
ARNI Pre-Operative Use and Vasoplegic Syndrome in Patients Undergoing Heart Transplantation or Left Ventricular Assist Device Surgery

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Vasoplegic Syndrome Definition
- -
- normal cardiac function by a transthoracic echocardiogram (left ventricular ejection fraction 55% or greater),
- -
- cardiac index > 2.2 L/min/m2
- -
- requirement a norepinephrine intravenous perfusion > 0.5 µg/kg/min for more than 24 h in the first 48 h postoperatively to maintain a mean arterial pressure ≥ 65 mm Hg
- -
- and the absence of documented sepsis or hemorrhagic shock.
- -
- ARNI
- -
- Other Renin-angiotensin blockers (ACEi and ARBs)
- -
- Norepinephrine
- -
- Absence of any vasoactive pre-operative treatment (reference group)
2.3. Study Endpoints
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Pre-Operative Treatment Use and VS
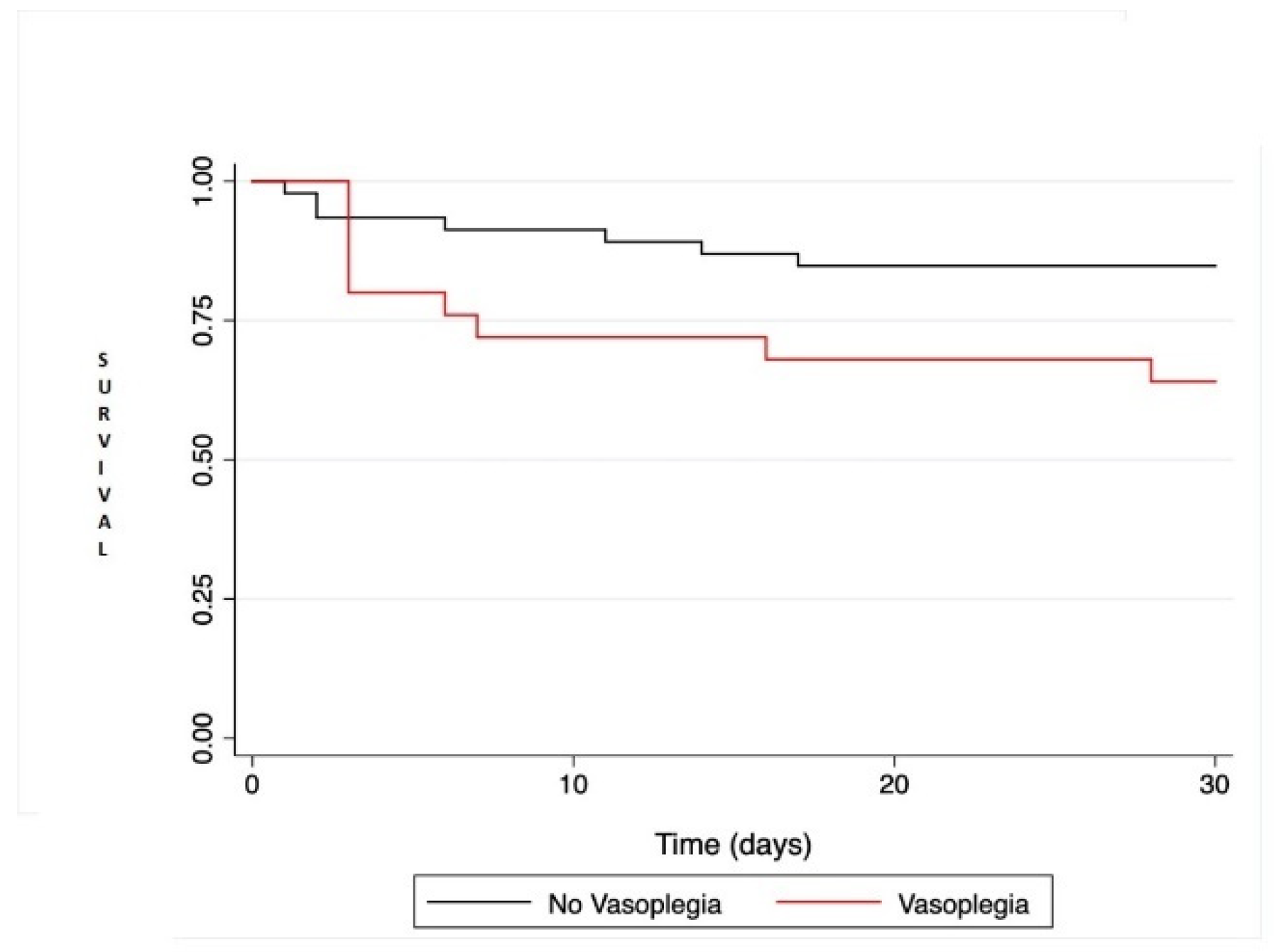
3.3. Vasoplegia and Adverse Outcomes
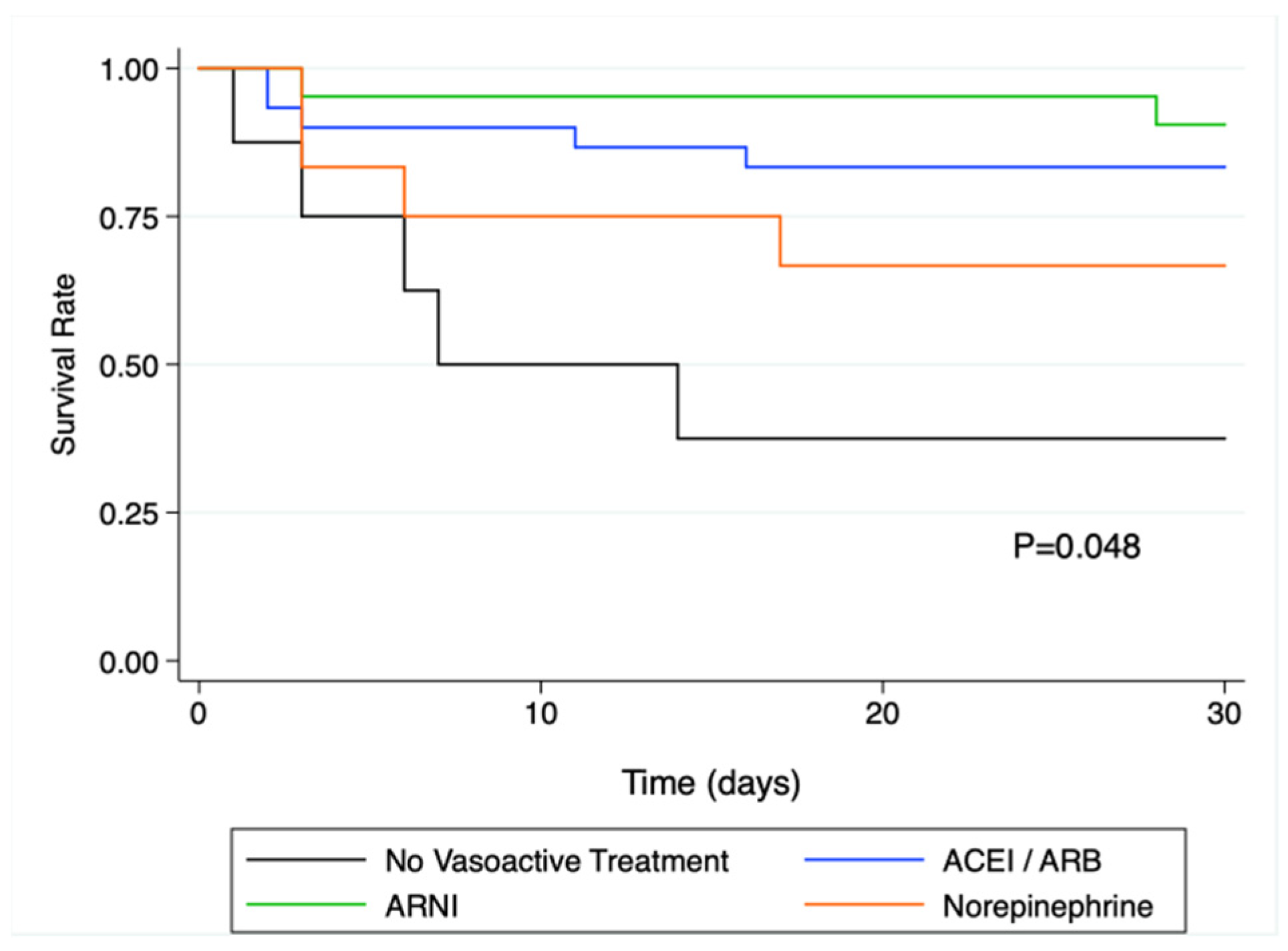
3.4. Preoperative Vasoactive Treatment and 30-Day Outcomes
4. Discussion
5. Limitations
6. Conclusions
7. Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fischer, G.W.; Levin, M.A. Vasoplegia During Cardiac Surgery: Current Concepts and Management. Semin. Thorac. Cardiovasc. Surg. 2010, 22, 140–144. [Google Scholar] [CrossRef]
- Chemmalakuzhy, J.; Costanzo, M.; Meyer, P.; Piccione, W.; Kao, W.; Winkel, E.; Saltzberg, M.; Heroux, A.; Parrillo, J. Hypotension, acidosis, and vasodilatation syndrome post–heart transplant: Prognostic variables and outcomes. J. Heart Lung Transplant. 2001, 20, 1075–1083. [Google Scholar] [CrossRef]
- Wan, S.; Marchant, A.; DeSmet, J.-M.; Antoine, M.; Zhang, H.; Vachiery, J.-L.; Goldman, M.; Vincent, J.-L.; LeClerc, J.-L. Human cytokine responses to cardiac transplantation and coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 1996, 111, 469–477. [Google Scholar] [CrossRef]
- Levin, R.L.; Degrange, M.A.; Bruno, G.F.; Del Mazo, C.D.; Taborda, D.J.; Griotti, J.J.; Boullon, F.J. Methylene blue reduces mortality and morbidity in vasoplegic patients after cardiac surgery. Ann. Thorac. Surg. 2004, 77, 496–499. [Google Scholar] [CrossRef]
- Argenziano, M.; Chen, J.M.; Choudhri, A.F.; Cullinane, S.; Garfein, E.; Weinberg, A.D.; Smith, C.R.; Rose, E.A.; Landry, D.W.; Oz, M.C. Management of vasodilatory shock after cardiac surgery: Identification of predisposing factors and use of a novel pressor agent. J. Thorac. Cardiovasc. Surg. 1998, 116, 973–980. [Google Scholar] [CrossRef] [Green Version]
- Lambden, S.; Creagh-Brown, B.C.; Hunt, J.; Summers, C.; Forni, L.G. Definitions and pathophysiology of vasoplegic shock. Crit. Care 2018, 22, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Cremer, J.; Martin, M.; Redl, H.; Bahrami, S.; Abraham, C.; Graeter, T.; Haverich, A.; Schlag, G.; Borst, H.-G. Systemic inflammatory response syndrome after cardiac operations. Ann. Thorac. Surg. 1996, 61, 1714–1720. [Google Scholar] [CrossRef]
- Mcmurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. N. Engl. J. Med. 2014, 5, 132–133. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Almufleh, A.; Mielniczuk, L.M.; Zinoviev, R.; Moeller, A.; Davies, R.A.; Stadnick, E.; Chan, V.; Chih, S. Profound Vasoplegia During Sacubitril/Valsartan Treatment After Heart Transplantation. Can. J. Cardiol. 2018, 34, 343.e5–343.e7. [Google Scholar] [CrossRef]
- Papadopoulos, G.; Sintou, E.; Siminelakis, S.; Koletsis, E.; Baikoussis, N.G.; Apostolakis, E. Perioperative infusion of low- dose of vasopressin for prevention and management of vasodilatory vasoplegic syndrome in patients undergoing coronary artery bypass grafting-A double-blind randomized study. J. Cardiothorac. Surg. 2010, 5, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colson, P.H.; Bernard, C.; Struck, J.; Morgenthaler, N.G.; Albat, B.; Guillon, G. Post cardiac surgery vasoplegia is associated with high preoperative copeptin plasma concentration. Crit. Care 2011, 15, R255. [Google Scholar] [CrossRef] [Green Version]
- Kortekaas, K.A.; Lindeman, J.H.; Reinders, M.; Palmen, M.; Klautz, R.J.; De Groot, P.G.; Roest, M. Pre-existing endothelial cell activation predicts vasoplegia after mitral valve surgery. Interact. Cardiovasc. Thorac. Surg. 2013, 17, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Colson, P.; Saussine, M.; Séguin, J.R.; Cuchet, D.; Chaptal, P.A.; Roquefeuil, B. Hemodynamic effects of anesthesia in patients chronically treated with angiotensin-converting enzyme inhibitors. Anesth. Analg. 1992, 74, 805–808. [Google Scholar] [CrossRef]
- Yates, A.P.; Hunter, D.N. Anaesthesia and angiotensin-converting enzyme inhibitors: The effect of enalapril on peri-operative cardiovascular stability. Anaesthesia 1988, 43, 935–938. [Google Scholar] [CrossRef] [PubMed]
- Kataja, J.H.; Kaukinen, S.; Viinamäki, O.V.; Metsä-Ketelä, T.J.; Vapaatalo, H. Hemodynamic and hormonal changes in patients pretreated with captopril for surgery of the abdominal aorta. J. Cardiothorac. Anesth. 1989, 3, 425–432. [Google Scholar] [CrossRef]
- Thaker, U.; Geary, V.; Chalmers, P.; Sheikh, F. Low systemic vascular resistance during cardiac surgery: Case reports, brief review, and management with angiotensin II. J. Cardiothorac. Anesth. 1990, 4, 360–363. [Google Scholar] [CrossRef]
- Sousa-Uva, M.; Head, S.J.; Milojevic, M.; Collet, J.-P.; Landoni, G.; Castella, M.; Dunning, J.; Gudbjartsson, T.; Linker, N.J.; Sandoval, E.; et al. 2017 EACTS Guidelines on perioperative medication in adult cardiac surgery. Eur. J. Cardio-Thorac. Surg. 2017, 53, 5–33. [Google Scholar] [CrossRef] [Green Version]
- Raja, S.G.; Fida, N. Should angiotensin converting enzyme inhibitors/angiotensin II receptor antagonists be omitted before cardiac surgery to avoid postoperative vasodilation? Interact. Cardiovasc. Thorac. Surg. 2008, 7, 470–475. [Google Scholar] [CrossRef] [Green Version]
- Velazquez, E.J.; Morrow, D.; Devore, A.D.; Duffy, C.I.; Ambrosy, A.P.; McCague, K.; Rocha, R.; Braunwald, E. Angiotensin–Neprilysin Inhibition in Acute Decompensated Heart Failure. N. Engl. J. Med. 2019, 380, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Ruilope, L.M.; Dukat, A.; Böhm, M.; Lacourcière, Y.; Gong, J.; Lefkowitz, M.P. Blood-pressure reduction with LCZ696, a novel dual-acting inhibitor of the angiotensin II receptor and neprilysin: A randomised, double-blind, placebo-controlled, active comparator study. Lancet 2010, 375, 1255–1266. [Google Scholar] [CrossRef]
- Domínguez, J.M.; García-Romero, E.; Pàmies, J.; Mirabet, S.; González-Costello, J.; Spitaleri, G.; Perez-Villa, F.; Farrero, M. Incidence of vasoplegic syndrome after cardiac transplantation in patients treated with sacubitril/valsartan. Clin. Transplant. 2020, 34, e13994. [Google Scholar] [CrossRef]
- Yandrapalli, S.; Andries, G.; Biswas, M.; Khera, S. Profile of sacubitril/valsartan in the treatment of heart failure: Patient selection and perspectives. Vasc. Health Risk Manag. 2017, 13, 369–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruno, R.M.; Taddei, S. Sacubitril/valsartan and low blood pressure in heart failure with reduced ejection fraction. Eur. Heart J. 2017, 38, 1144–1146. [Google Scholar] [CrossRef] [PubMed]
- Vardeny, O.; Claggett, B.; Kachadourian, J.; Pearson, S.M.; Desai, A.S.; Packer, M.; Rouleau, J.; Zile, M.R.; Swedberg, K.; Lefkowitz, M.; et al. Incidence, Predictors, and Outcomes Associated With Hypotensive Episodes Among Heart Failure Patients Receiving Sacubitril/Valsartan or Enalapril: The PARADIGM-HF Trial (Prospective Comparison of Angiotensin Receptor Neprilysin Inhibitor With Angioten-sin-Converting Enzyme Inhibitor to Determine Impact on Global Mortality and Morbidity in Heart Failure). Circ. Heart Fail. 2018, 11, e004745. [Google Scholar] [CrossRef] [PubMed]
- Truby, L.K.; Takeda, K.; Farr, M.; Beck, J.; Yuzefpolskaya, M.; Colombo, P.C.; Topkara, V.K.; Mancini, D.; Naka, Y.; Takayama, H. Incidence and Impact of On-Cardiopulmonary Bypass Vasoplegia During Heart Transplantation. ASAIO J. 2018, 64, 43–51. [Google Scholar] [CrossRef]
- Byrne, J.G.; Leacche, M.; Paul, S.; Mihaljevic, T.; Rawna, J.D.; Shernan, S.K.; Mudge, G.H.; Stevenson, L.W. Risk factors and outcomes for ‘vasoplegia syndrome’ following cardiac transplantation. Eur. J. Cardio-Thorac. Surg. 2004, 25, 327–332. [Google Scholar] [CrossRef] [Green Version]
- Patarroyo, M.; Simbaqueba, C.; Shrestha, K.; Starling, R.C.; Smedira, N.; Tang, W.W.; Taylor, D.O. Pre-operative risk factors and clinical outcomes associated with vasoplegia in recipients of orthotopic heart transplantation in the contemporary era. J. Heart Lung Transplant. 2011, 31, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Berger, R.; Kuchling, G.; Frey, B.; Kozanly, I.; Pacher, R.; Stanek, B. ACE inhibitor dosage at the time of listing predicts survival. J. Heart Lung Transplant. 2000, 19, 127–133. [Google Scholar] [CrossRef]
- Fearon, W.F.; Okada, K.; Kobashigawa, J.A.; Kobayashi, Y.; Luikart, H.; Sana, S.; Daun, T.; Chmura, S.A.; Sinha, S.; Cohen, G.; et al. Angiotensin-Converting Enzyme Inhibition Early After Heart Transplantation. J. Am. Coll. Cardiol. 2017, 69, 2832–2841. [Google Scholar] [CrossRef]
- Ding, Q.; Zhang, Z.; Liu, H.; Nie, H.; Berguson, M.; Goldhammer, J.E.; Young, N.; Boyd, D.; Morris, R.; Sun, J. Perioperative use of renin-angiotensin system inhibitors and outcomes in patients undergoing cardiac surgery. Nat. Commun. 2019, 10, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Baseline Characteristics | VS− (n = 48) | VS+ (n = 25) | Total (n = 73) | p |
|---|---|---|---|---|
| Age [years] | 50.9 ± 11.5 | 53.3 ± 12.3 | 51.7 ± 11.7 | 0.41 |
| Sex, male, n (%) | 42 (87.5%) | 23 (92%) | 65 (89%) | 0.71 |
| BMI [kg/m2] | 25.1 ± 4.1 | 25.9 ± 4.9 | 25.3 ± 4.4 | 0.47 |
| LVEF < 35%, n (%) | 45 (93.8%) | 20 (80%) | 65 (89%) | 0.11 |
| Euroscore II | 15.8 ± 9.9 | 17.5 ± 12.7 | 16.4 ± 10.9 | 0.53 |
| Pre transplant treatment n (%) | 0.30 | |||
| No vasoactive treatment | 5 (10.4%) | 3 (12%) | 8 (11%) | |
| ACEI/ARB | 24 (50%) | 7 (28%) | 31 (42.5%) | |
| ARNI | 12 (25%) | 10 (40%) | 22 (30.1%) | |
| Norepinephrine | 7 (14.6%) | 5 (20%) | 12 (16.4%) | |
| Betablockers | 25 (52.1%) | 13 (52%) | 38 (52.1%) | 1.00 |
| Initial Cardiac Disease, n (%) | 0.41 | |||
| ICM | 16 (33.3%) | 12 (48%) | 28 (38.4%) | |
| DCM | 17 (35.4%) | 6 (24%) | 23 (31.5%) | |
| HCM | 3 (6.3%) | 2 (8%) | 5 (6.8%) | |
| Two or more sternotomies | 6 (12.5%) | 6 (24%) | 12 (16.4%) | 0.32 |
| Type of surgery, n (%) | ||||
| Transplantation | 35 (72.9%) | 19 (76%) | 54 (74%) | 1.00 |
| LVAD | 13 (27.1%) | 6 (24%) | 19 (26%) | 1.00 |
| Pump time, min | 125.6 ± 45.5 | 125.6 ± 48.6 | 125.6 ± 40.1 | 0.91 |
| GFR ml/min | 60.9 ± 29.7 | 52.1 ± 26.0 | 57.9 ± 28.7 | 0.21 |
| ECMO, n (%) | 21 (43.8%) | 13 (52%) | 34 (46.6%) | 0.62 |
| Bleeding complications, n (%) | 7 (14.6%) | 7(28% | 14 (19.2%) | 0.21 |
| Septic event at 30 days, n (%) | 0.76 | |||
| No sepsis | 26 (54.1%) | 12 (48%) | 38 (52.1%) | |
| No documented sepsis | 12 (25%) | 6 (24%) | 18 (24.7%) | |
| Documented sepsis | 10 (20.83%) | 7 (28%) | 17 (23.3%) |
| No Vasoactive Treatment (n = 8) | ACEI/ARBs (n = 31) | ARNI (n = 22) | Norepinephrine (n = 12) | F-Test | |
|---|---|---|---|---|---|
| Norepinephrine duration, days | 3.9 ± 2.3 | 4.7 ± 4.7 | 7.1 ± 6.8 | 10.3 ± 9.3 | 0.045 |
| Norepinephrine, maximal dose mcg/kg/min | 1.5 ± 1.4 | 1.0 ± 0.9 | 1.0 ± 0.6 | 1.1 ± 0.9 | 0.65 |
| Post-Operative Adverse Event | VS− (n = 48) | VS+ (n = 25) | p-Value |
|---|---|---|---|
| Death at 30-days n, (%) | 9 (18.8) | 9 (36.0) | 0.051 |
| Sepsis/infection n, (%) | 22 (45.8) | 13 (52.0) | 0.61 |
| Hemorrhagic complication n, (%) | 7 (14.5) | 7 (28) | 0.17 |
| Renal Replacement Therapy n, (%) | 14 (29.2) | 17 (68) | 0.001 |
| Mesenteric ischemia n, (%) | 1 (2.08) | 4 (16) | 0.025 |
| Peripheral ischemia n, (%) | 0 (0) | 2 (8) | 0.047 |
| Invasive ventilation time, days | 5 ± 6 | 9 ± 11 | 0.06 |
| HR | 95% CI | p Value | |
|---|---|---|---|
| Preoperative treatment: | |||
| - RASi | 0.25 | 0.07–0.92 | 0.038 |
| - ARNI | 0.18 | 0.03–1.15 | 0.070 |
| - Norepinephrine | 0.42 | 0.11–1.65 | 0.217 |
| Age | 1.04 | 0.99–1.10 | 0.085 |
| LVEF | 0.76 | 0.18–3.16 | 0.707 |
| ECS duration | 1.02 | 1.01–1.04 | 0.010 |
| Surgery type | 2.53 | 0.51–12.56 | 0.255 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haider, L.; Hugon-Vallet, E.; Constantin, J.P.; Riad, Z.; Sebbag, L.; Mewton, N. ARNI Pre-Operative Use and Vasoplegic Syndrome in Patients Undergoing Heart Transplantation or Left Ventricular Assist Device Surgery. Med. Sci. 2022, 10, 2. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010002
Haider L, Hugon-Vallet E, Constantin JP, Riad Z, Sebbag L, Mewton N. ARNI Pre-Operative Use and Vasoplegic Syndrome in Patients Undergoing Heart Transplantation or Left Ventricular Assist Device Surgery. Medical Sciences. 2022; 10(1):2. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010002
Chicago/Turabian StyleHaider, Lamis, Elisabeth Hugon-Vallet, Jean Philippe Constantin, Zakaria Riad, Laurent Sebbag, and Nathan Mewton. 2022. "ARNI Pre-Operative Use and Vasoplegic Syndrome in Patients Undergoing Heart Transplantation or Left Ventricular Assist Device Surgery" Medical Sciences 10, no. 1: 2. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010002