
Emerging Tools to Capture Self-Reported Acute and Chronic Pain Outcome in Children and Adolescents: A Literature Review

 ,
,
Abstract
:1. Introduction
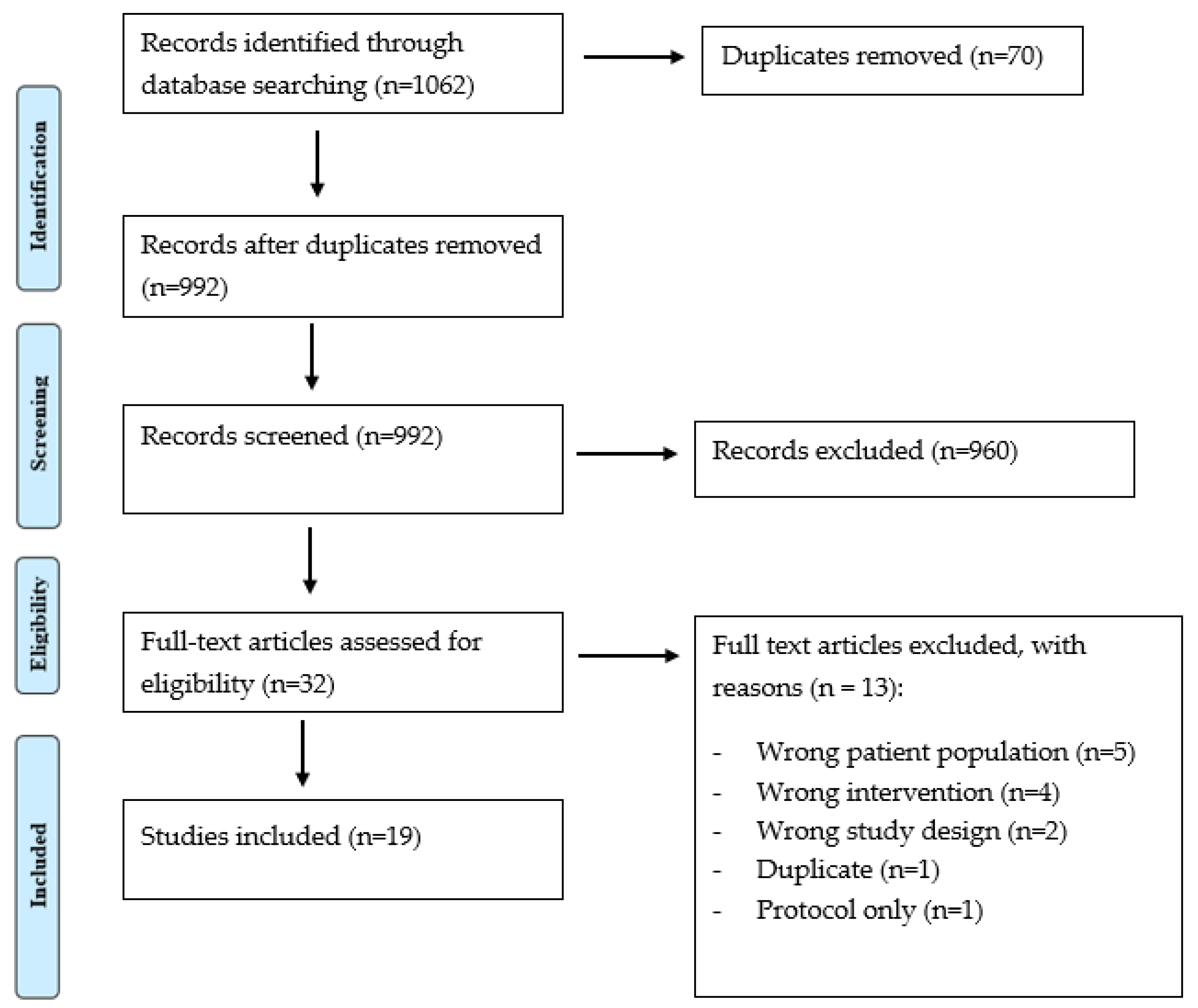
2. Materials and Methods
3. Results
4. Discussion
- (A)
- Electronic Devices, such as PC or laptops, where data is stored on the internal memory and then instantaneously uploaded to the cloud when a network is available or moved to an external device.
- (B)
- Smart Devices capable of WiFi connectivity or linked to 3G or 4G mobile networks. These devices are typically cordless, highly portable, with the option to capture the location of service, enable interactive text and voice call recording with the ability to take photos and videos. For example, these may include, but are not limited to: a Smartphone (i.e.: iPhone), tablet (i.e.: iPAD, Samsung Galaxy) or smart watch (i.e.: Apple watch). The advantages and disadvantages of these emerging technologies tested in children and adolescents, will form the basis of the following discussion.
4.1. Electronic Devices Used to Capture Symptom and Pain Progression
4.1.1. Electronic Diaries
4.1.2. PDA
4.1.3. Web-Based Multidimensional Pain Measure
4.1.4. Pain Measurement Tools Comparison
4.2. Smart Technology to Monitor Symptom and Pain Progression
4.3. Electronic and Smart Technology Compared to Traditional Outcome Measures
4.3.1. Clinical Implications and Considerations
4.3.2. Data Privacy
4.4. Digital Health and Clinical Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rabbitts, J.A.; Holley, A.L.; Groenewald, C.B.; Palermo, T.M. Association between widespread pain scores and functional impairment and health-related quality of life in clinical samples of children. J. Pain 2016, 17, 678–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hersh, A.O.; Salimian, P.K.; Weitzman, E.R. Using patient-reported outcome measures to capture the patient’s voice in research and care of juvenile idiopathic arthritis. Rheum. Dis. Clin. 2016, 42, 333–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miró, J.; Castarlenas, E.; Huguet, A. Evidence for the use of a numerical rating scale to assess the intensity of pediatric pain. Eur. J. Pain 2009, 13, 1089–1095. [Google Scholar] [CrossRef] [PubMed]
- Tsze, D.S.; von Baeyer, C.L.; Bulloch, B.; Dayan, P.S. Validation of self-report pain scales in children. Pediatrics 2013, 132, e971–e979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashikar-Zuck, S.; Carle, A.; Barnett, K.; Goldschneider, K.R.; Sherry, D.D.; Mara, C.A.; Cunningham, N.; Farrell, J.; Tress, J.; DeWitt, E.M. Longitudinal evaluation of patient-reported outcomes measurement information systems measures in pediatric chronic pain. Pain 2016, 157, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Garra, G.; Singer, A.J.; Taira, B.R.; Chohan, J.; Cardoz, H.; Chisena, E.; Thode, H.C., Jr. Validation of the Wong-Baker FACES pain rating scale in pediatric emergency department patients. Acad. Emerg. Med. 2010, 17, 50–54. [Google Scholar] [CrossRef]
- Cohen, L.L.; Vowles, K.E.; Eccleston, C. Adolescent chronic pain-related functioning: Concordance and discordance of mother-proxy and self-report ratings. Eur. J. Pain 2010, 14, 882–886. [Google Scholar] [CrossRef]
- Kamper, S.J.; Dissing, K.B.; Hestbaek, L. Whose pain is it anyway? Comparability of pain reports from children and their parents. Chiropr. Man. Ther. 2016, 24, 24. [Google Scholar] [CrossRef] [Green Version]
- Drendel, A.L.; Brousseau, D.C.; Gorelick, M.H. Pain assessment for pediatric patients in the emergency department. Pediatrics 2006, 117, 1511–1518. [Google Scholar] [CrossRef]
- Zisk-Rony, R.Y.; Lev, J.; Haviv, H. Nurses’ report of in-hospital pediatric pain assessment: Examining challenges and perspectives. Pain Manag. Nurs. 2015, 16, 112–120. [Google Scholar] [CrossRef]
- Quinn, B.L.; Sheldon, L.K.; Cooley, M.E. Pediatric pain assessment by drawn faces scales: A review. Pain Manag. Nurs. 2014, 15, 909–918. [Google Scholar] [CrossRef] [PubMed]
- Bird, M.-L.; Callisaya, M.L.; Cannell, J.; Gibbons, T.; Smith, S.T.; Ahuja, K.D. Accuracy, validity, and reliability of an electronic visual analog scale for pain on a touch screen tablet in healthy older adults: A clinical trial. Interact. J. Med. Res. 2016, 5, e4910. [Google Scholar] [CrossRef]
- Stone, A.A.; Shiffman, S.; Schwartz, J.E.; Broderick, J.E.; Hufford, M.R. Patient compliance with paper and electronic diaries. Control. Clin. Trials 2003, 24, 182–199. [Google Scholar] [CrossRef]
- Oliveira, N.; Gaspardo, C.; Linhares, M. Pain and distress outcomes in infants and children: A systematic review. Braz. J. Med. Biol. Res. 2017, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manworren, R.C.; Stinson, J. (Eds.) Pediatric Pain Measurement, Assessment, and Evaluation. In Seminars in Pediatric Neurology; Elsevier: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Palermo, T.M.; Valenzuela, D.; Stork, P.P. A randomized trial of electronic versus paper pain diaries in children: Impact on compliance, accuracy, and acceptability. Pain 2004, 107, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Fanciullo, G.J.; Cravero, J.P.; Mudge, B.O.; McHugo, G.J.; Baird, J.C. Development of a new computer method to assess children’s pain. Pain Med. 2007, 8 (Suppl. S3), S121–S128. [Google Scholar] [CrossRef] [PubMed]
- Stinson, J.N.; Stevens, B.J.; Feldman, B.M.; Streiner, D.; McGrath, P.J.; Dupuis, A.; Gill, N.; Petroz, G.C. Construct validity of a multidimensional electronic pain diary for adolescents with arthritis. Pain 2008, 136, 281–292. [Google Scholar] [CrossRef]
- Stinson, J.N.; Petroz, G.C.; Stevens, B.J.; Feldman, B.M.; Streiner, D.; McGrath, P.J.; Gill, N. Working out the kinks: Testing the feasibility of an electronic pain diary for adolescents with arthritis. Pain Res. Manag. 2008, 13, 375–382. [Google Scholar] [CrossRef] [Green Version]
- Cravero, J.P.; Fanciullo, G.J.; McHugo, G.J.; Baird, J.C. The validity of the Computer Face Scale for measuring pediatric pain and mood. Pediatric Anesth. 2013, 23, 156–161. [Google Scholar] [CrossRef]
- Stinson, J.N.; Jibb, L.A.; Lalloo, C.; Feldman, B.M.; McGrath, P.J.; Petroz, G.C.; Streiner, D.; Dupuis, A.; Gill, N.; Stevens, B. Comparison of average weekly pain using recalled paper and momentary assessment electronic diary reports in children with arthritis. Clin. J. Pain 2014, 30, 1044–1050. [Google Scholar] [CrossRef] [Green Version]
- Wood, C.; von Baeyer, C.L.; Falinower, S.; Moyse, D.; Annequin, D.; Legout, V. Electronic and paper versions of a faces pain intensity scale: Concordance and preference in hospitalized children. BMC Pediatr. 2011, 11, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luca, N.J.; Stinson, J.N.; Feldman, B.M.; Benseler, S.M.; Beaton, D.; Campillo, S.; LeBlanc, C.; van Wyk, M.; Bayoumi, A.M. Validation of the standardized universal pain evaluations for rheumatology providers for children and youth (SUPER-KIDZ). J. Orthop. Sports Phys. Ther. 2017, 47, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Jordan, A.; Begen, F.M.; Austin, L.; Edwards, R.T.; Connell, H. A usability and feasibility study of a computerized version of the Bath Adolescent Pain Questionnaire: The BAPQ-C. BMC Pediatr. 2020, 20, 6. [Google Scholar] [CrossRef] [PubMed]
- Stinson, J.N.; Jibb, L.; Nguyen, C.; Nathan, P.C.; Maloney, A.M.; Dupuis, L.; Gerstle, J.T.; Alman, B.; Hopyan, S.; Strahlendorf, C.; et al. Development and testing of a multidimensional iPhone pain assessment application for adolescents with cancer. J. Med. Internet Res. 2013, 15, e51. [Google Scholar] [CrossRef] [PubMed]
- Stinson, J.N.; Jibb, L.A.; Nguyen, C.; Nathan, P.C.; Maloney, A.M.; Dupuis, L.L.; Gerstle, J.T.; Hopyan, S.; Alman, B.A.; Strahlendorf, C.; et al. Construct validity and reliability of a real-time multidimensional smartphone app to assess pain in children and adolescents with cancer. Pain 2015, 156, 2607–2615. [Google Scholar] [CrossRef]
- Sun, T.; West, N.; Ansermino, J.M.; Montgomery, C.J.; Myers, D.; Dunsmuir, D.; Lauder, G.; Von Baeyer, C.L. A smartphone version of the Faces Pain Scale-Revised and the Color Analog Scale for postoperative pain assessment in children. Pediatric Anesth. 2015, 25, 1264–1273. [Google Scholar] [CrossRef]
- Cai, R.A.; Beste, D.; Chaplin, H.; Varakliotis, S.; Suffield, L.; Josephs, F.; Sen, D.; Wedderburn, L.R.; Ioannou, Y.; Hailes, S.; et al. Developing and evaluating JIApp: Acceptability and usability of a smartphone app system to improve self-management in young people with juvenile idiopathic arthritis. JMIR Mhealth Uhealth 2017, 5, e7229. [Google Scholar] [CrossRef] [Green Version]
- Jibb, L.A.; Stevens, B.J.; Nathan, P.C.; Seto, E.; Cafazzo, J.A.; Johnston, D.L.; Hum, V.; Stinson, J.N. Implementation and preliminary effectiveness of a real-time pain management smartphone app for adolescents with cancer: A multicenter pilot clinical study. Pediatric Blood Cancer 2017, 64, e26554. [Google Scholar] [CrossRef]
- Birnie, K.A.; Campbell, F.; Nguyen, C.; Lalloo, C.; Tsimicalis, A.; Matava, C.; Cafazzo, J.; Stinson, J. iCanCope PostOp: User-centered design of a smartphone-based app for self-management of postoperative pain in children and adolescents. JMIR Form. Res. 2019, 3, e12028. [Google Scholar] [CrossRef]
- Turnbull, A.; Sculley, D.; Escalona-Marfil, C.; Riu-Gispert, L.; Ruiz-Moreno, J.; Gironès, X.; Coda, A. Comparison of a Mobile Health Electronic Visual Analog Scale App With a Traditional Paper Visual Analog Scale for Pain Evaluation: Cross-Sectional Observational Study. J. Med. Internet Res. 2020, 22, e18284. [Google Scholar] [CrossRef]
- Martinez Garcia, E.; Catalan Escudero, P.; Mateos Arroyo, J.; Ramos Luengo, A.; Sanchez Alonso, F.; Reinoso Barbero FPainapple, R. Validation and evaluation of an electronic application for the management of acute pain in pediatric patients. Rev. Española Anestesiol. Reanim. 2020, 67, 139–146. [Google Scholar] [CrossRef]
- Lalloo, C.; Harris, L.R.; Hundert, A.S.; Berard, R.; Cafazzo, J.; Connelly, M.; Feldman, B.M.; Houghton, K.; Huber, A.; Laxer, R.M.; et al. The iCanCope pain self-management application for adolescents with juvenile idiopathic arthritis: A pilot randomized controlled trial. Rheumatology 2021, 60, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Rodriguez, E.; de la Vega, R.; Castarlenas, E.; Roset, R.; Miro, J. AN APP for the Assessment of Pain Intensity: Validity Properties and Agreement of Pain Reports When Used with Young People. Pain Med. 2015, 16, 1982–1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, M.; Al-Haiqi, A.; Zaidan, A.; Zaidan, B.; Kiah, M.; Iqbal, S.; Abdulnabi, M. A security framework for mHealth apps on Android platform. Comput. Secur. 2018, 75, 191–217. [Google Scholar] [CrossRef]
- Blenner, S.R.; Köllmer, M.; Rouse, A.J.; Daneshvar, N.; Williams, C.; Andrews, L.B. Privacy policies of android diabetes apps and sharing of health information. Jama 2016, 315, 1051–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfeld, L.; Torous, J.; Vahia, I.V. Data security and privacy in apps for dementia: An analysis of existing privacy policies. Am. J. Geriatr. Psychiatry 2017, 25, 873–877. [Google Scholar] [CrossRef]
- Thornton, S. Mobile phone use in children and young people: A public health concern? Br. J. Sch. Nurs. 2018, 13, 94–97. [Google Scholar] [CrossRef]
- Chiu, C.-T.; Chang, Y.-H.; Chen, C.-C.; Ko, M.-C.; Li, C.-Y. Mobile phone use and health symptoms in children. J. Formos. Med. Assoc. 2015, 114, 598–604. [Google Scholar] [CrossRef]
- Lanca, C.; Saw, S.M. The association between digital screen time and myopia: A systematic review. Ophthalmic Physiol. Opt. 2020, 40, 216–229. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| 1 | Pain outcome measure |
| 2 | Pain assess * |
| 3 | Pain measurem * |
| 4 | 1 or 2 or 3 |
| 5 | Child * |
| 6 | Adolescent.tw |
| 7 | 5 or 6 |
| 8 | Electronic * |
| 9 | Smartphone |
| 10 | Smart device |
| 11 | Smart-technolog * |
| 12 | 8 or 9 or 10 or 11 |
| 13 | Validation |
| 14 | Feasibility |
| 15 | 13 or 14 |
| 16 | 4 and 7 and 12 and 15 |
| Inclusion Criteria: | Exclusion Criteria: |
|---|---|
| Articles that do not explicitly state the exclusion of participants that have: | |
|
|
|
|
|
|
|
|
| Name | Study | Methodology and Sample | Findings | Limitations |
|---|---|---|---|---|
| Electronic pain outcome measures | ||||
| Electronic pain diary | Palermo et al., 2004 | Randomized clinical trial. n = 60, age range 8–16 mean=12.3 Headaches or Juvenile Idiopathic Arthritis | Children with e-diaries completed more days compared to p-diaries. P-diaries more errors. | Only included pain tracking at the end of the day, not multiple times of the day |
| Computer Face Scale | Fanciullo et al., 2007 | Cohort observational study evaluating feasibility of the computerised version of the Wong Baker Face scale. 54 in-patient children with mean age of 10.7; and a second convenience sample of 30 childrens with mean age of 7.2. Each sample used to test two objectives. | Authors reported that the majority (76%) of participants preferred to use the computer version over paper. Moreover, authors showed that children were able to show varying levels of emotion when expressing pain levels. | Data only collected at one time point and timeframe was not explicit. No control group. Difficult to quantitatively compare with other scales that use 0–10 numerical values. |
| eOuch | Stinson et al., 2008 | Descriptive study design. 13 adolescents with Juvenile Idiopathic Arthritis (JIA). | Participants required to complete eOuch 3 times per day. Most participants reported the ediary was easy to use. Phase 1 of study had 73% compliance and phase 2 had 70%. | Small sample size and sample only from one tertiary pediatric centre. Same patients were used in both usability and acceptability studies. |
| eOuch | Stinson et al., 2008 | A descriptive study design. Study 1: n = 76, age range 9–17, mean 13.4 Study 2: n = 36, age range 8–17, mean = 12.6 Rheumatology clinics | Data was collected by the children. Evidence of construct validity and feasibility of eOuch pain diary in adolescents with JIA. Provided more information (3 times a day) compared to Palermo et al. | 22% of data was missing potentially leading to a biased estimate of average weekly electronic pain ratings. |
| personal data assistants (PDA) FPS | Wood et al., 2011 | Observational, multicenter, randomized, cross-over, controlled, open trial. n = 202, age range 4–12. | Data was collected by hospitalised children. Mean levels of pain scores were 3.1 ± 2.3 and 3.2 ± 2.3 for paper and PDA scores, respectively. The mean absolute discrepancy between the two versions was not statistically different significant from zero | Participants from multiple wards—chronic disease and also day surgery. None of the studies had a mean time between the assessments of “less than 30 min” |
| Computer Face Scale | Cravero et al., 2013 | Validation study of the Computer Face Scale. Included 40 children aged 5–13 who underwent a tonsillectomy at Children’s Hospital at Dartmouth-Hitchcock Medical Center. Participants used a Dell Mobile PDA to display the face scale and arrows were used to cycle between each expression. | When comparing CFS to the verbal rating scale and wong baker scale, authors concluded good validity scores: “The correlation between the pain ratings from the Computer Face Scale and the Wong-Baker Faces Scale after surgery was 0.83”. | Sample population was limited to those undergoing surgery and therefore we were unable to generalise to other populations. No mention of CFS available for use on mobile phones and/or app stores across multiple devices. |
| eOuch | Stinson et al., 2014 | Construct validity study in children with JIA. Comparing momentary and recalled pain measurements with eOuch. 70 adolescent JIA participants. | Between-person momentary and recalled pain measurements showed a moderate Interclass Correlation Coeficient (ICC). Within-person measurements displayed weak ICC. | Sample sourced from one clinic. Study did not include a practice session. Weekly momentary analysis may have been influenced by 22% missing data reported. |
| SUPER-KIDZ | Luca et al., 2017 | Clinimetric study using prospectively collected repeated measures Study 1: n = 71, age range 8–18 Study 2: n = 29 (parent child dyads), age range 4–7 | For study 1, data was collected by the children Good internal consistency, responsiveness and satisfactory test–retest reliability. | Small sample size Reliability study compromised due to unstable pain levels |
| BAPQ-C | Jordan et al., 2020 | Fourteen adolescents with chronic pain (13 females; 13–16 years) were recruited from a hospital-based residential pain management programme. Qualitative study focusing on exploring the feasbility of the electronic version of Bath Adolescent Pain Questionnaire. | Authors reported high acceptability of the BAPQ-C. 93% of participants reported that the BAPQ-C was both ‘quicker’ and ‘easier’ to complete than the BAPQ. Only one participant preferred the paper version. | Small and specific sample population. Further validation required in patients outside hospital residential care. |
| Smart Technology Pain Outcome Measures | ||||
| Pain Squad | Stinson et al., 2013 | Usability, feasibility, compliance, and satisfaction study. Qualitative interviews followed by compliance and satisfaction data were obtained. 15 adolescents with cancer with average age of 13. | Participants during interviews provided feedback on the app and authors made adjustments accordingly. “88% of questions were rated as “important” or “very important by the majority (> 50%) of adolescents”. Compliance was high with mean of 81%. Authors also reported high satisfaction among the sample. | No direct examination of high compliance rates. App only accessed with iPhone or other apple devices. Information from interviewed participants was not verified with a follow-up interview. |
| Painometer | Sanchez Rodriguez et al., 2015 | Cross-Sectional Observational Study n = 180, age range 12–19 mean = 14.8 4 updated traditional outcome measures updated to smart devices | Data was collected by the children. 80% confidence interval—determined that they were interchangeable | Asked participants to remember maximum pain over last 3 months. Presentation order of scales was not randomised |
| Pain Squad | Stinson et al., 2015 | A prospective descriptive study design with repeated measures was used to test the construct validity, reliability, and feasibility. Study 1: n = 92, age range 8–18, mean 13.1. Study 2: n = 14, age range 9–18, mean 14.8 Pediatric cancer patients | Data was collected by the children Found that the multidimensional app was valid, reliable and feasible within a pediatric cancer setting | Small sample size in study 2—not enough participants recruited Measures collected morning and evening—may have missed other fluctuations leading to bias |
| Smartphone FPS-R and CAS | Sun et al., 2015 | observational, randomized, cross-over-controlled, open trial. Study 1: n = 62, age range 4–12, mean 7.5 Study 2: n = 66, age range 5–18 mean 13 Children scheduled for surgery with anticipated post operative pain | Data was collected by the children Panda correlated strongly with original scores. Mean pain scores higher in application compared to original tool—systematic bias, within clinical significance (80%) | Not multi dimensionsional—27% of scores were 0 on the FPS-R. Did not assess reliability of application. One sample location. |
| JIApp | Cai et al., 2017 | Design, develop, and evaluate the acceptability and usability of JIApp. 3 phase study on children with JIA. Participants ranged from ages 10–24 across the phased study. Three themes: (1) Remote monitoring; (2) Treatment adherence; (3) Education and Support. | Ability for patients with JIA to report and monitor several parameters associated with their disease including but not limited to pain, joint symptoms, psychological well-being, activity limitation. Young JIA patients reported a mean acceptability rating of 4.29 and expressed multiple benefits of the app. | Limited sample size. Will require further validation in a larger clinical trial. |
| Pain Squad+ | Jibb et al., 2017 | An cohort prospective design of adolescents ranging from 12–18 who were currently undergoing cancer treatment. 40 participants were recruited with a mean age of 14.2. | Overall adherence of Pain Squad+ was 77.2%. Acceptability e-scaled showed a minimum average of 3 in all items assessed indicating satisfactory acceptability. | Single group design. No control group. Pilot study and therefore requires further investigation on a larger sample size. |
| iCanCope PostOp app | Birnie et al., 2019 | User-centered design study with 2 principle phases. (1) Semi-structured interviews, (2) 2-stage Delphi Survey. 19 children with mean age of 15.26 who underwent surgery within a 7-day period were recruited. iCanCope: a smartphone-based app for children and adolescents’ self-management of acute postoperative pain. | All participants reported the three proposed features of the app as important (pain tracking, pain advice, and goal setting). Multiple features were proposed by participants, parents and health care workers. These include but are not limited to: Pain advice within the app; goal setting; direct communication with health care providers and medication tracking were also proposed. | Convenience sample. Potentially limited by a lack of comprehensiveness of all types of surgeries for potential end users. |
| Interactive Clinics App | Turnbull et al., 2020 | Cross-Sectional Observational Study. 47 children and adolescents (mean age 13.9 years, SD 2.89 years; range 10–18 years). | Authors concluded moderate to good ICC when interchanging the eVAS and pVAS. | Convenience sample. Possibly lower reliability in children/adolescent sample due to differences in scale sizes fo VAS measuring line. |
| PainAPPle® | Martínez García et al., 2020 | Descriptive cohort study of 44 paediatric patients post surgery. Mean age = 11.3. | Data were collected by children after they recovered from their anaesthetic post-surgery. PainAPPle was used at 30 min intervals to measure pain and other post-operative outcomes. Statistically significant correlations were produced when comparing the electronic and paper versions of PainAPPle. | Specific population sample. Not generalisable. Requires further testing for validation. |
| iCanCope app | Lalloo et al., 2021 | Feasibility and pilot RCT for the iCanCope app in adolescents with JIA. 60 adolescents with JIA recruited and randomised to a control or trial intervention. Mean age = 15.0. Trial invervention/condition was the iCanCope app + self management features. The control group only received the iCanCope app (no self-management). | Both study conditions were deployed with high success. Pain intensity improved in both groups by 1.73 (intervention) and 1.09 (control). No significant changes in quality of life or pain-related activity limitations. Overall, the app was adhered to well and acceptable to most adolescent JIA patients with pain. | Requires a third arm (with just usual care, i.e., no app) to assess the effectiveness of iCanCope on outcomes in children with JIA. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Turnbull, A.; Sculley, D.; Santos, D.; Maarj, M.; Chapple, L.; Gironès, X.; Fellas, A.; Coda, A. Emerging Tools to Capture Self-Reported Acute and Chronic Pain Outcome in Children and Adolescents: A Literature Review. Med. Sci. 2022, 10, 6. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010006
Turnbull A, Sculley D, Santos D, Maarj M, Chapple L, Gironès X, Fellas A, Coda A. Emerging Tools to Capture Self-Reported Acute and Chronic Pain Outcome in Children and Adolescents: A Literature Review. Medical Sciences. 2022; 10(1):6. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010006
Chicago/Turabian StyleTurnbull, Alexandra, Dean Sculley, Derek Santos, Mohammed Maarj, Lachlan Chapple, Xavier Gironès, Antoni Fellas, and Andrea Coda. 2022. "Emerging Tools to Capture Self-Reported Acute and Chronic Pain Outcome in Children and Adolescents: A Literature Review" Medical Sciences 10, no. 1: 6. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10010006