
Post-Mortem Computed Tomography Pulmonary Findings in Harbor Porpoises (Phocoena phocoena)

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Evaluation
2.3. Carcass Condition
2.4. Tracheobronchial Changes
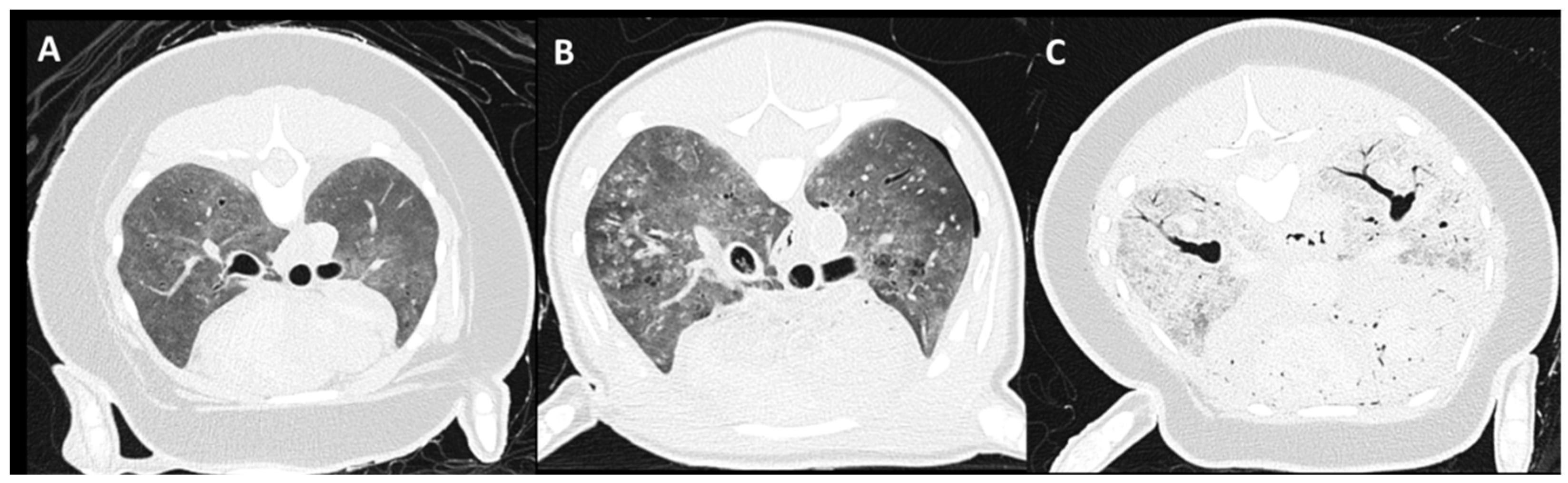
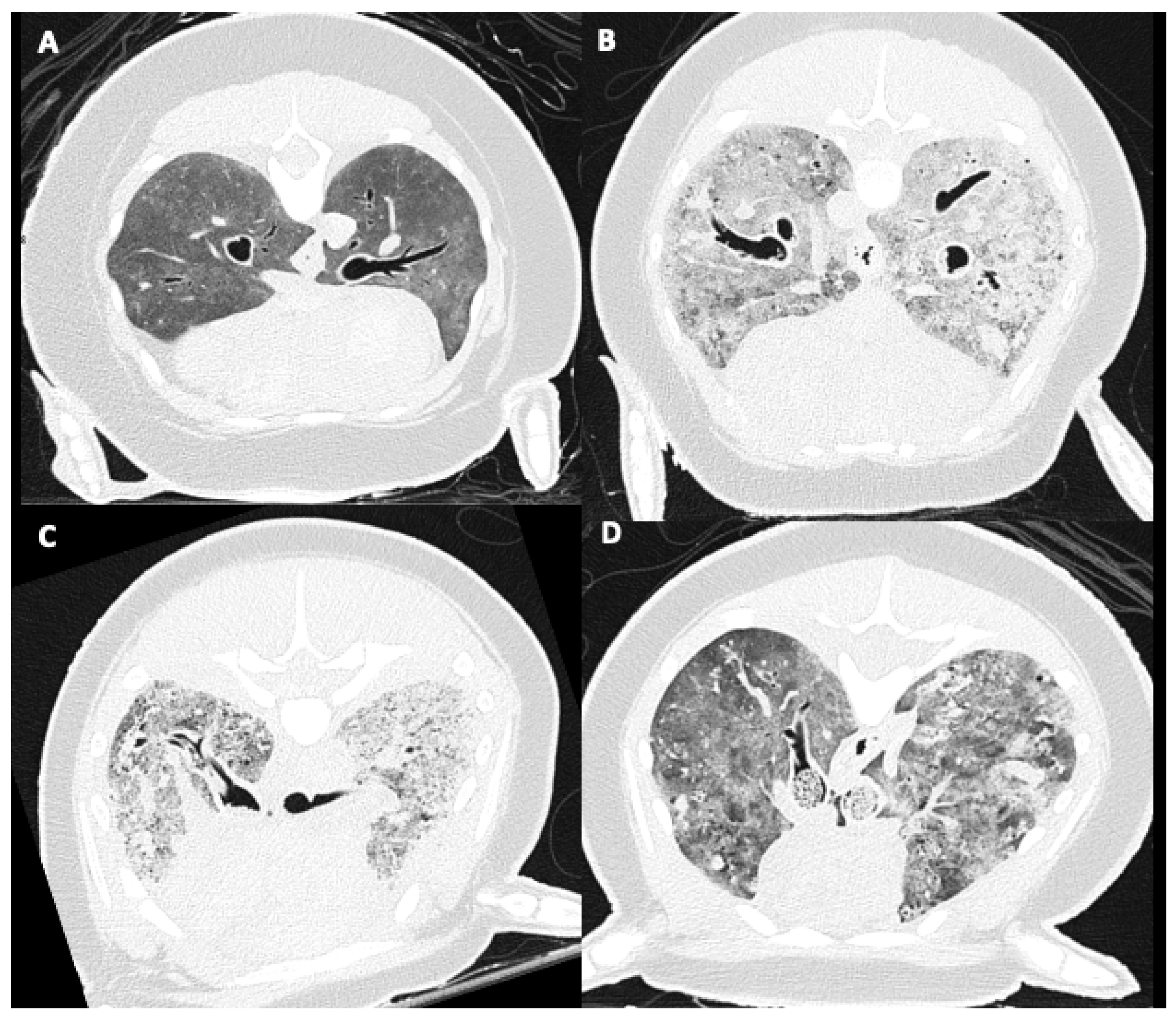
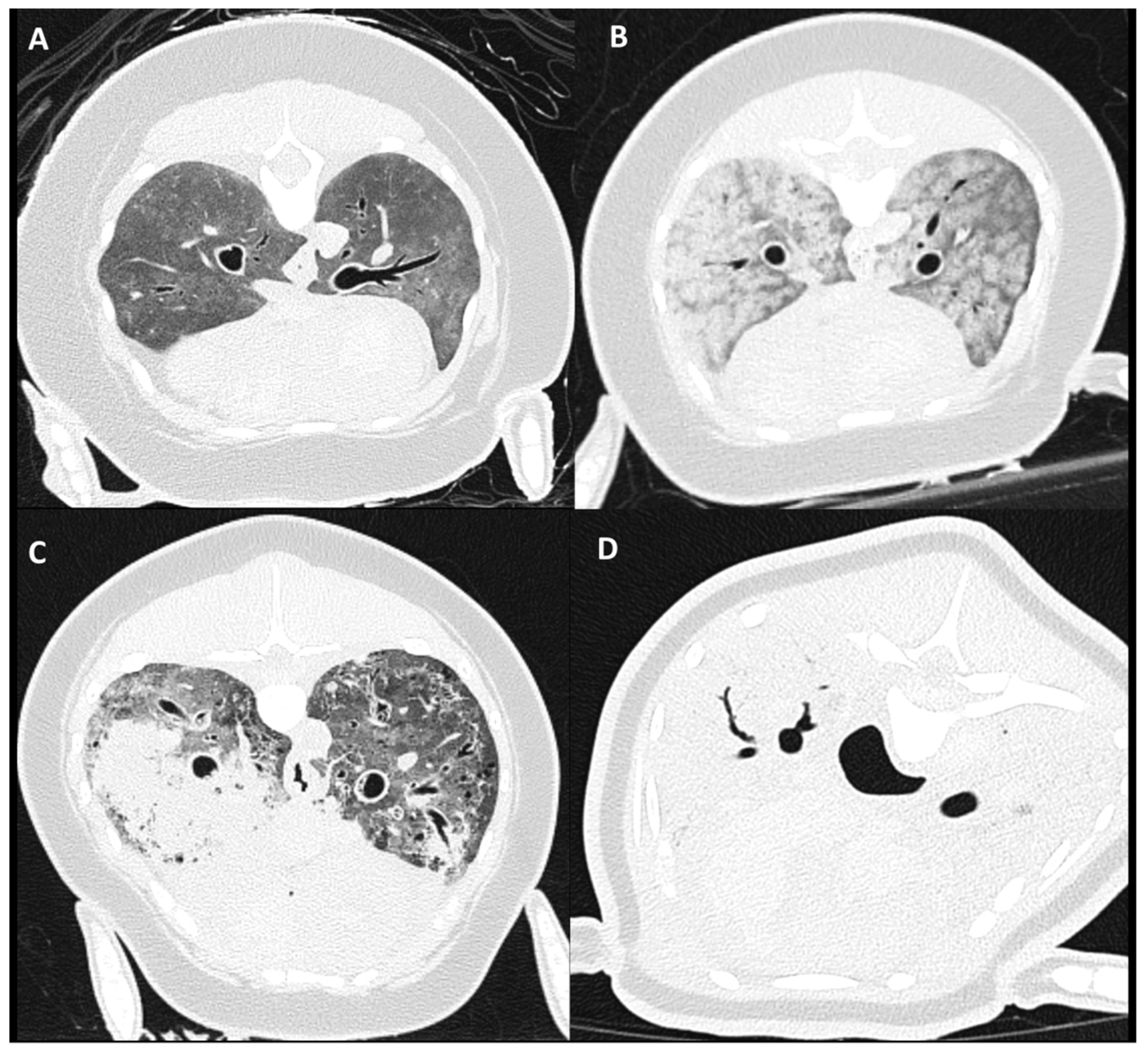
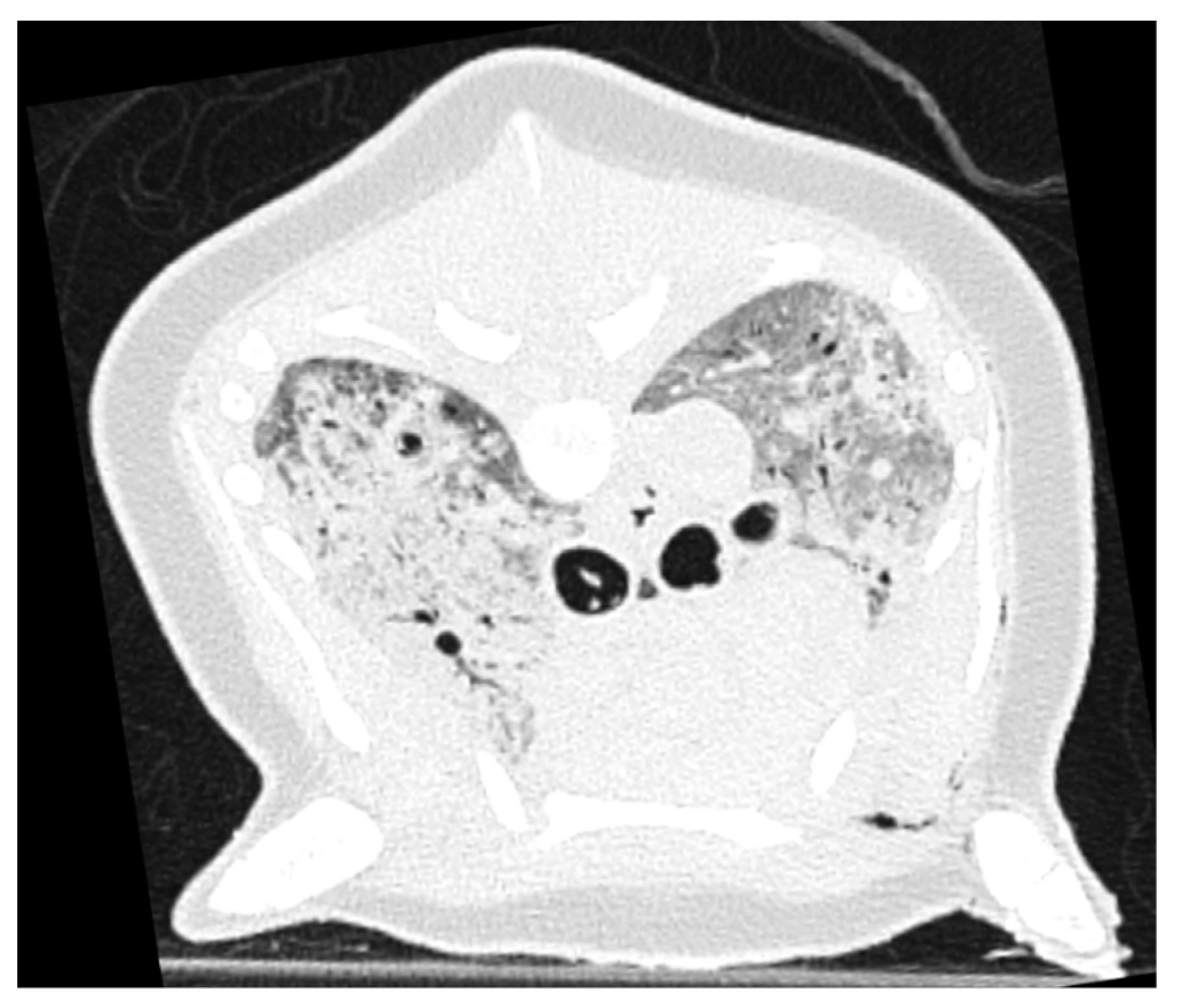
2.5. Pulmonary Parenchymal Attenuation Changes
3. Results
3.1. Subjects
3.2. Carcass Condition
3.3. Tracheobronchial Changes
3.4. Pulmonary Parenchymal Attenuation Changes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- IJsseldijk, L.L.; Doeschate, M.T.I.t.; Davison, N.J.; Gröne, A.; Brownlow, A.C. Crossing boundaries for cetacean conservation: Setting research priorities to guide management of harbour porpoises. Mar. Policy 2018, 95, 77–84. [Google Scholar] [CrossRef]
- Peltier, H.; Baagøe, H.J.; Camphuysen, K.C.; Czeck, R.; Dabin, W.; Daniel, P.; Deaville, R.; Haelters, J.; Jauniaux, T.; Jensen, L.F.; et al. The Stranding Anomaly as Population Indicator: The Case of Harbour Porpoise Phocoena phocoena in North-Western Europe. PLoS ONE 2013, 8, e62180. [Google Scholar] [CrossRef] [Green Version]
- Van Bressem, M.; Raga, J.A.; Di Guardo, G.; Jepson, P.D.; Duignan, P.J.; Siebert, U.; Barrett, T.; de Oliveira Santos, M.C.; Moreno, I.B.; Siciliano, S.; et al. Emerging infectious diseases in cetaceans worldwide and the possible role of environmental stressors. Dis. Aquat. Org. 2009, 86, 143–157. [Google Scholar] [CrossRef]
- Hamel, P.E.S.; Giglio, R.F.; Cassle, S.E.; Farina, L.L.; Leone, A.M.; Walsh, M.T. Postmortem computed tomography and magnetic resonance imaging findings in a case of coinfection of dolphin morbillivirus and aspergillus fumigatus in a juvenile bottlenose dolphin (Tursiops truncatus). J. Zoo Wildl. Med. 2020, 51, 448–454. [Google Scholar] [CrossRef]
- Camphuysen, C.J.; Smeenk, C.; Addink, M.J.; Jansen, O.E. Cetaceans stranded in the Netherlands from 1998 to 2007. Lutra 2008, 51, 87–122. [Google Scholar]
- Keijl, G.; Begeman, L.; Hiemstra, S.; IJsseldijk, L.L.; Kamminga, P.; dPB, C.R.; Applied Veterinary Research; Veterinair Pathologisch Diagnostisch Cnt. Cetaceans stranded in The Netherlands in 2008–2014. Lutra 2016, 59, 75. [Google Scholar]
- Camphuysen, K.C.J.; Siemensma, M.L. Conservation Plan for the Harbour Porpoise Phocoena phocoena in The Netherlands: Towards a Favourable Conservation Status; Royal Netherlands Institute for Sea Research: Texel, The Netherlands, 2011. [Google Scholar]
- Tsui, H.C.L.; Kot, B.C.W.; Chung, T.Y.T.; Chan, D.K.P. Virtopsy as a Revolutionary Tool for Cetacean Stranding Programs: Implementation and Management. Front. Mar. Sci. 2020, 7, 834. [Google Scholar] [CrossRef]
- Grela, M.; Listos, P.; Gryzińska, M.; Chagowski, W.; Buszewicz, G.; Teresiński, G. Imaging techniques as a method of sectional examination in forensic veterinary medicine. Med. Weter. 2018, 74, 751–758. [Google Scholar] [CrossRef] [Green Version]
- Watson, E.; Heng, H.G. Forensic radiology and imaging for veterinary radiologists. Vet. Radiol. Ultrasound 2017, 58, 245–258. [Google Scholar] [CrossRef]
- Alonso-Farré, J.M.; Gonzalo-Orden, M.; Barreiro-Vázquez, J.D.; Ajenjo, J.M.; Barreiro-Lois, A.; Llarena-Reino, M.; Degollada, E. Cross-Sectional Anatomy, Computed Tomography and Magnetic Resonance Imaging of the Thoracic Region of Common Dolphin (Delphinus delphis) and Striped Dolphin (Stenella coeruleoalba). Anat. Histol. Embryol. 2014, 43, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Ivančić, M.; Solano, M.; Smith, C.R. Computed Tomography and Cross-Sectional Anatomy of the Thorax of the Live Bottlenose Dolphin (Tursiops truncatus). Anat. Rec. 2014, 297, 901–915. [Google Scholar] [CrossRef]
- Kot, B.C.W.; Martelli, P. To see or not to see: Computed tomography features of postmortem change and decomposition in deceased cetaceans. In Proceedings of the International Association for Aquatic Animal Medicine (IAAAM), Cancun, Mexico, 19–23 May 2017. [Google Scholar]
- Kot, B.C.W.; Tsui, H.C.L.; Chung, T.Y.T.; Lau, A.P.Y. Postmortem Neuroimaging of Cetacean Brains Using Computed Tomography and Magnetic Resonance Imaging. Front. Mar. Sci. 2020, 7, 775. [Google Scholar] [CrossRef]
- Lundström, C.; Persson, A.; Ross, S.; Ljung, P.; Lindholm, S.; Gyllensvärd, F.; Ynnerman, A. State-of-the-art of visualization in post-mortem imaging. APMIS Acta Pathol. Microbiol. Immunol. Scand. 2012, 120, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Christe, A.; Flach, P.; Ross, S.; Spendlove, D.; Bolliger, S.; Vock, P.; Thali, M.J. Clinical radiology and postmortem imaging (Virtopsy) are not the same: Specific and unspecific postmortem signs. Leg. Med. 2010, 12, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Thali, M.; Yen, K.; Schweitzer, W.; Vock, P.; Boesch, C.; Ozdoba, C.; Schroth, G.; Ith, M.; Sonnenschein, M.; Doernhoefer, T.; et al. Virtopsy, a New Imaging Horizon in Forensic Pathology: Virtual Autopsy by Postmortem Multislice Computed Tomography (MSCT) and Magnetic Resonance Imaging (MRI)-a Feasibility Study. J. Forensic Sci. 2003, 48, 386–403. [Google Scholar] [CrossRef] [PubMed]
- Willems, D.; Ijsseldijk, L.; Gröne, A.; Veraa, S. Skeletal abnormalities in stranded harbor porpoises (Phocoena phocoena) detected by computed tomography. In Proceedings of the Abstract of the European Veterinary Diagnostic Imaging (EVDI) Congress, Basel, Switzerland, 21–24 August 2019. [Google Scholar]
- Willems, D.S.; IJsseldijk, L.L.; Broek, D.H.N.; Veraa, S. Vertebral pattern variation in the North Sea harbor porpoise (Phocoena phocoena) by computed tomography. Anat. Rec. 2021, 304, 968–978. [Google Scholar] [CrossRef]
- Kapetanou, A.; IJsseldijk, L.L.; Willems, D.S.; Broens, E.M.; Everaarts, E.; Buil, J.B.; Verweij, P.E.; Kik, M.J.L.; Grone, A. Mycotic Infections in Free-Ranging Harbor Porpoises (Phocoena phocoena). Front. Mar. Sci. 2020, 7, 344. [Google Scholar] [CrossRef]
- IJsseldijk, L.L.; Kik, M.J.L.; Gröne, A. Postmortaal Onderzoek van Bruinvissen (Phocoena Phocoena) uit Nederlandse Wateren, 2018: Biologische Gegevens, Gezondheidsstatus en Doodsoorzaken. WOt- Technical Report 150, IMARES 2019. Available online: https://www.wur.nl/nl/Publicatie-details.htm?publicationId=publication-way-353531373635 (accessed on 31 May 2022).
- Jepson, P.D.; Kuiken, T.; Bennett, P.M.; Baker, J.R.; Simpson, V.R.; Kennedy, S. Pulmonary pathology of harbour porpoises (Phocoena phocoena) stranded in England and Wales between 1990 and 1996. Vet. Rec. 2000, 146, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Kirkwood, J.K.; Bennett, P.M.; Jepson, P.D.; Kuiken, T.; Simpson, V.R.; Baker, J.R. Entanglement in fishing gear and other causes of death in cetaceans stranded on the coasts of England and Wales. Vet. Rec. 1997, 141, 94–98. [Google Scholar] [CrossRef]
- Siebert, U.; Wünschmann, A.; Weiss, R.; Frank, H.; Benke, H.; Frese, K. Post-mortem Findings in Harbour Porpoises (Phocoena phocoena) from the German North and Baltic Seas. J. Comp. Pathol. 2001, 124, 102–114. [Google Scholar] [CrossRef]
- Gibson, D.I.; Harris, E.A.; Bray, R.A.; Jepson, P.D.; Kuiken, T.; Baker, J.R.; Simpson, V.R. A survey of the helminth parasites of cetaceans stranded on the coast of England and Wales during the period 1990–1994. J. Zool. 1998, 244, 563–574. [Google Scholar] [CrossRef]
- Ten Doeschate, M.T.I.; Ijsseldijk, L.L.; Hiemstra, S.; De Jong, E.A.; Strijkstra, A.; Gröne, A.; Begeman, L. Quantifying parasite presence in relation to biological parameters of harbour porpoises phocoena phocoena stranded on the Dutch coast. Dis. Aquat. Org. 2017, 127, 49–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, M.J.; Bogomolni, A.L.; Dennison, S.E.; Early, G.; Garner, M.M.; Hayward, B.A.; Lentell, B.J.; Rotstein, D.S. Gas Bubbles in Seals, Dolphins, and Porpoises Entangled and Drowned at Depth in Gillnets. Vet. Pathol. 2009, 46, 536–547. [Google Scholar] [CrossRef] [PubMed]
- IJsseldijk, L.L.; Brownlow, A.C.; Mazzariol, S. Best practice on cetacean post mortem investigation and tissue sampling. Jt. ACCOBAMS ASCOBANS Doc. 2019. [Google Scholar] [CrossRef]
- IJsseldijk, L.L.; Scheidat, M.; Siemensma, M.L.; Couperus, B.; Leopold, M.F.; Morell, M.; Gröne, A.; Kik, M.J.L. Challenges in the Assessment of Bycatch: Postmortem Findings in Harbor Porpoises (Phocoena phocoena) Retrieved from Gillnets. Vet. Pathol. 2021, 58, 405–415. [Google Scholar] [CrossRef]
- Levy, A.D.; Harcke, H.T.; Mallak, C.T. Postmortem imaging: MDCT features of postmortem change and decomposition. Am. J. Forensic Med. Pathol. 2010, 31, 12–17. [Google Scholar] [CrossRef]
- Biljardt, S.; Brummel, A.; Tijhuis, R.; Sieswerda-Hoogendoorn, T.; Beenen, L.F.; van Rijn, R.R. Post-mortem fluid stasis in the sinus, trachea and mainstem bronchi; a computed tomography study in adults and children. J. Forensic Radiol. Imaging 2015, 3, 162–166. [Google Scholar] [CrossRef]
- McEwen, B.J.; Gerdin, J.A. Drowning and Bodies Recovered from Water. In Veterinary Forensic Pathology; Springer International Publishing: Cham, Switzerland, 2017; Volume 2, pp. 1–15. [Google Scholar]
- Bierens, J.J.L.M.; Lunetta, P.; Tipton, M.; Warner, D.S. Physiology of drowning: A review. Physiology 2016, 31, 147–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knieriem, A.; Hartmann, M.G. Comparative histopathology of lungs from by-caught Atlantic white-sided dolphins (Leucopleurus acutus). Aquat. Mamm. 2001, 27, 73. [Google Scholar]
- Lougheed, D.W.; Janes, J.M.; Hall, G.E. Physiological studies in experimental asphyxia and drowning. Can. Med. Assoc. J. 1939, 40, 423–428. [Google Scholar]
- Leger, J.S.; Raverty, S.; Mena, A. Cetacea. In Pathology of Wildlife and Zoo Animals; Academic Press: Cambridge, MA, USA, 2018; pp. 533–568. [Google Scholar] [CrossRef]
- Schwarz, T.; Johnson, V. Lungs and Bronchi. In Veterinary Computed Tomography; John Wiley & Sons, Ltd.: West Sussex, UK, 2011; pp. 261–277. [Google Scholar]
- Proisy, M.; Marchand, A.J.; Loget, P.; Bouvet, R.; Roussey, M.; Pelé, F.; Rozel, C.; Treguier, C.; Darnault, P.; Bruneau, B. Whole-body post-mortem computed tomography compared with autopsy in the investigation of unexpected death in infants and children. Eur. Radiol. 2012, 23, 1711–1719. [Google Scholar] [CrossRef] [PubMed]
- Thierry, F.; Handel, I.; Hammond, G.; King, L.G.; Corcoran, B.M.; Schwarz, T. Further characterization of computed tomographic and clinical features for staging and prognosis of idiopathic pulmonary fibrosis in West Highland white terriers. Vet Radiol. Ultrasound 2017, 58, 381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filograna, L.; Bolliger, S.A.; Ross, S.G.; Ruder, T.; Thali, M.J. Pros and cons of post-mortem CT imaging on aspiration diagnosis. Leg. Med. 2010, 13, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Filograna, L.; Thali, M.J. Post-mortem CT imaging of the lungs: Pathological versus non-pathological findings. Radiol. Med. 2017, 122, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Shiotani, S.; Kobayashi, T.; Hayakawa, H.; Kikuchi, K.; Kohno, M. Postmortem pulmonary edema: A comparison between immediate and delayed postmortem computed tomography. Leg. Med. 2011, 13, 151–155. [Google Scholar] [CrossRef]
- Shiotani, S.; Kohno, M.; Ohashi, N.; Yamazaki, K.; Nakayama, H.; Watanabe, K.; Oyake, Y.; Itai, Y. Non-traumatic postmortem computed tomographic (PMCT) findings of the lung. Forensic Sci. Int. 2004, 139, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Plaetsen, S.V.; De Letter, E.; Piette, M.; Van Parys, G.; Casselman, J.W.; Verstraete, K. Post-mortem evaluation of drowning with whole body CT. Forensic Sci. Int. 2015, 249, 35–41. [Google Scholar] [CrossRef]
- Levy, A.D.; Harcke, H.T.; Getz, J.M.; Mallak, C.T.; Caruso, J.L.; Pearse, L.; Frazier, A.A.; Galvin, J.R. Virtual Autopsy: Two- and Three-dimensional Multidetector CT Findings in Drowning with Autopsy Comparison1. Radiology 2007, 243, 862–868. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.I.; Lee, K.N.; Tomiyama, N.; Johkoh, T.; Ichikado, K.; Kim, C.W.; Lee, S.H. Near Drowning: Thin-Section CT Findings in Six Patients. J. Comput. Assist. Tomogr. 2000, 24, 562–566. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PMCT Parameter | Score |
|---|---|
| PMCT autolysis score | 0 absent, 1 mild, 2 moderate, 3 severe |
| Pneumothorax | 0 absent, 1 present |
| Tracheobronchial | |
| Intraluminal tracheobronchial tubular structures | 0 none, 1 mild, 2 moderate, 3 severe |
| Bronchial wall thickening | 0 absent, 1 present |
| Tracheobronchial fluid | 0 absent, 1 present |
| Pulmonary attenuation | |
| Severity of pulmonary soft tissue attenuation | 0 absent, 1 mild, 2 moderate, 3 severe |
| Dorsoventral distribution pulmonary soft tissue attenuation | 0 diffuse, 1 dorsal, 2 ventral |
| Left/right distribution pulmonary soft tissue attenuation | 0 bilateral, 1 left, 2 right |
| Pulmonary parenchymal nodules | 0 absent, 1 present |
| Pulmonary mineralization | 0 absent, 1 present |
| Pulmonary air entrapment | 0 absent, 1 present |
| Parameter | Score |
|---|---|
| Decomposition carcass condition (DCC) | 1–3 |
| Pleural space content | 0 absent, 1 present |
| Tracheobronchial | |
| Tracheal content | 0 absent, 1 edema, 2 foam |
| Tracheobronchial helminths | 0 none, 1 mild, 2 moderate, 3 severe |
| Pulmonary parenchyma | |
| Pulmonary edema | 0 absent, 1 present |
| Asymmetry lung volume | 0 absent, 1 present |
| Distribution pattern pulmonary lesions | 0 not mentioned, 1 diffuse, 2 cranioventral, 3 mid-dorsal |
| Pulmonary nodules | 0 absent, 1 present |
| Pulmonary mineralization macroscopically | 0 absent, 1 present |
| Pulmonary mineralization microscopically | 0 absent, 1 present |
| Histologic tissue reactions | 0 none mentioned, 1 fibrosis, 2 emphysema |
| PMCT | Number (%) | Conventional Necropsy | Number (%) |
|---|---|---|---|
| Autolysis Score | DCC | ||
| None | 0/46 (0) | - | |
| Mild | 26/46 (57) | 1 | 16/46 (35) |
| Moderate | 16/46 (35) | 2 | 24/46 (52) |
| Severe | 4/46 (9) | 3 | 6/46 (13) |
| Pneumothorax | 5/46 (11) | Pleural content | 0/46 (0) |
| Tracheobronchial changes | |||
| Tracheobronchial tubular structures | Helminthiasis | ||
| Absent | 14/46 (30) | Absent | 10/46 (22) |
| Mild | 4/46 (9) | Mild | 4/46 (9) |
| Moderate | 11/46 (24) | Moderate | 18/46 (40) |
| Severe | 17/46 (37) | Severe | 14/46 (30) |
| Bronchial wall thickening | 30/46 (65) | - | |
| Tracheobronchial content | Tracheal content | ||
| None | 20/46 (43) | None | 39/46 (85) |
| Fluid | 26/46 (57) | Edema | 2/46(4) |
| Foam | 5/46 (11) | ||
| Pulmonary parenchyma | |||
| PSTA severity | Pulmonary edema | 38/46 (83) | |
| None | 0/46 (0) | - | |
| Mild | 3/46 (7) | - | |
| Moderate | 24/46 (52) | - | |
| Severe | 19/46 (41) | - | |
| Asymmetry lung volume | 6/46 (13) | ||
| Distribution lung changes | |||
| Dorsal | 0/46 (0) | - | |
| Ventral | 2/46 (4) | - | |
| Left | 10/46 (22) | - | |
| Right | 10/46 (22) | - | |
| Bilateral | 26/46 (56) | Bilateral | 16/46 (35) |
| Parenchymal nodules | 22/46 (48) | Parenchymal nodules | 11/46 (24) |
| Mineralization | 23/46 (50) | Gross mineralization | 11/46 (24) |
| Pulmonary air entrapment | 33/46 (72) | - | - |
| Histology | |||
| - | Histologic mineralization | 28/46 (61) | |
| - | Histologic emphysema | 13/46 (28) | |
| - | Histologic fibrosis | 12/46 (26) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuijpers, N.W.; van Schalkwijk, L.; IJsseldijk, L.L.; Willems, D.S.; Veraa, S. Post-Mortem Computed Tomography Pulmonary Findings in Harbor Porpoises (Phocoena phocoena). Animals 2022, 12, 1454. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12111454
Kuijpers NW, van Schalkwijk L, IJsseldijk LL, Willems DS, Veraa S. Post-Mortem Computed Tomography Pulmonary Findings in Harbor Porpoises (Phocoena phocoena). Animals. 2022; 12(11):1454. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12111454
Chicago/Turabian StyleKuijpers, Nienke W., Linde van Schalkwijk, Lonneke L. IJsseldijk, Dorien S. Willems, and Stefanie Veraa. 2022. "Post-Mortem Computed Tomography Pulmonary Findings in Harbor Porpoises (Phocoena phocoena)" Animals 12, no. 11: 1454. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12111454