 1991–1997. [Google Scholar] [CrossRef]
- Ramos, J.M.; Millá, A.; Rodriguez, J.C.; López-Chejade, P.; Flóres, M.; Rodriguez, J.M.; Gutiérrez, F.; Flores-Chavez, M. Chagas disease in Latin American pregnant immigrants: Experience in a non-endemic country. Arch. Gynecol. Obstet. 2011, 285, 919–923. [Google Scholar] [CrossRef]
- Llenas-García, J.; Wikman-Jorgensen, P.; Gil-Anguita, C.; Sesma, V.R.; Torrús-Tendero, D.; Martínez-Goñi, R.; Romero-Nieto, M.; García-Abellán, J.; Esteban-Giner, M.J.; Antelo, K.; et al. Chagas disease screening in pregnant Latin American women: Adherence to a systematic screening protocol in a non-endemic country. PLOS Negl. Trop. Dis. 2021, 15, e0009281. [Google Scholar] [CrossRef] [PubMed]
- Generalitat Valenciana. Enfermedad de Chagas importada. Protocolo de actuación en la Comunitat Valenciana. Conselleria de Sanitat, Generalitat Valenciana, Valencia, Spain. 2009. Available online: http://publicaciones.san.gva.es/publicaciones/documentos/V-5243-2008.pdf. (accessed on 10 August 2021).
- Programa de prevención y control de la enfermedad de Chagas congénita en, Cataluña, Subdirección General de Vigilancia y Respuesta a Emergencias de Salud Pública. Protocolo de cribado, diagnótico, tratamiento de la Enfermedad de Chagas en mujeresembarazadas latinoamericanas y en sus hijos. Agencia de Salud Pública de Cataluña, Departamento de Salud, Barcelona, Spain. 2018. Available online: https://canalsalut.gencat.cat/web/.content/_A-Z/C/chagas/documents/arxius/protcolcribratgeidiagnostic_cast.pdf (accessed on 10 August 2021).
- Romay-Barja, M.; Iglesias-Rus, L.; Boquete, T.; Benito, A.; Blasco-Hernández, T. Key Chagas disease missing knowledge among at-risk population in Spain affecting diagnosis and treatment. Infect. Dis. Poverty 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Ramos-Sesma, V.; Navarro, M.; Llenas-García, J.; Gil-Anguita, C.; Torrus-Tendero, D.; Wikman-Jorgensen, P.; García-López, M.; Amador-Prous, C.; Ventero-Martín, M.P.; #CorazonesSinChagas Platform; et al. Community-based screening of Chagas disease among Latin American migrants in a non-endemic country: An observational study. Infect. Dis. Poverty 2021, 10, 117. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Year | No. Deaths/No. Cases | % of Total Death | CFR % (95% CI) |
|---|---|---|---|
| 1997 | 0/8 | 0.0 | 0.0 (0–32.4) |
| 1998 | 0/2 | 0.0 | 0.0 (0–65.7) |
| 1999 | 0/4 | 0.0 | 0.0 (0–48.6) |
| 2000 | 0/5 | 0.0 | 0.0 (0–43.6) |
| 2001 | 0/13 | 0.0 | 0.0 (0–22.8) |
| 2002 | 2/21 | 3.6 | 9.5 (2.6–28.9) |
| 2003 | 0/22 | 0.0 | 0.0 (0–14.7) |
| 2004 | 0/24 | 0.0 | 0.0 (0–13.8) |
| 2005 | 2/49 | 3.6 | 4.1 (1.1–13.7) |
| 2006 | 0/89 | 0.0 | 0.0 (0–4.1) |
| 2007 | 5/185 | 8.9 | 2.7 (1.1–6.2) |
| 2008 | 2/221 | 3.6 | 0.9 (0.3–3.0) |
| 2009 | 4/287 | 7.1 | 1.4 (0.5–3.5) |
| 2010 | 2/399 | 3.6 | 0.5 (0.1–1.8) |
| 2011 | 4/402 | 7.1 | 1.0 (0.4–2.5) |
| 2012 | 5/413 | 8.9 | 1.2 (0.5–2.8) |
| 2013 | 6/434 | 10.7 | 1.4 (0.6–2.9) |
| 2014 | 3/471 | 5.4 | 0.6 (0.2–1.8) |
| 2015 | 0/476 | 0.0 | 0.0 (0–0.8) |
| 2016 | 7/465 | 12.5 | 1.5 (0.7–3.1) |
| 2017 | 5/474 | 8.9 | 1.1 (0.5–2.4) |
| 2018 | 9/558 | 16.1 | 1.6 (0.8–3.1) |
| Total | 56/5022 | 100 | 1.1. (0.9–1.5) |
| Age in Years | No. Deaths/ No. Cases | % of Total Deaths | CFR (95% CI) | OR (95% CI) | p-Value |
|---|---|---|---|---|---|
| 0–9 | 2/149 | 3.6 | 1.3 (0.4–4.7) | 1 | - |
| 10–19 | 1/50 | 1.8 | 2.0 (0.4–10.5) | 1.50 (1.13–16.90) | 0.74 |
| 20–29 | 2/699 | 3.6 | 0.3 (0.08–1.0) | 0.21 (0.03–1.50) | 0.12 |
| 30–39 | 7/1888 | 12.5 | 0.4 (0.2–0.8) | 0.27 (0.56–1.32) | 0.11 |
| 40–49 | 8/1086 | 14.3 | 0.7 (0.4–1.5) | 0.54 (0.11–2.59) | 0.45 |
| 50–59 | 12/684 | 21.4 | 1.8 (1.0–3.0) | 1.31 (0.29–5.92) | 0.72 |
| 60–69 | 11/340 | 19.6 | 3.2(1.8–5.7) | 2.45 (0.53–11.22) | 0.25 |
| 70–79 | 7/89 | 12.5 | 7.9 (0.4–15.4) | 6.27 (1.27–30.90) | 0.024 |
| 80–89 | 5/30 | 8.9 | 16.7 (0.7–33.5) | 14.7 (2.70–79.90) | 0.002 |
| 90–100 | 1/7 | 1.8 | 14.3 (2.6–51) | 12.50 (0.98–154.12) | 0.53 |
| Demographic Variables | Total Cases | Non-Obstetrics/Gynecology Cases | |||
|---|---|---|---|---|---|
| Non-Survivors (n = 56) | Survivors (n = 4966) | p-Value | Survivors (n = 2937) | p-Value | |
| Age, median (IQR) | 54.5 (41, 68) | 38 (31,48) | <0.001 | 45 (36, 54) | <0.001 |
| Men, n (%) | 28 (50) | 1121 (22.6) | <0.001 | 1816 (61.8) | 0.071 |
| Comorbidities, n (%) | |||||
| Neoplasms | 11 (19.6) | 169 (3.4) | <0.001 | 152 (5.2) | <0.001 |
| Heart failure | 10 (17.9) | 359 (7.2) | 0.002 | 357 (12.2) | 0.20 |
| Diabetes mellitus | 7 (12.5) | 186 (3.7) | 0.001 | 182 (6.2) | 0.055 |
| Chronic kidney failure | 5 (8.9) | 80 (1.6) | <0.001 | 78 (2.7) | 0.018 |
| HIV infection | 5 (8.9) | 40 (0.8) | <0.001 | 36 (1.2) | <0.001 |
| Chronic lung diseases | 4 (7.1) | 140 (2.8) | 0.054 | 111 (3.8) | 0.20 |
| Ischemic cardiopathy | 4 (7.1) | 165 (3.3) | 0.12 | 161 (5.5) | 0.59 |
| Cerebrovascular diseases | 3 (5.4) | 130 (2.6) | 0.20 | 127 (4.3) | 0.71 |
| Lymphoma/leukemia | 3 (5.4) | 52 (1.0) | 0.023 | 52 (1.8) | 0.082 |
| Hospital admission, n (%) | |||||
| Obstetrics/gynecology Wards | 0 (0) | 2029 (40.9) | <0.001 | - | - |
| Medical wards | 48 (85.7) | 1758 (35.4) | <0.001 | 1758 (59.8) | <0.001 |
| Surgical wards | 4 (7.1) | 744 (15) | 0.10 | 744 (25.3) | 0.002 |
| Pediatric wards | 2 (3.6) | 140 (2.8) | 0.67 | 140 (4.8) | 0.67 |
| Days of admission, median (IQR) | 10 (3.25, 23.5) | 3 (2.0. 7.0) | <0.001 | 5 (2.0.10–0) | <0.001 |
| Readmission, n (%) a | 47 (11.4) | 298 (8.5) | 0.54 | 234 (11.8) | 0.95 |
| Country of birth, n (%) b | |||||
| Bolivia | 9 (50) | 705 (59.0) | 0.69 | 431 (58.2) | 0.49 |
| Spain | 3(16) | 368 (30.8) | 0.20 | 225 (30.4) | 0.21 |
| Ecuador | 1 (5.6) | 22 (1.8) | 0.25 | 19 (2.6) | 0.43 |
| Paraguay | 0 (0) | 28 (0.6) | 1.00 | 16 (2.2) | 1 |
| Argentina | 0 (0) | 21 (0.4) | 0.57 | 18 (2.4) | 1 |
| Colombia | 1 (5.6) | 12 (1.0) | 0.18 | 8 (1.1) | 0.20 |
| Venezuela | 0 (0) | 10 (0.8) | 1.00 | 7 (0.9) | 1 |
| El Salvador | 0 (0) | 9 (0.8) | 1.00 | 5 (0.5) | 1 |
| Brazil | 1 (1.8) | 6 (0.1) | 1.00 | 6 (0.8) | 0.16 |
| Chile | 0 (0) | 4 (0.3) | 1.00 | 3 (0.4) | 1 |
| Type of diagnostic, n (%) | |||||
| CD without organ involvement | 20 (35.7) | 2834 (57.1) | 0.001 | 1368 (46.6) | 0.11 |
| CD with heart involvement | 28 (50) | 1483 (29.9) | <0.001 | 1211 (41.2) | 0.19 |
| CD with organ involvement | 10 (17.9) | 619 (12.5) | 0.23 | 366 (12.5) | 0.29 |
| Trypanosomiasis non-specified | 4 (7.1) | 498 (10) | 0.47 | 221 (7.5) | 0.92 |
| Variables | Total Cases | Non-Obstetrics/Gynecology Cases | ||||
|---|---|---|---|---|---|---|
| Crude OR (95% CI) | Adjusted OR (95% CI) | p-Value | Crude OR (95% CIs) | Adjusted OR (95% CI) | p-Value | |
| Age | 1.06 (1.04, 1.08) | 1.05 (1.03, 1.07) | <0.001 | 1.04 (1.02, 1.06) | 1.04 (1.02, 1.23) | <0.001 |
| Sex, male | 3.42 (2.20, 5.81) | 1.79 (1.03, 3.14) | 0.039 | 1.96 (0.95, 1.48) | 1.40 (0.82, 2.41) | 0.22 |
| Neoplasms | 6.97 (3.56, 13.65) | 4.89 (2.13, 11.24) | <0.001 | 4.47 (2.27, 8.83) | 4.46 (1.97, 10.1) | <0.001 |
| Heart failure | 2.79 (1.39, 5.57) | 1.45 (0.67, 3.16) | 0.34 | 1.57 (0.78, 3.71) | 1.30 (0.81, 2.79) | 0.69 |
| Diabetes mellitus | 3.67 (1.64, 8.21) | 1.21 (0.48, 3.00) | 0.68 | 2.16 (0.96, 4.84) | 1.19 (0.49, 2.93) | 0.69 |
| Chronic kidney failure | 5.98 (2.32, 15.40) | 2.25 (0.80, 6.34) | 0.12 | 3.59 (1.39, 9.25) | 2.14 (0.77, 5.95) | 0.15 |
| HIV infection | 12.07 (4.57, 31.84) | 14.10 (4.88, 40.73) | <0.001 | 7.90 (2.97, 20.95) | 10.46 (3.65, 30.0) | <0.001 |
| Lymphoma/leukemia | 5.34 (1.61, 17.68) | 0.92 (0.21, 3.94) | 0.92 | 3.14 (0.95, 10.3) | 0.78 (0.18, 3.32) | 0.73 |
| CD with heart involvement | 2.39 (1.39, 3.98) | 1.57 (0.85, 3.91) | 0.15 | 1.42 (0.84, 2.14) | 0.94 (0.41, 2.15) | 0.89 |
| CD without organ involvement | 0.41 (0.24, 0.72) | 0.55 (0.26, 1.17) | 0.13 | 0.63 (0.36, 1.10) | 0.73 (0.31, 1.68) | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos-Rincon, J.-M.; Llenas-García, J.; Pinargote-Celorio, H.; Sánchez-García, V.; Wikman-Jorgensen, P.; Navarro, M.; Gil-Anguita, C.; Ramos-Sesma, V.; Torrus-Tendero, D. Chagas Disease-Related Mortality in Spain, 1997 to 2018. Microorganisms 2021, 9, 1991. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9091991
Ramos-Rincon J-M, Llenas-García J, Pinargote-Celorio H, Sánchez-García V, Wikman-Jorgensen P, Navarro M, Gil-Anguita C, Ramos-Sesma V, Torrus-Tendero D. Chagas Disease-Related Mortality in Spain, 1997 to 2018. Microorganisms. 2021; 9(9):1991. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9091991
Chicago/Turabian StyleRamos-Rincon, Jose-Manuel, Jara Llenas-García, Hector Pinargote-Celorio, Veronica Sánchez-García, Philip Wikman-Jorgensen, Miriam Navarro, Concepción Gil-Anguita, Violeta Ramos-Sesma, and Diego Torrus-Tendero. 2021. "Chagas Disease-Related Mortality in Spain, 1997 to 2018" Microorganisms 9, no. 9: 1991. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9091991