
Recent Considerations on Gaming Console Based Training for Multiple Sclerosis Rehabilitation

 , ,
, ,
Abstract
:1. Introduction
- To present a pilot study investigating whether a novel exercise adopter in a WFBB rehabilitation training program may improve physical abilities and QoL of patients compared to that of a conventional four-week rehabilitation training program. To this end, we consider two groups of patients: the first one performing a rehabilitation training program using WFBB, which we named the Wii group, and the second one performing a Standard Rehabilitation (SR) training program, which we named the SR group. In particular, for each group, we considered both demographic and clinical characteristics. In addition, we also focused on balance performance, walking, and functional independence measures.
- To discuss how such a rehabilitation training program could be adopted in the perspective of near future networks of medical IoT-based rehabilitation devices interconnected with a hospital Cloud system for big health data processing. On the one hand, this would allow for the analysis of aggregated data by providing clues about how to improve patients’ therapies, and on the other hand, facilitating scientific research about motor rehabilitation.
2. Literature Review
3. Materials and Methods
3.1. Population Study
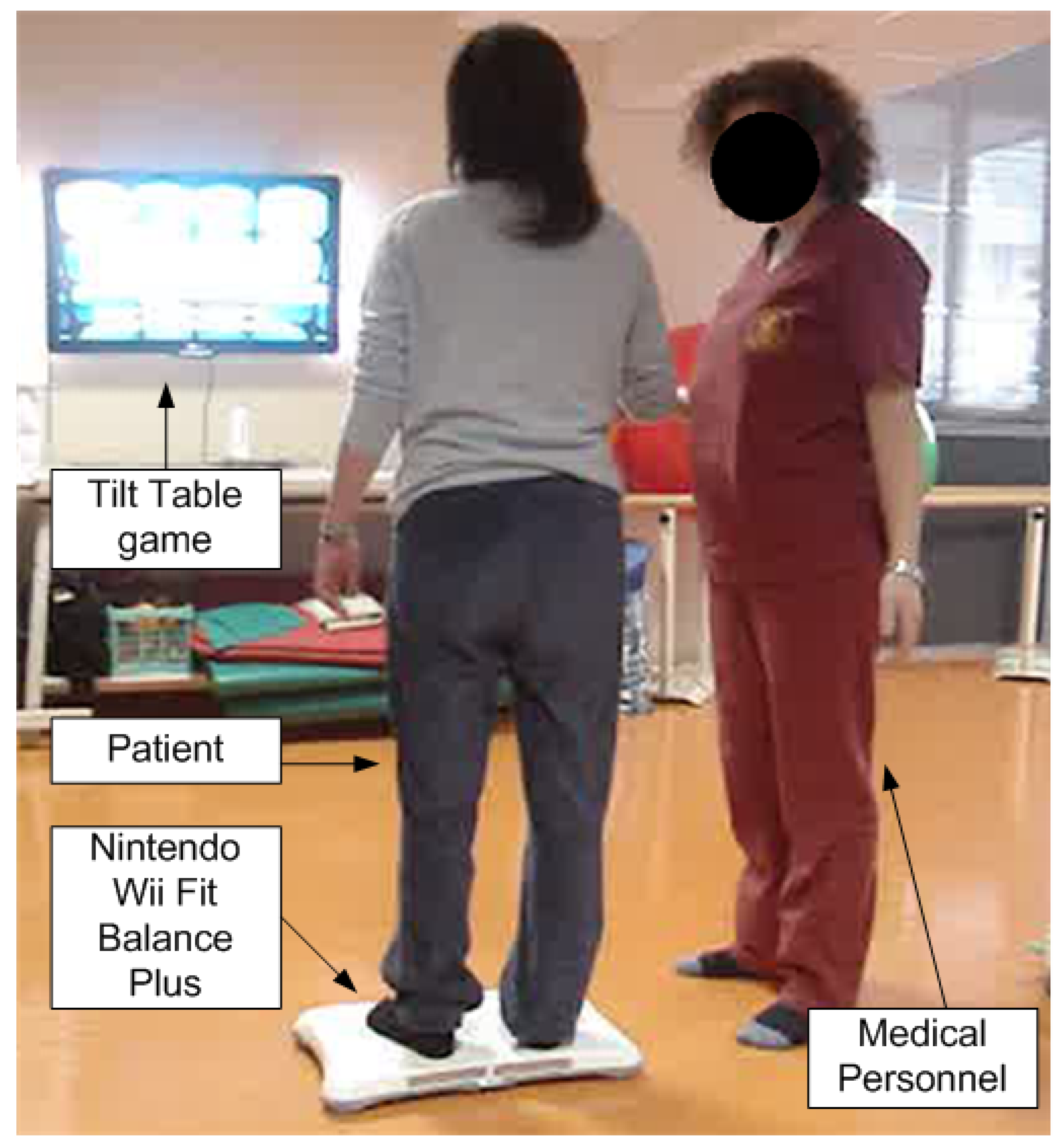
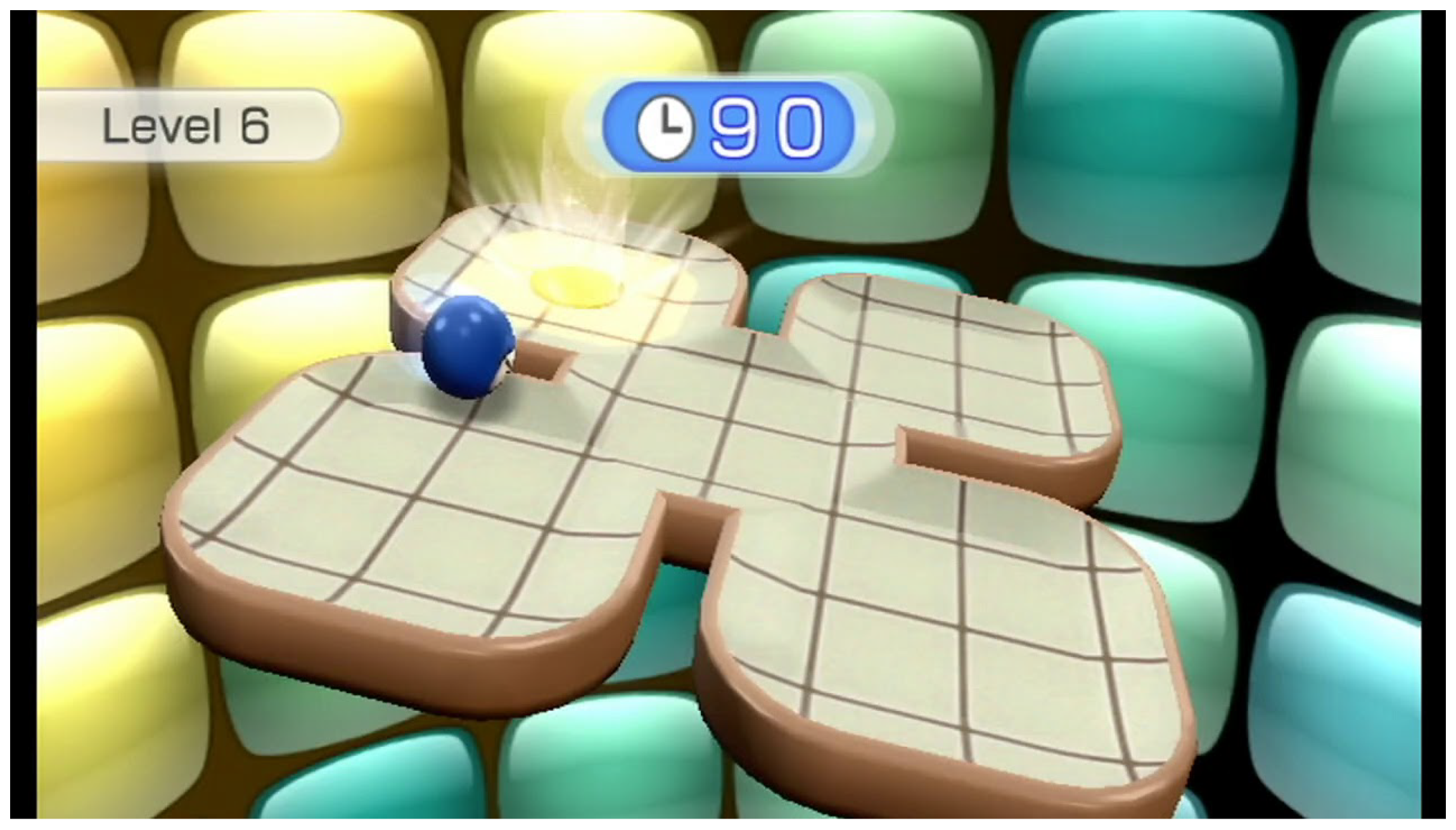
3.2. Intervention
3.3. Outcomes
3.4. Statistical Analysis
4. Results
- A small p-value (typically ≤ 0.05) indicates strong evidence against the hypothesis, so you reject the hypothesis.
- A large p-value (>0.05) indicates weak evidence against the hypothesis, so you fail to reject the hypothesis.
- p-values very close to the cutoff (0.05) are considered to be marginal.
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Compston, A.; Coles, A. Multiple sclerosis. Lancet 2002, 359, 1221–1231. [Google Scholar] [CrossRef]
- Scalfari, A.; Neuhaus, A.; Degenhardt, A.; Rice, G.; Muraro, P.; Daumer, M.; Ebers, G. The natural history of multiple sclerosis, a geographically based study 10: Relapses and long-term disability. Brain 2010, 133, 1914–1929. [Google Scholar] [CrossRef] [PubMed]
- Frohman, E.M.; Racke, M.; van den Noort, S. To Treat, or Not to Treat: The Therapeutic Dilemma of Idiopathic Monosymptomatic Demyelinating Syndromes. Arch. Neurol. 2000, 57, 930–932. [Google Scholar] [CrossRef] [PubMed]
- Conrad, A.; Coenen, M.; Schmalz, H.; Kesselring, J.; Cieza, A. Validation of the comprehensive ICF core set for multiple sclerosis from the perspective of physical therapists. Phys. Ther. 2012, 92, 799–820. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Turner-Stokes, L.; Ng, L.; Kilpatrick, T. Multidisciplinary rehabilitation for adults with multiple sclerosis. Postgrad. Med. J. 2008, 84, 385. [Google Scholar] [CrossRef]
- Patti, F.; Ciancio, M.; Reggio, E.; Lopes, R.; Palermo, F.; Cacopardo, M.; Reggio, A. The impact of outpatient rehabilitation on quality of life in multiple sclerosis. J. Neurol. 2002, 249, 1027–1033. [Google Scholar] [CrossRef]
- Patti, F.; Cacopardo, M.; Palermo, F.; Ciancio, M.; Lopes, R.; Restivo, D.; Reggio, A. Health-related quality of life and depression in an Italian sample of multiple sclerosis patients. J. Neurol. Sci. 2003, 211, 55–62. [Google Scholar] [CrossRef]
- Pappalardo, A.; D’Amico, E.; Leone, C.; Messina, S.; Chisari, C.; Rampello, L.; Torre, L.; Patti, F. Inpatient versus outpatient rehabilitation for multiple sclerosis patients: Effects on disability and quality of life. Mult. Scler. Demyelinating Disord. 2016, 1, 3. [Google Scholar] [CrossRef] [Green Version]
- Kalron, A.; Fonkatz, I.; Frid, L.; Baransi, H.; Achiron, A. The effect of balance training on postural control in people with multiple sclerosis using the CAREN VR system: A pilot randomized controlled trial. J. Neuroeng. Rehabil. 2016, 13, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Cimino, V.; Chisari, C.; Raciti, G.; Russo, A.; Veca, D.; Zagari, F.; Calabrò, R.; Patti, F. Objective evaluation of Nintendo Wii Fit plus balance program training on postural stability in Multiple Sclerosis patients: A pilot study. Int. J. Rehabil. Res. 2020, 43, 199–205. [Google Scholar] [CrossRef]
- De Cola, M.; De Luca, R.; Bramanti, A.; Bertè, F.; Bramanti, P.; Calabrò, R. Tele-health services for the elderly: A novel southern Italy family needs-oriented model. J. Telemed. Telecare 2016, 22, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Laver, K.; George, S.; Ratcliffe, J.; Crotty, M. Virtual reality stroke rehabilitation—hype or hope? Aust. Occup. Ther. J. 2011, 58, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Szturm, T.; Betker, A.; Moussavi, Z.; Desai, A.; Goodman, V. Effects of an interactive computer game exercise regimen on balance impairment in frail community-dwelling older adults: A randomized controlled trial. Phys. Ther. 2011, 91, 1460–1462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, J.; Dixon, J.; Macsween, A.; van Schaik, P.; Martin, D. The effects of exergaming on balance, gait, technology acceptance and flow experience in people with multiple sclerosis: A randomized controlled trial. BMC Sport. Sci. Med. Rehabil. 2015, 7, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripette, J.; Murakami, H.; Ryan, K.; Ohta, Y.; Miyachi, M. The contribution of Nintendo Wii Fit series in the field of health: A systematic review and meta-analysis. PeerJ 2017, 2017, e3600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plow, M.; Finlayson, M. Potential Benefits of Nintendo Wii Fit Among People with Multiple Sclerosis. Int. J. MS Care 2011, 13, 21–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil-Gomez, J.A.; Lloréns, R.; Alcñiz, M.; Colomer, C. Effectiveness of a Wii balance board-based system (eBaViR) for balance rehabilitation: A pilot randomized clinical trial in patients with acquired brain injury. J. Neuroeng. Rehabil. 2011, 8, 30. [Google Scholar] [CrossRef] [Green Version]
- Prosperini, L.; Fortuna, D.; Giannì, C.; Leonardi, L.; Marchetti, M.; Pozzilli, C. Home-based balance training using the wii balance board: A randomized, crossover pilot study in multiple sclerosis. Neurorehabilit. Neural Repair 2013, 27, 516–525. [Google Scholar] [CrossRef]
- McDonald, W.; Compston, A.; Edan, G.; Goodkin, D.; Hartung, H.P.; Lublin, F.; McFarland, H.; Paty, D.; Polman, C.; Reingold, S.; et al. Recommended diagnostic criteria for multiple sclerosis: Guidelines from the International Panel on the Diagnosis of Multiple Sclerosis. Ann. Neurol. 2001, 50, 121–127. [Google Scholar] [CrossRef]
- Kurtzke, J. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Kidd, D.; Stewart, G.; Baldry, J.; Johnson, J.; Rossiter, D.; Petruckevitch, A.; Thompson, A. The functional independence measure: A comparative validity and reliability study. Disabil. Rehabil. 1995, 17, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Ottenbacher, K.; Hsu, Y.; Granger, C.; Fiedler, R. The reliability of the functional independence measure: A quantitative review. Arch. Phys. Med. Rehabil. 1996, 77, 1226–1232. [Google Scholar] [CrossRef]
- Giné-Garriga, M.; Guerra, M.; Manini, T.; Marí-Dell’Olmo, M.; Pagès, E.; Unnithan, V. Measuring balance, lower extremity strength and gait in the elderly: Construct validation of an instrument. Arch. Gerontol. Geriatr. 2010, 51, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, D.; Regola, A.; Meotti, M. Validity of six balance disorders scales in persons with multiple sclerosis. Disabil. Rehabil. 2006, 28, 789–795. [Google Scholar] [CrossRef]
- Cattaneo, D.; Jonsdottir, J.; Repetti, S. Reliability of four scales on balance disorders in persons with multiple sclerosis. Disabil. Rehabil. 2007, 29, 1920–1925. [Google Scholar] [CrossRef]
- Cutter, G.; Baier, M.; Rudick, R.; Cookfair, D.; Fischer, J.; Petkau, J.; Syndulko, K.; Weinshenker, B.; Antel, J.; Confavreux, C.; et al. Development of a multiple sclerosis functional composite as a clinical trial outcome measure. Brain 1999, 122, 871–882. [Google Scholar] [CrossRef]
- Polman, C.; Rudick, R. The multiple sclerosis functional composite a clinically meaningful measure of disability. Neurology 2010, 74, S8–S15. [Google Scholar] [CrossRef]
- Dickson, H.; Köhler, F. The Functional Independence Measure: A comparative validity and reliability study. Disabil. Rehabil. 1995, 17, 456. [Google Scholar] [CrossRef]
- Prosperini, L.; Leonardi, L.; De Carli, P.; Mannocchi, M.; Pozzilli, C. Visuo-proprioceptive training reduces risk of falls in patients with multiple sclerosis. Mult. Scler. 2010, 16, 491–499. [Google Scholar] [CrossRef]
- Cattaneo, D.; Cardini, R. Computerized system to improve voluntary control of balance in neurological patients. Cyberpsychol. Behav. 2001, 4, 687–694. [Google Scholar] [CrossRef]
- Rougier, P. Optimising the visual feedback technique for improving upright stance maintenance by delaying its display: Behavioural effects on healthy adults. Gait Posture 2004, 19, 154–163. [Google Scholar] [CrossRef]
- Shafizadehkenari, M.; Abolfazli, R.; Platt, G.K. Effect of visual force biofeedback on balance control in people with Multiple Sclerosis- a Pilot Quasi-experimental study. J. Phys. Ther. 2012, 6, 21–27. [Google Scholar]
- Cameron, M.H.; Lord, S. Postural Control in Multiple Sclerosis: Implications for Fall Prevention. Curr. Neurol. Neurosci. Rep. 2010, 10, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Rizzolatti, G.; Fabbri-Destro, M.; Cattaneo, L. Mirror neurons and their clinical relevance. Nat. Clin. Pract. Neurol. 2009, 5, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Kleim, J. Neural plasticity and neurorehabilitation: Teaching the new brain old tricks. J. Commun. Disord. 2011, 44, 521–528. [Google Scholar] [CrossRef]
- Nitz, J.; Kuys, S.; Isles, R.; Fu, S. Is the Wii Fit™ a new-generation tool for improving balance, health and well-being? A pilot study. Climacteric 2010, 13, 487–491. [Google Scholar] [CrossRef]
- Nilsagard, Y.; Forsberg, A.; Von Koch, L. Balance exercise for persons with multiple sclerosis using Wii games: A randomised, controlled multi-center study. Mult. Scler. J. 2013, 19, 209–216. [Google Scholar] [CrossRef]
- Brichetto, G.; Spallarossa, P.; De Carvalho, M.; Battaglia, M. The effect of Nintendo® Wii® on balance in people with multiple sclerosis: A pilot randomized control study. Mult. Scler. J. 2013, 19, 1219–1221. [Google Scholar] [CrossRef]
- Thomas, S.; Fazakarley, L.; Thomas, P.W.; Collyer, S.; Brenton, S.; Perring, S.; Scott, R.; Thomas, F.; Thomas, C.; Jones, K.; et al. Mii-vitaliSe: A pilot randomised controlled trial of a home gaming system (Nintendo Wii) to increase activity levels, vitality and well-being in people with multiple sclerosis. BMJ Open 2017, 7, e016966. [Google Scholar] [CrossRef]
- Mocanu, D.C.; Mocanu, E.; Nguyen, P.H.; Gibescu, M.; Liotta, A. A topological insight into restricted Boltzmann machines. Mach. Learn. 2016, 104, 243–270. [Google Scholar] [CrossRef] [Green Version]
- Mocanu, D.; Exarchakos, G.; Liotta, A. Decentralized dynamic understanding of hidden relations in complex networks. Sci. Rep. 2018, 8, 1571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celesti, A.; Celesti, F.; Fazio, M.; Villari, M. Improving Tele-Rehabilitation Therapy through Machine Learning with a NoSQL Graph DBMS Approach. In Proceedings of the 2020 IEEE Globecom Workshops (GC Wkshps), Taipei, Taiwan, 7–11 December 2020. [Google Scholar] [CrossRef]
- Zhu, M.; Zhang, Z.; Hirdes, J.; Stolee, P. Using machine learning algorithms to guide rehabilitation planning for home care clients. BMC Med. Inform. Decis. Mak. 2007, 7, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Celesti, A.; Lay-Ekuakille, A.; Wan, J.; Fazio, M.; Celesti, F.; Romano, A.; Bramanti, P.; Villari, M. Information management in IoT cloud-based tele-rehabilitation as a service for smart cities: Comparison of NoSQL approaches. Meas. J. Int. Meas. Confed. 2020, 151, 107218. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wii 20 (47.6%) | SR 22 (52.3%) | p-Value | |
|---|---|---|---|
| M/F (%) | 11/9 (55) | 15/7 (68) | ns |
| Age (years)a | ns | ||
| Disease durationa | ns | ||
| RR (%) | 1 (5) | 1 (4.5) | ns |
| RR plus seq (%) | 8 (40) | 9 (40.9) | ns |
| SP (%) | 7 (35) | 7 (31.8) | ns |
| PP (%) | 4 (20) | 5 (22.7) | ns |
| EDSSa | ns | ||
| BBSa | ns | ||
| F25WTa | ns | ||
| FIMa | 0.07 | ||
| FIMmfa | 0.04 | ||
| Self-Care | ns | ||
| Sphincters | ns | ||
| Transfers | <0.05 | ||
| Locomotions | 0.03 | ||
| FIMcfa | ns | ||
| Communication | ns | ||
| Cognition | ns |
| Wii T0 | Wii T1 | SR T0 | SR T1 | p-Value | |
|---|---|---|---|---|---|
| BBS | * <0.001 | ||||
| F25WT | ns | ||||
| FIM | *∘ <0.001 §0.05 | ||||
| FIMmf | *∘ <0.001 | ||||
| Self-Care | ∘ 0.06 | ||||
| Sphincters | ns | ||||
| Transfers | *∘ <0.005 | ||||
| Locomotions | * 0.01 ∘ 0.001 | ||||
| FIMcf | ns | ||||
| Communication | ns | ||||
| Cognition | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Celesti, A.; Cimino, V.; Naro, A.; Portaro, S.; Fazio, M.; Villari, M.; Calabró, R.S. Recent Considerations on Gaming Console Based Training for Multiple Sclerosis Rehabilitation. Med. Sci. 2022, 10, 13. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010013
Celesti A, Cimino V, Naro A, Portaro S, Fazio M, Villari M, Calabró RS. Recent Considerations on Gaming Console Based Training for Multiple Sclerosis Rehabilitation. Medical Sciences. 2022; 10(1):13. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010013
Chicago/Turabian StyleCelesti, Antonio, Vincenzo Cimino, Antonino Naro, Simona Portaro, Maria Fazio, Massimo Villari, and Rocco Salvatore Calabró. 2022. "Recent Considerations on Gaming Console Based Training for Multiple Sclerosis Rehabilitation" Medical Sciences 10, no. 1: 13. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010013