
Gastric Mixed Neuroendocrine Non-Neuroendocrine Neoplasms: A Western Center Case Series


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analysis
3. Results
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Choi, N.Y.; Kim, B.S.; Oh, S.T.; Yook, J.H.; Kim, B.S. Comparative Outcomes in Patients With Small- and Large-Cell Neuroendocrine Carcinoma (NEC) and Mixed Neuroendocrine-Non-Neuroendocrine Neoplasm (MiNEN) of the Stomach. Am. Surg. 2021, 87, 631–637. [Google Scholar] [CrossRef]
- Sun, L.; Zhang, J.; Wang, C.; Zhao, S.; Shao, B.; Guo, Y.; Liu, Y.; Sun, Y. Chromosomal and molecular pathway alterations in the neuroendocrine carcinoma and adenocarcinoma components of gastric mixed neuroendocrine–nonneuroendocrine neoplasm. Mod. Pathol. 2020, 33, 2602–2613. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.; Nam, S.K.; Kwak, Y.; Kim, G.; Kim, K.K.; Lee, B.C.; Ahn, S.H.; Park, D.J.; Kim, H.H.; Park, K.U.; et al. Comprehensive genetic features of gastric mixed adenoneuroendocrine carcinomas and pure neuroendocrine carcinomas. J. Pathol. 2021, 253, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.P.; Zhao, Y.J.; He, Q.L.; Hao, H.K.; Tian, Y.T.; Zou, B.B.; Jiang, L.X.; Lin, W.; Zhou, Y.B.; Li, Z.; et al. Adjuvant chemotherapy for patients with gastric neuroendocrine carcinomas or mixed adenoneuroendocrine carcinomas. Br. J. Surg. 2020, 107, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Zhao, Y.J.; Zhou, Y.; He, Q.; Tian, Y.; Hao, H.; Qiu, X.; Jiang, L.; Zhao, G.; Huang, C.M. Modified staging system for gastric neuroendocrine carcinoma based on American Joint Committee on Cancer and European Neuroendocrine Tumor Society systems. Br. J. Surg. 2020, 107, 248–257. [Google Scholar] [CrossRef] [PubMed]
- van der Veen, A.; Seesing, M.F.J.; Wijnhoven, B.P.L.; de Steur, W.O.; van Berge Henegouwen, M.I.; Rosman, C.; van Sandick, J.W.; Mook, S.; Haj Mohammad, N.; Ruurda, J.P.; et al. Management of resectable esophageal and gastric (mixed adeno)neuroendocrine carcinoma: A nationwide cohort study. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2018, 44, 1955–1962. [Google Scholar] [CrossRef]
- Kwok, C.M. Mixed Adenoneuroendocrine Carcinoma of the Stomach. Case Rep. Gastroenterol. 2015, 9, 241–245. [Google Scholar] [CrossRef]
- Ma, F.; Wang, B.; Xue, L.; Kang, W.; Li, Y.; Li, W.; Liu, H.; Ma, S.; Tian, Y. Neoadjuvant chemotherapy improves the survival of patients with neuroendocrine carcinoma mixed adenoneuroendocrine carcinoma of the stomach. J. Cancer Res. Clin. Oncol. 2020, 146, 2135–2142. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.W.; Lu, J.; Wang, J.B.; Lin, J.X.; Chen, Q.Y.; Cao, L.L.; Lin, M.; Tu, R.H.; Huang, Z.N.; Lin, J.L.; et al. Prognostic factors for survival after curative resection of gastric mixed adenoneuroendocrine carcinoma: A series of 80 patients. BMC Cancer 2018, 18, 1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosman, T.F.; Carneiro, F.; Hruban, R.H.; Theise, N.D. WHO Classification of Tumours of the Digestive System, 4th ed.; International Agency for Research on cancer (IARC); IARC Press: Lyon, Frace, 2010. [Google Scholar]
- Szor, D.J.; Roncon Dias, A.; Pereira, M.A.; Ramos, M.F.K.P.; Zilberstein, B.; Cecconello, I.; Ribeiro, U. Neutrophil-lymphocyte ratio is associated with prognosis in patients who underwent potentially curative resection for gastric cancer. J. Surg. Oncol. 2018, 117, 851–857. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Doyle, D.J.; Garmon, E.H. American Society of Anesthesiologists Classification (ASA Class). In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2017. [Google Scholar]
- Ajani, J.A.; In, H.; Sano, T.; Gaspar, L.E.; Erasmus, J.J.; Tang, L.H.; Washington, M.K.; Gerdes, H. American Joint Committee on Cancer (AJCC), Cancer Staging Manual, 8th ed.; Springer: Berlin/Heidelberg, Germany, 2017; Volume 17, pp. 203–220. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer: Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2017, 20, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barchi, L.C.; Ramos, M.F.K.P.; Dias, A.R.; Andreollo, N.A.; Weston, A.C.; Lourenço, L.G.; Malheiros, C.A.; Kassab, P.; Zilberstein, B.; Ferraz, Á.A.B.; et al. II Brazilian Consensus on Gastric Cancer By The Brazilian Gastric Cancer Association; ABCD Arquivos Brasileiros de Cirurgia Digestiva: São Paulo, Brazil, 2020; Volume 33, p. e1514. [Google Scholar] [CrossRef]
- Zheng, H.; Zhao, Y.; He, Q.; Hao, H.; Tian, Y.; Zou, B.; Jiang, L.; Qiu, X.; Zhou, Y.; Li, Z.; et al. Multi-institutional development and validation of a nomogram to predict recurrence after curative resection of gastric neuroendocrine/mixed adenoneuroendocrine carcinoma. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2021, 24, 503–514. [Google Scholar] [CrossRef]
- Khan, M.S.; Pritchard, D.M. Neuroendocrine tumours: What gastroenterologists need to know. Frontline Gastroenterol. 2020. [Google Scholar] [CrossRef]
- Scardoni, M.; Vittoria, E.; Volante, M.; Rusev, B.; Bersani, S.; Mafficini, A.; Gottardi, M.; Giandomenico, V.; Malleo, G.; Butturini, G.; et al. Mixed adenoneuroendocrine carcinomas of the gastrointestinal tract: Targeted next-generation sequencing suggests a monoclonal origin of the two components. Neuroendocrinology 2014, 100, 310–316. [Google Scholar] [CrossRef]
- Lin, Z.; Chen, J.; Guo, Y. Efficacy of XELOX adjuvant chemotherapy for gastric mixed adenoneuroendocrine carcinoma: A case report. Medicine 2019, 98, e16000. [Google Scholar] [CrossRef]
- Dias, A.R.; Azevedo, B.C.; Alban, L.B.V.; Yagi, O.K.; Ramos, M.; Jacob, C.E.; Barchi, L.C.; Cecconello, I.; Ribeiro, U.; Zilberstein, B., Jr. Gastric Neuroendocrine Tumor: Review and Update. Arq. Bras. De Cir. Dig. Braz. Arch. Dig. Surg. 2017, 30, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Granata, V.; Fusco, R.; Setola, S.V.; Castelguidone, E.L.D.; Camera, L.; Tafuto, S.; Avallone, A.; Belli, A.; Incollingo, P.; Palaia, R.; et al. The multidisciplinary team for gastroenteropancreatic neuroendocrine tumours: The radiologist’s challenge. Radiol. Oncol. 2019, 53, 373–387. [Google Scholar] [CrossRef] [Green Version]
- Sanli, Y.; Garg, I.; Kandathil, A.; Kendi, T.; Zanetti, M.J.B.; Kuyumcu, S.; Subramaniam, R.M. Neuroendocrine Tumor Diagnosis and Management: (68)Ga-DOTATATE PET/CT. Am. J. Roentgenol. 2018, 211, 267–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.M.; Chiu, N.C.; Li, A.F.; Liu, C.A.; Chou, Y.H.; Chiou, Y.Y. Unusual gastric tumors and tumor-like lesions: Radiological with pathological correlation and literature review. World J. Gastroenterol. 2017, 23, 2493–2504. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.S.; Tsai, C.L.; Chu, Y.Y.; Chen, K.C.; Lin, J.C.; Chen, B.C.; Sun, W.C.; Yen, H.H.; Chen, C.Y.; Wu, I.C.; et al. Clinical features and outcomes of gastric neuroendocrine tumors after endoscopic diagnosis and treatment: A Digestive Endoscopy Society of Tawian (DEST). Medicine 2018, 97, e12101. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, C.R.; Metz, D.C. Gastric Neuroendocrine Tumors (Carcinoids). Curr. Gastroenterol. Rep. 2019, 21, 13. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.J.; Fu, X.L.; Liu, W.; Zheng, L.Y.; Zhang, J.F.; Huo, Y.M.; Li, J.; Hua, R.; Liu, Q.; Sun, Y.W. Clinicopathological, treatment, and prognosis study of 43 gastric neuroendocrine carcinomas. World J. Gastroenterol. 2017, 23, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Pham, Q.D.; Mori, I.; Osamura, R.Y. A Case Report: Gastric Mixed Neuroendocrine-Nonneuroendocrine Neoplasm with Aggressive Neuroendocrine Component. Case Rep. Pathol. 2017, 2017, 9871687. [Google Scholar] [CrossRef]
- Ramos, M.; Pereira, M.A.; Yagi, O.K.; Dias, A.R.; Charruf, A.Z.; Oliveira, R.J.; Zaidan, E.P.; Zilberstein, B.; Ribeiro-Junior, U.; Cecconello, I. Surgical treatment of gastric cancer: A 10-year experience in a high-volume university hospital. Clinics 2018, 73 (Suppl. 1), e543s. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Gastric Adenocarcinoma | MiNEN | ||
|---|---|---|---|---|
| n = 597 (%) | n = 5 (%) | p | ||
| Sex | 0.334 | |||
| Female | 247 (41.4) | 1 (20) | ||
| Male | 350 (58.6) | 4 (80) | ||
| Age (years) | 0.589 | |||
| Mean (SD) | 62.8 (12.6) | 65.8 (11.7) | ||
| Body mass index (Kg/m²) | 0.053 | |||
| Mean (SD) | 24.6 (5.0) | 29.6 (7.9) | ||
| Hemoglobin (g/dL) | 0.791 | |||
| Mean (SD) | 12.5 (5.5) | 11.8 (3.5) | ||
| Albumin (g/dL) | 0.573 | |||
| Mean (SD) | 4.0 (1.4) | 4.4 (0.3) | ||
| Neutrophil-lymphocyte ratio (NLR) | 0.778 | |||
| Mean (SD) | 2.74 (2.64) | 3.07 (1.05) | ||
| Charlson–Deyo Comorbidity Index (CCI) | 0.054 | |||
| 0 | 389 (65.2) | 1 (20) | ||
| ≥1 | 208 (34.8) | 4 (80) | ||
| ASA (American Society of Anesthesiologists) | 0.015 | |||
| I/II | 450 (75.4) | 1 (20) | ||
| III/IV | 147 (24.6) | 4 (80) | ||
| Type of Gastrectomy | 0.662 | |||
| Subtotal | 387 (64.8) | 4 (80) | ||
| Total | 210 (35.2) | 1 (20) | ||
| Surgical access | 1.0 | |||
| Open | 491 (82.2) | 4 (80) | ||
| Laparoscopic | 106 (17.8) | 1 (20) | ||
| Lymphadenectomy | 0.204 | |||
| D1 | 101 (16.9) | 2 (40) | ||
| D2 | 496 (83.1) | 3 (60) | ||
| Variables | Gastric Adenocarcinoma | MiNEN | ||
|---|---|---|---|---|
| n = 597 (%) | n = 5 (%) | p | ||
| Tumor size (cm) | 0.879 | |||
| Mean (SD) | 4.7 (3.0) | 4.5 (3.4) | ||
| Lymphatic Invasion | 1.0 | |||
| Absent | 308 (51.6) | 3 (60) | ||
| Present | 289 (48.4) | 2 (40) | ||
| Venous Invasion | 1.0 | |||
| Absent | 402 (67.3) | 3 (60) | ||
| Present | 195 (32.7) | 2 (40) | ||
| Perineural invasion | 0.378 | |||
| Absent | 317 (53.1) | 4 (80) | ||
| Present | 280 (46.9) | 1 (20) | ||
| pT status | 1.0 | |||
| pT1/T2 | 251 (42) | 2 (40) | ||
| pT3/T4 | 346 (58) | 3 (60) | ||
| Number of Lymph node dissected | 0.329 | |||
| Mean (SD) | 40.7 (18.1) | 32.8 (17.7) | ||
| pN status | 1.0 | |||
| pN0 | 262 (43.9) | 2 (40) | ||
| pN+ | 335 (56.1) | 3 (60) | ||
| pTNM | 0.395 | |||
| I/II | 337 (56.4) | 4 (80) | ||
| III/IV | 260 (43.6) | 1 (20) | ||
| Number of Case | |||||
|---|---|---|---|---|---|
| Variables | 1 | 2 | 3 | 4 | 5 |
| Sex | Female | Male | Male | Male | Male |
| Age (years) | 69.6 | 82.7 | 50.8 | 61.1 | 65.0 |
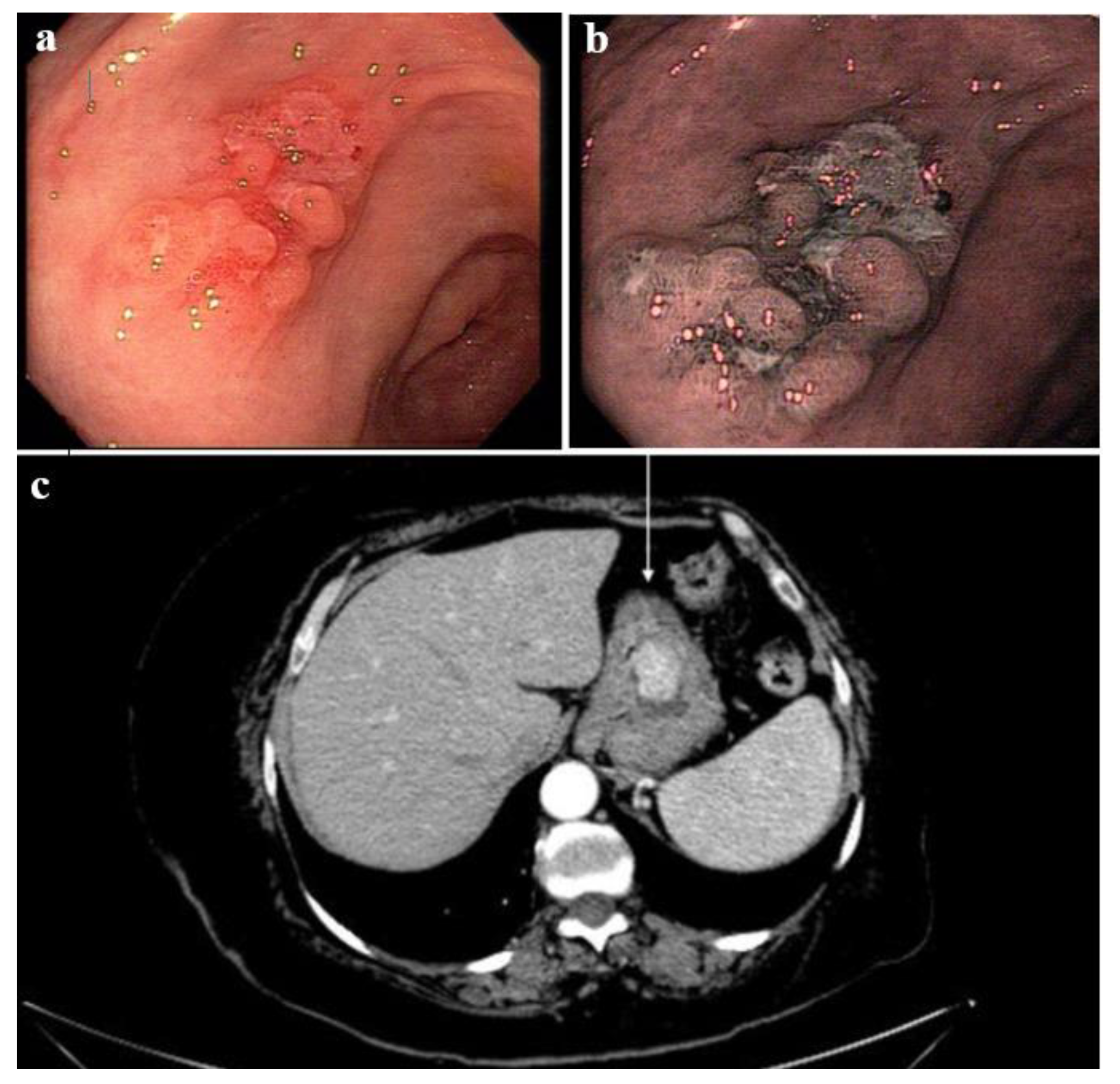
| Tumor Location | middle third | middle third | lower third | middle third | lower third |
| Tumor size (cm) | 3.0 | 1.8 | 3.2 | 10.6 | 4.0 |
| Neuroendocrine vs. Adenocarcinoma (%) | 70% vs. 30% | 70% vs. 30% | 60% vs. 40% | 70% vs. 30% | 70% vs. 30% |
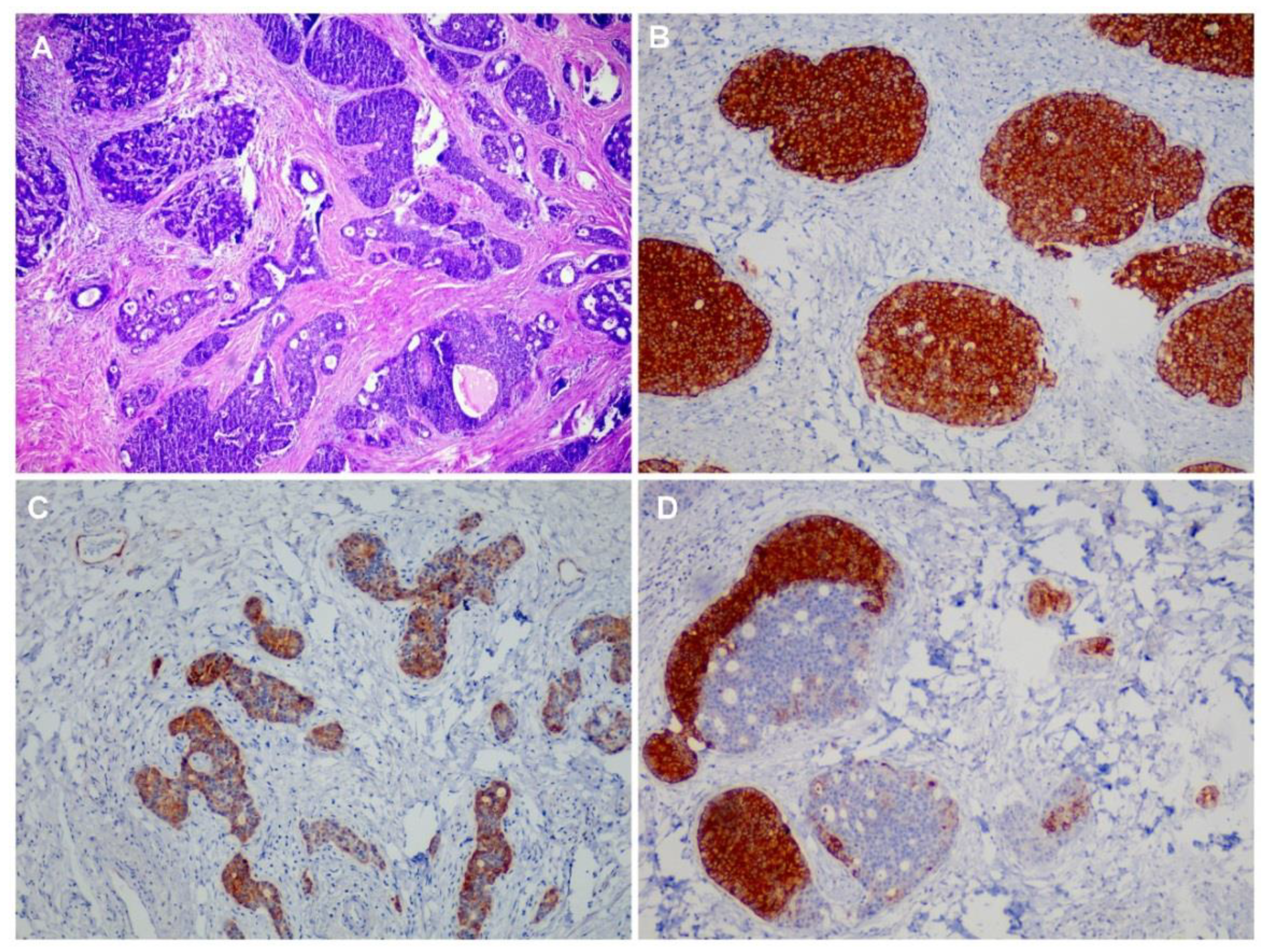
| IHC(+) for Adenocarcinoma component | CK7 | CK7, CK20, and CDX-2 | CK7 and CK20 | AE1/AE3 | AE1/AE3 |
| IHC(+) for Neuroendocrine component | Chromogranin A and Synaptophysin | Chromogranin A, Synaptophysin, and CK35BH11 | Chromogranin A and Synaptophysin | Chromogranin A, Synaptophysin, and CK35BH11 | Chromogranin A and Synaptophysin |
| Mitotic count per 10 HPFs | — | 5 | 1 | — | 20 |
| Ki67 labeling index (%) | 15 | 5 | 80 | 40 | 70 |
| Presence of necrosis | Absent | Absent | Absent | Present | Absent |
| Lymphatic Invasion | Present | Present | Present | Absent | Absent |
| Venous Invasion | Present | Present | Present | Absent | Absent |
| Perineural invasion | Absent | Present | Absent | Present | Absent |
| LN+/LNs total | 0+/46 | 1+/5 | 2+/26 | 2+/40 | 0+/47 |
| pTNM | T4a N0 M0 | T4a N1 M0 | T1b N1 M0 | T3 N1 M0 | T1b N0 M0 |
| Final Stage | IIB | IIIA | IB | IIB | IA |
| DFS (months) | 1.3 | 8.7 | 37.0 | 54.2 | 17.3 |
| OS (months) | 1.3 | 16.7 | 37.0 | 54.2 | 17.3 |
| Patient status | Death | Death | Alive, without disease | Alive, without disease | Alive, without disease |
| Variables | Gastric Adenocarcinoma | MiNEN | ||
|---|---|---|---|---|
| n = 597 (%) | n = 5 (%) | p | ||
| Length of hospital stay (days) | 0.371 | |||
| Mean (SD) | 12.0 (9.4) | 16.3 (14.7) | ||
| Postoperative complication (POC) | 0.022 | |||
| No POC/Minor POC | 515 (86.3) | 2 (40) | ||
| Major POC | 82 (13.7) | 3 (60) | ||
| 30-day mortality | 1.0 | |||
| No | 576 (96.5) | 5 (100) | ||
| Yes | 21 (3.5) | 0 (0) | ||
| 90-day mortality | 0.311 | |||
| No | 555 (93) | 4 (80) | ||
| Yes | 42 (7) | 1 (20) | ||
| Chemotherapy | 0.204 | |||
| No | 288 (48.2) | 4 (80) | ||
| Yes | 309 (51.8) | 1 (20) | ||
| Recurrence | — | |||
| No | 468 (78.4) | 4 (80) | ||
| Yes | 129 (21.6) | 1 (20) | ||
| Death | — | |||
| No | 390 (65.3) | 3 (60) | ||
| Yes | 207 (34.7) | 2 (40) | ||
| Disease-free survival rate | 0.925 * | |||
| DFS (%) | 71.3 | 71.7 | ||
| Overall survival rate | 0.612 * | |||
| OS (%) | 56.7 | 60.0 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos, M.F.K.P.; Pereira, M.A.; Arabi, A.Y.M.; Mazepa, M.M.; Dias, A.R.; Ribeiro, U., Jr.; Zilberstein, B.; Nahas, S.C. Gastric Mixed Neuroendocrine Non-Neuroendocrine Neoplasms: A Western Center Case Series. Med. Sci. 2021, 9, 47. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci9030047
Ramos MFKP, Pereira MA, Arabi AYM, Mazepa MM, Dias AR, Ribeiro U Jr., Zilberstein B, Nahas SC. Gastric Mixed Neuroendocrine Non-Neuroendocrine Neoplasms: A Western Center Case Series. Medical Sciences. 2021; 9(3):47. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci9030047
Chicago/Turabian StyleRamos, Marcus Fernando Kodama Pertille, Marina Alessandra Pereira, Arthur Youssif Mota Arabi, Melissa Mello Mazepa, Andre Roncon Dias, Ulysses Ribeiro, Jr., Bruno Zilberstein, and Sergio Carlos Nahas. 2021. "Gastric Mixed Neuroendocrine Non-Neuroendocrine Neoplasms: A Western Center Case Series" Medical Sciences 9, no. 3: 47. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci9030047