
The Dorsomedian Ligamentous Strand: An Evaluation In Vivo with Epiduroscopy


1
Mininvasive Surgery Department, Unit of Pain Medicine IRCCS Maugeri Pavia, 27100 Pavia, Italy
2
I Service Anesthesia, Critical Care, Azienda Ospedaliero Universitaria Parma, 43121 Parma, Italy
3
ISAL Foundation, Institute for Pain Research, 47900 Rimini, Italy
*
Author to whom correspondence should be addressed.
Med. Sci. 2022, 10(1), 18; https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010018
Submission received: 20 December 2021
/
Revised: 23 January 2022
/
Accepted: 4 March 2022
/
Published: 7 March 2022
(This article belongs to the Section Neurosciences)
Abstract
:Several anatomical studies have described the morphology of the spinal space; however, researchers do not all agree on the presence of the dorsomedian ligamentous strand (DLS), which divides the epidural space. The possible existence of this structure still influences some clinical practice, such as locoregional anesthesia and pain therapy. Since the number of procedures occurring inside the epidural space have increased, this study’s primary objective was to describe the composition of this space through epiduroscopy. We conducted a retrospective analysis of video recorded during epiduroscopy. Two independent doctors performed blind analyses of morphological aspects of peridural space visualized during the procedure in each patient for the maximum possible extension depending on the underlying pathology in the tract from S1 to L1. We enrolled 106 patients who underwent epiduroscopy; 100% of patients presented no medial longitudinal segmentation dividing the epidural channel at any level of the spinal tract investigated, including in the epidural space with pathological fibrotic scars and in those with no adherence. The main finding of our study was the visual absence of any anatomical structure dividing the epidural channel. We report that in vivo, in our experience, with direct epiduroscopy, the DLS is not visible.
1. Introduction
Since the 1900s, many anatomical studies have attempted to describe the structural and morphological features of the spinal space [1]. Despite the many procedures developed over the years using the anatomical and functional specificity of this space and surgical practices on its components, little is known about the composition of the epidural space. Although this space is a common site of interventional and surgical procedures, few studies have investigated this anatomical compartment.
In addition to orthopedic surgeons, neurosurgeons, and anesthesiologists, pain therapists, radiologists, and neurologists work on the epidural space for diagnostic and therapeutic purposes by applying anatomical landmarks based on dated studies [1].
A division of the epidural space into two compartments has been described since 1970 using names such as “plica mediana dorsalis” [2] or “dorsomedian dural fold” [3]. This segmentation is considered real despite some papers that encourage reflection on the evidence of this “dorsomedian ligament” [4]. Analyzing the studies conducted on this anatomical structure, which specify its morphological characteristics, indicates that, while some support its presence based on anatomical verification or CT documentation, others deny it, considering it an autoptic artifact.
The existence of a median segmentation has been controversial since its first description in 1963 [5]. Luyendijk first described the so-called “plica mediana dorsalis” using epidurography and then confirmed its discovery, in 1976, by photographs taken during laminectomy [2]. In 1980, Husemeyer and White published a study showing this segmentation (defined as a dorsomedian dural fold), having injected polyester resin into the epidural space of adult cadavers [3]. Through endoscopy, Blomberg [6] et al. described a band of connective tissue on the dorsal midline of the epidural space in 48 analyzed cadavers. Furthermore, in 1989, Savolaine [7], using CT to examine the epidural space, identified, in all 40 patients studied, that the posterior epidural space was divided by a DLS and supplementary radial connective tissue. However, a debate was immediately sparked concerning whether the DLS existed or was only an artifact. In 1991, Hogan [8], through analyzing cryomicrotome sections of the lumbar spines of 38 frozen cadavers (obtained within 15 h of death), showed that no median ligamentous strand appeared in any of them. The ligament would probably reflect an artifact due to the dural tension (in the presence of an unnatural transmural pressure during distention of the epidural space).
Introducing endoscopic procedures did not improve this uncertainty. Blomberg documented the presence of connective tissue between the rear of the dural sac and the yellow ligament defined as “dorsomedian ligamentous strands”, which, due to the traction exerted on the dura, produced the plica mediana dorsalis [6]. This anatomical theory was countered by cadaveric anatomical studies [9] and using endoscopic procedures that improved the resolution power with adequate optical sources over the years. This debate is not only theoretical since it reflects on the choice of procedure: anesthesiological selective block [10], neuromodulation/neurostimulation methods for pain therapy [4], and minimally invasive spinal surgery [11]. Since epidural space procedures to relieve pain and provide anesthesia are gaining broader therapeutic value, and the use of therapeutic epiduroscopy is increasing [12,13,14], we believe it is useful to review the composition of the spinal space.
This study aims to highlight the presence or absence of signs supporting the existence of the ligament by in vivo epiduroscopic analysis.
2. Materials and Methods
The epiduroscopy procedures were performed in the context of the PainOmics study. The authorizations of the ethics committee and informed consent signed by all the patients allowed for the analysis of video recorded for retrospective study and clinical reasons. We made a retrospective review of the video recorded during the execution of epiduroscopy procedures performed from 2014 to 2016 in a single center by a single operator.
Patients were enrolled with the following inclusion criteria:
- -
- Age 18–85 years
- -
- Patients with failed back surgery syndrome (FBSS) and spinal stenosis
- -
- Able to sign an informed consent form
The following exclusion criteria were applied:
- -
- Patients with clinically unstable disease (all morbid forms whose treatment is not stable over time but requires continuous pharmacological and dosage adjustments or require further investigations)
- -
- Patients who have been diagnosed with severe neuropsychiatric disease and have received pharmacological treatment under constant medical supervision for which there is a contraindication for invasive treatments
- -
- History of vertebral fractures
- -
- Tumors or infections affecting the spine
- -
- Visual impairment (glaucoma, diabetic retinopathy)
- -
- Chronic primary or secondary headache
- -
- Pregnancy
- -
- Coagulopathies (INR > 1.5)
General medical aspects (unstable primary pathologies recommend a waiting attitude for non-urgent procedures) and specific clinical aspects for the epiduroscopy maneuver defined the exclusion criteria to limit the risks of infectious and neurological complications as reported in the literature [15].
For each patient, we analyzed images related to the macroscopic morphology of the contents of the epidural space from S1 to T12–L1. Particularly, we searched for a DLS (and whether it appears as a small embryo), which should divide the epidural space according to previous literature [13].
The channel was explored within the most extensive tract from S1 to L1 allowed by the patient’s pathology.
For each video, analysis was performed independently by two clinicians who were experts in epiduroscopy (more than 100 procedures each). In case of non-agreement, the video was reviewed by the most expert operator (Dr. Raffaeli) for a third opinion.
For a detailed description of the epiduroscopy, refer to previously published articles [15].
3. Results
We analyzed videos of 106 patients (41 men and 65 women) with a median age of 58 years.
The diagnoses that led to the indication of periduroscopy are summarized in Table 1.
We included 11 cases (10%) in the data analysis where it was impossible to explore at least up to L2.
Cases where it was impossible to explore at least up to L3 (4%) were excluded from data analysis.
The macroscopic composition of the epidural space includes the epidural channel, dura, roots, and yellow ligament.
Independently from the pain syndrome described in the diagnosis, 100% of patients presented no medial longitudinal structure dividing the channel.
Due to an abnormal laxity of the dura in one case (0.16%), we observed a segmentation-like feature secondary to the traction exerted by the video guide and Fogarty balloon working, which induced a shake.
The video analysis enabled some original images to be obtained that could explain how it could be possible to find morphological abnormalities responsible for false radiological findings in some cases.
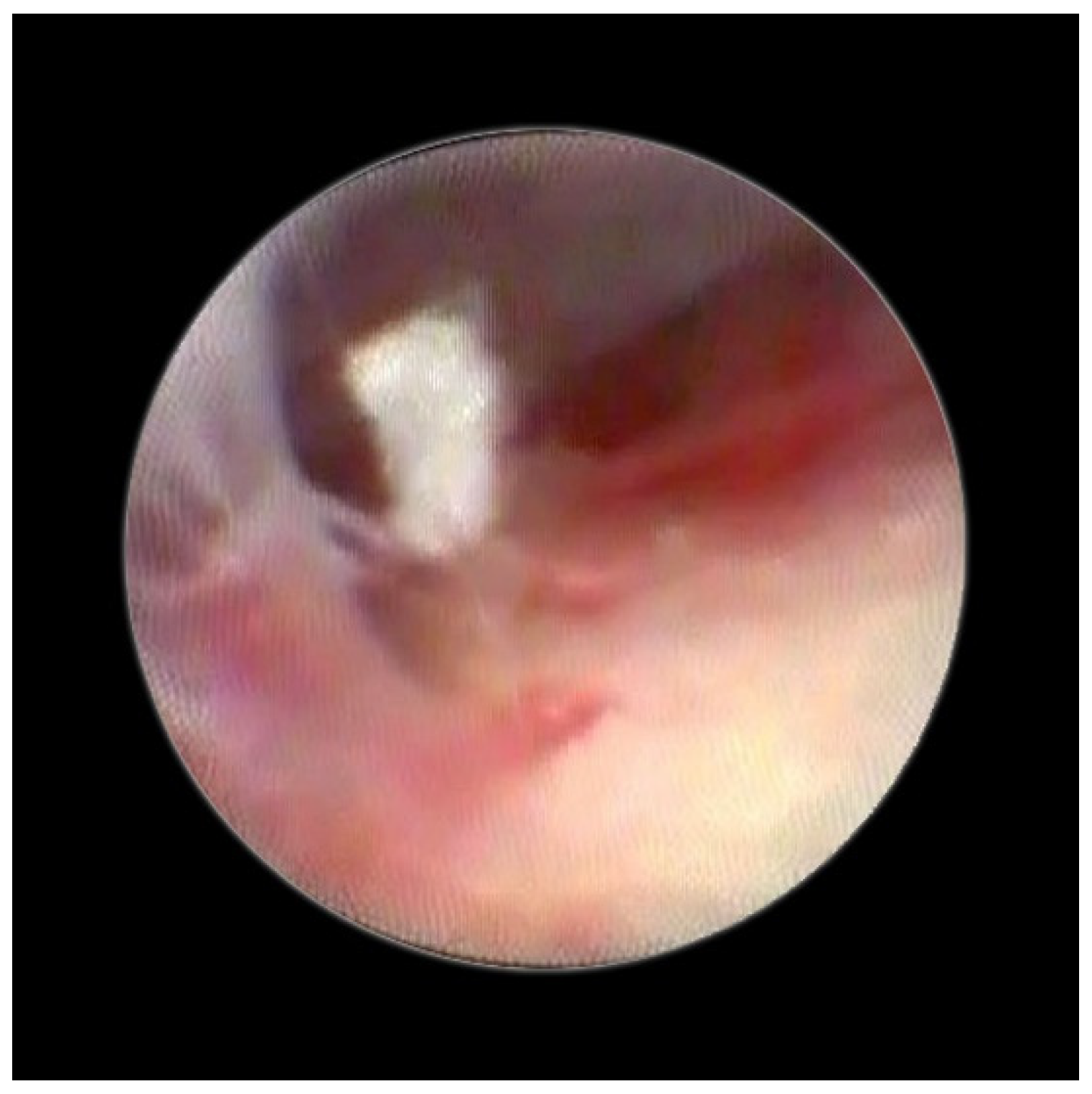
Figure 1 enables visualization of the composition of the normal dura and the other structure and directly indicates the absence of any median strand.
Figure 2 shows the lifting of the meningeal dura for dural mobility abnormalities with an underlying lifting of the spinal root, which determines a pseudo-lifting of the dura, potentially resulting in a false diagnostic radiology interpretation of a median ligament. Moreover, the presence of a Fogarty catheter inside the bed of the dura in the midline causes lifting of the dura mater in relation to the root below, which can mimic a false longitudinal ligament in radiodiagnostic imaging (Figure 3). Morphological analysis of the pathological spaces also showed that, in these cases, no segmentation occurred. The left side of Figure 4 shows a fibrotic septum grafted on the dura. However, underlying dural bases exhibit no segmentation.
4. Discussion
Our previous studies have highlighted that epidural space has different morphological characteristics based on the presence or absence of alterations of the dural cloth, roof, vessels, and channel. This study confirms, in a significant number of patients, what we had previously reported [14]: no connective septum exists in the epidural space. None of the patients in our study showed a medial longitudinal ligament.
Our in vivo experience does not confirm the findings arising from the initial endoscopic procedures by Blomberg [6] and suggests that the DLS may be a cadaver artifact.
In the first diagnostic part of the procedure, a low volume of saline (between 20 and 100 mL) was used; we suppose that this small volume cannot be hidden or modify the presence of a solid structure from yellow ligament to dural meningeal pannus.
Thus, an even larger volume (300–500 mL), as used during the therapeutic phase of adherence lysis, probably cannot change the anatomy of a hypothetical DLS.
The presence of fibrotic septa, without apparent cause and limited to a single vertebral body, was detected in a few cases. In our video review, we found one patient with a segmentation-like feature. This appeared to be the result of a raising of the dura due to loss of its elasticity and the presence of a hyperpressure on the dural cloth (Figure 2), as previously reported [16].
We consider that the descriptions given by many authors of images obtained through endoscopy or radiological imaging can be attributed to errors due to the technology of cadaver fixation, according to Morisot [17]. Alternatively, they may be interpretations of a dorsal membrane in pathologies (i.e., compartmental fibrosis in stenosis) that present features that CT cannot detect. A polyester resin print of epidural space with injection in cadavers has shown only in a few cases a faint dorso-median fold of the dura [18].
The study was carried out more accurately through the injection of contrast medium after insertion of epidural catheter. The execution of both CT and spiral CT and MRI showed, but only at the thoracic level, the presence of a fold, however, with an extensive presentation variable [19].
At the lumbar level, there are not, to our knowledge, similar rigorous studies. The most recent literature only shows anectodical descriptions of dorsal plica during diagnostic radiological studies (such as for oncological pathologies) [19].
In accordance with Hogan [9], we believe that the membrane could be attributed to raising of the dural cloth due to pressure secondary to the use of rigid instruments on the dura (Figure 3). Moreover, in the presence of tractions secondary to pathological events (such as post-surgical or post-inflammatory fibrosis) on the dura mater, the membrane could be raised by generating, with its “sail” shape, a segmentation-like feature [16] (Figure 4). Hogan claimed that in addition to the absence of any “fibrous barrier across the intervertebral neural canals” a narrow fibrous band could sometimes be seen adjacetn to the superior edge of pedicle epidural space … and epidural space is widely open on its lateral aspect” [8]. Asato published a paper indicating that no obstacle existed to the spread of epidural solution due to a median epidural septum, and the epidurography, performed in seven patients with unilateral epidural block, showed that the cause of the unilateral block was the placement of the catheter into the anterior or transforaminal epidural space [18]. Transversal segmentation, which divides the space into two sections, can be present in subjects with diseases secondary to chronic polyfactorial stenosis or where previous spinal surgery justifies abnormalities in fluid distribution, based on the CT findings by Savolaine [7].
5. Conclusions
Our video analysis involved over 100 patients, a significant number for a “subjective” visual analysis such as the one we performed. This evaluation cannot be definitive but raises further doubts concerning the existence of the DLS in vivo, particularly due to the total absence in any patient of signs of its presence.
Further studies in vivo, with high-resolution neuroimaging (for example, 3 Tesla MRI) or with fresh cadavers, could support or reject the hypothesis of the existence of a structure partitioning the posterior epidural space.
Author Contributions
W.R. performed the conceptualization of the study, surgical procedures, and the final revision of the paper. M.M. performed surgical procedures and video analysis and wrote the original draft. E.S. performed video analysis, revised the original draft, and conducted bibliography research. All authors have read and agreed to the published version of the manuscript.
Funding
The epiduroscopy procedures were performed with support from a grant of the European FP7 Collaborative Project: PainOmics—multidimensional OMIC approach in stratification of patients with low back pain (grant agreement 602736). The video analysis was performed without the support of a research fund.
Institutional Review Board Statement
The epiduroscopies were conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of the University of Parma (protocol code 13479, date 15 April 2014). The video analyses did not require further approval from the ethics committee, as they were conducted on data already archived, with patient anonymity and aggregated data.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study regarding the periduroscopy procedure. All patients were informed of the registration of the procedure for clinical and research purposes.
Data Availability Statement
The data presented in this study are not available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Sample Availability
Samples of the compounds are not available from the authors.
References
- MacIntosh, R.R.; Mushin, W.W. Observations on the epidural space. Anaesthesia 1947, 2, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Luyendijk, W. The plica mediana dorsalis of the dura mater and its relation to lumbar peridurography (Canalography). Neuroradiology 1976, 11, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Husemeyer, R.P.; White, D.C. Topography of the lumbar epidural space. A study in cadavers using injected polyester resin. Anaesthesia 1980, 35, 7–11. [Google Scholar]
- Stevens, D.S.; Balkany, A.D. Appearance of plica mediana dorsalis during epidurography. Pain Phys. 2006, 9, 268–270. [Google Scholar]
- Luyendijk, W. Canalography. Roentgenological examination of the peridural space in the lumbo-sacral part of the vertebral canal. J. Belg. Radiol. 1963, 46, 236–254. [Google Scholar] [PubMed]
- Blomberg, R. The dorsomedian connective tissue band in the lumbar epidural space of humans: An anatomical study using epiduroscopy in autopsy cases. Anesth. Analg. 1986, 65, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Savolaine, E.R.; Pandya, J.B.; Greenblatt, S.H.; Conover, S.R. Anatomy of the human lumbar epidural space: New insights using CT-epidurography. Anesthesiology 1988, 68, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Hogan, Q.H. Lumbar Epidural Anatomy A New Look by Cryomicrotome Section. Anesthesiology 1991, 75, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Hogan, Q. Distribution of solution in the epidural space: Examination by cryomicrotome section. Reg. Anesth. Pain Med. 2002, 27, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Gajraj, N.M. Selective nerve root blocks for low back pain and radiculopathy. Reg. Anesth. Pain Med. 2004, 9, 243–256. [Google Scholar] [CrossRef]
- Racz, G.B.; Heavner, J.E.; Trescot, A. Percutaneous Lysis of Epidural Adhesions—Evidence for Safety and Efficacy. Pain Pract. 2008, 8, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Manchikanti, L.; Boswell, M.V.; Raj, P.P.; Racz, G.B. Evolution of interventional pain management. Pain Phys. 2003, 6, 485–494. [Google Scholar]
- Raffaeli, W.; Righetti, D. Surgical radio-frequency epiduroscopy technique (R-ResAblator) and FBSS treatment: Preliminary evaluations. Acta Neurochir. Suppl. 2005, 92, 121–125. [Google Scholar] [PubMed]
- Raffaeli, W.; Righetti, D.; Andruccioli, J.; Sarti, D. Periduroscopy: General Review of Clinical Features and Development of Operative Models. Acta Neurochir. Suppl. 2010, 108, 55–65. [Google Scholar] [CrossRef]
- Marchesini, M.; Flaviano, E.; Bellini, V.; Baciarello, M.; Bignami, E.G. Complication of epiduroscopy: A brief review and case report. Korean J. Pain 2018, 31, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Raffaeli, W.; Sarti, D. Epidural space and chronic pain. Eur. J. Pain Suppl. 2010, 4, 269–272. [Google Scholar] [CrossRef]
- Morisot, P. Is posterior lumbar epidural space partitioned? Ann. Fr. Anesth. Reanim. 1992, 11, 72–81. [Google Scholar] [CrossRef]
- Asato, F.; Goto, F. What caused the unilateral epidurogram and bilateral epidural analgesia? Anesth. Analg. 1992, 75, 310–311. [Google Scholar] [CrossRef] [PubMed]
- Tomczak, R.; Seeling, W.; Rieber, A.; Sokiranski, R.; Rilinger, N.; Brambs, H.J. Epidurography: Comparison with CT, spiral CT and MR epidurography. Rofo Fortschr. Auf Dem Geb. Rontgenstrahlen Nukl. 1996, 165, 123–129. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Normal dura in epiduroscopy.

Figure 2.
Normal dura, root lifting.

Figure 3.
Fogarty catheter close to dura.

Figure 4.
Fibrotic septum in epidural space.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Description of types of chronic persistent lumbar pain with or without radicular pain.
| Diagnosis | Number N (%) |
|---|---|
| Peristent back pain secondary to spinal stenosis (ostogenic, discopaty) | 40 (37.7%) |
| Persistent pain secondary to spine surgery (failed back surgery syndrome) | 60 (56.7%) |
| Persistent back pain with no instrumental diagnosis | 4 (3.8%) |
| Pain from extra-spinal conditions (traumatic sacrococcygeal pain) without documented lumbar disease | 2 (1.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Marchesini, M.; Schiappa, E.; Raffaeli, W. The Dorsomedian Ligamentous Strand: An Evaluation In Vivo with Epiduroscopy. Med. Sci. 2022, 10, 18. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010018
AMA Style
Marchesini M, Schiappa E, Raffaeli W. The Dorsomedian Ligamentous Strand: An Evaluation In Vivo with Epiduroscopy. Medical Sciences. 2022; 10(1):18. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010018
Chicago/Turabian StyleMarchesini, Maurizio, Eleonora Schiappa, and William Raffaeli. 2022. "The Dorsomedian Ligamentous Strand: An Evaluation In Vivo with Epiduroscopy" Medical Sciences 10, no. 1: 18. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010018
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.