
A Mouse Model for Studying Post-Acute Arthritis of Chikungunya

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Biosafety
2.3. Virus
2.4. Animal Studies
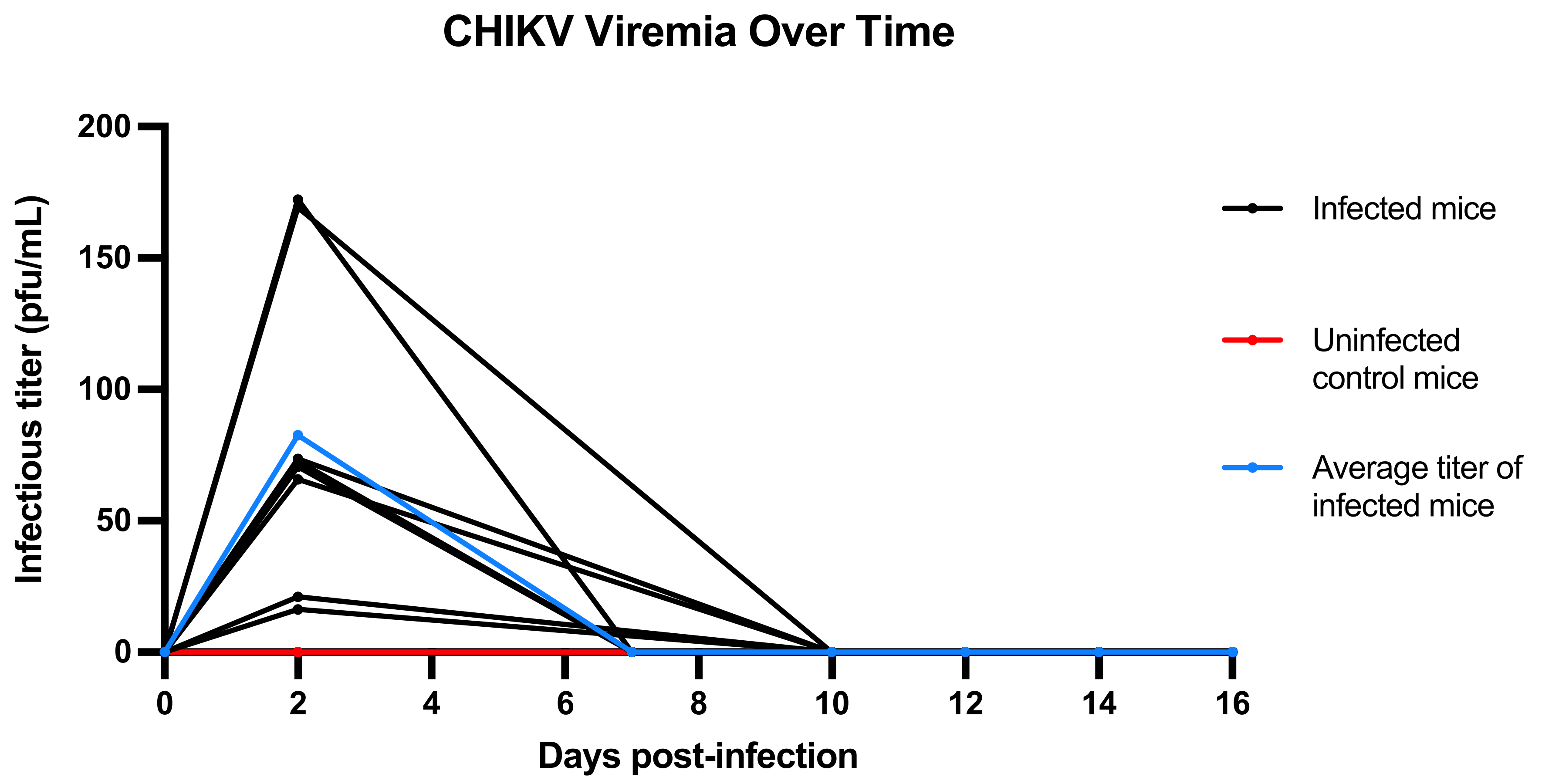
2.5. Viremia Measurement
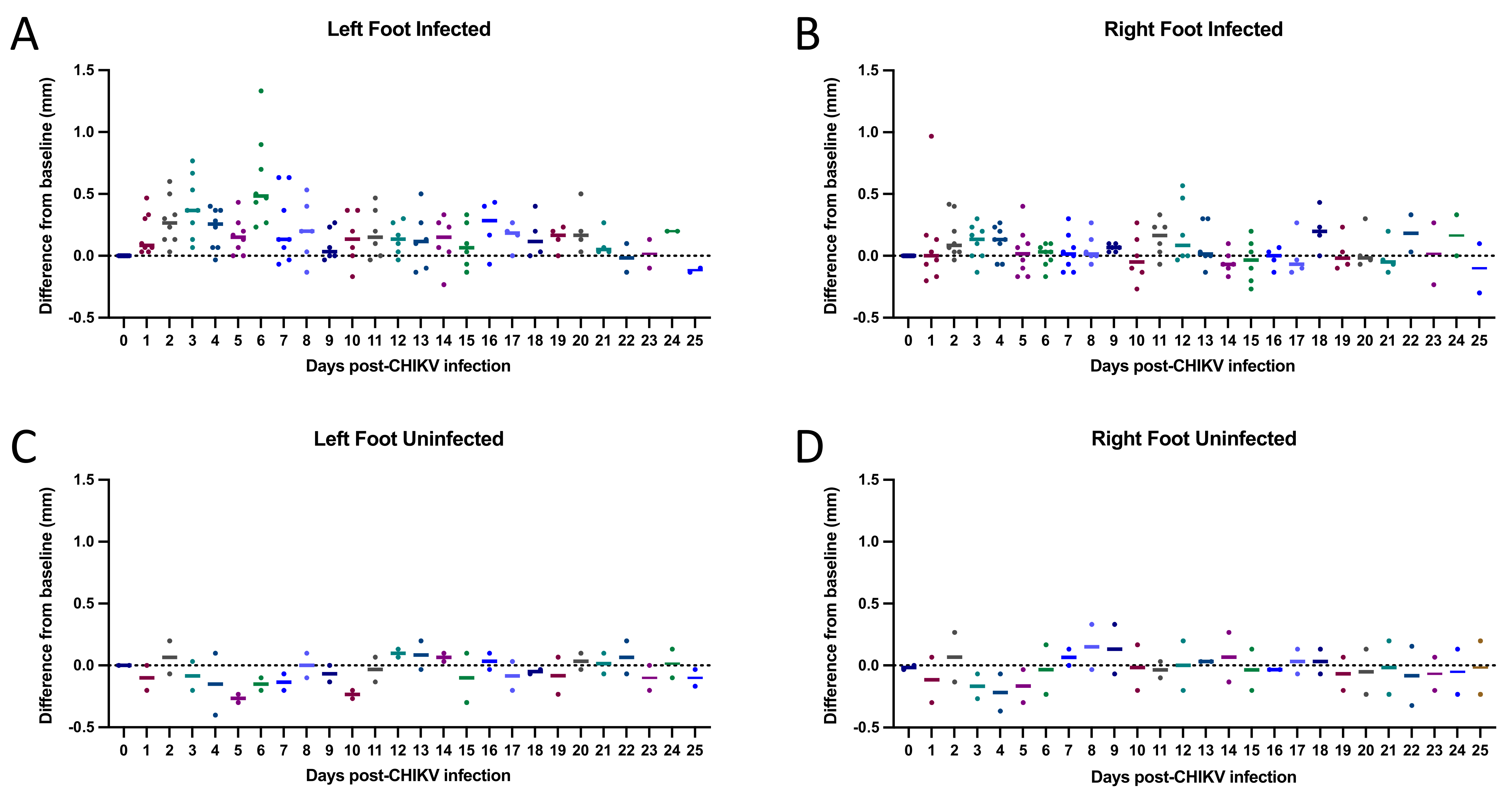
2.6. Tarsal Joint Measurement
2.7. Histology
2.8. Histologic Inflammation Scoring System
3. Results
3.1. CHIKV SAH2123 Reliably Causes Infection in Adult C57BL/6J Mice at 48 h Post Infection
3.2. Viremia Resolves by 10–16 DPI
3.3. CHIKV SAH2123 Inoculation Results in Ipsilateral Tarsal Joint Swelling for 10 Days
3.4. Histologic Findings: CHIKV SAH2123 Infection Results in Histologic Evidence of Arthritis, Synovitis, Periostitis and Myositis That Persist to 21 DPI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Chikungunya disease: Gaps and opportunities in public health and research in the Americas. Wkly. Epidemiol. Rec. 2016, 90, 571–576. [Google Scholar]
- Pan American Health Organization. Chikungunya: Data, Maps and Statistics. Available online: https://www.paho.org/hq/dmdocuments/2015/2015-may-15-cha-CHIKV-cumulative-cases.pdf (accessed on 16 September 2021).
- Chang, A.Y.; Encinales, L.; Porras, A.; Pacheco, N.; Reid, S.P.; Martins, K.A.O.; Pacheco, S.; Bravo, E.; Navarno, M.; Mendoza, A.R.; et al. Frequency of Chronic Joint Pain Following Chikungunya Virus Infection. Arthritis Rheumatol. 2018, 70, 578–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnamoorthy, K.; Harichandrakumar, K.T.; Krishna Kumari, A.; Das, L.K. Burden of chikungunya in India: Estimates of disability adjusted life years (DALY) lost in 2006 epidemic. J. Vector Borne Dis. 2009, 46, 26–35. [Google Scholar] [PubMed]
- Gopalan, S.S.; Das, A. Household economic impact of an emerging disease in terms of catastrophic out-of-pocket health care expenditure and loss of productivity: Investigation of an outbreak of chikungunya in Orissa, India. J. Vector Borne Dis. 2009, 46, 57–64. [Google Scholar] [PubMed]
- Olivia, L.W.; Obanda, V.; Bucht, G.; Mosomtai, G.; Otieno, V.; Ahlm, C.; Evander, M. Global emergence of Alphaviruses that cause arthritis in humans. Infect. Ecol. Epidemiol. 2015, 5, 29853. [Google Scholar]
- Couderc, T.; Chretien, F.; Schilte, C.; Disson, O.; Brigitte, M.; Guivel-Benhassine, F.; Touret, Y.; Barau, G.; Cayet, N.; Schuffenecker, I.; et al. A Mouse Model for Chikungunya: Young Age and Inefficient Type-I Interferon Signaling Are Risk Factors for Severe Disease. PLoS Pathog. 2008, 4, e29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardner, J.; Anraku, I.; Le, T.T.; Larcher, T.; Major, L.; Roques, P.; Schroder, W.A.; Higgs, S.; Suhrbier, A. Chikungunya virus arthritis in adult wild-type mice. J. Virol. 2010, 84, 8021–8032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goupil, B.A.; McNulty, M.A.; Martin, M.J.; McCracken, M.K.; Christofferson, R.C.; Mores, C.N. Novel Lesions of Bones and Joints Associated with Chikungunya Virus Infection in Two Mouse Models of Disease: New Insights into Disease Pathogenesis. PLoS ONE 2016, 11, e0155243. [Google Scholar] [CrossRef] [PubMed]
- Morrison, T.E.; Oko, L.; Montgomery, S.A.; Whitmore, A.C.; Lotstein, A.R.; Gunn, B.M.; Elmore, S.A.; Heise, M.T. A mouse model of chikungunya virus-induced musculoskeletal inflammatory disease: Evidence of arthritis, tenosynovitis, myositis, and persistence. Am. J. Pathol. 2011, 178, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Miner, J.J.; Cook, L.E.; Hong, J.P.; Smith, A.M.; Richner, J.M.; Shimak, R.M.; Young, A.R.; Monte, K.; Poddar, S.; Crowe, J.E.; et al. Therapy with CTLA4-Ig and an antiviral monoclonal antibody controls chikungunya virus arthritis. Sci. Transl. Med. 2017, 9, eaah3438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.W.L.; Teo, T.-H.; Her, Z.; Lum, F.-M.; Kam, Y.-W.; Haase, D.; Rénia, L.; Rötzschke, O.; Ng, L.F.P.; Dermody, T.S. Expanding Regulatory T Cells Alleviates Chikungunya Virus-Induced Pathology in Mice. J. Virol. 2015, 89, 7893–7904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, W.W.L.; Teo, T.-H.; Lum, F.-M.; Aappan, A.K.; Amrun, S.N.; Rénia, L.; Rötzschke, O.; Ng, L.F.P. Virus infection drives IL-2 antibody complexes into pro-inflammatory agonists in mice. Sci. Rep. 2016, 6, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegler, S.A.; Lu, L.; da Rosa, A.P.A.T.; Xiao, S.-Y.; Tesh, R.B. An animal model for studying the pathogenesis of chikungunya virus infection. Am. J. Trop. Med. Hyg. 2008, 79, 133–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langsjoen, R.M.; Haller, S.L.; Roy, C.J.; Vinet-Oliphant, H.; Bergren, N.A.; Erasmus, J.H.; Livengood, J.A.; Powell, T.D.; Weaver, S.C.; Rossi, S.L. Chikungunya Virus Strains Show Lineage-Specific Variations in Virulence and Cross-Protective Ability in Murine and Nonhuman Primate Models. mBio 2018, 9, e02449-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosco-Lauth, A.M.; Han, S.; Hartwig, A.; Bowen, R.A. Development of a Hamster Model for Chikungunya Virus Infection and Pathogenesis. PLoS ONE 2015, 10, e0130150. [Google Scholar]
- Naveca, F.G.; Claro, I.; Giovanetti, M.; de Jesus, J.G.; Xavier, J.; Iani, F.C.M.; do Nascimento, V.A.; de Souza, V.C.; Silveira, P.P.; Lourenço, J.; et al. Genomic, epidemiological and digital surveillance of Chikungunya virus in the Brazilian Amazon. PLoS Negl. Trop Dis. 2019, 13, e0007065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gargan, T.P.; Bailey, C.L.; Higbee, G.A.; Gad, A.; El Said, S. The Effect of Laboratory Colonization on the Vector-Pathogen Interactions of Egyptian Culex pipiens and Rift Valley Fever Virus. Am. J. Trop. Med. Hyg. 1983, 32, 1154–1163. [Google Scholar] [CrossRef] [PubMed]
- Pesko, K.; Westbrook, C.J.; Mores, C.N.; Lounibos, P.L.; Reiskind, M.H. Effects of Infectious Virus Dose and Bloodmeal Delivery Method on Susceptibility of Aedes aegypti and Aedes albopictus to Chikungunya Virus. J. Med. Entomol. 2009, 46, 395–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miner, J.J.; Aw Yeang, H.X.; Fox, J.M.; Taffner, S.; Malkova, O.N.; Oh, S.T.; Kim, A.H.J.; Diamond, M.S.; Lenschow, D.J.; Yokoyama, W.M. Brief Report: Chikungunya Viral Arthritis in the United States: A Mimic of Seronegative Rheumatoid Arthritis. Arthritis Rheumatol. 2015, 67, 1214–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 7 DPI | 15 DPI | 21 DPI | 25 DPI | |||||
|---|---|---|---|---|---|---|---|---|
| Chikungunya inoculated Mice (n = 8) | 10 | 10 | 5 | 5 | 5 | 4 | 0 | 6 |
| Non-inoculated Controls (n = 2) | 2 | 0 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, A.Y.; Tritsch, S.R.; Porzucek, A.J.; Schwartz, A.M.; Seyler-Schmidt, M.; Glass, A.; Latham, P.S.; Reid, S.P.; Simon, G.L.; Mores, C.N. A Mouse Model for Studying Post-Acute Arthritis of Chikungunya. Microorganisms 2021, 9, 1998. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9091998
Chang AY, Tritsch SR, Porzucek AJ, Schwartz AM, Seyler-Schmidt M, Glass A, Latham PS, Reid SP, Simon GL, Mores CN. A Mouse Model for Studying Post-Acute Arthritis of Chikungunya. Microorganisms. 2021; 9(9):1998. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9091998
Chicago/Turabian StyleChang, Aileen Y., Sarah R. Tritsch, Abigail J. Porzucek, Arnold M. Schwartz, Margaux Seyler-Schmidt, Arielle Glass, Patricia S. Latham, St. Patrick Reid, Gary L. Simon, and Christopher N. Mores. 2021. "A Mouse Model for Studying Post-Acute Arthritis of Chikungunya" Microorganisms 9, no. 9: 1998. https://0-doi-org.brum.beds.ac.uk/10.3390/microorganisms9091998