
Clinical Impact of Immune Checkpoint Inhibitor (ICI) Response, DNA Damage Repair (DDR) Gene Mutations and Immune-Cell Infiltration in Metastatic Melanoma Subtypes

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Immunohistochemistry Staining and Scoring
2.3. Targeted Sequencing and Analysis
2.4. Statistical Analysis
3. Results
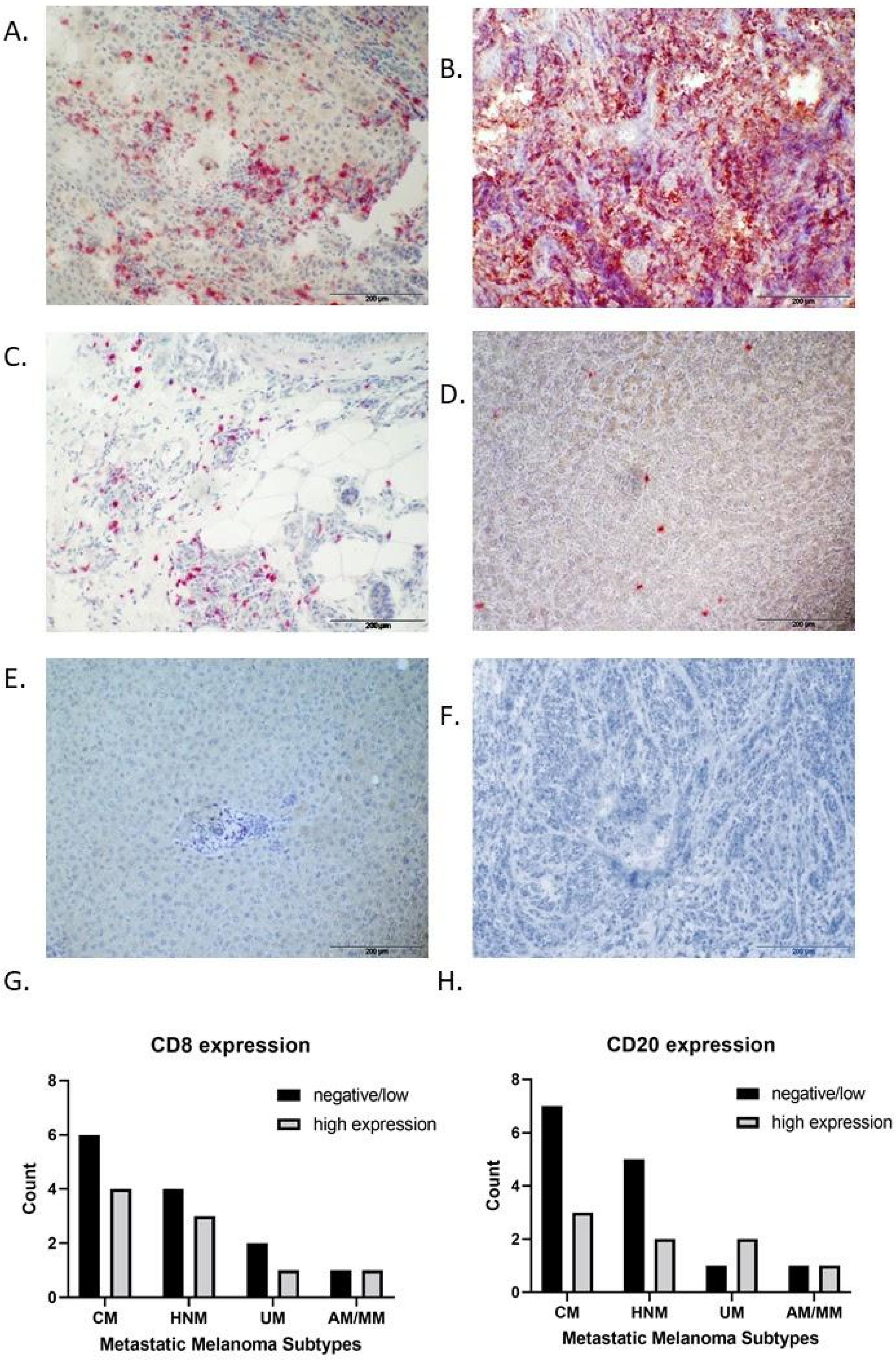
3.1. IHC Expression of CD8 and CD20 in Metastatic Melanoma Subtypes
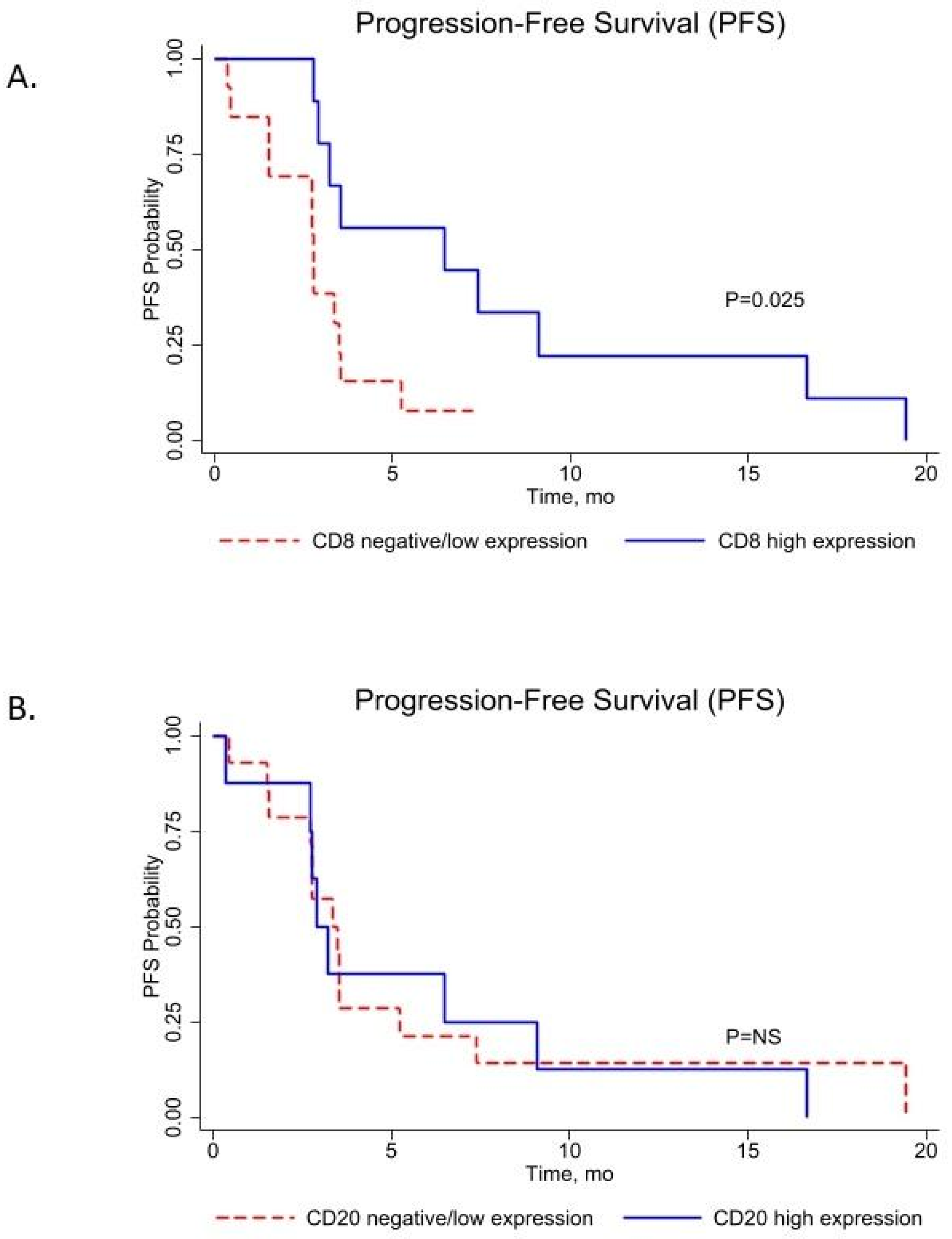
3.2. CD8 and CD20 Cell Infiltration Score Associated with Progression-Free Survival (PFS) in Metastatic Melanoma Subtypes
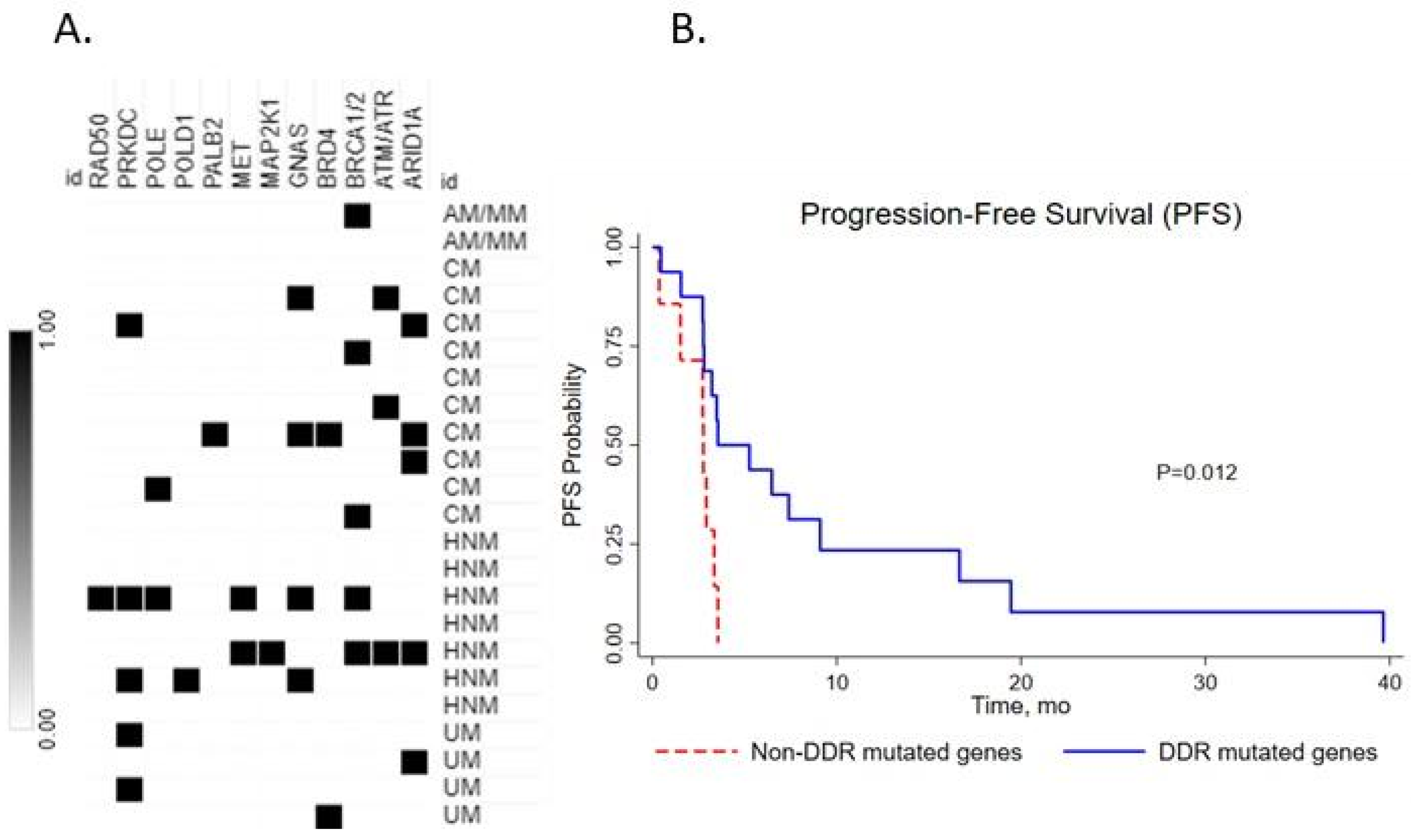
3.3. Impact of DNA Damage Repair (DDR) Gene Mutation on Clinical Outcome
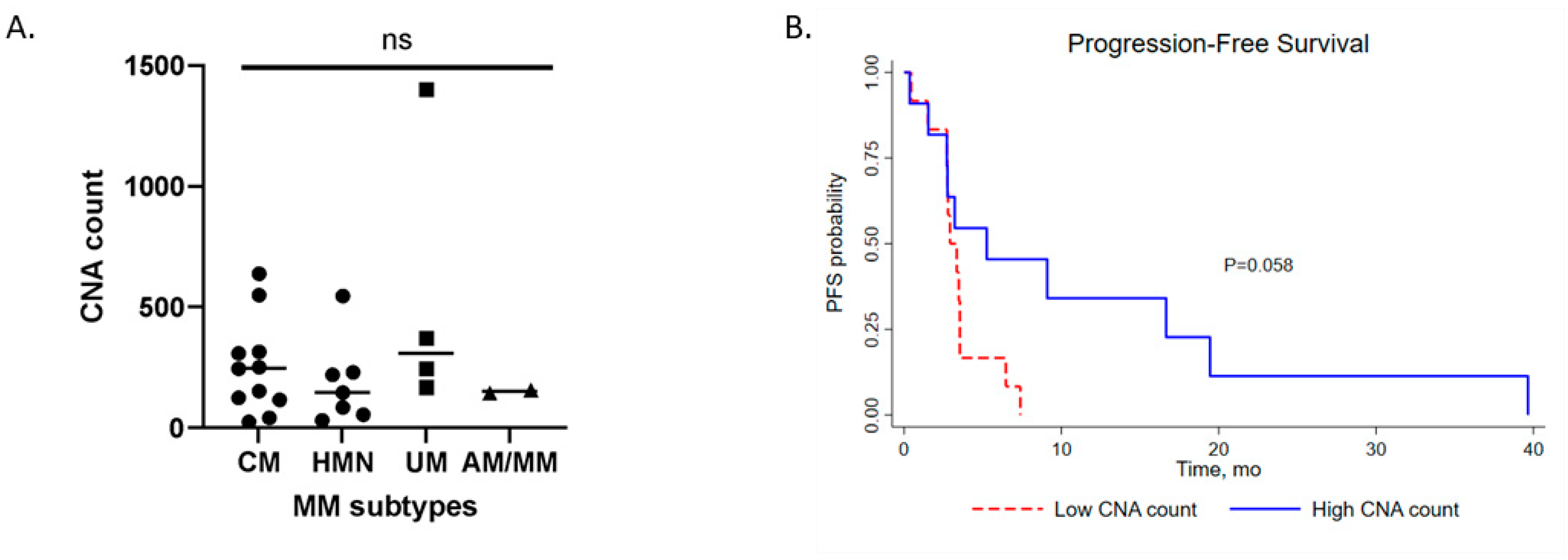
3.4. Copy Number Aberrations (CNA) of Metastatic Melanoma Subtypes and Clinical Impact
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, C.; Thomas, L.; Bondarenko, I.; O’Day, S.; Weber, J.; Garbe, C.; Lebbe, C.; Baurain, J.-F.; Testori, A.; Grob, J.-J.; et al. Ipilimumab plus Dacarbazine for Previously Untreated Metastatic Melanoma. N. Engl. J. Med. 2011, 364, 2517–2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prieto, P.A.; Yang, J.C.; Sherry, R.M.; Hughes, M.S.; Kammula, U.S.; White, D.E.; Levy, C.L.; Rosenberg, S.A.; Phan, G.Q. CTLA-4 Blockade with Ipilimumab: Long-Term Follow-up of 177 Patients with Metastatic Melanoma. Clin. Cancer Res. 2012, 18, 2039–2047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, L.; Garraway, L.A.; Fisher, D.E. Malignant Melanoma: Genetics and Therapeutics in the Genomic Era. Genes Dev. 2006, 20, 2149–2182. [Google Scholar] [CrossRef] [Green Version]
- Tas, F.; Keskin, S.; Karadeniz, A.; Daǧoǧlu, N.; Sen, F.; Kilic, L.; Yildiz, I. Noncutaneous Melanoma Have Distinct Features from Each Other and Cutaneous Melanoma. Oncology 2012, 81, 353–358. [Google Scholar] [CrossRef]
- Whiteman, D.C.; Pavan, W.J.; Bastian, B.C. The Melanomas: A Synthesis of Epidemiological, Clinical, Histopathological, Genetic, and Biological Aspects, Supporting Distinct Subtypes, Causal Pathways, and Cells of Origin. Pigment Cell Melanoma Res. 2011, 24, 879–897. [Google Scholar] [CrossRef] [Green Version]
- Shashanka, R.; Smitha, B.R. Head and Neck Melanoma. ISRN Surg. 2012, 2012, 143–152. [Google Scholar] [CrossRef] [Green Version]
- Al-Qurayshi, Z.; Hassan, M.; Srivastav, S.; Sperry, S.; Pagedar, N.; Hamner, J.; Kandil, E. Risk and Survival of Patients with Head and Neck Cutaneous Melanoma: National Perspective. Oncology 2017, 93, 18–28. [Google Scholar] [CrossRef]
- Zito, P.M.; Scharf, R. Melanoma of the Head and Neck. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Rabbie, R.; Ferguson, P.; Molina-Aguilar, C.; Adams, D.J.; Robles-Espinoza, C.D. Melanoma Subtypes: Genomic Profiles, Prognostic Molecular Markers and Therapeutic Possibilities. J. Pathol. 2019, 247, 539–551. [Google Scholar] [CrossRef]
- Chacón, M.; Pfluger, Y.; Angel, M.; Waisberg, F.; Enrico, D. Uncommon Subtypes of Malignant Melanomas: A Review Based on Clinical and Molecular Perspectives. Cancers 2020, 12, 2362. [Google Scholar] [CrossRef]
- Johnson, D.B.; Peng, C.; Abramson, R.G.; Ye, F.; Zhao, S.; Wolchok, J.D.; Sosman, J.A.; Carvajal, R.D.; Ariyan, C.E. Clinical Activity of Ipilimumab in Acral Melanoma: A Retrospective Review. Oncologist 2015, 20, 648–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klemen, N.D.; Wang, M.; Rubinstein, J.C.; Olino, K.; Clune, J.; Ariyan, S.; Cha, C.; Weiss, S.A.; Kluger, H.M.; Sznol, M. Survival after Checkpoint Inhibitors for Metastatic Acral, Mucosal and Uveal Melanoma. J. Immunother. Cancer 2020, 8, e000341. [Google Scholar] [CrossRef] [PubMed]
- Bai, R.; Lv, Z.; Xu, D.; Cui, J. Predictive Biomarkers for Cancer Immunotherapy with Immune Checkpoint Inhibitors. Biomark. Res. 2020, 8, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Schatz, S.; Falk, M.; Jóri, B.; Ramdani, H.O.; Schmidt, S.; Willing, E.M.; Menon, R.; Groen, H.J.M.; Diehl, L.; Kröger, M.; et al. Integration of Tumor Mutation Burden and PD-L1 Testing in Routine Laboratory Diagnostics in Non-Small Cell Lung Cancer. Cancers 2020, 12, 1685. [Google Scholar] [CrossRef]
- Chen, E.Y.; Tan, C.M.; Kou, Y.; Duan, Q.; Wang, Z.; Meirelles, G.V.; Clark, N.R.; Ma’ayan, A. Enrichr: Interactive and Collaborative HTML5 Gene List Enrichment Analysis Tool. BMC Bioinform. 2013, 14, 128. [Google Scholar] [CrossRef] [Green Version]
- Kuleshov, M.V.; Jones, M.R.; Rouillard, A.D.; Fernandez, N.F.; Duan, Q.; Wang, Z.; Koplev, S.; Jenkins, S.L.; Jagodnik, K.M.; Lachmann, A.; et al. Enrichr: A Comprehensive Gene Set Enrichment Analysis Web Server 2016 Update. Nucleic Acids Res. 2016, 44, W90–W97. [Google Scholar] [CrossRef] [Green Version]
- Xie, Z.; Bailey, A.; Kuleshov, M.V.; Clarke, D.J.B.; Evangelista, J.E.; Jenkins, S.L.; Lachmann, A.; Wojciechowicz, M.L.; Kropiwnicki, E.; Jagodnik, K.M.; et al. Gene Set Knowledge Discovery with Enrichr. Curr. Protoc. 2021, 1, e90. [Google Scholar] [CrossRef]
- Grossman, J.E.; Vasudevan, D.; Joyce, C.E.; Hildago, M. Is PD-L1 a Consistent Biomarker for Anti-PD-1 Therapy? The Model of Balstilimab in a Virally-Driven Tumor. Oncogene 2021, 40, 1393–1395. [Google Scholar] [CrossRef]
- Naumann, R.W.; Hollebecque, A.; Meyer, T.; Devlin, M.-J.; Oaknin, A.; Kerger, J.; López-Picazo, J.M.; Machiels, J.-P.; Delord, J.-P.; Evans, T.R.J.; et al. Safety and Efficacy of Nivolumab Monotherapy in Recurrent or Metastatic Cervical, Vaginal, or Vulvar Carcinoma: Results From the Phase I/II CheckMate 358 Trial. J. Clin. Oncol. 2019, 37, 2825–2834. [Google Scholar] [CrossRef]
- Kefford, R.; Ribas, A.; Hamid, O.; Robert, C.; Daud, A.; Wolchok, J.D.; Joshua, A.M.; Hodi, F.S.; Gangadhar, T.C.; Hersey, P.; et al. Clinical Efficacy and Correlation with Tumor PD-L1 Expression in Patients (Pts) with Melanoma (MEL) Treated with the Anti-PD-1 Monoclonal Antibody MK-3475. J. Clin. Oncol. 2014, 32 (Suppl. 15), 3005. [Google Scholar] [CrossRef]
- Mehra, R.; Seiwert, T.Y.; Gupta, S.; Weiss, J.; Gluck, I.; Eder, J.P.; Burtness, B.; Tahara, M.; Keam, B.; Kang, H.; et al. Efficacy and Safety of Pembrolizumab in Recurrent/Metastatic Head and Neck Squamous Cell Carcinoma: Pooled Analyses after Long-Term Follow-up in KEYNOTE-012. Br. J. Cancer 2018, 119, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.; Delord, J.-P.; Perets, R.; Italiano, A.; Shapira-Frommer, R.; Manzuk, L.; Piha-Paul, S.; Xu, L.; Jin, F.; Norwood, K.; et al. Pembrolizumab Treatment of Advanced Cervical Cancer: Updated Results from the Phase II KEYNOTE-158 Study. Gynecol. Oncol. 2021, 162, S27. [Google Scholar] [CrossRef]
- Shain, A.H.; Bastian, B.C. From Melanocytes to Melanomas. Nature Reviews Cancer. Nat. Rev. Cancer 2016, 16, 345–358. [Google Scholar] [CrossRef]
- Pham, T.V.; Boichard, A.; Goodman, A.; Riviere, P.; Yeerna, H.; Tamayo, P.; Kurzrock, R. Role of Ultraviolet Mutational Signature versus Tumor Mutation Burden in Predicting Response to Immunotherapy. Mol. Oncol. 2020, 14, 1680–1694. [Google Scholar] [CrossRef]
- Paijens, S.T.; Vledder, A.; de Bruyn, M.; Nijman, H.W. Tumor-Infiltrating Lymphocytes in the Immunotherapy Era. Cell. Mol. Immunol. 2020, 18, 842–859. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Bollin, K.; de Macedo, M.P.; Carapeto, F.; Kim, K.B.; Roszik, J.; Wani, K.M.; Reuben, A.; Reddy, S.T.; Williams, M.D.; et al. Immune Profiling of Uveal Melanoma Identifies a Potential Signature Associated with Response to Immunotherapy. J. Immunother. Cancer 2020, 8, e000960. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; de Macedo, M.P.; Reuben, A.; Forget, M.-A.; Haymaker, C.; Bernatchez, C.; Spencer, C.N.; Gopalakrishnan, V.; Reddy, S.; Cooper, Z.A.; et al. Parallel Profiling of Immune Infiltrate Subsets in Uveal Melanoma versus Cutaneous Melanoma Unveils Similarities and Differences: A Pilot Study. Oncoimmunology 2017, 6, e1321187. [Google Scholar] [CrossRef] [Green Version]
- Eroglu, Z.; Zaretsky, J.M.; Hu-Lieskovan, S.; Kim, D.W.; Algazi, A.; Johnson, D.B.; Liniker, E.; Kong, B.; Munhoz, R.; Rapisuwon, S.; et al. High Response Rate to PD-1 Blockade in Desmoplastic Melanomas. Nature 2018, 553, 347–350. [Google Scholar] [CrossRef]
- Frydenlund, N.; Leone, D.; Yang, S.; Hoang, M.P.; Deng, A.; Hernandez-Perez, M.; Singh, R.; Biswas, A.; Yaar, R.; Mahalingam, M. Tumoral PD-L1 Expression in Desmoplastic Melanoma Is Associated with Depth of Invasion, Tumor-Infiltrating CD8 Cytotoxic Lymphocytes and the Mixed Cytomorphological Variant. Mod. Pathol. 2017, 30, 357–369. [Google Scholar] [CrossRef]
- Kraft, S.; Fernandez-Figueras, M.-T.; Richarz, N.A.; Flaherty, K.T.; Hoang, M.P. PDL1 Expression in Desmoplastic Melanoma Is Associated with Tumor Aggressiveness and Progression. J. Am. Acad. Dermatol. 2017, 77, 534–542. [Google Scholar] [CrossRef]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor Mutational Burden and Response Rate to PD-1 Inhibition. N. Engl. J. Med. 2017, 377, 2500. [Google Scholar] [CrossRef] [PubMed]
- FDA. Approves Pembrolizumab for Adults and Children with TMB-H Solid Tumors FDA. Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-pembrolizumab-adults-and-children-tmb-h-solid-tumors (accessed on 4 October 2021).
- McGrail, D.J.; Pilié, P.G.; Rashid, N.U.; Voorwerk, L.; Slagter, M.; Kok, M.; Jonasch, E.; Khasraw, M.; Heimberger, A.B.; Lim, B.; et al. High Tumor Mutation Burden Fails to Predict Immune Checkpoint Blockade Response across All Cancer Types. Ann. Oncol. 2021, 32, 661–672. [Google Scholar] [CrossRef] [PubMed]



 ; HNM ; UM
; HNM ; UM  ; AM/MM
; AM/MM  ). (B). Progression-free survival (PFS) of CNA low (red line) and high (blue line) in the total metastatic melanoma cohort. Kaplan–Meier survival curves with a log-rank test were used for the analysis. ns, not significant.
; HNM ; UM ; AM/MM ). (B). Progression-free survival (PFS) of CNA low (red line) and high (blue line) in the total metastatic melanoma cohort. Kaplan–Meier survival curves with a log-rank test were used for the analysis. ns, not significant.
). (B). Progression-free survival (PFS) of CNA low (red line) and high (blue line) in the total metastatic melanoma cohort. Kaplan–Meier survival curves with a log-rank test were used for the analysis. ns, not significant.
; HNM ; UM ; AM/MM ). (B). Progression-free survival (PFS) of CNA low (red line) and high (blue line) in the total metastatic melanoma cohort. Kaplan–Meier survival curves with a log-rank test were used for the analysis. ns, not significant.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CD8 (n = 22) | CD20 (n = 22) | DDR Mutation (n = 23) | ||||||||
| Neg/Low | High | p-Value | Neg/Low | High | p-Value | Neg | Pos | p-Value | ||
| (n = 14) | (n = 8) | (n = 14) | (n = 8) | (n = 7) | (n = 16) | |||||
| Age | <62 | 5 | 5 | 0.221 | 4 | 6 | 0.048 | 6 | 4 | 0.012 |
| ≥62 | 9 | 3 | 10 | 2 | 1 | 12 | ||||
| Melanoma subtype | CM | 7 | 3 | 0.917 | 7 | 3 | 0.720 | 2 | 8 | 0.171 |
| HNM | 4 | 3 | 5 | 2 | 4 | 3 | ||||
| UM | 2 | 1 | 1 | 2 | 0 | 4 | ||||
| AM/MM | 1 | 1 | 1 | 1 | 1 | 1 | ||||
| Chemotherapy | Yes | 2 | 4 | 0.096 | 3 | 3 | 0.369 | 1 | 5 | 0.382 |
| No | 12 | 4 | 11 | 5 | 6 | 11 | ||||
| Immunotherapy | 1 ICI | 7 | 4 | 0.670 | 7 | 4 | 0.670 | 5 | 7 | 0.222 |
| 2+ ICI | 7 | 4 | 7 | 4 | 2 | 9 | ||||
| CD20 | High | 3 | 5 | 0.072 | 3 | 5 | 0.510 | |||
| Neg/Low | 11 | 3 | 4 | 10 | ||||||
| DDR mutation | Positive | 9 | 6 | 0.490 | ||||||
| Negative | 5 | 2 | ||||||||
| CNA count | High | 5 | 5 | 0.221 | 5 | 5 | 0.221 | 3 | 8 | 0.556 |
| Low | 9 | 3 | 9 | 3 | 4 | 8 | ||||
| PFS | Univariate Analysis | OS | Univariate Analysis | |||||
| Median PFS, Months (Range) | HR (95% CI) | p-Value | Median OS, Months (Range) | HR (95% CI) | p-Value | |||
| 3.35 (0.36–39.65) | 27.72 (1.80–177.74) | |||||||
| Categories (n = 23) | ||||||||
| Age | <62 | 10 | 3.23 (0.36–16.65) | Ref | 44.13 (5.12–100.66) | Ref | ||
| ≥62 | 13 | 3.35 (0.45–39.65) | 0.74 (0.30–1.78) | 0.502 | 27.36 (1.80–177.74) | 1.27 (0.415–3.92) | 0.670 | |
| Melanoma Subtype | CM | 10 | 3.54 (0.36–19.45) | Ref | 51.51 (1.8–100.67) | Ref | ||
| HNM | 7 | 2.92 (1.51–7.46) | 1.38 (0.48–3.98) | 0.548 | 27.73 (5.12–177.74) | 1.66 (0.36–7.66) | 0.513 | |
| UM | 4 | 3.01 (1.54–39.65) | 0.82 (0.22–3.07) | 0.777 | 19.52 (10.74–50.13) | 4.86 (1.12–21.05) | 0.034 | |
| AM/MM | 2 | 5.05 (2.72–7.39) | 1.27 (0.27–6.01) | 0.756 | 20.90 (14.06–27.72) | 5.23 (0.86–31.73) | 0.072 | |
| Chemo-Therapy | Yes | 6 | 4.40 (2.92–7.39) | Ref | 38.04 (23.52–100.66) | Ref | ||
| No | 17 | 2.79 (0.36–39.65) | 1.00 (0.37–2.69) | 0.997 | 27.30 (1.80–177.74) | 0.69 (1.87–2.55) | 0.582 | |
| Immuno-Therapy | 1 ICI | 12 | 2.85 (0.36–39.65) | Ref | 25.74 (1.80–80.91) | Ref | ||
| 2+ ICI | 11 | 3.48 (2.72–19.44) | 0.99 (0.41–2.35) | 0.984 | 35.58 (14.06–177.74) | 0.36 (0.11–1.20) | 0.098 | |
| DDR Mutation | Neg | 16 | 2.75 (0.36–3.54) | Ref | 40.50 (5.12–177.74) | Ref | ||
| Pos | 7 | 4.40 (0.45–39.65) | 0.28 (0.10–0.81) | 0.019 | 27.54 (1.80–100.66) | 0.98 (0.29–3.25) | 0.984 | |
| CNA Count | Low | 12 | 2.92 (1.51–3.54) | Ref | 31.65 (1.80–177.74) | Ref | ||
| High | 11 | 5.25 (1.54–19.4) | 0.39 (0.14–1.08) | 0.070 | 23.75 (5.12–100.66) | 1.24 (0.417–3.74) | 0.690 | |
| Categories (n = 22) | ||||||||
| CD8 Expression | Neg/Low | 14 | 2.78 (0.36–7.45) | Ref | 27.72 (1.81–177.74) | Ref | ||
| High | 8 | 6.93 (2.75–19.44) | 0.32 (0.11–0.94) | 0.039 | 34.11 (5.12–53.61) | 0.83 (0.24–2.81) | 0.773 | |
| CD20 Expression | Neg/Low | 14 | 3.41 (0.45–19.44) | Ref | 27.54 (1.81–177.74) | Ref | ||
| High | 8 | 3.07 (0.36–16.65) | 1.03 (0.41–2.57) | 0.935 | 32.01 (10.74–80.91) | 0.91 (0.27–3.07) | 0.888 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andrieu, C.; McNamee, N.; Larkin, A.-M.; Maguire, A.; Menon, R.; Mueller-Eisert, J.; Horgan, N.; Kennedy, S.; Gullo, G.; Crown, J.; et al. Clinical Impact of Immune Checkpoint Inhibitor (ICI) Response, DNA Damage Repair (DDR) Gene Mutations and Immune-Cell Infiltration in Metastatic Melanoma Subtypes. Med. Sci. 2022, 10, 26. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10020026
Andrieu C, McNamee N, Larkin A-M, Maguire A, Menon R, Mueller-Eisert J, Horgan N, Kennedy S, Gullo G, Crown J, et al. Clinical Impact of Immune Checkpoint Inhibitor (ICI) Response, DNA Damage Repair (DDR) Gene Mutations and Immune-Cell Infiltration in Metastatic Melanoma Subtypes. Medical Sciences. 2022; 10(2):26. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10020026
Chicago/Turabian StyleAndrieu, Charlotte, Niamh McNamee, Anne-Marie Larkin, Alanna Maguire, Roopika Menon, Judith Mueller-Eisert, Noel Horgan, Susan Kennedy, Giuseppe Gullo, John Crown, and et al. 2022. "Clinical Impact of Immune Checkpoint Inhibitor (ICI) Response, DNA Damage Repair (DDR) Gene Mutations and Immune-Cell Infiltration in Metastatic Melanoma Subtypes" Medical Sciences 10, no. 2: 26. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci10020026