
Drug-Dosing Adjustment in Dogs and Cats with Chronic Kidney Disease


1
Faculty of Veterinary Medicine, Veterinary Teaching Hospital, University of Teramo, Località Piano d’Accio, 64100 Teramo, Italy
2
Department of Veterinary Medical Sciences, Alma Mater Studiorum, University of Bologna, Via Tolara di Sopra 50, 40064 Bologna, Italy
*
Author to whom correspondence should be addressed.
Animals 2022, 12(3), 262; https://0-doi-org.brum.beds.ac.uk/10.3390/ani12030262
Submission received: 20 November 2021
/
Revised: 13 January 2022
/
Accepted: 18 January 2022
/
Published: 21 January 2022
(This article belongs to the Special Issue Advances in Canine and Feline Nephropathies)
Abstract
:Simple Summary
Adjusting drug dosages in dogs and cats with chronic kidney disease (CKD) can be challenging in clinical practice due to the lack of specific indications in the current literature; moreover, the evaluation of renal function through the measurement of glomerular filtration rate (GFR), which is unanimously considered as a requisite for most adjustment strategies, is often hard to perform in clinical settings. Therefore, the present review aims to provide practical guidelines for dosage adjustment in CKD patients through an overview of the available literature.
Abstract
Chronic kidney disease is a common kidney disorder in adult and aged dogs and cats; the management of associated complications and comorbidities generally requires a life-long medical treatment to ensure a good quality of life of affected patients. However, indications and the literature on drug dosing in dogs and cats with chronic kidney disease are often lacking. The aim of this review is to revise the current literature on drug dosing in canine and feline patients with renal impairment, with a special focus on the most commonly used medications to manage chronic kidney disease and possible comorbidities.
1. Introduction: Chronic Kidney Disease and Implications in Drug Dosing
Chronic kidney disease (CKD) is the most commonly recognized form of kidney disorder in dogs and cats and, in most instances, it represents an irreversible and progressive condition [1]. The prevalence of CKD has been estimated to be 0.5–1.0% in dogs and 1.0–3.0% in cats, with a higher prevalence in older animals and a rate as high as 80% in the geriatric cat population [2,3,4].
The clinical consequences of CKD reflect the extent of a reduction in renal function rather than the impact of structural lesions [3]. Given the progressive nature of the disease, these patients often require lifelong medical treatment to limit the progression of renal injury and improve their quality of life. The conservative medical management of CKD consists of a supportive and symptomatic therapy designed to ameliorate clinical signs of uremia, correct fluid and electrolyte imbalance, provide adequate nutritional requirements and slower the progression of renal failure [5]. Antihypertensive and antiproteinuric drugs, phosphate binders, antiemetic and antacid medications are usually administered to manage the clinical signs and long-term complications related to renal failure [5,6,7]. Furthermore, in dogs with protein losing nephropathy (PLN), which are considered at risk for the development of thrombosis, antithrombotic prophylaxis is recommended [8].
Liver metabolism and renal excretion are the major drug-elimination pathways [9]. For this reason, patients with an impaired renal function could require adjustment of the usual drug-dosage regimen, not only to overcome serious adverse reactions because of excessive drug accumulation but also to avoid treatment failure [10,11]. In fact, either sub- or supratherapeutic dosing can occur when appropriate dose adjustments are not made in patients with kidney disease, and both have negative effects on patient outcomes [10].
In veterinary clinical practice, dose adjustment for CKD patients is rarely performed: there is no widely available, easy-to-perform method to measure the glomerular filtration rate (GFR), which is generally required to establish an appropriate dosing strategy. Furthermore, there are no practical guidelines to perform dose adjustments in animals with CKD. Indeed, information on specific dose adjustment in dogs with renal impairment is sparse [12] and the available information for cats is often extrapolated from canine or human reports [13].
The present review describes the mechanisms of altered drug handling in CKD and discusses the rationale of dose adjustment regimens in the most commonly used classes of medication in CKD management and related complications; moreover, the effective need to adjust the dose of other commonly used drugs in clinical practice, and their potential impact on renal function, will be analyzed.
2. Evaluation of Renal Function
A thorough assessment of renal function is required to establish an appropriate dose adjustment. Glomerular function is generally considered the best indicator of renal function and can be evaluated by means of both indirect and direct tests.
The measurement of GFR is deemed the most sensitive test directly measuring kidney filtration and excretion that can detect decreases in organ function [14,15]. An evaluation of GFR may provide critical information on kidney function far earlier than the more widely used markers of renal function in dogs and cats with unexplained polyuria and polydipsia and might help predict the risk of developing overt renal failure after nephrectomy in animals with unilateral kidney disease [16]. Furthermore, the measurement of GFR could be useful for the diagnosis of CKD before the onset of azotemia, for ruling out pre-azotemic acute kidney injury (AKI) and for dose adjustments of chemotherapy and other potentially nephrotoxic medications [16,17].
Glomerular filtration rate is defined as the volume of ultrafiltrate produced by glomerular filtration per unit of time and can be measured using the urinary or plasmatic clearance of appropriate markers, where the clearance describes the relationship between the transfer rate of the marker and its concentration in urine or plasma, respectively [14,15]. Thus, an ideal GFR marker should be freely filtered by the glomeruli, not reabsorbed or secreted by the renal tubule, nor metabolized or produced by the kidney, and should not alter the GFR value itself; when the plasma clearance approach is used, the marker should also be totally cleared by the kidneys [14]. The markers that are currently used to measure GFR in animals include inulin, exogenous creatinine, radionucleotides and iohexol. Due to its ease of use, low cost and wider availability, plasma clearance of iohexol is the most commonly used marker of GFR in veterinary and human medicine [17,18]. The principle underlying plasma clearance methods is the repeated measurement of the elected marker in several blood samples taken over time, following the initial administration. Clearance (Cl) is expressed as mL/min/kg and calculated using the formula: Cl = dose/AUC, where AUC is the area under the plasma disappearance curve of the marker [19]. Sampling should ideally continue until all the administered marker is excreted. The longer the period of collection, the more accurate the GFR measurement. However, given that repeated blood sampling is not always feasible in clinical practice, correction formulae derived from human medicine (e.g., the Brøchner–Mortensen formula) have been proposed and applied in dogs and cats to estimate GFR from the clearance, determined with a limited sampling strategy [17,18,20,21,22].
As with indirect makers of renal function, GFR is also influenced by several extra-renal factors, including sex, age, breed, dietary protein intake, hydration status, sodium balance, and day-to-day circadian rhythm [19]. Furthermore, given the high variability that exists in dogs and cats, a standardization of GFR to body size is needed. To this end, GFR has been related to body surface area, body mass and extracellular fluid volume; in veterinary medicine, GFR is generally related to body mass and is thus expressed in mL/kg/min [14,19]. Most published normal values for GFR are between 2 and 5 mL/kg/min in dogs and cats and a value below 1.5 mL/kg/min is generally assumed to be abnormal in average-sized dogs [23]. A cut-off value of 2.1 mL/kg/min should be considered for a body weight of <10 kg and about 1.2 mL/kg/min for dogs with a body weight of >45 kg [15]. Plasma clearance references were proposed for cats, considering a range of 1.0–3.5 mL/kg/min for iohexol and 1.3–3.8 mL/kg/min for creatinine [22]. To date, despite its accuracy in evaluating renal function in comparison with indirect markers, the assessment of GFR is rarely performed in veterinary clinical practice due to its poor feasibility and limitations in the interpretation of results.
Among the indirect methods used to assess renal function, the combination of plasma or serum creatinine (sCr), urea concentrations and urine specific gravity (USG) is commonly evaluated in veterinary medicine [24]. Based on these variables, the International Renal Interest Society (IRIS) has proposed a scoring system for staging CKD in dogs and cats to assist clinicians in determining the appropriate therapy, forecasting prognosis, and implementing follow-up steps required for appropriate disease management. According to the IRIS staging guidelines, renal function has to be measured in a hydrated and stable patient, by fasting sCr concentration (possibly combined with symmetric dimethylarginine, SDMA), on at least two occasions. The subsequent sub-classification is then based on the evaluation of proteinuria and blood pressure [25].
Serum creatinine concentration is currently considered the best indirect marker of GFR. Creatinine is produced by the degradation of creatine and creatine phosphate in skeletal muscles at a relatively constant rate and, once in the blood stream, it is completely filtered by the glomeruli, without significant tubular reabsorption or secretion [14,15,26]. The increase in sCr concentration above the reference interval is assumed to be representative of a loss of function of at least 67–75% of nephrons [15]. The relationship between sCr concentration and GFR is represented by a steep curvilinear trend, which means that a significant reduction in GFR is required before a corresponding increase in sCr concentration is seen. Nevertheless, even sCr values within the reference interval can be used to predict a decline in GFR over time, provided that the non-renal factors influencing creatinine remain stable [24,27,28]. Serum creatinine concentration can, therefore, be considered a more sensitive marker in the late course of CKD rather than in the early stages. Although a high sCr concentration is typically associated with severe renal dysfunction, some other conditions should be considered, such as the high muscle production of creatinine, reduction in extracellular fluid volume and intestinal absorption of exogenous creatinine. Hence, physiological factors such as age, muscle mass, breed, exercise and the effect of meals should be taken into account when an increase in plasma creatinine is observed. Furthermore, sCr has shown lower sensitivity as a marker of renal function in dogs with portosystemic shunts and in cats with hyperthyroidism [15,29]. To overcome the aforementioned limits of sensitivity and sensibility, the IRIS staging guidelines recommend that sCr should be evaluated in fasted, stable, well-hydrated patients on at least two occasions. Moreover, the result should be interpreted considering the breed, muscle mass and age of the animal [24].
Urea is the main form in which nitrogen is eliminated from the body and its concentration in serum or plasma can be expressed as blood urea nitrogen (BUN) [15]. Serum urea concentration is increased in renal failure; however, in contrast to creatinine, it is considered a worse indirect indicator of GFR due to its tubular re-absorption. Moreover, BUN can be increased in several non-renal conditions such as prerenal azotemia, high-protein diet, gastrointestinal bleeding, tetracycline or corticosteroid administration. Conversely, its concentration can be decreased in hepatic insufficiency, polyuria and polydipsia and low-protein diets. Given its poor sensibility and specificity as marker of renal function, it is generally recommended that BUN is evaluated in conjunction with creatinine concentration and USG measurements [30].
Urine-specific gravity provides important information about the renal urine concentrating capacity and it is widely reported that, in dogs with pre-renal azotemia, USG should exceed 1.030, whilst in cats, it should exceed 1.035 [15,31]. However, cats may also maintain some urine concentration ability, despite significant reductions in renal mass, especially when dehydrated [24,32].
Symmetrical dimethylarginine is a compound produced in cells through the methylation of arginine residues and it is subsequently released into the circulation during proteolysis [33,34]. In recent years, research has focused on how SDMA may be utilized in veterinary medicine, and assays for its measurement are currently available in clinical practice. Despite analytical and intra-individual variability, there is evidence that SDMA is not influenced by muscle mass, and is thus likely to provide a more accurate representation of GFR than creatinine, especially in patients with sarcopenia [35,36]. Based on this concept, SDMA has been incorporated into the IRIS staging system. The relationship between SDMA and serum or plasma creatinine and GFR seems to be very similar, but SDMA can detect a decline in renal function earlier, highlighting its possible role as an earlier marker of CKD [24,28,36,37]. Nevertheless, the possible influence of non-renal diseases on the specificity and sensibility of SDMA as a marker of renal function is still under investigation.
3. Mechanisms Underlying Altered Renal Drug Handling in CKD
The mechanisms responsible for the altered renal drug handling in renal impairment are different and complex, and involve both pharmacokinetic and pharmacodynamic processes [38].
Pharmacokinetics is a branch of pharmacology that describes the body’s effect on a drug, reflecting the physiologic processes of absorption, distribution, metabolism and excretion; all of these phases may be altered in patients with kidney disease. Conversely, pharmacodynamics studies the effects of the drug on the body, including interactions between the drug, its target and downstream biochemical effects [10].
The adsorption of drugs from the gastrointestinal tract may be highly variable in CKD patients, and can increase due to an impairment in the gut wall barrier function or due to an abnormal function or expression of efflux transporters [39]. Furthermore, the interactions between several orally administered drugs should be considered, as in the case of phosphate binders that significantly influence the intestinal absorption of other orally administered drugs [40].
An expansion in the volume of distribution (Vd) is reported in advanced CKD because of fluid retention, hypoalbuminemia and the subsequent decreased protein binding [11,39]. Specifically, the reduction in plasma protein binding is a consequence of several mechanisms, such as hypoalbuminemia, that occur in protein-losing nephropathies (PLN), the accumulation of endogenous substances, which competitively displace acidic drugs from the binding sites of albumin, or even conformational changes in the binding sites. In fact, uremic toxins such as urea, indoxyl sulphate and cytokines may be responsible for transcriptional, translational or post-translational modifications to several transporter and enzyme functions [41,42,43,44].
Glomerular filtration, tubular secretion and tubular reabsorption are the three main renal drug excretion pathways, although other pathways, such as metabolism and P-glicoprotein activity, can contribute [9]. The glomerular filtration of a drug is a passive process involving the plasmatic unbound drug fraction, and is dependent on the renal blood flow available for filtration. The tubular secretion is an active system of transport that occurs via membrane transporters, such as organic cation transporters (OCT) and organic anion transporters (OAT) located in the proximal tubule of the nephron; competition for the transporters can be responsible for drug interactions. The tubular reabsorption is mainly a passive transport process allowing low-molecular-weight, lipophilic and un-ionized molecules to be passively reabsorbed based on diffusion principles. Less commonly, the reabsorption process in the proximal tubule can be actively mediated by specific transporters [9].
The renal excretion of drugs in CKD is generally decreased as a result of the reduction in GFR. Nevertheless, the mechanisms underlying drug excretion in renal impairment are complex. The practical approach based on the “intact nephron hypothesis”, which assumes that renal drug clearance will almost entirely decrease in proportion to the reduction in GFR, is subjected to several limits and is not suitable for all drugs, types of kidney disease and different GFRs [45,46]. In fact, recent evidence suggests that renal drug handling pathways may not decline in parallel, and thus the evaluation of each of these pathways may be more adequate [9,10,39].
Only a few drugs are eliminated almost entirely unchanged by the kidneys, and most of them undergo metabolization reactions [11]. Although the renal metabolism is generally lower than that of the liver or gastrointestinal tract, it has been suggested that the kidneys may be responsible for 15–40% of the metabolization of some drugs, mainly through the reaction of sulphation and glucuronidation [9,47]. In patients with kidney dysfunction, the renal excretion of parent drugs and/or active metabolites is often impaired, possibly due to alterations in drug-metabolizing enzyme activity caused by the accumulation of uremic toxins, leading to their excessive accumulation in the body [48,49]. Moreover, the non-renal clearance of drugs in patients with CKD can be additionally compromised due to reduced metabolic enzyme activity and alterations in the function of transporters caused by uremic toxins [11].
4. Rational Design of Dosing Regimens in CKD Patients
The goal of rational drug dosing is to maximize the benefits while minimizing the risks related to a given medication. Although indications of dosage adjustment in patients with kidney disease are often provided by the product label, several limitations should be considered; for example, the difficulty of testing pharmacokinetics in a large sick population, in which interpatient pharmacokinetic variability exists. Moreover, this is further complicated when a heterogeneous mix of etiologies is implied. Moreover, a dosage adjustment is generally based on the simplistic assumption that only renal clearance is changed. As a result, manufacturers may recommend that a given medication is contraindicated in patients with advanced kidney disease [39].
A common practical approach for drug dosing in patients with renal disease is to use a conservative approach with progressive dose escalation; however, this method may be reasonable for drugs that yield a clinical benefit from long-term treatment but is not indicated for drugs requiring a rapid onset of effect, such as antibiotics or immunosuppressive medications [39].
The main principles that should be taken into account when a dose adjustment is considered are the therapeutic target, the initial dose, the maintenance dose and the frequency of administration [39]. The dose fraction (Kf) represents a key factor for dosages adjustment. It is defined as Kf = GFRr/GFRn, where GFRr and GFRn are the GFR values in renal impairment and healthy conditions, respectively [50].
The “constant-interval, dose reduction” method is one of the possible applicable strategies for dose adjustment and is more indicated when the dosage interval is less than the elimination half-life, and with drugs with a narrow therapeutic index, such as aminoglycosides; this method is generally associated with the achievement of a more constant drug concentration [51]. The dosing interval is unchanged and the dose is multiplied by Kf [50,52]; alternatively, a dose reduction to 75% and 50% of the standard dose could generally be expected for moderate and severe renal disease, respectively [53].
In the “constant-dose, interval extension” method, the dose is unchanged and the dosing interval is increased by dividing it by Kf. From a practical perspective, a formula based on serum creatinine can alternatively be used to determine the dose interval, as follows: new interval = normal dosing interval × (patient creatinine/normal creatinine) [54]. However, given that the change in GFR is considered the best indicator of renal dysfunction and alterations in drug renal clearance, the first step in dosage regimen adjustment should be the determination of GFR value in the patient [15,55,56]. This method works well with medications that have a broad therapeutic window and a long half-life, such as penicillin and cephalosporins [51]. It is worth noting that, for antibacterial drugs with a concentration-dependent kill rate, this method is appropriate, while for those with time-dependent activity, the “constant-interval, dose-reduction” method is recommended to maintain plasma concentrations above the minimum inhibitory concentration (MIC) [50,51,52,57]. When a dosage adjustment is required, the risks of subtherapeutic serum concentrations must be weighed against the risks of adverse events. Consequently, combining dose reduction with interval extension could be a valuable option in the CKD population [51].
Provided that the time required to reach a steady state is generally increased in renal impairment, the administration of a loading dose at the beginning of treatment could be an effective strategy to allow therapeutic concentrations to be reached more rapidly [52]. This concept should be taken into account for antimicrobial drugs, for which a loading dose is often required to bring the serum level above MIC within a reasonable time period [51]. The appropriate loading dose could be ascertained using the following calculation: loading dose = Vd × IBW × Cp, where Vd is the volume of distribution measured in liters per kilogram, IBW is the ideal body weight in kilograms, and Cp is the desired medication plasma concentration in milligrams per liter [51]. Alternatively, if the constant-interval method is employed, the usual dose can be administered as a loading dose, followed by the calculated reduced dose. If the constant-dose method is used, the initial two doses should be given according to the usual interval [43].
Therapeutic drug monitoring (TDM) consists of monitoring plasma drug concentrations at regular intervals to optimize the effectiveness of the treatment. If drugs with a narrow therapeutic index are used under renal impairment conditions, this should be performed if renal dysfunction progresses, or adverse reactions or therapeutic failure occur [50,55,58].
In the following sections, an overview of the main literature on drug-dosing in CKD canine and feline patients will be revised, and recommendations for dose adjustments to the most commonly used drugs will be provided. A summary of the main indications and recommendations is provided in Table 1.
5. Antimicrobial Agents
Antimicrobials are frequently prescribed in CKD patients due to the high prevalence of urinary tract infection (UTI), which is reported to be approximately 15–30% in cats [115,116] and 8% in dogs with CKD [117].
Renal excretion is the major route of elimination for almost all antimicrobials, and dosage adjustments are commonly made in human patients with renal insufficiency due to concerns regarding their potential nephrotoxicity and efficacy [118]. The major variables for bactericidal drugs are the peak of concentration and the area under the plasma concentration time curve, while the “constant-interval, dose reduction method” seems to be more appropriate to maintain therapeutic levels of bacteriostatic antimicrobials [55].
Varying degrees of nephrotoxicity are reported for aminoglycosides, cephalosporins, tetracyclines and sulfonamides; a negligible nephrotoxic potential is attributed to penicillins and fluoroquinolones due to their high therapeutic index and partial renal excretion, respectively [55].
5.1. Aminoglycosides
Aminoglycosides are among the best choices for the treatment of severe Gram-negative aerobe bacterial infections [59,119,120]. The introduction of broad-spectrum antibiotics with better safety profiles, such as fluoroquinolones and extended-spectrum β-lactam antimicrobials, has led to a reappraisal of the indications for aminoglycoside therapy. To date, their use is limited to the short-term treatment of infections caused by susceptible microorganisms that are resistant to less toxic antibiotics [59].
Aminoglycosides are poorly adsorbed from the gastrointestinal tract and have a low protein binding. These drugs are almost entirely eliminated by glomerular filtration; however, they progressively accumulate in the renal cortex, causing their toxic effect [55]. Among other side effects, the nephrotoxic risk is a major concern, especially when parenterally administered, for long-term therapies and when pre-existing renal impairment conditions are present. In addition, the risk associated with topical administration should not be underestimated [55,121]. The risk of nephrotoxicity increases with the treatment duration, as aminoglycoside nephrotoxicity is cumulative [59,122]. Neomycin and gentamicin are the most nephrotoxic aminoglycosides, while tobramycin is less nephrotoxic than gentamicin at equivalent doses [55]. The nephrotoxic effect, which is due to acute tubular necrosis, is usually reversible with early discontinuation, and this risk may be reduced by using short-term therapies and allowing the plasma drug concentration to drop below the recommended concentrations doses. Nevertheless, caution should be used for all aminoglycosides in patients with preexisting renal disease and conditions such as dehydration, fever or sepsis [55,59]. Although cats are reported to be less susceptible to gentamicin-induced nephrotoxicity than dogs, its administration in both dogs and cats affected by CKD is discouraged [7].
For many years, aminoglycosides were administered in multiple daily doses. However, the total daily dose in one administration lowers the risk of toxicity, as it reduces the proportion of the total daily dose that can accumulate within the kidney [59]. Indeed, many in vitro and in vivo studies suggest that administration in a single daily-dosing (SDD) regimen is as effective as, or more effective than, conventional regimens and reduces the associated toxicity [123,124,125,126]. Aminoglycosides provide a post-antibiotic effect (PAE), which is defined as the ability to promote a bacteriostatic effect even after serum drug concentrations have fallen below the minimum MIC of the organism in question. This peculiarity allows for longer dosing intervals, according to the fixed-dose interval extension method [55,59,120,125,127].
Due to the interpatient variability in pharmacokinetic variables, such as volume of distribution and renal function, TDM has been the standard of care in people treated with traditional multiple-daily-dosing regimens to ensure adequate peak concentrations and prevent toxicity; moreover, TDM is also recommended with SDD when treatment duration is longer than 5–7 days or for patients at high risk of toxicity [59,120,125]. As toxicity is both dose- and time-dependent, the treatment duration should be minimized as much as possible.
The daily monitoring of renal function through the evaluation of increases in plasma creatinine, urine sediment for granular casts and reduction in urine output is recommended; if any sign of toxicosis is observed, the administration should be interrupted [59,128].
Recommended gentamicin doses under a SDD regimen via intravenous (IV), intramuscular (IM) or subcutaneous (SC) routes ranges between 9 and 14 mg/kg in dogs and 5 and 8 mg/kg in cats [129]. Serum peak concentrations 30 min after IV administration or 60 min after IM administration could be evaluated in TDM and should fall between 15 and 20 mg/mL; alternatively, a concentration measured 2–4 h before the next dose should not exceed 1 µg/mL or be undetectable [59]. Recommended doses for amikacin at a SDD regimen range between 15 and 30 mg/kg in dogs and 10 and 14 mg/kg in cats [129]. Serum peak concentrations should fall between 30 and 40 mcg/mL; through concentration should not exceed 2.5 µg/mL or be undetectable [59].
5.2. Penicillins
Penicillins exert a bactericidal action against Gram-positive and some Gram-negative bacteria. However, although the nephrotoxic effect in dogs and cats attributed to penicillin is generally negligible because of the high therapeutic index of these antibiotics [55,60,121], it is worth to consider the potential impact on kidney function in patients with renal impairment.
In human patients with decreased renal function, potentiated penicillin has a decreased renal clearance, resulting in higher serum concentrations in comparison with patients with normal renal function; thus, since potentiated penicillin is predominately excreted by the kidneys, dose adjustment of potentiated penicillin (i.e., decreased dose or decreased frequency) has been recommended in human patients with a severe reduction in GFR (i.e., <30 mL/min) to avoid excessive drug accumulation [57,130].
Similarly to those in humans, penicillin-related side effects seem to be limited in dogs with renal insufficiency due to their high therapeutic index. However, since it has been shown for ampicillin that drug accumulation might occur beyond 48 h of administration, dose adjustment should be considered [55,61]. In particular, in dogs with severe azotemia (creatinine > 4 mg/dL), after a single 22 mg/kg ampicillin dose, a slower clearance and increased plasma concentrations of ampicillin has been reported; in such cases, an interval extension can be adopted in order to reduce the risk of drug accumulation while still maintaining an effective therapeutic level for susceptible bacteria [61].
The dose adjustment of penicillin in cats with impaired renal function appears to be unnecessary due to the wide therapeutic window of these antimicrobials, which could be classified as “probably safe” in CKD patients [7,13]. The side effects of amoxicillin–clavulanic acid were evaluated in feline patients with and without azotemic CKD, with altered pharmacokinetics observed in cats with azotemic CKD; however, the need for dose adjustments in azotemic feline patients remains to be determined [62].
5.3. Cephalosporins
Cephalosporins are broad-spectrum bactericidal agents, active against Gram-positive and Gram-negative bacteria. They are classified into four generations, characterized by an increasing resistance to β-lactamase destruction, and often by an extended, although variable, spectrum [60].
The pharmacokinetic properties of cephalosporins are similar to those of penicillin. The plasma protein binding is <40% and the main route of elimination is tubular excretion, although cephalothin, cephapirin and cefotaxime have a substantial hepatic metabolism [131].
Cephalosporins are a class of relatively safe antimicrobial agents; nevertheless, high doses or very prolonged use have been associated with interstitial nephritis and tubular necrosis [57,60]. With the exception of those which are mainly eliminated by the extrarenal route, such as cefoperazone or cefixime [118,132], cephalosporins clearance is decreased in human patients with renal failure, and a dosage regimen adjustment is recommended if a moderate-to-severe reduction in GFR occurs [63]. These antimicrobials are suitable for interval adjustment; for instance, the standard q8h interval of cefazolin can be adjusted to q12h in patients with CKD Stage 3. In very severe cases (i.e., serum creatinine > 8.5 mg/dL), the dose interval should be extended at 48 h [64]. Once-daily dosing is recommended for cefotetan at IRIS Stage 3 and administration every other day (EOD) can be recommended at IRIS Stage 4 [64]. Similarly, the risk of nephrotoxic effects should be considered in renal-impaired dogs, especially when associated with aminoglycosides [55,60]. Dose adjustment in cats is recommended in moderate or severe CKD (IRIS stages 3 and 4) [7].
5.4. Sulfonamides
Sulfonamides are bacteriostatic agents for Gram-positive and several species of Gram-negative bacteria. They can be highly bound to serum proteins with possible competitive interactions with other drugs, but the specific extent of binding is species- and drug-dependent. Sulfonamides are excreted via glomerular filtration in their unbound form and through tubular secretion. Metabolism is principally performed by the liver, through acetylation and glucuronidation reactions, but the extra-hepatic metabolism is also involved [60].
Trimethoprim-sulfonamide is a potentiated antimicrobial agent that, in contrast with sulfonamides alone, provides a bactericidal action. The association of trimethoprim with different sulfonamides has been labeled, such as sulfadiazine and sulfamethoxazole. There is considerable controversy regarding the dosage recommendation and frequency of administration of these combinations, due to inconsistencies in the pharmacokinetic data. Furthermore, since different organisms have different MIC values and the optimal ratio of trimethoprim-sulfa also differs from organism to organism, this problem is exacerbated [60,85].
Sulfonamides may induce a variety of adverse effects. Specifically, the possible onset of crystalluria, as a result of the sulfonamide’s precipitation in renal tubules, should be taken into account due to its potential impact on kidney function; thus, although a tubular obstruction has been anecdotally reported in animals receiving sulfonamides, dehydration should be avoided [65]. Since the acetylated metabolites are characterized by a lower solubility, crystallization in the urine can occur with some sulfonamides, particularly in an acidic environment. Prolonged administration and highly concentrated urine may also be contributing factors in the onset of crystalluria, hematuria and renal tubule obstruction [60,85]. In dogs, acetylation reactions do not occur and tubular secretion does not appear to be a major route of elimination, making this species less susceptible to renal tubular damage [55]. Nevertheless, because of the risk of accumulation, they are contraindicated in patients with severe renal impairment (i.e., serum creatine > 8.5 mg/dL) and should also be used with caution in patients with diminished renal function or urinary obstruction. It has been recommended that the normal dose should be halved in dogs at IRIS Stage 4, while no adjustments have been suggested for plasmatic creatinine < 5.0 mg/dL [12,64].
Furthermore, delayed hypersensitivity reactions caused by sulfadiazine, sulfadimethoxine or sulfamethoxazole have primarily been described in dogs [133,134], with a suspected increased susceptibility in Doberman Pinschers [135,136,137]. Glomerulopathy, polymyositis, polyarthritis, dermatological signs, fever, hepatotoxicity and hematological disorders have been encountered as manifestations of hypersensitivity reactions [65]. Acute interstitial nephritis is also reported in isolated case reports [138]. For both sulfonamides alone and the association trimethoprim-sulfonamides, a 50% dose reduction is recommended in cats with moderate or severe CKD [7,64].
5.5. Tetracyclines
Tetracyclines are broad-spectrum bacteriostatic antibiotics. With the exception of doxycycline and minocycline, they are generally excreted unchanged in urine and, to a lesser extent, in bile. It has been shown for tetracycline and oxytetracycline that renal impairment in dogs induces a dramatic decrease in body clearance and the apparent volume of distribution, as well as a prolonged half-life and drug accumulation with repeated dosing [55,60,85]. In advanced CKD, with the exception of doxycycline, the accumulation of tetracyclines and their metabolites can increase the risk of adverse effects [7,55]. Therefore, when indicated, doxycycline has been identified as the tetracycline of choice in these patients because of its lower rate of renal elimination. Minocycline can also be used in patients with moderate renal insufficiency without dosage adjustment, which is required for oliguric renal failure [60].
5.6. Fluoroquinolones
Fluoroquinolones exert bactericidal activity primary against most Gram-negative bacteria, Mycoplasma and some Gram-positive bacteria [55].
Fluoroquinolones undergo renal and non-renal elimination pathways; approximately 15–50% are eliminated unchanged by glomerular filtration and tubular secretion, while a significant proportion is metabolized by both the liver and kidneys and eliminated in feces and urine as a few active metabolites. Approximately 10–40% of circulating enrofloxacin is metabolized to ciprofloxacin in most species, including dogs and cats [55,66]. Due to the dual means of elimination, patients with severely impaired renal function may have slightly prolonged half-lives and higher serum levels, which may not require dosage adjustment [55,139]. In CKD feline patients with moderate disease, an interval extension is recommended because of the high risk of retinopathy at standard therapeutic doses, especially with enrofloxacin [7]; alternatively, less retinotoxic fluoroquinolones, such as marbofloxacin, should be considered [64].
6. Anti-Inflammatory Drugs
6.1. Non-Steroidal Anti-Inflammatory Drugs
Non-steroidal anti-inflammatory drugs (NSAIDs) are largely used in small-animal practice for their anti-inflammatory, antipyretic and analgesic properties [55,67,140,141]. Nevertheless, NSAIDs also have some undesirable effects that can be seen in both therapeutic dose and overdose situations, although the overall incidence of adverse effects in companion animals is not known [67,68,142]. The most commonly reported adverse effects of NSAIDs are gastrointestinal, renal, hepatic, and coagulation disorders [143,144]. NSAIDs are regarded as harmful for patients with CKD and clinical guidelines for humans currently recommend the avoidance of prolonged NSAID use in CKD with GFR > 30 mL/min/1.73 m2 and complete avoidance with GFR < 30 mL/min/1.73 m2 [145,146,147]. NSAID-associated nephrotoxicity is predominantly hemodynamically mediated, resulting in a reversible reduction in renal blood flow (RBF) and/or GFR and in severe cases, acute ischemic tubular injury that may lead to acute kidney injury (AKI) [70,147,148]. In dogs with CKD, RBF maintenance is increasingly dependent on prostaglandins; therefore, the use of NSAIDs increases the risk of renal vasoconstriction thorough a decreased prostaglandins production, meaning that AKI from NSAIDs is more likely to occur in dogs that already have decreased renal function [70].
In order to reduce the incidence and the severity of these complications, several molecules with better safety profiles have been developed over the years. The primary mode of action of NSAIDs is blocking the cellular expression of the enzyme cyclooxygenase (COX) in cell membranes, resulting in diminished prostaglandins (PGs) and thromboxane production. COX-2 selectivity and the sparing of COX-1 were reported as safety factors to reduce NSAIDs… [143]. However, besides its proinflammatory effect, COX-2 has a secondary but important role in the regulation of certain physiological functions, whose inhibition would likely lead to adverse consequences [140]. While COX-2 selectivity seems to be clinically significant in reducing gastrointestinal (GI) adverse reactions, it may have little effect on potential renal toxicity, liver toxicity or coagulative functions. After the GI effects, nephrotoxicity is the second most important NSAIDs safety concern and, since COX-1 and COX-2 are both constitutively present in normal kidneys, seems unrelated to COX selectivity [143,149].
Nonsteroidal anti-inflammatory drugs might negatively affect renal function through the suppression of homeostatic renal PGs; this inhibition is particularly important under hypovolemia and hypotension conditions, such as after trauma or in the perioperative period, due to the risk of developing ischemic injury [143,144].
Non-steroidal anti-inflammatory drugs are generally well-absorbed by the gastrointestinal tract, they are highly bound to plasma proteins and have a low apparent volume of distribution. They undergo hepatic transformation and the excretion of unchanged drug by the kidney is usually low with profound interspecies differences in the elimination half-lives that exist among molecules. In neonates and patients with renal or hepatic disease, the half-lives of NSAIDs are usually increased [55,67]. Non-steroidal, anti-inflammatory drugs are contraindicated in patients with renal insufficiency, dehydration and hypotension, and the concurrent use of other potentially nephrotoxic drugs, such as aminoglycosides, is discouraged [140,143]. Screening and monitoring are essential parts of the judicious use of NSAIDs to identify preexisting pathologic conditions or early signs of adverse effects, especially in older animals and when long-term use is expected [143,150].
Carprofen, deracoxib, firocoxib, grapiprant, meloxicam and robenacoxib are some of the approved molecules for the management of osteoarthritis, perioperative pain and inflammation in dogs; these molecules have all been approved for long-term use, with the exception of robenacoxib. To date, only meloxicam and robenacoxib have been approved in cats for the short-term management of perioperative pain and inflammation [69]. Although the cautious use of NSAIDs is usually recommended in cats due to the limited hepatic glucuronidation, there is a significant body of evidence highlighting their value and safety in this species, particularly concerning newer compounds. While molecules that are mainly metabolized by glucuronidation, such as aspirin, acetaminophen, and carprofen, have relatively prolonged elimination half-lives in cats compared with dogs, drugs cleared by oxidative enzymes, such as piroxicam and meloxicam, have been shown to have similar or reduced half-lives in cats [144]. Furthermore, other NSAIDs elimination pathways have been identified in cats, such as the elimination of unchanged flunixin through organic anion transporters into bile [151], and thioesterification of ketoprofen [152].
Data regarding the nephrotoxicity of NSAIDs in cats or the use of these drugs in feline patients with preexisting renal disease are controversial [153]; however, from the nephrological perspective, all these drugs should be used with extreme caution in renal disease. Despite anecdotal reports of acute renal failure and death associated with the use of meloxicam in cats [67], the short-term administration of NSAIDs seems to be an uncommon cause of nephrotoxicity [154]. Moreover, long-term NSAIDs therapy was found to be safe and effective when administered to cats with osteoarthritis for approximately 6 months [155]. Recent publications suggest that NSAIDs can also be administered to cats with CKD, providing a high level of monitoring and care [156,157,158,159]. Furthermore, recent evidence suggests that the use of NSAIDs in cats with CKD may lead to a slowdown in the progression of the disease, probably due to the direct renal anti-inflammatory effect or to the relief of pain and a subsequent appropriate food and water intake [156]. Nevertheless, a recent publication found that, although low-dose meloxicam administration did not negatively affect the serum creatinine concentration, SDMA or GFR of cats with CKD, it resulted in a worsening of proteinuria [160]. For most of the NSAIDs used in cats, it is unknown if repeated long-term dosing alters the pharmacokinetics or pharmacodynamics of the drug. Since NSAIDs have historically been contraindicated in cats with CKD, no specific recommendations are available for dose adjustment in these patients. General guidelines exist on their rationale long-term use in cats, promoting the cautious adoption of the “lowest effective dose” principle when possible, leaving the frequency of dosing unchanged [7]. As not all cats are satisfactory candidates for long-term NSAIDs therapy, extreme caution is needed before making the decision to treat these patients. Cats must have a stable CKD and the maintenance of proper hydration is paramount [153].
The potential for the development of adverse reactions in dogs is well accepted, with extensive reports of toxicity over the years. Nevertheless, the strength of evidence concerning adverse drug reactions is highly variable among published studies and single NSAIDs. Although the overall incidence of side effects related to the administration of NSAIDs is currently unknown, the most serious adverse effects seem to be rather rare [68]. Acute kidney injury from NSAIDs is more likely to occur in dogs that already have a decreased renal function, probably as a consequence of the increased need for PGs to maintain an adequate RBF [69,70]. In dogs with CKD, concurrent medication that can impair these mechanisms should be considered, such as angiotensin-converting enzyme inhibitors (ACEis), angiotensin receptor blockers (ARBs) or diuretics [70,161,162].
Specific recommendations about dose adjustments of NSAIDs in dogs with CKD are not available, and general guidelines for their judicious administration are commonly observed, such as the use of the lowest effective dose and dose optimization on lean body weight, the avoidance of exposure to additional risk factors (i.e., hypotension, concurrent administration of other potentially nephrotoxic drugs) and an appropriate baseline evaluation of renal function with re-evaluation of laboratory parameters two weeks after initiating treatment [70,163]. Moreover, laboratory monitoring is recommended every 6 months in low-risk patients and every 2–4 months in at-risk patients [164]. Furthermore, observing an adequate washout period (5–7 days) is recommended for cases in which an animal is switched from one NSAID to another or has been treated with corticosteroids, to avoid adverse drug interactions [143]. In the case of long-acting corticosteroids or aspirin, a longer washout period should be considered [164].
6.2. Corticosteroids
Corticosteroids are widely used in veterinary and human medicine due to their potent anti-inflammatory and immunosuppressive effects.
It has been reported that corticosteroids should be avoided in the treatment of uremic dogs because they enhance protein metabolism, worsening azotemia [55]; furthermore, the administration of glucocorticoids has been associated with the onset of proteinuria in dogs without evidence of preexisting glomerular disease [71]. The mechanisms underlying glucocorticoids-induced proteinuria are poorly understood, although glomerular hypertension and ultrastructural alterations to the glomerular barrier have been implied [71,165].
Several studies have also documented that corticosteroids administration induces a rise in serum cystatin C in humans and in canine species [166]. Nevertheless, the clinical significance of these findings remains to be determined.
On the other hand, the administration of immunosuppressive therapy could be considered in dogs with persistent or progressive glomerular disease in which there is renal biopsy-supported evidence of immune-mediated pathogenesis [167]. In these cases, glucocorticoids should be limited to short-term therapy and other immunosuppressive agents should be preferred [72].
7. Antiproteinuric and Antihypertensive Drugs
Renin–angiotensin–aldosterone system (RAAS) inhibitors and calcium channel blockers (CCBs) are the most recommended classes of antihypertensive agents in dogs. Furthermore, RAAS inhibitors are also prescribed as first-line antihypertensive agents in CKD dogs due to their antiproteinuric effect [73]. On the other hand, CCBs and specifically amlodipine besylate have been the first choice for antihypertensive treatment in CKD cats because of their established efficacy [77,168,169]. The potential of antihypertensive agents such as RAAS inhibitors and CCBs to cause hypovolemia and hypotension and induce changes in intrarenal hemodynamics should be carefully taken into account [78]. It is thus advisable that patients receiving antiproteinuric or antihypertensive medications are clinically stable prior to the introduction of these agents, and dehydration should be avoided [72,73].
7.1. Renin-Angiotensin-Aldosterone System (RAAS) Inhibitors
The renin–angiotensin–aldosterone system (RAAS) is essential for the regulation of sodium balance, fluid volume and blood pressure; it is also directly implicated in the progression of hypertension, heart failure and kidney disease [170]. Angiotensin-converting enzyme inhibitors (ACEis) and ARBs selectively inhibit the RAAS and are shown to be particularly beneficial in patients with renal disease, despite a mild increase in renal function markers [73].
The reno-protective effect of ACEis has been linked to the reduction in systemic arterial pressure, glomerular capillary pressure and glomerular volume [171]; thus, they are commonly used in dogs and cats to manage hypertension and proteinuria and their use in CKD patients appears to be safe and related to positive outcomes [72,73,172,173,174,175,176].
Benazepril and its active metabolite, benazeprilat, are largely eliminated by the biliary route, with a smaller fraction being excreted in the urine; impaired renal function does not affect the clearance of this drug in dogs and cats [173,174,177,178]. In contrast, enalapril and its active metabolite, enalaprilat, are primarily eliminated by the kidney, and a 33% reduction in dose may be required in dogs with mild renal impairment [177,179]. Provided that animals are clinically stable and euvolemic before the introduction of ACEis, a severe worsening of azotemia seems to be un uncommon finding. Nevertheless, some caution is warranted when administering an ACEi to a dog or cat in stage 3 or stage 4 CKD; in these cases, a low initial starting dose (i.e., 50% of the total daily dose) followed by small incremental increases may be considered to improve renal tolerance [64,72]. In addition, a close monitoring (3–7 days after starting the therapy) of serum creatinine, potassium and systemic blood pressure should be performed to identify signs of worsening renal function, especially after any dose adjustment or the introduction of other antiproteinuric drugs [72]. Furthermore, the concurrent administration of potentially nephrotoxic drugs such as diuretics or NSAIDs should be carefully evaluated, assessing the risk and benefits [177].
Angiotensin II receptor blockers (ARBs) selectively antagonize the angiotensin II, subtype-1 (AT1) receptor, which mediates the pathologic effects of angiotensin II [74]. Telmisartan is an ARB, currently licensed in Europe for the treatment of feline proteinuria due to CKD, and was recently demonstrated to also be safe and effective for the management of systemic hypertension in feline species [180]. Telmisartan, used at antihypertensive dosages, appeared to be safe in cats with CKD of IRIS stages 1–3, with a low rate of acute exacerbation of renal azotemia noted within a 28-day study period and in a 6-month extended-use phase [74]. Telmisartan was also recently evaluated in dogs as a suitable first-line choice for the treatment of renal proteinuria, providing similar or even better results for reducing UPC in comparison with enalapril [75] and, as observed for cats, it was recently found to also be safe and effective as an antihypertensive agent in CKD dogs [76].
The potential for acute exacerbation of azotemia should be taken into account with the concurrent administration of ACEis and ARB, and careful monitoring is recommended [73].
7.2. Amlodipine
Amlodipine is a potent peripheral arterial dilator belonging to the class of calcium channel blockers (CCBs). These drugs directly act on vascular smooth muscle, causing a reduction in systemic vascular resistance and blood pressure with minimal cardiac effects [181].
Due to its established efficacy, amlodipine has been identified as the first-choice antihypertensive treatment in cats with hypertension and CKD [7,73,77].
The use of CCBs as monotherapy in dogs should be avoided; in fact, the local hypertensive effect of RAAS is not inhibited by CCBs, which preferentially dilate the renal afferent arteriole, potentially exposing the glomerulus to deleterious increases in glomerular capillary hydrostatic pressure. For this reason, ACEis or ARBs that preferentially dilate the renal efferent arteriole should be co-administered with a CCB in dogs [73].
7.3. Other Cardiovascular Drugs
Many drugs commonly used in conditions of cardiac disease, which are primarily excreted by the kidneys, may require close monitoring and dosage adjustments in animals with AKI or CKD [182].
Furosemide is a loop diuretic that decreases the reabsorption of both sodium and chloride and increases the excretion of potassium in the distal renal tubule; it is predominantly excreted by proximal tubular secretion. Furosemide is contraindicated in patients with progressive renal disease or if increases in azotemia and oliguria occur during therapy; it should be also used with caution in patients with preexisting electrolyte or water-balance abnormalities; therefore, the careful monitoring of these variables is recommended [55,60]. Nevertheless, loop diuretics may have conflicting effects on renal function in cardiorenal syndrome (CRS). By reducing renal congestion, they may improve GFR and delay the progression of CKD; on the other hand, excessive doses of diuretics may also decrease renal perfusion and, consequently, GFR. If indicated in these cases, treatment should be established with the appropriate monitoring of renal function. The combination of loop diuretics and thiazide diuretics has a synergistic effect that may cause excessive volume depletion and electrolyte disturbances; therefore, they should be used with caution in azotemic patients with CRS [78]. The concomitant administration of potentially nephrotoxic agents, such as NSAIDs, aminoglycosides and cephalosporins, should be cautiously evaluated [55].
8. Antithrombotic Drugs
Thromboembolism is a well-recognized complication of proteinuria in dogs and humans, although the underlying cause of hypercoagulability in dogs with protein-losing nephropathy (PLN) remains to be elucidated [183,184]. The glomerular loss of antithrombin (AT) and increased platelet aggregation secondary to hypoalbuminemia were observed in dogs with nephrotic syndrome (NS) and identified as possible causes [176,184]. While, in humans with NS, thrombosis is primarily attributed to venous thromboembolism (VTE), no strong evidence is available in dogs regarding the nature of thrombosis in PLN; nevertheless, clinical observations suggest that VTE in dogs may be more common that arterial thromboembolism (ATE) [183].
Antithrombotic therapies are recommended for clot prevention in dogs with PLN [8,185]. According to recent consensus guidelines, anticoagulants seem to be more effective than antiplatelet agents for preventing VTE in dogs [8]. Nevertheless, the mechanism of action of unfractionated heparin (UFH) and low-molecular-weight heparin (LMWH), whose target is AT, should be taken into account. Hence, the response to heparin could be highly variable depending on the AT levels and the severity of the underlying disease; in these cases, monitoring the clotting time (i.e., activated partial thromboplastin time, aPTT) is warranted [79]. Little information is available regarding the use of these drugs in dogs and cats with renal impairment but, since LMWHs are excreted by renal clearance, a prolongation of elimination time should be considered under conditions of reduced renal function [79]. In human patients with stage 4 CKD, a decreased clearance of enoxaparin and drug accumulation occur, leading to an increased half-life, drug exposure and bleeding risk; therefore, a prolongation of dosing intervals from 12 to 24 h is recommended [80].
An uncommon feature that should be considered in patients with renal disease receiving heparin, which could experience imbalances in potassium metabolism, is the heparin-induced hyperkalemia. This syndrome is related to the transient suppression of aldosterone synthesis that resolves after heparin discontinuation. It has been observed in humans receiving UFH and LMWH and also been reported in a dog with CKD [186].
Conversely to anticoagulants, the use of antiplatelet drugs such as low doses of acetylsalicylic acid and clopidogrel has been extensively described for thromboprophylaxis in dogs with PLN [41,176,183].
Acetylsalicylic acid or aspirin is an NSAID used as antiplatelet drug at low dosages, and it has been recommended for thromboprophylaxis in glomerular diseases due to its anti-inflammatory effects, which could have a role in reducing disease progression [41,176,183]; at low doses, aspirin may be more effective in inhibiting COX-1 and suppressing the production of thromboxane (TXA2) [85].
The use of low-dose aspirin in renal disease in humans with CKD rises some concerns related to the potential inhibition of renal prostaglandins, which could lead to a further deterioration in renal function [80]; moreover, several studies have shown potential risks in elderly patients and those with CKD [81,82,83,84].
On the other hand, no controlled clinical studies documenting the efficacy of low-dose aspirin are available in animals [85]. The therapeutic index of acetylsalicylic acid is narrow and, similarly to other NSAIDs, caution should be used under conditions of renal hypoperfusion [86]. According to these considerations, the concomitant administration of other NSAIDs should be avoided in these patients and renal function should be monitored.
The prevalence of PLN seems to be lower in cats and, conversely to dogs, there is no evidence supporting the adoption of antithrombotic medications [8,185,187]. Although it is not licensed for use in cats and its efficacy remains unproven, acetylsalicylic acid at low doses has been encountered as antiplatelet agent in cats for the prevention of thrombosis and in particular ATE; reported dosages range widely (i.e., 5–80 mg per cat every 72 h), and special attention should be paid to the prolonged time of excretion in feline species [85,86]. Since clopidogrel was shown to be more effective than aspirin in reducing the likelihood of recurrent cardiogenic ATE [188], recent consensus guidelines on the rational use of antithrombotic recommend using clopidogrel rather than aspirin in cats when required [8].
Clopidogrel is a platelet inhibitor belonging to the class of thienopyridines that inhibits diphosphate (ADP)-receptor-mediated platelet activity [85]. The pharmacokinetics of clopidogrel is influenced by genetic polymorphisms in the genes encoding for cytochrome (CYP) 2C19, determining a high inter-individual variability in treatment response [89]. Although dose adjustment seems to be unnecessary under conditions of reduced renal function, therapeutic experience with clopidogrel is limited in human patients with advanced CKD [80,87,88]. Concerns exist regarding the benefits deriving from the use of clopidogrel in CKD patients and, specifically, in end-stage kidney disease (ESKD). Hence, a lower antiplatelet effect of clopidogrel was observed in CKD patients [90] and has been associated with an increased risk of death, death from bleeding, and hospitalization for bleeding in patients with ESKD [88]; as a result, the summary of product characteristics of clopidogrel recommends caution when using clopidogrel in the CKD population [80]. Clinical studies on clopidogrel in dogs and cats with CKD are lacking; according to a recent study, no differences in clopidogrel metabolite concentrations were found between healthy dogs and those with PLN and early CKD stages, suggesting that the drug’s metabolism is not altered in these patients [91]. Nevertheless, caution should be adopted when administering clopidogrel in dogs and cats with advanced CKD.
Although a combined administration of clopidogrel and aspirin can be used, due to their different mechanisms of action, an increased risk of gastrointestinal side effects has been reported in humans and is also likely to occur in animals [189].
9. Gastroprotectants, Antiemetics and Appetite Stimulants
The gastrointestinal complications of CKD, including nausea, vomiting, uremic stomatitis and gastrointestinal erosions, are common in dogs and cats with advanced renal disease. The treatment of these complications is largely symptomatic and include the administration of specific drugs to limit gastric acidity, suppress nausea and vomiting and provide mucosal protection [1].
Oral antacids comprise a group of inorganic and relatively insoluble salts of aluminum hydroxide, calcium carbonate and magnesium hydroxide that lack systemic effects [190]. In renal failure, magnesium and aluminum accumulation may be a problem and aluminum toxicity has been documented in dogs with advanced renal failure [92,191]. Further concerns related to these drugs arise from their interference with the absorption of concurrent orally administered medications [40].
Histamine type-2 receptor antagonists (H2RAs) include cimetidine, ranitidine and famotidine, which exert their action through the inhibition of acid secretion by competitively blocking H2 receptors on the gastric parietal cells. Dose adjustments of H2RAs based on GFR are recommended in humans because of the renal elimination of these drugs. Mental status changes and other central nervous system disturbances disturbances have been reported in people with decreased GFR when receiving H2 without appropriate dose reductions [93]. Although no specific indications are available in dogs and cats [94], either a dose reduction or extended dosing interval can be used at IRIS Stages 3 and 4.
Omeprazole, pantoprazole, esomeprazole and lansoprazole are classified as proton-pump inhibitors (PPIs) and are identified as first-choice treatments of acid-related gastrointestinal ulceration and erosion. Retrospective reports have linked PPIs to acute interstitial nephritis, AKI and CKD in people but the quality of evidence underlying this association, as well as for other adverse effects, is consistently low in dogs and cats [94,95,96,192,193]. To date, there is no evidence supporting the prophylactic use of gastroprotectants in dogs and cats with CKD IRIS stage 1–3 and additional studies are warranted to determine the benefits of acid suppression in animals with IRIS stage 4 disease; no dose adjustment is required in patients with renal impairment [94].
Sucralfate is a complex salt of sucrose octasulfate and aluminum hydroxide that provide protection of the damaged mucosa through the formation of stable complexes with proteins in an acidic environment [194]. Although sucralfate is a relatively safe compound with minimal adverse effects, caution should be used with long-term treatment in patients with renal insufficiency to avoid aluminum intoxication; moreover, the possible influence on the absorption of other orally administrated drugs should be considered [195,196].
Metoclopramide is a dopamine receptor antagonist, widely used in dogs and cats, to stimulate the stomach and upper-small-intestine motility. This action helps prevent esophageal reflux and move ingesta from the stomach into the intestine. Metoclopramide is also used in dogs and, less commonly, in cats to treat nausea [60]. The use of this drug at standard constant rate infusion dosages (1–2 mg/kg/day) may cause tremor and ataxia in azotemic patients. The dose could be reduced by up to the 25–50% of the standard dose and titrate to a dosage that elicits a therapeutic effect without tremor [64].
Maropitant is a selective neurokinin-1 (NK-1) receptor antagonist whose mechanism of action is to effectively block the binding of emetic-eliciting substance P, the most potent tachykinin, at the NK-1 receptor. It is highly bound to plasma proteins in dogs and cats, and is mainly excreted by the liver; thus, it is recommended to use it with caution with other highly protein-bound medications and in patients with hepatic dysfunction. Maropitant is safe and effective in the treatment of vomiting induced by several conditions in dogs, including motion sickness, and preventing vomiting induced by chemotherapy [97,98,197,198]; it was also shown to be safe and effective in cats and daily administration orally for 2 weeks resulted in a statistically significant decrease in vomiting in cats with CKD [99,199].
Ondansetron is a 5HT3 receptor antagonist used for severe vomiting in dogs and cats. No canine data are available for ondansetron pharmacokinetics, while, in cats, subcutaneous bioavailability was found to be prolonged (3.2 h) in comparison with oral and intravenous routes [200]. Ondansetron is extensively metabolized by the liver. The pharmacokinetics of ondansetron was evaluated in healthy geriatric cats, cats with CKD and liver disease, finding no significant differences between healthy geriatric cats and those with renal disease [100]. Thus, renal dysfunction seems unlikely to affect the pharmacokinetics of ondansetron in these patients [100].
Mirtazapine
Mirtazapine is used as oral or transdermal formulation for nutritional support in both dogs and cats with acute and chronic illness.
The mechanisms of action include antagonism of the serotonin 2C (5HT2C) and histamine 1 (H1) receptors, both of which are involved in appetite regulation, and an antiemetic action through the inhibition of serotonin 3 receptor (5HT3) [103,201,202,203]. Due to its high affinity for 5HT3, competition with 5HT3-receptor antagonists (e.g., ondansetron) should be considered when choosing antiemetic and anti-nausea regimens.
The efficacy of mirtazapine as an appetite stimulant has been thoroughly studied in cats. In feline patients with CKD, it provides significative appetite stimulation and weight gain [101,103,201,204,205,206]. The half-life of oral mirtazapine is prolonged in elderly cats (12.1 h) and cats with CKD (15.2 h) and/or liver disease (15.1 h) [101,207]. There are differences in pharmacokinetics among formulations, with a lower mean peak and total plasma concentration recorded with a transdermal ointment than oral dosing [208]. The most commonly reported adverse effects include neurologic signs, agitation, vocalization, hypersalivation, tachypnea, tachycardia and lethargy, and were more commonly reported in cats receiving 3.75 mg than in cats receiving 1.88 mg; therefore, the lower dosage seems to be more appropriate as a starting dose [102,103]. Given the prolonged half-life of mirtazapine in CKD cats, oral administration of the medication every 48 h is recommended [101]. To minimize its adverse effects, the dosage should be titrated to the lowest effective dose for appetite stimulation with both the oral and transdermal formulations. The recommendations provided by the manufacturer of a transdermal formulation (Mirataz 20 mg/g, Dechra Veterinary Products®) state that the product has not been studied in patients with severe CKD and for a treatment duration of longer than 14 days; nevertheless, a good safety and efficacy profile was recently shown in a study evaluating the clinical efficacy of mirtazapine in cats with stage 2 and 3 CKD, receiving a compounded transdermal formulation for 21 days [206]. Side effects reported by the manufacturer include vomiting, polyuria and an increase in BUN consequent to dehydration.
Fewer studies regarding the use of mirtazapine have been conducted in dogs, with limited evidence supporting it as an appetizing agent in comparison with feline species. The suggested dose interval for dogs is 0.6–1 mg/kg every 12 h, but studies evaluating pharmacokinetic properties in dogs with renal disease have not been conducted to date [104].
10. Antileishmanial Drugs
Canine leishmaniasis is a common cause of glomerulopathy (particularly glomerulonephritis), which can cause proteinuria and progressive chronic kidney disease [113,209,210,211,212]. When leishmaniosis-induced kidney disease is identified, together with an active form of the disease, specific treatment should be started immediately, either alone or together with the standard treatment for CKD. Nevertheless, treatment should be tailored to each individual case and the risk-to-benefit ratio should be carefully considered [113,213].
The association of meglumine antimoniate and allopurinol is the most widely described and effective treatment for leishmaniosis; when this regimen is not feasible, the alternative combination of miltefosine and allopurinol could be administered [214,215]. All these drugs may improve the patient’s clinical condition and prevent the progression of kidney disease [106,216,217,218]. Although nephrotoxicity is a recognized side effect of antimonials, no impact on kidney function was observed in dogs treated with meglumine antimoniate and the only reported evidence of pathological renal damage (mainly tubular lesions) was not associated with clinical or clinicopathological alterations [105,106,107]. Nevertheless, the manufacturer of a veterinary formulation (Glucantime, Boehringer Ingelheim® Ingelheim, Germany) recommends reducing dosage in the case of renal impairment and monitoring serum creatinine and proteinuria during treatment; administration in cases of severe renal insufficiency is discouraged.
Miltefosine is generally considered a second-line treatment for canine leishmaniosis; it shows a good safety profile and seems to have a low impact on renal function. The only reported adverse effects are transient gastrointestinal signs such as vomiting and diarrhea.
Allopurinol is a purine analogue leishmaniostatic agent used to treat canine leishmaniosis over long periods to maintain a low parasite load. Xanthine urolithiasis, which can potentially result in kidney mineralization, was observed with a prolonged therapy [113,219]. Given xanthine lithiasis’ potential impact on kidney function (particularly when the upper urinary tract is involved), a closer follow-up through urinalysis and ultrasound is required to detect the early onset of such an adverse effect. If xanthine uroliths were detected or suspected, the dose of allopurinol can be reduced to 10 mg/kg once a day or less [113,213,214] and other approaches to minimize xanthine-associated crystalluria can be started (e.g., increase in water intake, specific purine-restricted diets, urine alkalinization).
Many dogs with leishmaniosis may also require antiproteinuric treatment, which should be based on the available guidelines, considering the previously discussed remarks on renal impairment [214,220].
Leishmaniasis in cats is a possible underestimated cause of renal disease. According to the limited information available on treatment regimens, which is mostly based on single case reports, the same protocols that are used in dogs are generally prescribed in cats [221,222]. However, it should be specified that the efficacy and safety of these protocols have never been evaluated in feline-controlled studies and cats, particularly those affected by renal disease, should be monitored very carefully for adverse effects during treatment. The administration of allopurinol was found to be associated with the onset of acute of kidney injury in cats [114], while no nephrotoxicity was recorded for meglumine antimoniate or miltefosine [223].
11. Conclusions
Practical guidelines on dosage adjustment regimens seem to be lacking in the veterinary literature and most of the available indications are based on the measurement of GFR by means of plasma clearance methods. In contrast to humans, the assessment of GFR in dogs and cats is generally not performed in clinical practice for both financial and practical reasons and, to date, it is mainly performed in research settings. Typically, dose adjustments in humans are made when GFR drops to approximatively 0.7 mL/kg/min, roughly equivalent to a serum creatinine of 3.5 mg/dL in cats. On the other hand, data in dogs are still lacking and equivalent dose adjustment studies are warranted in both species. For these reasons, the recommendations for dosage adjustment based on indirect tests evaluating kidney function and reflecting the severity of the CKD can be extrapolated from human studies and adapted from expert opinion. Practical dose adjustments of drugs characterized by a high therapeutic index should be taken into account from IRIS stage 3, while drugs with a narrow therapeutic window could require dosage adjustments at an earlier stage (i.e., IRIS stages 2) (Figure 1). Moreover, given the lack of safety studies in CKD populations, specific recommendations regarding dosage adjustment are seldom provided by manufacturers. As a result, potentially nephrotoxic drugs might not be prescribed in patients with renal impairment even if they are clearly required, with a possible negative impact on treatment outcomes and quality of life.
In conclusion, treatment decisions should always be made on a case-by-case basis, assessing risks and benefits; the severity of the disease and the effective need for a given medication should be carefully evaluated. Furthermore, indications provided by the manufacturers should be integrated and compared with the available literature to obtain a more complete overview of the decision-making process.
From a future perspective, prospective clinical trials evaluating the efficacy and safety of specific medications in dogs and cats with various stages of CKD could help to provide practical guidelines for dosage adjustment in veterinary medicine.
Author Contributions
Conceptualization, F.D.S., A.B., F.D. and P.E.C.; writing—original draft preparation, F.D.S.; writing—review and editing, A.B., F.D. and P.E.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Polzin, D.J. Chronic Kidney Disease in Small Animals. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 15–30. [Google Scholar] [CrossRef]
- Brown, S.A. Management of Chronic Kidney Disease. In BSAVA Manual of Canine and Feline Nephrology and Urology; British Small Animal Veterinary Association, Ed.; British Small Animal Veterinary Association: Gloucs, UK, 2007; ISBN 978-0905214931. [Google Scholar]
- Polzin, D.J. Chronic Kidney Disease. In Nephrology and Urology of Small Animals; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2011; ISBN 978-0-8138-1717-0. [Google Scholar]
- Marino, C.L.; Lascelles, B.D.X.; Vaden, S.L.; Gruen, M.E.; Marks, S.L. Prevalence and Classification of Chronic Kidney Disease in Cats Randomly Selected from Four Age Groups and in Cats Recruited for Degenerative Joint Disease Studies. J. Feline Med. Surg. 2014, 16, 465–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roudebush, P.; Polzin, D.J.; Adams, L.G.; Towell, T.L.; Forrester, S.D. An Evidence-Based Review of Therapies for Canine Chronic Kidney Disease. J. Small Anim. Pract. 2010, 51, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Polzin, D.J. Evidence-Based Step-Wise Approach to Managing Chronic Kidney Disease in Dogs and Cats: Managing Chronic Kidney Disease. J. Vet. Emerg. Crit. Care 2013, 23, 205–215. [Google Scholar] [CrossRef]
- Sparkes, A.H.; Caney, S.; Chalhoub, S.; Elliott, J.; Finch, N.; Gajanayake, I.; Langston, C.; Lefebvre, H.P.; White, J.; Quimby, J. ISFM Consensus Guidelines on the Diagnosis and Management of Feline Chronic Kidney Disease. J. Feline Med. Surg. 2016, 18, 219–239. [Google Scholar] [CrossRef]
- Goggs, R.; Bacek, L.; Bianco, D.; Koenigshof, A.; Li, R.H.L. Consensus on the Rational Use of Antithrombotics in Veterinary Critical Care (CURATIVE): Domain 2-Defining Rational Therapeutic Usage. J. Vet. Emerg. Crit. Care 2019, 29, 49–59. [Google Scholar] [CrossRef] [Green Version]
- Tett, S.E.; Kirkpatrick, C.M.J.; Gross, A.S.; McLachlan, A.J. Principles and Clinical Application of Assessing Alterations in Renal Elimination Pathways. Clin. Pharmacokinet. 2003, 42, 1193–1211. [Google Scholar] [CrossRef]
- Lea-Henry, T.N.; Carland, J.E.; Stocker, S.L.; Sevastos, J.; Roberts, D.M. Clinical Pharmacokinetics in Kidney Disease: Fundamental Principles. CJASN 2018, 13, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Verbeeck, R.K.; Musuamba, F.T. Pharmacokinetics and Dosage Adjustment in Patients with Renal Dysfunction. Eur. J. Clin. Pharm. 2009, 65, 757–773. [Google Scholar] [CrossRef]
- Riviere, J.E.; Vaden, S.L. Drug Therapy during Renal Disease and Renal Failure. In Canine and Feline Nephrology and Urology; Williams and Wilkins: Philadelphia, PA, USA, 1995; ISBN 0683066668. [Google Scholar]
- Albarellos, G.A.; Landoni, M.F. Current Concepts on the Use of Antimicrobials in Cats. Vet. J. 2009, 180, 304–316. [Google Scholar] [CrossRef]
- Linnetz, E.H.; Graves, T.K. Glomerular Filtration Rate in General Small Animal Practice. Compend. Contin. Educ. Vet. 2010, 32, E1–E5. [Google Scholar]
- Lefebvre, H.P. Renal Function Testing. In Nephrology and Urology of Small Animals; Wiley-Blackwell: Hoboken, NJ, USA, 2011; ISBN 978-0-8138-1717-0. [Google Scholar]
- Pressler, B.M. Clinical Approach to Advanced Renal Function Testing in Dogs and Cats. Clin. Lab. Med. 2015, 35, 487–502. [Google Scholar] [CrossRef] [PubMed]
- McKenna, M.; Pelligand, L.; Elliott, J.; Walker, D.; Jepson, R. Clinical Utility of Estimation of Glomerular Filtration Rate in Dogs. J. Vet. Intern. Med. 2020, 34, 195–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pocar, P.; Scarpa, P.; Berrini, A.; Cagnardi, P.; Rizzi, R.; Borromeo, V. Diagnostic Potential of Simplified Methods for Measuring Glomerular Filtration Rate to Detect Chronic Kidney Disease in Dogs. J. Vet. Intern. Med. 2019, 33, 2105–2116. [Google Scholar] [CrossRef] [PubMed]
- Von Hendy-Willson, V.E.; Pressler, B.M. An Overview of Glomerular Filtration Rate Testing in Dogs and Cats. Vet. J. 2011, 188, 156–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, S.A.; Finco, D.R.; Boudinot, F.D.; Wright, J.; Taver, S.L.; Cooper, T. Evaluation of a Single Injection Method, Using Iohexol, for Estimating Glomerular Filtration Rate in Cats and Dogs. Am. J. Vet. Res. 1996, 57, 105–110. [Google Scholar] [PubMed]
- Bexfield, N.H.; Heiene, R.; Gerritsen, R.J.; Risøen, U.; Eliassen, K.A.; Herrtage, M.E.; Michell, A.R. Glomerular Filtration Rate Estimated by 3-Sample Plasma Clearance of Iohexol in 118 Healthy Dogs. J. Vet. Intern. Med. 2008, 22, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Heiene, R.; Reynolds, B.S.; Bexfield, N.H.; Larsen, S.; Gerritsen, R.J. Estimation of Glomerular Filtration Rate via 2- and 4-Sample Plasma Clearance of Iohexol and Creatinine in Clinically Normal Cats. Am. J. Vet. Res. 2009, 70, 176–185. [Google Scholar] [CrossRef]
- Heiene, R.; Moe, L. Pharmacokineatic Aspects of Measurement of Glomerular Filtration Rate in the Dog: A Review. J. Vet. Intern. Med. 1998, 12, 401–414. [Google Scholar] [CrossRef]
- Sargent, H.J.; Elliott, J.; Jepson, R.E. The New Age of Renal Biomarkers: Does SDMA Solve All of Our Problems? J. Small Anim. Pr. 2021, 62, 71–81. [Google Scholar] [CrossRef]
- IRIS Kidney—Guidelines—IRIS Staging of CKD. Available online: http://www.iris-kidney.com/guidelines/staging.html (accessed on 10 October 2021).
- Finco, D.R.; Brown, S.A.; Crowell, W.A.; Barsanti, J.A. Exogenous Creatinine Clearance as a Measure of Glomerular Filtration Rate in Dogs with Reduced Renal Mass. Am. J. Vet. Res. 1991, 52, 1029–1032. [Google Scholar]
- Finch, N. Measurement of Glomerular Filtration Rate in Cats: Methods and Advantages over Routine Markers of Renal Function. J. Feline Med. Surg. 2014, 16, 736–748. [Google Scholar] [CrossRef] [PubMed]
- Nabity, M.B.; Lees, G.E.; Boggess, M.M.; Yerramilli, M.; Obare, E.; Yerramilli, M.; Rakitin, A.; Aguiar, J.; Relford, R. Symmetric Dimethylarginine Assay Validation, Stability, and Evaluation as a Marker for the Early Detection of Chronic Kidney Disease in Dogs. J. Vet. Intern. Med. 2015, 29, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.P.; Lefebvre, H.P.; Watson, A.D.J. Creatinine in the Dog: A Review. Vet. Clin. Pathol. 2003, 32, 162–179. [Google Scholar] [CrossRef]
- Barsanti, J.A. Urinary Disorders. In Small Animal Clinical Diagnosis by Laboratory Methods; Elsevier: Amsterdam, The Netherlands, 2012; ISBN 978-1-4377-0657-4. [Google Scholar]
- Wamsley, H.; Alleman, R. Complete Urinalysis. In BSAVA Manual of Canine and Feline Nephrology and Urology; British Small Animal Veterinary Association: Gloucester, UK, 2017; ISBN 978-1-905319-94-7. [Google Scholar]
- Adams, L.G.; Polzin, D.J.; Osborne, C.A.; O’Brien, T.D. Effects of Dietary Protein and Calorie Restriction in Clinically Normal Cats and in Cats with Surgically Induced Chronic Renal Failure. Am. J. Vet. Res. 1993, 54, 1653–1662. [Google Scholar]
- Kielstein, J.T.; Salpeter, S.R.; Bode-Boeger, S.M.; Cooke, J.P.; Fliser, D. Symmetric Dimethylarginine (SDMA) as Endogenous Marker of Renal Function—A Meta-Analysis. Nephrol. Dial. Transpl. 2006, 21, 2446–2451. [Google Scholar] [CrossRef] [Green Version]
- Bedford, M.T.; Clarke, S.G. Protein Arginine Methylation in Mammals: Who, What, and Why. Mol. Cell 2009, 33, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, J.A.; Yerramilli, M.; Obare, E.; Yerramilli, M.; Melendez, L.D.; Jewell, D.E. Relationship between Lean Body Mass and Serum Renal Biomarkers in Healthy Dogs. J. Vet. Intern. Med. 2015, 29, 808–814. [Google Scholar] [CrossRef]
- Yerramilli, M.; Farace, G.; Quinn, J.; Yerramilli, M. Kidney Disease and the Nexus of Chronic Kidney Disease and Acute Kidney Injury. Vet. Clin. N. Am. Small Anim. Pract. 2016, 46, 961–993. [Google Scholar] [CrossRef]
- Hall, J.A.; Yerramilli, M.; Obare, E.; Yerramilli, M.; Jewell, D.E. Comparison of Serum Concentrations of Symmetric Dimethylarginine and Creatinine as Kidney Function Biomarkers in Cats with Chronic Kidney Disease. J. Vet. Intern. Med. 2014, 28, 1676–1683. [Google Scholar] [CrossRef] [Green Version]
- Doogue, M.P.; Polasek, T.M. Drug Dosing in Renal Disease. Clin. Biochem. Rev. 2011, 32, 69–73. [Google Scholar] [PubMed]
- Roberts, D.M.; Sevastos, J.; Carland, J.E.; Stocker, S.L.; Lea-Henry, T.N. Clinical Pharmacokinetics in Kidney Disease: Application to Rational Design of Dosing Regimens. CJASN 2018, 13, 1254–1263. [Google Scholar] [CrossRef]
- Papich, M. Drugs for Treating Gastrointestinal Diseases. In Veterinary Pharmacology and Therapeutics; Wiley-Blackwell: Hoboken, NJ, USA, 2018; pp. 1245–1277. ISBN 978-1-118-85588-1. [Google Scholar]
- Littman, M.P. Protein-Losing Nephropathy in Small Animals. Vet. Clin. N. Am. Small Anim. Pr. 2011, 41, 31–62. [Google Scholar] [CrossRef] [PubMed]
- Jansen, J.; Jankowski, J.; Gajjala, P.R.; Wetzels, J.F.M.; Masereeuw, R. Disposition and Clinical Implications of Protein-Bound Uremic Toxins. Clin. Sci. 2017, 131, 1631–1647. [Google Scholar] [CrossRef] [PubMed]
- Riviere, J.E. Pharmacokinetics. In Veterinary Pharmacology and Therapeutics; Wiley-Blackwell: Hoboken, NJ, USA, 2017; ISBN 978-1-118-85588-1. [Google Scholar]
- Santana Machado, T.; Poitevin, S.; Paul, P.; McKay, N.; Jourde-Chiche, N.; Legris, T.; Mouly-Bandini, A.; Dignat-George, F.; Brunet, P.; Masereeuw, R.; et al. Indoxyl Sulfate Upregulates Liver P-Glycoprotein Expression and Activity through Aryl Hydrocarbon Receptor Signaling. J. Am. Soc. Nephrol. 2018, 29, 906–918. [Google Scholar] [CrossRef]
- Bricker, N.S.; Morrin, P.A.F.; Kime, S.W. The Pathologic Physiology of Chronic Bright’s Disease. Am. J. Med. 1960, 28, 77–98. [Google Scholar] [CrossRef]
- Pradhan, S.; Duffull, S.B.; Walker, R.J.; Wright, D.F.B. The Intact Nephron Hypothesis as a Model for Renal Drug Handling. Eur. J. Clin. Pharm. 2019, 75, 147–156. [Google Scholar] [CrossRef]
- Bonate, P.L.; Reith, K.; Weir, S. Drug Interactions at the Renal Level: Implications for Drug Development. Clin. Pharmacokinet. 1998, 34, 375–404. [Google Scholar] [CrossRef]
- Sun, H.; Huang, Y.; Frassetto, L.; Benet, L.Z. Effects of Uremic Toxins on Hepatic Uptake and Metabolism of Erythromycin. Drug Metab. Dispos. 2004, 32, 1239–1246. [Google Scholar] [CrossRef] [Green Version]
- Michaud, J.; Dubé, P.; Naud, J.; Leblond, F.A.; Desbiens, K.; Bonnardeaux, A.; Pichette, V. Effects of Serum from Patients with Chronic Renal Failure on Rat Hepatic Cytochrome P450: Human Uremic Serum Downregulates Cytochrome P450. Br. J. Pharmacol. 2005, 144, 1067–1077. [Google Scholar] [CrossRef] [Green Version]
- Lefebvre, H.P. Dosage Regimen Adjustment in Renal Failure: Why, When and How. Ph.D. Thesis, National Veterinary School of Toulouse, Toulouse, France, 2002. [Google Scholar]
- Gabardi, S.; Abramson, S. Drug Dosing in Chronic Kidney Disease. Med. Clin. N. Am. 2005, 89, 649–687. [Google Scholar] [CrossRef] [PubMed]
- Swan, S.K.; Bennett, W.M. Drug Dosing Guidelines in Patients with Renal Failure. West. J. Med. 1992, 156, 633–638. [Google Scholar] [PubMed]
- Wiebe, V.J. Drug Therapy for Infectious Diseases of the Dog and Cat: Wiebe/Drug Therapy for Infectious Diseases of the Dog and Cat; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015; ISBN 978-1-118-91116-7. [Google Scholar]
- Drug Dose Adjustments for Disease (Proceedings). Available online: https://www.dvm360.com/view/drug-dose-adjustments-disease-proceedings (accessed on 10 October 2021).
- Lefebvre, H.P.; Braun, J.P.; Toutain, P.L. Drug Prescription in Renal-Impaired Dogs. Rev. Méd. Vét. 1996, 147, 757–782. [Google Scholar]
- Hornum, M.; Feldt-Rasmussen, B. Drug Dosing and Estimated Renal Function—Any Step Forward from Effersoe? Nephron 2017, 136, 268–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aloy, B.; Launay-Vacher, V.; Bleibtreu, A.; Bortolotti, P.; Faure, E.; Filali, A.; Gauzit, R.; Gilbert, M.; Lesprit, P.; Mahieu, R.; et al. Antibiotics and Chronic Kidney Disease: Dose Adjustment Update for Infectious Disease Clinical Practice. Méd. Mal. Infect. 2020, 50, 323–331. [Google Scholar] [CrossRef]
- Boothe, D.M. Therapeutic Drug Monitoring. In Small Animal Clinical Diagnosis by Laboratory Methods; Elsevier: St. Louis, MO, USA, 2012; ISBN 978-1-4377-0657-4. [Google Scholar]
- Groman, R.P. Aminoglycosides. In Small Animal Critical Care Medicine; Elsevier Health Sciences: Amsterdam, The Netherlands, 2014; ISBN 978-1-4557-0306-7. [Google Scholar]
- Plumb, D.C. Plumb’s Veterinary Drug Handbook, 8th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2015; Volume 93, ISBN 978-1-118-91192-1. [Google Scholar]
- Monaghan, K.N.; Labato, M.A.; Papich, M.G. Ampicillin Pharmacokinetics in Azotemic and Healthy Dogs. J. Vet. Intern. Med. 2021, 35, 987–992. [Google Scholar] [CrossRef]
- Benson, K.K.; Quimby, J.M.; Dowers, K.L.; Sieberg, L.G.; Daniels, J.B.; Langston, C.E.; Lunghofer, P.J.; Gustafson, D.L. Pilot Study of Side Effects and Serum and Urine Concentrations of Amoxicillin–Clavulanic Acid in Azotemic and Non-Azotemic Cats. J. Feline Med. Surg. 2020, 22, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Matzke, G.R.; Aronoff, G.R.; Atkinson, A.J.; Bennett, W.M.; Decker, B.S.; Eckardt, K.-U.; Golper, T.; Grabe, D.W.; Kasiske, B.; Keller, F.; et al. Drug Dosing Consideration in Patients with Acute and Chronic Kidney Disease—A Clinical Update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2011, 80, 1122–1137. [Google Scholar] [CrossRef] [Green Version]
- Trepanier, L.A. Applying Pharmacokinetics to Veterinary Clinical Practice. Vet. Clin. N. Am. Small Anim. Pract. 2013, 43, 1013–1026. [Google Scholar] [CrossRef]
- Papich, M.G. Sulfonamides and Potentiated Sulfonamides. In Veterinary Pharmacology and Therapeutics; Wiley-Blackwell: Hoboken, NJ, USA, 2017; ISBN 978-1-118-85588-1. [Google Scholar]
- Trouchon, T.; Lefebvre, S. A Review of Enrofloxacin for Veterinary Use. OJVM 2016, 06, 40–58. [Google Scholar] [CrossRef] [Green Version]
- McLean, M.K.; Khan, S.A. Toxicology of Frequently Encountered Nonsteroidal Anti-Inflammatory Drugs in Dogs and Cats. Vet. Clin. N. Am. Small Anim. Pract. 2018, 48, 969–984. [Google Scholar] [CrossRef]
- Monteiro-Steagall, B.P.; Steagall, P.V.M.; Lascelles, B.D.X. Systematic Review of Nonsteroidal Anti-Inflammatory Drug-Induced Adverse Effects in Dogs. J. Vet. Intern. Med. 2013, 27, 1011–1019. [Google Scholar] [CrossRef] [PubMed]
- Papich, M.G. An Update on Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) in Small Animals. Vet. Clin. N. Am. Small Anim. Pract. 2008, 38, 1243–1266. [Google Scholar] [CrossRef] [PubMed]
- Lomas, A.L.; Grauer, G.F. The Renal Effects of NSAIDs in Dogs. J. Am. Anim. Hosp. Assoc. 2015, 51, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Waters, C.B.; Adams, L.G.; Scott-Moncrieff, J.C.; DeNicola, D.B.; Snyder, P.W.; White, M.R.; Gasparini, M. Effects of Glucocorticoid Therapy on Urine Protein-to-Creatinine Ratios and Renal Morphology in Dogs. J. Vet. Intern. Med. 1997, 11, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Vaden, S.L.; Elliott, J. Management of Proteinuria in Dogs and Cats with Chronic Kidney Disease. Vet. Clin. N. Am. Small Anim. Pract. 2016, 46, 1115–1130. [Google Scholar] [CrossRef] [Green Version]
- Acierno, M.J.; Brown, S.; E. Coleman, A.; E. Jepson, R.; Papich, M.; L. Stepien, R.; M. Syme, H. ACVIM Consensus Statement: Guidelines for the Identification, Evaluation, and Management of Systemic Hypertension in Dogs and Cats. J. Jpn. Assoc. Vet. Nephrol. Urol. 2020, 12, 30–49. [Google Scholar] [CrossRef]
- Coleman, A.E.; Brown, S.A.; Traas, A.M.; Bryson, L.; Zimmering, T.; Zimmerman, A. Safety and Efficacy of Orally Administered Telmisartan for the Treatment of Systemic Hypertension in Cats: Results of a Double-blind, Placebo-controlled, Randomized Clinical Trial. J. Vet. Intern. Med. 2019, 33, 478–488. [Google Scholar] [CrossRef]
- Lourenço, B.N.; Coleman, A.E.; Brown, S.A.; Schmiedt, C.W.; Parkanzky, M.C.; Creevy, K.E. Efficacy of Telmisartan for the Treatment of Persistent Renal Proteinuria in Dogs: A Double-masked, Randomized Clinical Trial. J. Vet. Intern. Med. 2020, 34, 2478–2496. [Google Scholar] [CrossRef]
- Miyagawa, Y.; Akabane, R.; Sakatani, A.; Ogawa, M.; Nagakawa, M.; Miyakawa, H.; Takemura, N. Effects of Telmisartan on Proteinuria and Systolic Blood Pressure in Dogs with Chronic Kidney Disease. Res. Vet. Sci. 2020, 133, 150–156. [Google Scholar] [CrossRef]
- Taylor, S.S.; Sparkes, A.H.; Briscoe, K.; Carter, J.; Sala, S.C.; Jepson, R.E.; Reynolds, B.S.; Scansen, B.A. ISFM Consensus Guidelines on the Diagnosis and Management of Hypertension in Cats. J. Feline Med. Surg. 2017, 19, 288–303. [Google Scholar] [CrossRef]
- Orvalho, J.S.; Cowgill, L.D. Cardiorenal Syndrome. Vet. Clin. N. Am. Small Anim. Pract. 2017, 47, 1083–1102. [Google Scholar] [CrossRef]
- Papich, M.G. Anticoagulant, Antiplatelet, and Hemostatic Drugs. In Veterinary Pharmacology and Therapeutics; Wiley-Blackwell: Hoboken, NJ, USA, 2018; ISBN 978-1-118-85588-1. [Google Scholar]
- Capodanno, D.; Angiolillo, D.J. Antithrombotic Therapy in Patients With Chronic Kidney Disease. Circulation 2012, 125, 2649–2661. [Google Scholar] [CrossRef] [Green Version]
- Segal, R.; Lubart, E.; Leibovitz, A.; Iaina, A.; Caspi, D. Renal Effects of Low Dose Aspirin in Elderly Patients. Isr. Med. Assoc. J. 2006, 8, 679–682. [Google Scholar] [PubMed]
- Kim, A.J.; Lim, H.J.; Ro, H.; Ko, K.-P.; Han, S.Y.; Chang, J.H.; Lee, H.H.; Chung, W.; Jung, J.Y. Low-Dose Aspirin for Prevention of Cardiovascular Disease in Patients with Chronic Kidney Disease. PLoS ONE 2014, 9, e104179. [Google Scholar] [CrossRef]
- Tsai, M.-H.; Liou, H.-H.; Huang, Y.-C.; Lee, T.-S.; Chen, M.; Fang, Y.-W. Hazardous Effect of Low-Dose Aspirin in Patients with Predialysis Advanced Chronic Kidney Disease Assessed by Machine Learning Method Feature Selection. Healthcare 2021, 9, 1484. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.J.; Kim, A.J.; Ro, H.; Chang, J.H.; Lee, H.H.; Chung, W.; Hyun, Y.Y.; Lee, J.; Kim, Y.H.; Han, S.H.; et al. Low-Dose Aspirin Was Associated with an Increased Risk of Cardiovascular Events in Patients with Chronic Kidney Disease and Low Bodyweight: Results from KNOW-CKD Study. Sci. Rep. 2021, 11, 6691. [Google Scholar] [CrossRef] [PubMed]
- Papich, M.G. Saunders Handbook of Veterinary Drugs: Small and Large Animal, 4th ed.; Elsevier: St. Louis, MI, USA, 2016; ISBN 978-0-323-24485-5. [Google Scholar]
- Sparkes, A.H.; Heiene, R.; Lascelles, B.D.X.; Malik, R.; Real, L.; Robertson, S.; Scherk, M.; Taylor, P. ISFM and AAFP Consensus Guidelines: Long-Term Use of NSAIDs in Cats. J. Feline Med. Surg. 2010, 12, 521–538. [Google Scholar] [CrossRef] [PubMed]
- Deray, G.; Bagnis, C.; Brouard, R.; Necciari, J.; Leenhardt, A.F.; Raymond, F.; Baumelou, A. Clopidogrel Activities in Patients with Renal Function Impairment. Clin. Drug Investig. 1998, 16, 319–328. [Google Scholar] [CrossRef]
- Tanios, B.Y.; Itani, H.S.; Zimmerman, D.L. Clopidogrel Use in End-Stage Kidney Disease. Semin. Dial. 2015, 28, 276–281. [Google Scholar] [CrossRef]
- Jiang, X.-L.; Samant, S.; Lesko, L.J.; Schmidt, S. Clinical Pharmacokinetics and Pharmacodynamics of Clopidogrel. Clin. Pharm. 2015, 54, 147–166. [Google Scholar] [CrossRef] [Green Version]
- Nishi, T.; Ariyoshi, N.; Nakayama, T.; Fujimoto, Y.; Sugimoto, K.; Wakabayashi, S.; Hanaoka, H.; Kobayashi, Y. Impact of Chronic Kidney Disease on Platelet Inhibition of Clopidogrel and Prasugrel in Japanese Patients. J. Cardiol. 2017, 69, 752–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shropshire, S.; Johnson, T.; Olver, C. Platelet Aggregometry Testing during Aspirin or Clopidogrel Treatment and Measurement of Clopidogrel Metabolite Concentrations in Dogs with Protein-losing Nephropathy. J. Vet. Intern. Med. 2020, 34, 710–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segev, G.; Naylor, S.; Cowgill, L.D. Hematological and Neurological Side Effects Associated with the Use of Aluminum Based Phosphate Binders in Dogs with Chronic Kidney Disease. Isr. J. Vet. Med. 2016, 71, 31–38. [Google Scholar]
- Manlucu, J.; Tonelli, M.; Ray, J.G.; Papaioannou, A.; Youssef, G.; Thiessen-Philbrook, H.R.; Holbrook, A.; Garg, A.X. Dose-Reducing H2 Receptor Antagonists in the Presence of Low Glomerular Filtration Rate: A Systematic Review of the Evidence. Nephrol Dial. Transpl. 2005, 20, 2376–2384. [Google Scholar] [CrossRef] [PubMed]
- Marks, S.L.; Kook, P.H.; Papich, M.G.; Tolbert, M.K.; Willard, M.D. ACVIM Consensus Statement: Support for Rational Administration of Gastrointestinal Protectants to Dogs and Cats. J. Vet. Intern. Med. 2018, 32, 1823–1840. [Google Scholar] [CrossRef] [PubMed]
- Sierra, F.; Suarez, M.; Rey, M.; Vela, M.F. Systematic Review: Proton Pump Inhibitor-Associated Acute Interstitial Nephritis: Systematic Review: PPI-Induced Interstitial Nephritis. Aliment. Pharmacol. Ther. 2007, 26, 545–553. [Google Scholar] [CrossRef]
- Lazarus, B.; Chen, Y.; Wilson, F.P.; Sang, Y.; Chang, A.R.; Coresh, J.; Grams, M.E. Proton Pump Inhibitor Use and the Risk of Chronic Kidney Disease. JAMA Intern. Med. 2016, 176, 238. [Google Scholar] [CrossRef] [Green Version]
- de la Puente-Redondo, V.A.; Siedek, E.M.; Benchaoui, H.A.; Tilt, N.; Rowan, T.G.; Clemence, R.G. The Anti-Emetic Efficacy of Maropitant (Cerenia?) In the Treatment of Ongoing Emesis Caused by a Wide Range of Underlying Clinical Aetiologies in Canine Patients in Europe. J. Small Anim. Pract. 2007, 48, 93–98. [Google Scholar] [CrossRef]
- Ramsey, D.S.; Kincaid, K.; Watkins, J.A.; Boucher, J.F.; Conder, G.A.; Eagleson, J.S.; Clemence, R.G. Safety and Efficacy of Injectable and Oral Maropitant, a Selective Neurokinin 1 Receptor Antagonist, in a Randomized Clinical Trial for Treatment of Vomiting in Dogs. J. Vet. Pharmacol. Ther. 2008, 31, 538–543. [Google Scholar] [CrossRef]
- Quimby, J.M.; Brock, W.T.; Moses, K.; Bolotin, D.; Patricelli, K. Chronic Use of Maropitant for the Management of Vomiting and Inappetence in Cats with Chronic Kidney Disease: A Blinded, Placebo-Controlled Clinical Trial. J. Feline Med. Surg. 2015, 17, 692–697. [Google Scholar] [CrossRef]
- Fitzpatrick, R.L.; Wittenburg, L.A.; Hansen, R.J.; Gustafson, D.L.; Quimby, J.M. Limited Sampling Pharmacokinetics of Subcutaneous Ondansetron in Healthy Geriatric Cats, Cats with Chronic Kidney Disease, and Cats with Liver Disease. J. Vet. Pharmacol. Therap. 2016, 39, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Quimby, J.M.; Gustafson, D.L.; Lunn, K.F. The Pharmacokinetics of Mirtazapine in Cats with Chronic Kidney Disease and In Age-Matched Control Cats. J. Vet. Intern. Med. 2011, 25, 985–989. [Google Scholar] [CrossRef]
- Ferguson, L.E.; McLean, M.K.; Bates, J.A.; Quimby, J.M. Mirtazapine Toxicity in Cats: Retrospective Study of 84 Cases (2006–2011). J. Feline Med. Surg. 2016, 18, 868–874. [Google Scholar] [CrossRef]
- Benson, K.K.; Zajic, L.B.; Morgan, P.K.; Brown, S.R.; Hansen, R.J.; Lunghofer, P.J.; Wittenburg, L.A.; Gustafson, D.L.; Quimby, J.M. Drug Exposure and Clinical Effect of Transdermal Mirtazapine in Healthy Young Cats: A Pilot Study. J. Feline Med. Surg. 2017, 19, 998–1006. [Google Scholar] [CrossRef]
- Giorgi, M.; Yun, H. Pharmacokinetics of Mirtazapine and Its Main Metabolites in Beagle Dogs: A Pilot Study. Vet. J. 2012, 192, 239–241. [Google Scholar] [CrossRef] [PubMed]
- Bianciardi, P.; Brovida, C.; Valente, M.; Aresu, L.; Cavicchioli, L.; Vischer, C.; Giroud, L.; Castagnaro, M. Administration of Miltefosine and Meglumine Antimoniate in Healthy Dogs: Clinicopathological Evaluation of the Impact on the Kidneys. Toxicol. Pathol. 2009, 37, 770–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daza González, M.A.; Miró, G.; Fermín Rodríguez, M.; Rupérez Noguer, C.; Fragío Arnold, C. Short Term Impacts of Meglumine Antimoniate Treatment on Kidney Function in Dogs with Clinical Leishmaniosis. Res. Vet. Sci. 2019, 126, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Kasabalis, D.; Chatzis, M.K.; Apostolidis, K.; Petanides, T.; Athanasiou, L.V.; Xenoulis, P.G.; Mataragka, A.; Ikonomopoulos, J.; Leontides, L.S.; Saridomichelakis, M.N. A Randomized, Blinded, Controlled Clinical Trial Comparing the Efficacy of Aminosidine (Paromomycin)-Allopurinol Combination with the Efficacy of Meglumine Antimoniate-Allopurinol Combination for the Treatment of Canine Leishmaniosis Due to Leishmania Infantum. Exp. Parasitol. 2020, 214, 107903. [Google Scholar] [CrossRef]
- Woerly, V.; Maynard, L.; Sanquer, A.; Eun, H.-M. Clinical Efficacy and Tolerance of Miltefosine in the Treatment of Canine Leishmaniosis. Parasitol. Res. 2009, 105, 463. [Google Scholar] [CrossRef]
- Manna, L.; Vitale, F.; Reale, S.; Picillo, E.; Neglia, G.; Vescio, F.; Gravino, A.E. Study of Efficacy of Miltefosine and Allopurinol in Dogs with Leishmaniosis. Vet. J. 2009, 182, 441–445. [Google Scholar] [CrossRef]
- Mateo, M.; Maynard, L.; Vischer, C.; Bianciardi, P.; Miró, G. Comparative Study on the Short Term Efficacy and Adverse Effects of Miltefosine and Meglumine Antimoniate in Dogs with Natural Leishmaniosis. Parasitol. Res. 2009, 105, 155. [Google Scholar] [CrossRef]
- Andrade, H.M.; Toledo, V.P.C.P.; Pinheiro, M.B.; Guimarães, T.M.P.D.; Oliveira, N.C.; Castro, J.A.; Silva, R.N.; Amorim, A.C.; Brandão, R.M.S.S.; Yoko, M.; et al. Evaluation of Miltefosine for the Treatment of Dogs Naturally Infected with L. infantum (=L. chagasi) in Brazil. Vet. Parasitol. 2011, 181, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iarussi, F.; Paradies, P.; Foglia Manzillo, V.; Gizzarelli, M.; Caratozzolo, M.F.; Navarro, C.; Greco, B.; Rubino, G.T.R.; Oliva, G.; Sasanelli, M. Comparison of Two Dosing Regimens of Miltefosine, Both in Combination With Allopurinol, on Clinical and Parasitological Findings of Dogs With Leishmaniosis: A Pilot Study. Front. Vet. Sci. 2020, 7, 577395. [Google Scholar] [CrossRef] [PubMed]
- Roura, X.; Cortadellas, O.; Day, M.J.; Benali, S.L.; Zatelli, A.; Canine Leishmaniosis Working Group; D’Anna, N.; Fondati, A.; Gradoni, L.; Lubas, G.; et al. Canine Leishmaniosis and Kidney Disease: Q&A for an Overall Management in Clinical Practice. J. Small Anim. Pr. 2021, 62, 3. [Google Scholar] [CrossRef]
- Pennisi, M.G.; Persichetti, M.F. Feline Leishmaniosis: Is the Cat a Small Dog? Vet. Parasitol. 2018, 251, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Dorsch, R.; Teichmann-Knorrn, S.; Sjetne Lund, H. Urinary Tract Infection and Subclinical Bacteriuria in Cats: A Clinical Update. J. Feline Med. Surg. 2019, 21, 1023–1038. [Google Scholar] [CrossRef] [Green Version]
- Hindar, C.; Chang, Y.; Syme, H.M.; Jepson, R.E. The Association of Bacteriuria with Survival and Disease Progression in Cats with Azotemic Chronic Kidney Disease. J. Vet. Intern. Med. 2020, 34, 2516–2524. [Google Scholar] [CrossRef]
- Lamoureux, A.; Da Riz, F.; Cappelle, J.; Boulouis, H.; Benchekroun, G.; Cadoré, J.; Krafft, E.; Maurey, C. Frequency of Bacteriuria in Dogs with Chronic Kidney Disease: A Retrospective Study of 201 Cases. J. Vet. Intern. Med. 2019, 33, 640–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St Peter, W.L.; Redic-Kill, K.A.; Halstenson, C.E. Clinical Pharmacokinetics of Antibiotics in Patients with Impaired Renal Function. Clin. Pharmacokinet. 1992, 22, 169–210. [Google Scholar] [CrossRef]
- Swan, S.K. Aminoglycoside Nephrotoxicity. Semin. Nephrol. 1997, 17, 27–33. [Google Scholar]
- Greene, C.E.; Boothe, D.M. Antimicrobial Chemotherapy. In Infectious Diseases of the Dog and Cat; Elsevier/Saunders: St. Louis, Mo, USA, 2012; ISBN 978-1-4160-6130-4. [Google Scholar]
- Yeary, R.A. Systemic Toxic Effects of Chemotherapeutic Agents in Domestic Animals. Vet. Clin. N. Am. 1975, 5, 51–69. [Google Scholar] [CrossRef]
- Beaucaire, G. Does Once-Daily Dosing Prevent Nephrotoxicity in All Aminoglycosides Equally? Clin. Microbiol. Infect. 2000, 6, 355–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez, L.S.; Spencer, J.P. Aminoglycosides: A Practical Review. Am. Fam. Physician 1998, 58, 1811–1820. [Google Scholar]
- Albarellos, G.; Montoya, L.; Ambros, L.; Kreil, V.; Hallu, R.; Rebuelto, M. Multiple Once-Daily Dose Pharmacokinetics and Renal Safety of Gentamicin in Dogs. J. Vet. Pharm. 2004, 27, 21–25. [Google Scholar] [CrossRef]
- Avent, M.L.; Rogers, B.A.; Cheng, A.C.; Paterson, D.L. Current Use of Aminoglycosides: Indications, Pharmacokinetics and Monitoring for Toxicity: Aminoglycosides: Review and Monitoring. Intern. Med. J. 2011, 41, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Pagkalis, S.; Mantadakis, E.; Mavros, M.N.; Ammari, C.; Falagas, M.E. Pharmacological Considerations for the Proper Clinical Use of Aminoglycosides. Drugs 2011, 71, 2277–2294. [Google Scholar] [CrossRef] [PubMed]
- Riviere, J.E.; Carver, M.P.; Coppoc, G.L.; Carlton, W.W.; Lantz, G.C.; Shy-Modjeska, J. Pharmacokinetics and Comparative Nephrotoxicity of Fixed-Dose versus Fixed-Interval Reduction of Gentamicin Dosage in Subtotal Nephrectomized Dogs. Toxicol. Appl. Pharmacol. 1984, 75, 496–509. [Google Scholar] [CrossRef]
- IRIS Kidney—Guidelines—Preventing Aminoglycoside-Induced AKI. Available online: http://www.iris-kidney.com/education/prevention.html (accessed on 30 September 2021).
- Papich, M.G. Table of Common Drugs: Approximate Dosages. In Kirk’s Current Veterinary Therapy XIV; Saunders/Elsevier: Philadelphia, PA, USA, 2008; ISBN 978-1-4377-1152-3. [Google Scholar]
- Horber, F.F.; Frey, F.J.; Descoeudres, C.; Murray, A.T.; Reubi, F.C. Differential Effect of Impaired Renal Function on the Kinetics of Clavulanic Acid and Amoxicillin. Antimicrob. Agents Chemother. 1986, 29, 614–619. [Google Scholar] [CrossRef] [Green Version]
- Caprile, K.A. The Cephalosporin Antimicrobial Agents: A Comprehensive Review. J. Vet. Pharmacol. Ther. 1988, 11, 1–32. [Google Scholar] [CrossRef]
- Klepser, M.E.; Marangos, M.N.; Patel, K.B.; Nicolau, D.P.; Quintiliani, R.; Nightingale, C.H. Clinical Pharmacokinetics of Newer Cephalosporins. Clin. Pharmacokinet. 1995, 28, 361–384. [Google Scholar] [CrossRef]
- Trepanier, L.A. Delayed Hypersensitivity Reactions to Sulphonamides: Syndromes, Pathogenesis and Management. Vet. Derm. 1999, 10, 241–248. [Google Scholar] [CrossRef]
- Trepanier, L.A.; Danhof, R.; Toll, J.; Watrous, D. Clinical Findings in 40 Dogs with Hypersensitivity Associated with Administration of Potentiated Sulfonamides. J. Vet. Intern. Med. 2003, 17, 647–652. [Google Scholar] [CrossRef]
- Giger, U.; Werner, L.L.; Millichamp, N.J.; Gorman, N.T. Sulfadiazine-Induced Allergy in Six Doberman Pinschers. J. Am. Vet. Med. Assoc. 1985, 186, 479–484. [Google Scholar]
- Cribb, A.E. Idiosyncratic Reactions to Sulfonamides in Dogs. J. Am. Vet. Med. Assoc. 1989, 195, 1612–1614. [Google Scholar] [PubMed]
- Cribb, A.E.; Spielberg, S.P. An in Vitro Investigation of Predisposition to Sulphonamide Idiosyncratic Toxicity in Dogs. Vet. Res. Commun. 1990, 14, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Hadrick, M.K.; Vaden, S.L.; Geoly, F.J.; Cullen, J.M.; Douglass, J.P. Acute Tubulointerstitial Nephritis with Eosinophiluria in a Dog. J. Vet. Intern. Med. 1996, 10, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, H.P.; Schneider, M.; Dupouy, V.; Laroute, V.; Costes, G.; Delesalle, L.; Toutain, P.L. Effect of Experimental Renal Impairment on Disposition of Marbofloxacin and Its Metabolites in the Dog. J. Vet. Pharmacol. Ther. 1998, 21, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Mathews, K.A. Nonsteroidal Anti-Inflammatory Analgesics. Vet. Clin. N. Am. Small Anim. Pract. 2000, 30, 783–804. [Google Scholar] [CrossRef]
- Mathews, K.; Kronen, P.W.; Lascelles, D.; Nolan, A.; Robertson, S.; Steagall, P.V.; Wright, B.; Yamashita, K. Guidelines for Recognition, Assessment and Treatment of Pain: WSAVA Global Pain Council Members and Co-Authors of This Document. J. Small Anim. Pr. 2014, 55, E10–E68. [Google Scholar] [CrossRef]
- Hampshire, V.A.; Doddy, F.M.; Post, L.O.; Koogler, T.L.; Burgess, T.M.; Batten, P.O.; Hudson, R.; McAdams, D.R.; Brown, M.A. Adverse Drug Event Reports at the United States Food and Drug Administration Center for Veterinary Medicine. J. Am. Vet. Med. Assoc. 2004, 225, 533–536. [Google Scholar] [CrossRef]
- Lascelles, B.D.X.; McFarland, J.M.; Swann, H. Guidelines for Safe and Effective Use of NSAIDs in Dogs. Vet. Ther. 2005, 6, 237–251. [Google Scholar]
- Lascelles, B.D.X.; Court, M.H.; Hardie, E.M.; Robertson, S.A. Nonsteroidal Anti-Inflammatory Drugs in Cats: A Review. Vet. Anaesth. Analg. 2007, 34, 228–250. [Google Scholar] [CrossRef]
- Launay-Vacher, V.; Karie, S.; Fau, J.-B.; Izzedine, H.; Deray, G. Treatment of Pain in Patients with Renal Insufficiency: The World Health Organization Three-Step Ladder Adapted. J. Pain 2005, 6, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Kurella Tamura, M.; Feldman, H.I. KDOQI US Commentary on the 2012 KDIGO Clinical Practice Guideline for the Evaluation and Management of CKD. Am. J. Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, M.; Perazella, M.A. NSAIDs in CKD: Are They Safe? Am. J. Kidney Dis. 2020, 76, 546–557. [Google Scholar] [CrossRef] [PubMed]
- Kongara, K.; Cave, N.; Weidgraaf, K.; Rao Dukkipati, V.S. Effect of Non-Steroidal Anti-Inflammatory Drugs on Glomerular Filtration Rate and Urinary N-Acetyl-β-D-Glucosaminidase Activity in Cats after Dental Surgery. Vet. Anaesth. Analg. 2020, 47, 631–636. [Google Scholar] [CrossRef]
- Khan, K.N.M.; Venturini, C.M.; Bunch, R.T.; Brassard, J.A.; Koki, A.T.; Morris, D.L.; Trump, B.E.; Maziasz, T.J.; Alden, C.L. Interspecies Differences in Renal Localization of Cyclooxygenase Isoforms: Implications in Nonsteroidal Antiinflammatory Drug-Related Nephrotoxicity. Toxicol. Pathol. 1998, 26, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Papich, M.G. Pharmacologic Considerations for Opiate Analgesic and Nonsteroidal Anti-Inflammatory Drugs. Vet. Clin. N. Am. Small Anim. Pract. 2000, 30, 815–837. [Google Scholar] [CrossRef]
- Horii, Y.; Ikenaga, M.; Shimoda, M.; Kokue, E. Pharmacokinetics of Flunixin in the Cat: Enterohepatic Circulation and Active Transport Mechanism in the Liver. J. Vet. Pharm. 2004, 27, 65–69. [Google Scholar] [CrossRef]
- Castro, E.; Soraci, A.; Fogel, F.; Tapia, O. Chiral Inversion of R(-) Fenoprofen and Ketoprofen Enantiomers in Cats. J. Vet. Pharm. 2000, 23, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, B.; Steagall, P.V.M.; Lascelles, B.D.X.; Robertson, S.; Murrell, J.C.; Kronen, P.W.; Wright, B.; Yamashita, K. Long-Term Use of Non-Steroidal Anti-Inflammatory Drugs in Cats with Chronic Kidney Disease: From Controversy to Optimism. J. Small Anim. Pract. 2019, 60, 459–462. [Google Scholar] [CrossRef] [PubMed]
- Pages, J.-P. Néphropathies Dues Aux Anti-Inflammatoires Non Stéroïdiens [AINS] Chez Le Chat: 21 Observations (1993–2001). Prat. Méd. Chir. L’animal Cie 2005, 40, 177–181. [Google Scholar]
- Gunew, M.N.; Menrath, V.H.; Marshall, R.D. Long-Term Safety, Efficacy and Palatability of Oral Meloxicam at 0.01–0.03 Mg/Kg for Treatment of Osteoarthritic Pain in Cats. J. Feline Med. Surg. 2008, 10, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Gowan, R.A.; Lingard, A.E.; Johnston, L.; Stansen, W.; Brown, S.A.; Malik, R. Retrospective Case—Control Study of the Effects of Long-Term Dosing with Meloxicam on Renal Function in Aged Cats with Degenerative Joint Disease. J. Feline Med. Surg. 2011, 13, 752–761. [Google Scholar] [CrossRef]
- Gowan, R.A.; Baral, R.M.; Lingard, A.E.; Catt, M.J.; Stansen, W.; Johnston, L.; Malik, R. A Retrospective Analysis of the Effects of Meloxicam on the Longevity of Aged Cats with and without Overt Chronic Kidney Disease. J. Feline Med. Surg. 2012, 14, 876–881. [Google Scholar] [CrossRef]
- King, J.N.; King, S.; Budsberg, S.C.; Lascelles, B.D.X.; Bienhoff, S.E.; Roycroft, L.M.; Roberts, E.S. Clinical Safety of Robenacoxib in Feline Osteoarthritis: Results of a Randomized, Blinded, Placebo-Controlled Clinical Trial. J. Feline Med. Surg. 2016, 18, 632–642. [Google Scholar] [CrossRef]
- Surdyk, K.K.; Brown, C.A.; Brown, S.A. Evaluation of Glomerular Filtration Rate in Cats with Reduced Renal Mass and Administered Meloxicam and Acetylsalicylic Acid. Am. J. Vet. Res. 2013, 74, 648–651. [Google Scholar] [CrossRef]
- KuKanich, K.; George, C.; Roush, J.K.; Sharp, S.; Farace, G.; Yerramilli, M.; Peterson, S.; Grauer, G.F. Effects of Low-Dose Meloxicam in Cats with Chronic Kidney Disease. J. Feline Med. Surg. 2021, 23, 138–148. [Google Scholar] [CrossRef]
- Surdyk, K.K.; Sloan, D.L.; Brown, S.A. Evaluation of the Renal Effects of Ibuprofen and Carprofen in Euvolemic and Volume-Depleted Dogs. Int. J. Appl. Res. Vet. Med. 2011, 9, 130. [Google Scholar]
- Surdyk, K.K.; Sloan, D.L.; Brown, S.A. Renal Effects of Carprofen and Etodolac in Euvolemic and Volume-Depleted Dogs. Am. J. Vet. Res. 2012, 73, 1485–1490. [Google Scholar] [CrossRef]
- KuKanich, B.; Bidgood, T.; Knesl, O. Clinical Pharmacology of Nonsteroidal Anti-Inflammatory Drugs in Dogs. Vet. Anaesth. Analg. 2012, 39, 69–90. [Google Scholar] [CrossRef]
- Nine Ways to Minimize the Risks of Nonsteroidal Anti-Inflammatory Drugs (NSAIDs). Available online: https://www.aaha.org/aaha-guidelines/pain-management-config/implementation-toolkit/nine-ways-to-minimize-the-risks-of-nonsteroidal-anti-inflammatory-drugs-nsaids/ (accessed on 30 September 2021).
- Smets, P.M.Y.; Lefebvre, H.P.; Aresu, L.; Croubels, S.; Haers, H.; Piron, K.; Meyer, E.; Daminet, S. Renal Function and Morphology in Aged Beagle Dogs Before and after Hydrocortisone Administration. PLoS ONE 2012, 7, e31702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz, J.; Soblechero, P.; Duque, F.J.; Macías-García, B.; Ruiz, P.; Zaragoza, C.; Barrera, R. Effects of Oral Prednisone Administration on Serum Cystatin C in Dogs. J. Vet. Intern. Med. 2017, 31, 1765–1770. [Google Scholar] [CrossRef] [Green Version]
- IRIS Canine GN Study Group Established Pathology Subgroup; Segev, G.; Cowgill, L.D.; Heiene, R.; Labato, M.A.; Polzin, D.J. Consensus Recommendations for Immunosuppressive Treatment of Dogs with Glomerular Disease Based on Established Pathology. J. Vet. Intern. Med. 2013, 27, S44–S54. [Google Scholar] [CrossRef] [Green Version]
- Elliott, J.; Barber, P.J.; Syme, H.M.; Rawlings, J.M.; Markwell, P.J. Feline Hypertension: Clinical Findings and Response to Antihypertensive Treatment in 30 Cases. J. Small Anim. Pr. 2001, 42, 122–129. [Google Scholar] [CrossRef]
- Jepson, R.E.; Brodbelt, D.; Vallance, C.; Syme, H.M.; Elliott, J. Evaluation of Predictors of the Development of Azotemia in Cats. J. Vet. Intern. Med. 2009, 23, 806–813. [Google Scholar] [CrossRef] [PubMed]
- Schmieder, R. Mechanisms for the Clinical Benefits of Angiotensin II Receptor Blockers. Am. J. Hypertens. 2005, 18, 720–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lefebvre, H.; Brown, S.; Chetboul, V.; King, J.; Pouchelon, J.-L.; Toutain, P. Angiotensin-Converting Enzyme Inhibitors in Veterinary Medicine. CPD 2007, 13, 1347–1361. [Google Scholar] [CrossRef] [PubMed]
- Grauer, G.F.; Greco, D.S.; Getzy, D.M.; Cowgill, L.D.; Vaden, S.L.; Chew, D.J.; Polzin, D.J.; Barsanti, J.A. Effects of Enalapril versus Placebo as a Treatment for Canine Idiopathic Glomerulonephritis. J. Vet. Intern. Med. 2000, 14, 526–533. [Google Scholar] [CrossRef] [PubMed]
- King, J.N.; Gunn-Moore, D.A.; Tasker, S.; Gleadhill, A.; Strehlau, G. Tolerability and Efficacy of Benazepril in Cats with Chronic Kidney Disease. J. Vet. Intern. Med. 2006, 20, 1054–1064. [Google Scholar] [CrossRef] [PubMed]
- Mizutani, H.; Koyama, H.; Watanabe, T.; Kitagawa, H.; Nakano, M.; Kajiwara, K.; King, J.N. Evaluation of the Clinical Efficacy of Benazepril in the Treatment of Chronic Renal Insufficiency in Cats. J. Vet. Intern. Med. 2006, 20, 1074–1079. [Google Scholar] [CrossRef] [PubMed]
- Tenhündfeld, J.; Wefstaedt, P.; Nolte, I.J.A. A Randomized Controlled Clinical Trial of the Use of Benazepril and Heparin for the Treatment of Chronic Kidney Disease in Dogs. J. Am. Vet. Med. Assoc. 2009, 234, 1031–1037. [Google Scholar] [CrossRef] [PubMed]
- Harley, L.; Langston, C. Proteinuria in Dogs and Cats. Can. Vet. J. 2012, 53, 631–638. [Google Scholar]
- Toutain, P.L.; Lefebvre, H.P. Pharmacokinetics and Pharmacokinetic/Pharmacodynamic Relationships for Angiotensin-Converting Enzyme Inhibitors. J. Vet. Pharm. 2004, 27, 515–525. [Google Scholar] [CrossRef] [PubMed]
- King, J.N.; Strehlau, G.; Wernsing, J.; Brown, S.A. Effect of Renal Insufficiency on the Pharmacokinetics and Pharmacodynamics of Benazepril in Cats. J. Vet. Pharm. 2002, 25, 371–378. [Google Scholar] [CrossRef]
- Lefebvre, H.P.; Laroute, V.; Concordet, D.; Toutain, P.L. Effects of Renal Impairment on the Disposition of Orally Administered Enalapril, Benazepril, and Their Active Metabolites. J. Vet. Intern. Med. 1999, 13, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, T.L.; Coleman, A.E.; Schmiedt, C.W.; Brown, S.A. Attenuation of the Pressor Response to Exogenous Angiotensin by Angiotensin Receptor Blockers and Benazepril Hydrochloride in Clinically Normal Cats. Am. J. Vet. Res. 2015, 76, 807–813. [Google Scholar] [CrossRef]
- Tissier, R.; Perrot, S.; Enriquez, B. Amlodipine: One of the Main Anti-Hypertensive Drugs in Veterinary Therapeutics. J. Vet. Cardiol. 2005, 7, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Pouchelon, J.L.; Atkins, C.E.; Bussadori, C.; Oyama, M.A.; Vaden, S.L.; Bonagura, J.D.; Chetboul, V.; Cowgill, L.D.; Elliot, J.; Francey, T.; et al. Cardiovascular–Renal Axis Disorders in the Domestic Dog and Cat: A Veterinary Consensus Statement. J. Small Anim. Pr. 2015, 56, 537–552. [Google Scholar] [CrossRef] [Green Version]
- IRIS Canine GN Study Group Standard Therapy Subgroup; Brown, S.; Elliott, J.; Francey, T.; Polzin, D.; Vaden, S. Consensus Recommendations for Standard Therapy of Glomerular Disease in Dogs. J. Vet. Intern. Med. 2013, 27, S27–S43. [Google Scholar] [CrossRef] [PubMed]
- Lennon, E.M.; Hanel, R.M.; Walker, J.M.; Vaden, S.L. Hypercoagulability in Dogs with Protein-Losing Nephropathy as Assessed by Thromboelastography. J. Vet. Intern. Med. 2013, 27, 462–468. [Google Scholar] [CrossRef] [PubMed]
- de Laforcade, A.; Bacek, L.; Blais, M.-C.; Goggs, R.; Lynch, A.; Rozanski, E. Consensus on the Rational Use of Antithrombotics in Veterinary Critical Care (CURATIVE): Domain 1-Defining Populations at Risk. J. Vet. Emerg. Crit. Care 2019, 29, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Geesaman, B.; Bach, J.; Monaghan, K. Heparin-Induced Hyperkalemia in a Dog Receiving Continuous Renal Replacement Treatment. J. Vet. Intern. Med. 2015, 29, 1629–1632. [Google Scholar] [CrossRef] [Green Version]
- Rayhel, L.H.; Quimby, J.M.; Cianciolo, R.E.; Cléroux, A.; McLeland, S.M.; Franken, T. Clinicopathologic and Pathologic Characteristics of Feline Proteinuric Kidney Disease. J. Feline Med. Surg. 2020, 22, 1219–1229. [Google Scholar] [CrossRef]
- Hogan, D.F.; Fox, P.R.; Jacob, K.; Keene, B.; Laste, N.J.; Rosenthal, S.; Sederquist, K.; Weng, H.-Y. Secondary Prevention of Cardiogenic Arterial Thromboembolism in the Cat: The Double-Blind, Randomized, Positive-Controlled Feline Arterial Thromboembolism; Clopidogrel vs. Aspirin Trial (FAT CAT). J. Vet. Cardiol. 2015, 17, S306–S317. [Google Scholar] [CrossRef]
- Giustino, G.; Baber, U.; Sartori, S.; Mehran, R.; Mastoris, I.; Kini, A.S.; Sharma, S.K.; Pocock, S.J.; Dangas, G.D. Duration of Dual Antiplatelet Therapy After Drug-Eluting Stent Implantation. J. Am. Coll. Cardiol. 2015, 65, 1298–1310. [Google Scholar] [CrossRef] [Green Version]
- Maton, P.N.; Burton, M.E. Antacids Revisited: A Review of Their Clinical Pharmacology and Recommended Therapeutic Use. Drugs 1999, 57, 855–870. [Google Scholar] [CrossRef]
- Segev, G.; Bandt, C.; Francey, T.; Cowgill, L.D. Aluminum Toxicity Following Administration of Aluminum-Based Phosphate Binders in 2 Dogs with Renal Failure. J. Vet. Intern. Med. 2008, 22, 1432–1435. [Google Scholar] [CrossRef]
- Xie, Y.; Bowe, B.; Li, T.; Xian, H.; Balasubramanian, S.; Al-Aly, Z. Proton Pump Inhibitors and Risk of Incident CKD and Progression to ESRD. JASN 2016, 27, 3153–3163. [Google Scholar] [CrossRef] [Green Version]
- Schubert, M.L. Adverse Effects of Proton Pump Inhibitors: Fact or Fake News? Curr. Opin. Gastroenterol. 2018, 34, 451–457. [Google Scholar] [CrossRef]
- Nagashima, R. Mechanisms of Action of Sucralfate. J. Clin. Gastroenterol. 1981, 3, 117–127. [Google Scholar] [PubMed]
- Leung, A.C.; Henderson, I.S.; Halls, D.J.; Dobbie, J.W. Aluminium Hydroxide versus Sucralfate as a Phosphate Binder in Uraemia. BMJ 1983, 286, 1379–1381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, J.A. Sucralfate, Intestinal Aluminum Absorption, and Aluminum Toxicity in a Patient on Dialysis. Ann. Intern. Med. 1989, 111, 179. [Google Scholar] [CrossRef]
- Conder, G.A.; Sedlacek, H.S.; Boucher, J.F.; Clemence, R.G. Efficacy and Safety of Maropitant, a Selective Neurokinin 1 Receptor Antagonist, in Two Randomized Clinical Trials for Prevention of Vomiting Due to Motion Sickness in Dogs. J. Vet. Pharmacol. Ther. 2008, 31, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Benchaoui, H.A.; Cox, S.R.; Schneider, R.P.; Boucher, J.F.; Clemence, R.G. The Pharmacokinetics of Maropitant, a Novel Neurokinin Type-1 Receptor Antagonist, in Dogs. J. Vet. Pharm. 2007, 30, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Hickman, M.A.; Cox, S.R.; Mahabir, S.; Miskell, C.; Lin, J.; Bunger, A.; McCALL, R.B. Safety, Pharmacokinetics and Use of the Novel NK-1 Receptor Antagonist Maropitant (CereniaTM ) for the Prevention of Emesis and Motion Sickness in Cats. J. Vet. Pharm. 2008, 31, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Quimby, J.M.; Lake, R.C.; Hansen, R.J.; Lunghofer, P.J.; Gustafson, D.L. Oral, Subcutaneous, and Intravenous Pharmacokinetics of Ondansetron in Healthy Cats. J. Vet. Pharmacol. Therap. 2014, 37, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Quimby, J.M.; Lunn, K.F. Mirtazapine as an Appetite Stimulant and Anti-Emetic in Cats with Chronic Kidney Disease: A Masked Placebo-Controlled Crossover Clinical Trial. Vet. J. 2013, 197, 651–655. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Deng, C.; Huang, X.-F. The Role of Hypothalamic H1 Receptor Antagonism in Antipsychotic-Induced Weight Gain. CNS Drugs 2013, 27, 423–434. [Google Scholar] [CrossRef]
- Schellekens, H.; De Francesco, P.N.; Kandil, D.; Theeuwes, W.F.; McCarthy, T.; van Oeffelen, W.E.P.A.; Perelló, M.; Giblin, L.; Dinan, T.G.; Cryan, J.F. Ghrelin’s Orexigenic Effect Is Modulated via a Serotonin 2C Receptor Interaction. ACS Chem. Neurosci. 2015, 6, 1186–1197. [Google Scholar] [CrossRef] [Green Version]
- Quimby, J.M.; Gustafson, D.L.; Samber, B.J.; Lunn, K.F. Studies on the Pharmacokinetics and Pharmacodynamics of Mirtazapine in Healthy Young Cats: Mirtazapine Pharmacokinetics and Pharmacodynamics in Cats. J. Vet. Pharmacol. Ther. 2011, 34, 388–396. [Google Scholar] [CrossRef]
- Fantinati, M.; Trnka, J.; Signor, A.; Dumond, S.; Jourdan, G.; Verwaerde, P.; Priymenko, N. Appetite-Stimulating Effect of Gabapentin vs Mirtazapine in Healthy Cats Post-Ovariectomy. J. Feline Med. Surg. 2020, 22, 1176–1183. [Google Scholar] [CrossRef]
- Quimby, J.M.; Benson, K.K.; Summers, S.C.; Saffire, A.; Herndon, A.K.; Bai, S.; Gustafson, D.L. Assessment of Compounded Transdermal Mirtazapine as an Appetite Stimulant in Cats with Chronic Kidney Disease. J. Feline Med. Surg. 2020, 22, 376–383. [Google Scholar] [CrossRef]
- Fitzpatrick, R.L.; Quimby, J.M.; Benson, K.K.; Ramirez, D.; Sieberg, L.G.; Wittenburg, L.A.; Gustafson, D.L. In Vivo and in Vitro Assessment of Mirtazapine Pharmacokinetics in Cats with Liver Disease. J. Vet. Intern. Med. 2018, 32, 1951–1957. [Google Scholar] [CrossRef] [PubMed]
- Buhles, W.; Quimby, J.M.; Labelle, D.; Williams, V.S. Single and Multiple Dose Pharmacokinetics of a Novel Mirtazapine Transdermal Ointment in Cats. J. Vet. Pharm. Ther. 2018, 41, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.A.L.; Goto, H.; Saldanha, L.C.B.; Silva, S.M.M.S.; Sinhorini, I.L.; Silva, T.C.; Guerra, J.L. Histopathologic Patterns of Nephropathy in Naturally Acquired Canine Visceral Leishmaniasis. Vet. Pathol. 2003, 40, 677–684. [Google Scholar] [CrossRef] [Green Version]
- Zatelli, A.; Borgarelli, M.; Santilli, R.; Bonfanti, U.; Nigrisoli, E.; Zanatta, R.; Tarducci, A.; Guarraci, A. Glomerular Lesions in Dogs Infected with Leishmania Organisms. Am. J. Vet. Res. 2003, 64, 558–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aresu, L.; Benali, S.; Ferro, S.; Vittone, V.; Gallo, E.; Brovida, C.; Castagnaro, M. Light and Electron Microscopic Analysis of Consecutive Renal Biopsy Specimens From Leishmania-Seropositive Dogs. Vet. Pathol. 2013, 50, 753–760. [Google Scholar] [CrossRef] [Green Version]
- Koutinas, A.F.; Koutinas, C.K. Pathologic Mechanisms Underlying the Clinical Findings in Canine Leishmaniosis Due to Leishmania Infantum/Chagasi. Vet. Pathol. 2014, 51, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Vaden, S.L. Glomerular Disease. In Nephrology and Urology of Small Animals; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2011; ISBN 978-0-8138-1717-0. [Google Scholar]
- Oliva, G.; Dvm, X.R.; Crotti, A.; Maroli, M.; Castagnaro, M.; Gradoni, L.; Lubas, G.; Paltrinieri, S.; Zatelli, A.; Zini, E. Guidelines for Treatment of Leishmaniasis in Dogs. J. Am. Vet. Med. Assoc. 2010, 236, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Solano-Gallego, L.; Miró, G.; Koutinas, A.; Cardoso, L.; Pennisi, M.G.; Ferrer, L.; Bourdeau, P.; Oliva, G.; Baneth, G. LeishVet Guidelines for the Practical Management of Canine Leishmaniosis. Parasites Vectors 2011, 4, 86. [Google Scholar] [CrossRef] [Green Version]
- Plevraki, K.; Koutinas, A.F.; Kaldrymidou, H.; Roumpies, N.; Papazoglou, L.G.; Saridomichelakis, M.N.; Savvas, I.; Leondides, L. Effects of Allopurinol Treatment on the Progression of Chronic Nephritis in Canine Leishmaniosis (Leishmania infantum). J. Vet. Intern. Med. 2006, 20, 228–233. [Google Scholar] [CrossRef]
- Pierantozzi, M.; Roura, X.; Paltrinieri, S.; Poggi, M.; Zatelli, A. Variation of Proteinuria in Dogs with Leishmaniasis Treated with Meglumine Antimoniate and Allopurinol: A Retrospective Study. J. Am. Anim. Hosp. Assoc. 2013, 49, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Proverbio, D.; Spada, E.; de Giorgi, G.B.; Perego, R. Proteinuria Reduction after Treatment with Miltefosine and Allopurinol in Dogs Naturally Infected with Leishmaniasis. Vet. World 2016, 9, 904–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, M.; Pastor, J.; Roura, X.; Tabar, M.D.; Espada, Y.; Font, A.; Balasch, J.; Planellas, M. Adverse Urinary Effects of Allopurinol in Dogs with Leishmaniasis: Urinary Adverse Effects of Allopurinol. J. Small Anim. Pr. 2016, 57, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Paltrinieri, S.; Solano-Gallego, L.; Fondati, A.; Lubas, G.; Gradoni, L.; Castagnaro, M.; Crotti, A.; Maroli, M.; Oliva, G.; Roura, X.; et al. Guidelines for Diagnosis and Clinical Classification of Leishmaniasis in Dogs. J. Am. Vet. Med. Assoc. 2010, 236, 1184–1191. [Google Scholar] [CrossRef]
- Pennisi, M.G.; Hartmann, K.; Lloret, A.; Addie, D.; Belák, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hosie, M.J.; et al. Leishmaniosis in Cats: ABCD Guidelines on Prevention and Management. J. Feline Med. Surg. 2013, 15, 638–642. [Google Scholar] [CrossRef]
- Fernandez-Gallego, A.; Feo Bernabe, L.; Dalmau, A.; Esteban-Saltiveri, D.; Font, A.; Leiva, M.; Ortuñez-Navarro, A.; Peña, M.-T.; Tabar, M.-D.; Real-Sampietro, L.; et al. Feline Leishmaniosis: Diagnosis, Treatment and Outcome in 16 Cats. J. Feline Med. Surg. 2020, 22, 993–1007. [Google Scholar] [CrossRef]
- Pennisi, M.-G.; Cardoso, L.; Baneth, G.; Bourdeau, P.; Koutinas, A.; Miró, G.; Oliva, G.; Solano-Gallego, L. LeishVet Update and Recommendations on Feline Leishmaniosis. Parasites Vectors 2015, 8, 302. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Proposed practical guideline for drug dosage adjustments in canine and feline chronic kidney disease. CKD: Chronic Kidney Disease; GFR: Glomerular Filtration Rate; Kf: Filtration Coefficient.
Figure 1.
Proposed practical guideline for drug dosage adjustments in canine and feline chronic kidney disease. CKD: Chronic Kidney Disease; GFR: Glomerular Filtration Rate; Kf: Filtration Coefficient.


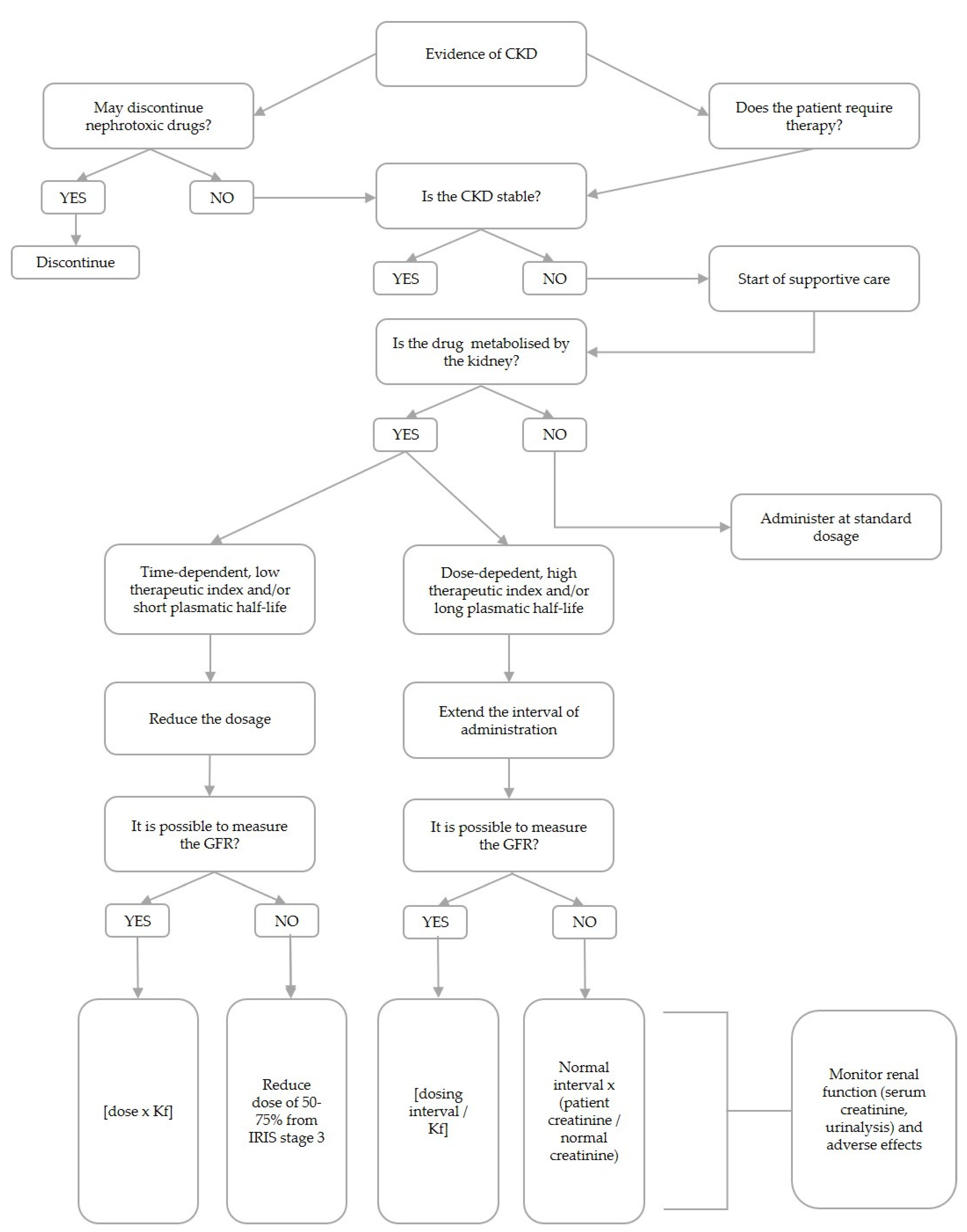{kind=link}
Table 1.
Summary of the main recommendation on the use of the revised class of drugs in patients with impaired renal function. CKD: chronic kidney disease; SDD: single daily dose; TDM: therapeutic drug monitoring; GFR: glomerular filtration rate; NSAIDs: non-steroidal anti-inflammatory drugs; ACEIs: Angiotensin II Converting Enzyme Inhibitors; ARBs: angiotensin receptor blockers; UPC: urinary protein to creatinine ratio; SBP: sistolic blood pressure; CCBs: calcium channel blockers; CRS: cardiorenal syndrome; LMWHs: low-molecular-weight heparins; H2RAs: histamine type-2 receptor antagonists; IRIS: International Renal Interest Society; PPis: proton pump inhibitors; AKI: acute kidney injury.
Table 1.
Summary of the main recommendation on the use of the revised class of drugs in patients with impaired renal function. CKD: chronic kidney disease; SDD: single daily dose; TDM: therapeutic drug monitoring; GFR: glomerular filtration rate; NSAIDs: non-steroidal anti-inflammatory drugs; ACEIs: Angiotensin II Converting Enzyme Inhibitors; ARBs: angiotensin receptor blockers; UPC: urinary protein to creatinine ratio; SBP: sistolic blood pressure; CCBs: calcium channel blockers; CRS: cardiorenal syndrome; LMWHs: low-molecular-weight heparins; H2RAs: histamine type-2 receptor antagonists; IRIS: International Renal Interest Society; PPis: proton pump inhibitors; AKI: acute kidney injury.
| Class | Drug | Comments |
|---|---|---|
| Antimicrobial agents | Aminoglycosides | Potentially nephrotoxic. Their use is generally discouraged in CKD patients [55]. When clinically indicated, the patients should be hemodynamically stable, and the concomitant use of other nephrotoxic drugs should be avoided. SDD regimen is recommended in association with TDM. The duration of treatment should be minimized (<7 days) [59]. |
| Penicillins | High therapeutic index [60]. Due to the possible accumulation, dose adjustment could be considered for ampicillin in dogs with severe azotemia [61]. Although penicillins have been classified as “probably safe” in cats with CKD [7,13], the need for dose adjustment in azotemic feline patients remains to be determined [62]. | |
| Cephalosporins | Dosage regimen adjustment based on an extension of the administration interval is recommended in humans with a moderate to severe reduction in GFR [63]; interval extension should be considered in dogs and cats with moderate or severe CKD [64]. | |
| Sulfonamides | Potential nephrotoxicity due to crystalluria and hypersensitivity reactions. Dehydration should be avoided [65]. In patients with reduced renal function dose adjustment could be considered (i.e., halving the dose or doubling the interval of administration) [64]. | |
| Tetracyclines | Increased risk of nephrotoxicity for water-soluble medications (e.g., oxytetracycline). In patients with altered renal function, doxycycline or minocycline should be preferred [60]. | |
| Fluoroquinolones | Undergo renal and non-renal elimination pathways. Dose adjustment may not be required in dogs [66]. Due to the high risk of retinopathy, an interval extension is recommended in CKD feline patients with moderate disease [7]. | |
| Anti-inflammatory drugs | NSAIDs | Potentially nephrotoxic [67,68]. When clinically indicated, the patients should be hemodynamically stable and the concomitant use of other nephrotoxic drugs should be avoided; close monitoring of renal function and administration of the lowest effective dose are recommended [7,69,70]. A washout period should be envisaged between different NSAIDs molecules and corticosteroids [69]. |
| Corticosteroids | Poor evidence of nephrotoxicity in dogs and cats. Possible worsening of azotemia and development of proteinuria reported in dogs [71]. | |
| Antiproteinuric and antihypertensive drugs | ACEis | Potentially nephrotoxic. Patients should be hemodynamically stabilized before administration and adoption of a lower starting dose and monitoring of renal function, SBP and serum electrolytes are recommended [72]. Caution should be used in an advanced stage of CKD and if administered in association with ARBs [73]. |
| ARBs | Potentially nephrotoxic. Telmisartan is safe and effective in reducing UPC and SBP in dogs and cats with CKD [74,75,76]. Caution should be used in advanced CKD stages and if administered in association with an ACEi [73]. | |
| CCBs | Amlodipine is a safe antihypertensive agent in cats with CKD [7,73,77]. Since CCBs preferentially dilate the renal afferent arteriole, exposing the glomerulus to increased hydrostatic pressure, their use as the sole antihypertensive drug in dogs is discouraged [73]. | |
| Diuretics | Furosemide | Potentially nephrotoxic due to excessive volume depletion. Contraindicated in patients with unstable renal function or volume depletion conditions; close monitoring of renal function is strongly recommended and association with other nephrotoxic drugs is discouraged [55,60]. Its use may be required in CRS [78]. |
| Antithrombotic agents | LMWHs | Risk of accumulation should be considered under conditions of reduced renal function [79]. Interval extension is recommended in humans with stage 4 CKD [80]. |
| Acetylsalicylic acid | Potentially dangerous in human CKD patients [81,82,83,84].No controlled clinical studies are available in animals [85]. Caution should be used under renal hypoperfusion conditions [86]. The concomitant administration of other NSAIDs should be avoided and renal function should be monitored. Prolonged time of excretion in cats [85]. | |
| Clopidogrel | Dose adjustments seem to not be required in humans with CKD [87,88]; however, the marked variability in pharmacokinetics of clopidogrel justifies its cautious use in patients with advanced CKD [80,88,89]; a lower antiplatelet effect has been observed in CKD patients [90]. Drug metabolism may not be altered in dogs with PLN and early CKD [91]. | |
| Gastroprotectants | Antacids | Although they generally lack systemic effects, the possible accumulation of aluminum and hypermagnesemia should be considered for aluminum/magnesium-containing salts in dogs with advanced renal failure [92]. No specific indications for dose adjustment are available in dogs and cats with CKD. |
| H2RAs | Dose adjustments recommended in humans [93]. Although no specific indications are available in dogs and cats [94], either decreasing the dose or extending the dosing interval can be used in IRIS Stages 3 and 4. | |
| PPIs | Nephrotoxicity (interstitial nephritis) reported in humans [95,96]. Poor evidence of nephrotoxicity in dogs and cats [94]. | |
| Sucralfate | Relatively safe compound. Caution should be used with long-term treatment in patients with renal insufficiency to avoid aluminum intoxication [94]. | |
| Antiemetics | Metoclopramide | Administration at standard constant rate infusion dosages (1–2 mg/kg/day) may cause tremors and ataxia in azotemic patients. The dose could be reduced by up to the 25–50% of the standard dose and titrate to dosage, which elicit a therapeutic effect without tremor [64]. |
| Maropitant | Safe in dogs and cats with renal impairment [97,98,99]. | |
| Ondansentron | Safe in cats with renal impairment [100]. No pharmacokinetic data are available for dogs. | |
| Appetite stimulants | Mirtazapine | 1.88 mg/cat q 24–48 h may be suitable as a starting dose in cats with CKD [101,102,103]. Limited data are available for dogs [104]. |
| Antileishmanial drugs | Meglumine antimoniate | Despite the limited evidence of nephrotoxicity, dose reduction and a monitoring of renal function are recommended [105,106,107]. Use in dogs with advanced renal failure is discouraged. Limited data on use in cats. |
| Miltefosine | Low impact on renal function in dogs [105,108,109,110,111,112]. Limited data on use in cats. | |
| Allopurinol | In cases of xantinuria, mineralization or uroliths, the interval of administration should be prolonged (i.e., 10 mg/kg q24 h) [113]. Limited data are available for cats; development of AKI reported [114]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
De Santis, F.; Boari, A.; Dondi, F.; Crisi, P.E. Drug-Dosing Adjustment in Dogs and Cats with Chronic Kidney Disease. Animals 2022, 12, 262. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12030262
AMA Style
De Santis F, Boari A, Dondi F, Crisi PE. Drug-Dosing Adjustment in Dogs and Cats with Chronic Kidney Disease. Animals. 2022; 12(3):262. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12030262
Chicago/Turabian StyleDe Santis, Francesca, Andrea Boari, Francesco Dondi, and Paolo Emidio Crisi. 2022. "Drug-Dosing Adjustment in Dogs and Cats with Chronic Kidney Disease" Animals 12, no. 3: 262. https://0-doi-org.brum.beds.ac.uk/10.3390/ani12030262
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.