Artificial Neural Network as a Tool to Predict Facial Nerve Palsy in Parotid Gland Surgery for Benign Tumors

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Prognostic Parameters
2.2. Surgical Technique
2.3. Statistical Analysis
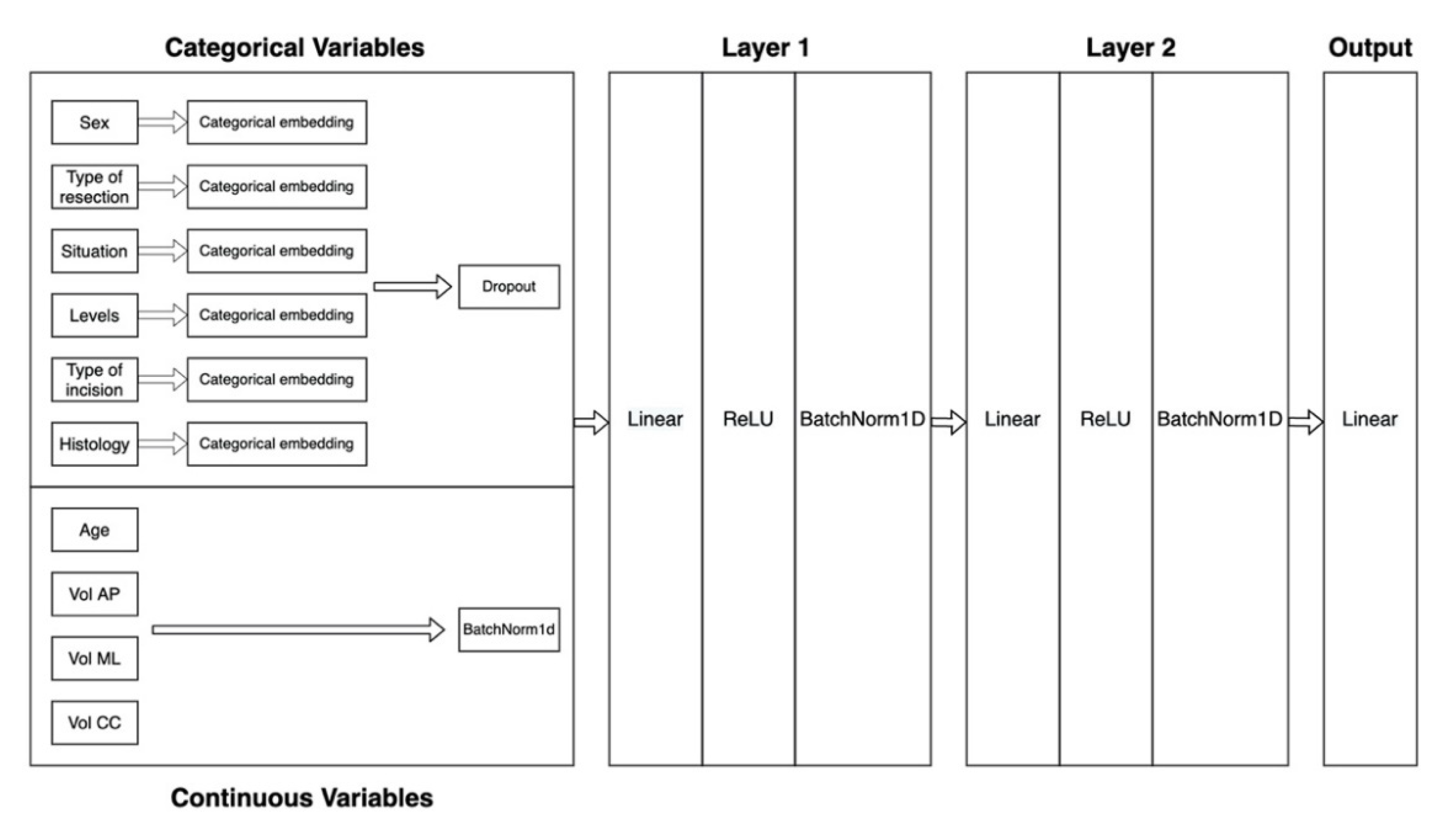
2.4. Model Training
2.5. Validation
3. Results
3.1. Demographic Data
3.2. Artificial Neural Network Vs Multivariate Logistic Regression Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Guntinas-Lichius, O.; Gabriel, B.; Klussmann, P.J. Risk of facial palsy and severe Frey’s syndrome after conservative parotidectomy for benign disease: Analysis of 610 operations. Acta Otolaryngol. 2006, 126, 1104–1109. [Google Scholar] [CrossRef] [PubMed]
- Guntinas-Lichius, O.; Klussmann, J.P.; Wittekindt, C.; Stennert, E. Parotidectomy for benign parotid disease at a university teaching hospital: Outcome of 963 operations. Laryngoscope 2006, 116, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Moeller, K.; Esser, D.; Boeger, D.; Buentzel, J.; Hoffmann, K.; Jecker, P. Parotidectomy and submandibulectomy for benign diseases in Thuringia, Germany: A population-based study on epidemiology and outcome. Eur. Arch. Otorhinolaryngol. 2013, 270, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Grosheva, M.; Klussmann, J.P.; Grimminger, C.; Wittekindt, C.; Beutner, D.; Pantel, M.; Volk, G.F.; Guntinas-Lichius, O. Electromyographic facial nerve monitoring during parotidectomy for benign lesions does not improve the outcome of postoperative facial nerve function: A prospective two-center trial. Laryngoscope 2009, 119, 2299–2305. [Google Scholar] [CrossRef]
- Nitzan, D.; Kronenberg, J.; Horowitz, Z.; Wolf, M.; Bedrin, L.; Chaushu, G.; Talmi, Y.P. Quality of life following parotidectomy for malignant and benign disease. Plast. Reconstr. Surg. 2004, 114, 1060–1067. [Google Scholar] [CrossRef]
- Ryzenman, J.M.; Pensak, M.L.; Tew, J.M., Jr. Facial paralysis and surgical rehabilitation: A quality of life analysis in a cohort of 1,595 patients after acoustic neuroma surgery. Otol. Neurotol. 2005, 26, 516–521. [Google Scholar] [CrossRef] [Green Version]
- Bur, A.M.; Shew, M.; New, J. Artificial intelligence for the otolaryngologist: A state of the art review. Otolaryngol. Head Neck Surg. 2019, 160, 603–611. [Google Scholar] [CrossRef]
- Chen, Y.P. A model to predict 3-month mortality risk of acute-on-chronic hepatitis B liver failure using artificial neural network. J. Viral. Hepat. 2013, 20, 248–255. [Google Scholar]
- Biglarian, A.; Hajizadeh, E.; Kazemnejad, A.; Zayeri, F. Determining of prognostic factors in gastric cancer patients using artificial neural networks. Asian Pac. J. Cancer Prev. 2010, 11, 533–536. [Google Scholar]
- Biglarian, A.; Hajizadeh, E.; Kazemnejad, A.; Zali, M. Application of artificial neural network in predicting the survival rate of gastric cancer patients. Iran. J. Public Health 2011, 40, 80–86. [Google Scholar]
- Amiri, Z.; Mohammad, K.; Mahmoudi, M.; Zeraati, H.; Fotouhi, A. Assessment of gastric cancer survival: Using an artificial hierarchical neural network. Pak. J. Biol. Sci. 2008, 11, 1076–1084. [Google Scholar] [PubMed] [Green Version]
- Faradmal, J.; Soltanian, A.R.; Roshanaei, G.; Khodabakhshi, R.; Kasabian, A. Comparison of the performance of log-logistic regression and artificial neural networks for predicting breast cancer relapse. Asian Pac. J. Cancer Prev. 2014, 15, 5883–5888. [Google Scholar] [CrossRef] [PubMed]
- Abouzari, M.; Goshtasbi, K.; Sarna, B.; Khosravi, P.; Reutershan, T.; Mostaghni, N.; Lin, H.W.; Djalilian, H.R. Prediction of vestibular schwannoma recurrence using artificial neural network. Laryngoscope Investig. Otolaryngol. 2020, 5, 278–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alabi, R.O.; Elmusrati, M.; Sawazaki-Calone, I.; Kowalski, L.P.; Haglund, C.; Coletta, R.D.; Mäkitie, A.A.; Salo, T.; Leivo, I.; Almangush, A. Machine learning application for prediction of locoregional recurrences in early oral tongue cancer: A Web-based prognostic tool. Virchows Arch. 2019, 475, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Quer, M.; Guntinas-Lichius, O.; Marchal, F.; Vander Poorten, V.; Chevalier, D.; León, X.; Eisele, D.; Dulguerov, P. Classification of parotidectomies: A proposal of the European Salivary Gland Society. Eur. Arch. Otorhinolaryngol. 2016, 273, 3307–3312. [Google Scholar] [CrossRef] [PubMed]
- Quer, M.; Vander Poorten, V.; Takes, R.P.; Silver, C.E.; Boedeker, C.C.; de Bree, R.; Rinaldo, A.; Sanabria, A.; Shaha, A.R.; Pujol, A.; et al. Surgical options in benign parotid tumors: A proposal for classification. Eur. Arch. Otorhinolaryngol. 2017, 274, 3825–3836. [Google Scholar] [CrossRef] [PubMed]
- Witt, R.L. Facial nerve monitoring in parotid surgery: The standard of care? Otolaryngol. Head Neck Surg. 1998, 119, 468–470. [Google Scholar] [CrossRef]
- Dulguerov, P.; Marchal, F.; Lehmann, W. Postparotidectomy facial nerve paralysis: Possible etiologic factors and results with routine facial nerve monitoring. Laryngoscope 1999, 109, 754–762. [Google Scholar] [CrossRef]
- Mehle, M.E.; Kraus, D.H.; Wood, B.G.; Benninger, M.S.; Eliachar, I.; Levine, H.L.; Tucker, H.M.; Lavertu, P. Facial nerve morbidity following parotid surgery for benign disease: The Cleveland Clinic Foundation experience. Laryngoscope 1993, 103, 386–388. [Google Scholar] [CrossRef]
- Bron, L.P.; O’Brien, C.J. Facial nerve function after parotidectomy. Arch Otolaryngol Head Neck Surg. 1997, 123, 1091–1096. [Google Scholar] [CrossRef]
- Mra, Z.; Komisar, A.; Blaugrund, S.M. Functional facial nerve weakness after surgery for benign parotid tumors: A multivariate statistical analysis. Head Neck 1993, 15, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Ward, C.M. Injury of the facial nerve during surgery of the parotid gland. Br. J. Surg. 1975, 62, 401–403. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Gao, Z.; Jiang, H.; Yang, H.; Lv, W.; Wang, Z.; Niu, Y.; Feng, G. Predictors of facial palsy after surgery for benign parotid disease: Multivariate analysis of 626 operations. Head Neck 2009, 31, 1588–1592. [Google Scholar] [CrossRef]
- Ikoma, R.; Ishitoya, J.; Sakuma, Y.; Hirama, M.; Shiono, O.; Komatsu, M.; Shiono, O.; Komatsu, M.; Oridate, N. Temporary facial nerve dysfunction after parotidectomy correlates with tumor location. Auris Nasus Larynx. 2014, 41, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Domenick, N.A.; Johnson, J.T. Parotid tumor size predicts proximity to the facial nerve. Laryngoscope 2011, 121, 2366–2370. [Google Scholar] [CrossRef] [PubMed]
- Grosheva, M.; Pick, C.; Granitzka, T.; Sommer, B.; Wittekindt, C.; Klussmann, J.P.; Guntinas-Lichius, O.; Beutner, D. Impact of extent of parotidectomy on early and long-term complications: A prospective multicenter cohort trial. Head Neck 2019, 41, 1943–1951. [Google Scholar] [PubMed]
- Jin, H.; Kim, B.Y.; Kim, H.; Lee, E.; Park, W.; Choi, S.; Chung, M.K.; Son, Y.I.; Baek, C.H.; Jeong, H.S. Incidence of postoperative facial weakness in parotid tumor surgery: A tumor subsite analysis of 794 parotidectomies. BMC Surg. 2019, 19, 199. [Google Scholar]
- Ripley, B.D. Pattern Recognition and Neural Networks; Cambridge University Press: Cambridge, UK, 1996. [Google Scholar]
- Schroeder, L.D.; Sjoquist, D.L.; Stephan, P.E. Understanding Regression Analysis; Sage: Beveley Hills, CA, USA, 1986. [Google Scholar]
- Morse, J.C.; Shilts, M.H.; Ely, K.A.; Li, P.; Sheng, Q.; Huang, L.C.; Wannemuehler, T.J.; Chowdhury, N.I.; Chandra, R.K.; Das, S.R.; et al. Patterns of olfactory dysfunction in chronic rhinosinusitis identified by hierarchial cluster analysis and machine learning algorithms. Int. Forum Allergy Rhinol. 2019, 9, 255–264. [Google Scholar] [CrossRef]
- Bur, A.M.; Holcomb, A.; Goodwin, S.; Woodroof, J.; Karadaghy, O.; Shnayder, Y.; Kakarala, K.; Brant, J.; Shew, M. Machine learning to predict occult nodal metastasis in early oral squamous cell carcinoma. Oral Oncol. 2019, 92, 20–25. [Google Scholar]
- Schmueli, G. To explain or to predict? Stat. Sci. 2010, 25, 289–310. [Google Scholar]
- Bzdok, D.; Altman, N.; Krzywinski, M. Statistics versus machine learning. Nat. Methods 2018, 15, 233–234. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | N | % |
|---|---|---|
| Sex | ||
| Male | 192 | 55.7 |
| Female | 153 | 44.3 |
| Mean Age | 58 ± 13.9 years (min: 18/max: 87) | |
| Size | ||
| <3 cm | 216 | 62.6 |
| >3 cm | 129 | 37.4 |
| Maximum length per plane | ||
| - Anterior to posterior | 2.45 ± 1.15 cc (min: 0.9/max: 6.5) | |
| - Medial to lateral | 2.17 ± 1.07 cc (min: 0.7/max: 6) | |
| - Cephalic to caudal | 2.22 ± 0.99 cc (min: 0.76/max: 6.8) | |
| Type of resection | ||
| I | 141 | 40.9 |
| II | 48 | 13.9 |
| III | 99 | 28.7 |
| IV | 57 | 16.5 |
| Anatomic situation in the gland | ||
| Parotid tail | 162 | 47 |
| Mid lobe | 45 | 13 |
| Superior lobe | 21 | 6.1 |
| Deep lobe | 24 | 7 |
| Superior and middle lobe | 15 | 4.3 |
| Inferior and middle lobe | 54 | 15.7 |
| All superficial | 24 | 6.9 |
| Levels | ||
| I | 6 | 1.7 |
| II | 159 | 46.1 |
| I and II | 120 | 34.8 |
| I to III | 45 | 13 |
| I to IV | 9 | 2.6 |
| III and IV | 6 | 1.7 |
| Histology | ||
| Pleomorphic adenoma | 153 | 44.3 |
| Warthin tumor | 132 | 38.3 |
| Oncocytoma | 15 | 4.3 |
| First branch branchial cyst | 15 | 4.3 |
| Basal cell adenoma | 9 | 2.6 |
| Oncocytic papillary cystadenoma | 9 | 2.6 |
| Microcystic adenoma | 6 | 1.8 |
| Chondroma | 3 | 0.9 |
| Transient facial palsy | ||
| Yes | 84 | 24.3 |
| No | 261 | 75.7 |
| Definitive facial palsy (branch) | ||
| Yes | 12 | 3.47 |
| No | 333 | 96.53 |
| Facial nerve lesion by branch | ||
| MMB | 48 | 13.8 |
| BB | 6 | 1.8 |
| ZB | 9 | 2.6 |
| OB | 9 | 2.6 |
| FB | 9 | 2.6 |
| All branches | 15 | 4.3 |
| Model | Sensitivity (%)—95% CI | Specificity (%)—95% CI | Positive Predictive Value (%)—95% CI | Negative Predictive Value (%)—95% CI | Accuracy (%)—95% CI | ROC–AUC | 95% CI—for the ROC–AUC |
|---|---|---|---|---|---|---|---|
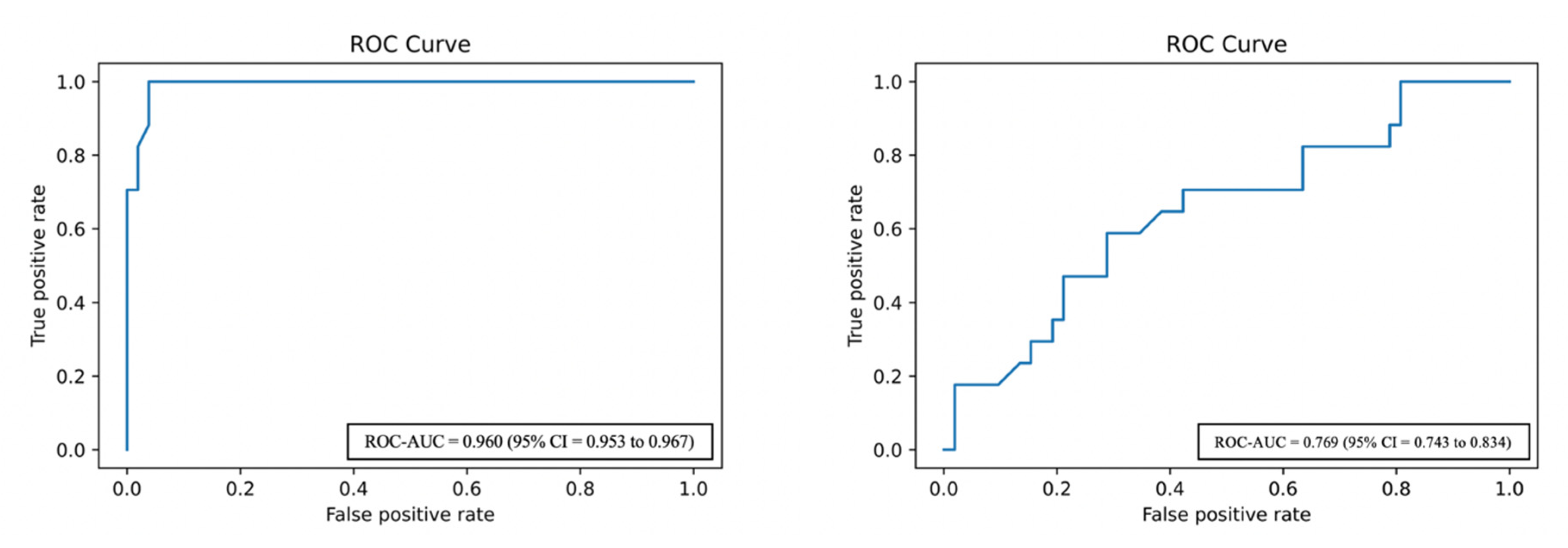
| ANN | 86.53 (79.41 to 91.47) | 95.67 (85.30 to 99.14) | 87.28 (83.16 to 92.23) | 95.68 (86.13 to 98.19) | 93.42 (88.34 to 96.19) | 0.960 | 0.953 to 0.967 |
| MLR | 46.23 (41.11 to 51.18) | 92.59 (86.33 to 94.87) | 66.94 (61.27 to 69.17) | 83.37 (78.47 to 87.29) | 80.42 (76.16 to 83.11) | 0.769 | 0.743 to 0.834 |
| LMR | ANN | ||||
|---|---|---|---|---|---|
| Variable | p | OR | 95% Confidence Interval | Variable | Importance |
| Sex | 0.004 | 0.409 | 0.221 to 0.755 | Situation | 0.227389 |
| TOR | 0.006 | 0.600 | 0.418 to 0.861 | Vol CC | 0.096018 |
| Vol > 3 cm | 0.517 | 1.423 | 0.490 to 4.134 | Histology | 0.030937 |
| Situation | 0.004 | 0.809 | 0.701 to 0.933 | Vol AP | 0.029990 |
| Levels | 0.156 | 0.829 | 0.640 to 1.074 | Age | 0.018491 |
| TOI | 0.788 | 1.096 | 0.562 to 2.136 | TOI | 0.017908 |
| Histology | 0.753 | 0.982 | 0.880 to 1.097 | Levels | 0.013154 |
| Age | 0.017 | 1.027 | 1.005 to 1.050 | Vol < 3 cm | 0.000694 |
| Vol AP | 0.434 | 0.803 | 0.464 to 1.391 | TOR | −0.000495 |
| Vol ML | 0.075 | 1.624 | 0.953 to 2.769 | Vol > 3 cm | −0.001494 |
| Vol CC | 0.953 | 1.013 | 0.662 to 1.550 | Vol ML | −0.001810 |
| Sex | −0.022819 | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiesa-Estomba, C.M.; Sistiaga-Suarez, J.A.; González-García, J.Á.; Larruscain, E.; Cammaroto, G.; Mayo-Yánez, M.; Lechien, J.R.; Calvo-Henríquez, C.; Altuna, X.; Medela, A. Artificial Neural Network as a Tool to Predict Facial Nerve Palsy in Parotid Gland Surgery for Benign Tumors. Med. Sci. 2020, 8, 42. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci8040042
Chiesa-Estomba CM, Sistiaga-Suarez JA, González-García JÁ, Larruscain E, Cammaroto G, Mayo-Yánez M, Lechien JR, Calvo-Henríquez C, Altuna X, Medela A. Artificial Neural Network as a Tool to Predict Facial Nerve Palsy in Parotid Gland Surgery for Benign Tumors. Medical Sciences. 2020; 8(4):42. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci8040042
Chicago/Turabian StyleChiesa-Estomba, Carlos M, Jon A Sistiaga-Suarez, José Ángel González-García, Ekhiñe Larruscain, Giovanni Cammaroto, Miguel Mayo-Yánez, Jerome R Lechien, Christian Calvo-Henríquez, Xabier Altuna, and Alfonso Medela. 2020. "Artificial Neural Network as a Tool to Predict Facial Nerve Palsy in Parotid Gland Surgery for Benign Tumors" Medical Sciences 8, no. 4: 42. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci8040042