
COVID-19 Community Transmission among Healthcare Workers at a Tertiary Care Cardiac Center

 ,
, 
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Ethical Approval
2.3. Measurements and Definitions
2.4. Home Isolation
2.5. Hospital Admission
2.6. Contact Tracing
2.7. Data Collection
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | coronavirus disease 2019 |
| HCWs | healthcare workers |
| KSA | Kingdom of Saudi Arabia |
| RT-PCR | real-time reverse transcriptase polymerase chain reaction |
References
- Ahmad, T.; Haroon, B.M.; Hui, J. Coronavirus disease 2019 (COVID-19) pandemic and economic impact. Pak. J. Med. Sci. 2020, 36, S73–S78. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 as a Public Health Emergency of International Concern (PHEIC) under the IHR 2020. Available online: https://extranet.who.int/sph/covid-19-public-health-emergency-international-concern-pheic-under-ihr (accessed on 5 January 2021).
- Robert, A.A. COVID-19 in People with Diabetes: Perspectives from Saudi Arabia. Curr. Diabetes Rev. 2020, 16, 1–7. [Google Scholar] [CrossRef]
- Al Dawish, M.A. COVID-19 in People with Diabetes: Epidemiological Perspectives and Public Health Actions in the Middle East and North Africa (MENA) Region. Curr. Diabetes Rev. 2021, 17, 1–6. [Google Scholar] [CrossRef]
- Adalja, A.A.; Toner, E.; Inglesby, T.V. Priorities for the US Health Community Responding to COVID-19. JAMA 2020, 323, 1343. [Google Scholar] [CrossRef] [Green Version]
- Stern, R.H. Locally Informed Simulation to Predict Hospital Capacity Needs During the COVID-19 Pandemic. Ann. Intern. Med. 2020, 173, 679–680. [Google Scholar] [CrossRef]
- Rees, E.M.; Nightingale, E.S.; Jafari, Y.; Waterlow, N.R.; Clifford, S.; Pearson, C.A.B.; CMMID Working Group; Jombart, T.; Procter, S.; Knight, G.M. COVID-19 length of hospital stay: A systematic review and data synthesis. BMC Med. 2020, 18, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Mukherjee, K.; Bhattacharjee, D.; Garai, D.; Chakraborty, R. Status of Health-care Workers in Relation to COVID-19 Infection: A Retrospective Study in a Level 4 COVID Hospital in Eastern India. J. Assoc. Physicians India 2020, 68, 55–57. [Google Scholar] [PubMed]
- Rekatsina, M.; Paladini, A.; Moka, E.; Yeam, C.T.; Urits, I.; Viswanath, O.; Kaye, A.D.; Morgan, J.A.; Varrassi, G. Healthcare at the time of COVID-19: A review of the current situation with emphasis on anesthesia providers. Best Pract. Res. Clin. Anaesthesiol. 2020, 34, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Dilaghi, E.; Prestigiacomo, C.; Alessio, G.; Marcellini, L.; Simmaco, M.; Santino, I.; Orsi, G.B.; Anibaldi, P.; Marcolongo, A.; et al. Prevalence of Sars-Cov-2 Infection in Health Workers (HWs) and Diagnostic Test Performance: The Experience of a Teaching Hospital in Central Italy. Int. J. Environ. Res. Public Health 2020, 17, 4417. [Google Scholar] [CrossRef]
- World Health Organization. Novel Coronavirus–China 2020. Available online: https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed on 5 February 2021).
- COVID-19 Dashboard. Available online: https://covid19.moh.gov.sa/ (accessed on 27 March 2021).
- Black, J.R.M.; Bailey, C.; Przewrocka, J.; Dijkstra, K.K.; Swanton, C. COVID-19: The case for health-care worker screening to prevent hospital transmission. Lancet 2020, 395, 1418–1420. [Google Scholar] [CrossRef]
- Ehrlich, H.; McKenney, M.; Elkbuli, A. Protecting our healthcare workers during the COVID-19 pandemic. Am. J. Emerg. Med. 2020, 38, 1527–1528. [Google Scholar] [CrossRef] [PubMed]
- Driggin, E.; Madhavan, M.V.; Bikdeli, B.; Chuich, T.; Laracy, J.; Biondi-Zoccai, G.; Brown, T.S.; Der-Nigoghossian, C.; Zidar, D.A.; Haythe, J.; et al. Cardiovascular Considerations for Patients, Health Care Workers, and Health Systems During the COVID-19 Pandemic. J. Am. Coll. Cardiol. 2020, 75, 2352–2371. [Google Scholar] [CrossRef]
- Al Hayek, A.A.; Robert, A.A.; Matar, A.B.; Algarni, A.; Alkubedan, H.; Alharbi, T.; Al Amro, A.; Alrashidi, S.A.; Al Dawish, M. Risk factors for hospital admission among COVID-19 patients with diabetes. a study from Saudi Arabia. Saudi Med. J. 2020, 41, 1090–1097. [Google Scholar] [CrossRef] [PubMed]
- Do, D.; Sarker, M.; Chen, S.; Lenjani, A.; Tikka, P.; Bärnighausen, T.; Geldsetzer, P. Healthcare worker attendance during the early stages of the COVID-19 pandemic: A longitudinal analysis of fingerprint-verified data from all public-sector secondary and tertiary care facilities in Bangladesh. J. Glob. Health 2020, 10. [Google Scholar] [CrossRef]
- Caballero, A.; Ceriello, A.; Misra, A.; Aschner, P.; McDonnell, M.; Hassanein, M.; Ji, L.; Mbanya, J.; Fonseca, V. COVID-19 in people living with diabetes: An international consensus. J. Diabetes Complicat. 2020, 34, 107671. [Google Scholar] [CrossRef]
- Alsofayan, Y.M.; Althunayyan, S.M.; Khan, A.A.; Hakawi, A.M.; Assiri, A.M. Clinical characteristics of COVID-19 in Saudi Arabia: A national retrospective study. J. Infect. Public Health 2020, 13, 920–925. [Google Scholar] [CrossRef] [PubMed]
- Abolfotouh, M.A.; Almutairi, A.F.; BaniMustafa, A.A.; Hussein, M.A. Perception and attitude of healthcare workers in Saudi Arabia with regard to Covid-19 pandemic and potential associated predictors. BMC Infect. Dis. 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Barry, M.; AlMohaya, A.; Al Hijji, A.; Akkielah, L.; Al Rajhi, A.; Al Majid, F.; Alsharidi, A.; Al-Shahrani, F.S.; Alotaibi, N.H.; Alanazi, A.; et al. Clinical characteristics and outcome of hospitalized COVID-19 patients in a MERS-CoV endemic area. J. Epidemiol. Glob. Health 2020, 10, 214–221. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Garout, M.A.; Gautret, P. Preparing for emerging respiratory pathogens such as SARS-CoV, MERS-CoV, and SARS-CoV-2. Infez Med. 2020, 28, 64–70. [Google Scholar]
- Barry, M.; Phan, M.V.; Akkielah, L.; Al-Majed, F.; Alhetheel, A.; Somily, A.; Alsubaie, S.S.; McNabb, S.J.; Cotten, M.; Zumla, A.; et al. Nosocomial outbreak of the Middle East Respiratory Syndrome coronavirus: A phylogenetic, epidemiological, clinical and infection control analysis. Travel Med. Infect. Dis. 2020, 37, 101807. [Google Scholar] [CrossRef]
- Baker, J.M.; Nelson, K.N.; Overton, E.; Lopman, B.A.; Lash, T.L.; Photakis, M.; Jacob, J.T.; Roback, J.D.; Fridkin, S.K.; Steinberg, J.P.; et al. Quantification of occupational and community risk factors for SARS-CoV-2 seropositivity among health care workers in a large U.S. health care system. Ann. Intern. Med. 2021, 174, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Al Maskari, Z.; Al Blushi, A.; Khamis, F.; Al Tai, A.; Al Salmi, I.; Al Harthi, H.; Al Saadi, M.; Al Mughairy, A.; Gutierrez, R.; Al Blushi, Z. Characteristics of healthcare workers infected with COVID-19: A cross-sectional observational study. Int. J. Infect. Dis. 2021, 102, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Kim, R.; Nachman, S.; Fernandes, R.; Meyers, K.; Taylor, M.; Leblanc, D.; Singer, A.J. Comparison of COVID-19 infections among healthcare workers and non-healthcare workers. PLoS ONE 2020, 15, e0241956. [Google Scholar] [CrossRef]
- Barry, M.; Althabit, N.; Akkielah, L.; Al Mohaya, A.; Alotaibi, M.; Alhasani, S.; Aldrees, A.; Al Rajhi, A.; Al Hiji, A.; Almajid, F.; et al. Clinical Characteristics and Outcomes of Hospitalized COVID-19 Patients in a MERS-CoV Referral Hospital during the Peak of the Pandemic. Int. J. Infect. Dis. 2021, 106, 43–51. [Google Scholar] [CrossRef]
- Heinzerling, A.; Stuckey, M.; Scheuer, T.; Xu, K.; Perkins, K.; Resseger, H.; Magill, S.; Verani, J.; Jain, S.; Acosta, M.; et al. Transmis-sion of COVID-19 to Health Care Personnel During Exposures to a Hospitalized Patient—Solano County, California, February 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 472–476. [Google Scholar] [CrossRef] [Green Version]
- Kambhampati, A.; O’Halloran, A.; Whitaker, M.; Magill, S.; Chea, N.; Chai, S.J.; Kirley, P.D.; Herlihy, R.K.; Kawasaki, B.; Meek, J.; et al. COVID-19–Associated Hospitalizations Among Health Care Personnel—COVID-NET, 13 States, 1 March–31 May 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1576–1583. [Google Scholar] [CrossRef]
- Al Ateeq, D.A.; Aljhani, S.; Althiyabi, I.; Majzoub, S. Mental health among healthcare providers during coronavirus disease (COVID-19) outbreak in Saudi Arabia. J. Infect. Public Health 2020, 13, 1432–1437. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.M. CTVNews.ca 1500 Nurses Dead from COVID-19 across 44 Countries: International Council of Nurses. Available online: https://www.ctvnews.ca/health/coronavirus/1-500-nurses-dead-from-covid-19-across-44-countries-international-council-of-nurses-1.5165352 (accessed on 15 April 2021).
- Buerhaus, P.I.; Auerbach, D.I.; Staiger, D.O. Older Clinicians and the Surge in Novel Coronavirus Disease 2019 (COVID-19). JAMA 2020, 30. [Google Scholar] [CrossRef]
- Al-Dossary, R.; Alamri, M.; AlBaqawi, H.; Al Hosis, K.; Aljeldah, M.; Aljohan, M.; Aljohani, K.; Almadani, N.; Alrasheadi, B.; Falatah, R.; et al. Awareness, Attitudes, Prevention, and Perceptions of COVID-19 Outbreak Among Nurses in Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 8269. [Google Scholar] [CrossRef]
- Alosaimi, D.N.; Ahmad, M. The Challenges of Cultural Competency Among Expatriate Nurses Working in Kingdom of Saudi Arabia. Res. Theory Nurs. Pract. 2016, 30, 302–319. [Google Scholar] [CrossRef]
- Johns Hopkins University & Medicine. Coronavirus Resource Center: COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE). Available online: https://0-coronavirus-jhu-edu.brum.beds.ac.uk/map.html (accessed on 25 March 2021).
- Mounts, A.; World Health Organization; De La Rocque, S.; Fitzner, J.; Garcia, E.; Thomas, H.; Brown, D.; Schuster, H.; Vandemaele, K.; Esmat, H.; et al. The early response to a novel coronavirus in the Middle East. East. Mediterr. Health J. 2013, 19, S19–S25. [Google Scholar] [CrossRef]
- Malik, M.R.; Mahjour, J. Closing the knowledge gaps on MERS: Three and half years since its detection, what have we learnt and what needs to be done urgently? East Mediterr. Health J. 2016, 22, 85–86. [Google Scholar] [CrossRef]
- Barry, M.; Ghonem, L.; Alsharidi, A.; Alanazi, A.; Alotaibi, N.; Al-Shahrani, F.; Majid, F.; BaHammam, A. Coronavirus disease-2019 pandemic in the Kingdom of Saudi Arabia: Mitigation measures and hospital preparedness. J. Nat. Sci. Med. 2020, 3, 155. [Google Scholar] [CrossRef]
- Alandijany, T.A.; Faizo, A.A.; Azhar, E.I. Coronavirus disease of 2019 (COVID-19) in the Gulf Cooperation Council (GCC) countries: Current status and management practices. J. Infect. Public Health 2020, 13, 839–842. [Google Scholar] [CrossRef]
- The Milli Chronicle. Saudi Arabia and UAE in Top-20 Safest Coronavirus Countries List: Hong Kong-Based Research 2020. Available online: https://millichronicle.com/tag/deep-knowledge-group/ (accessed on 5 February 2021).
- Alajmi, J.; Jeremijenko, A.M.; Abraham, J.C.; Alishaq, M.; Concepcion, E.G.; Butt, A.A.; Abou-Samra, A.-B. COVID-19 infection among healthcare workers in a national healthcare system: The Qatar experience. Int. J. Infect. Dis. 2020, 100, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Güldaval, F.; Anar, C.; Gayaf, M.; Büyükşirin, M.; Polat, G.; Karadeniz, G.; Alpözen, A.; Ayrancı, A.; Üçsular, F.; Seymenoğlu, Z.; et al. Clinical presentation of health care workers with symptoms of coronavirus disease 2019 at the İzmir tertiary education hospital, during an early phase of the pandemic. Tuberk. Toraks 2020, 68, 218–226. [Google Scholar] [CrossRef]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.-M.; Bai, P.; He, W.; Wu, F.; Liu, X.-F.; Han, D.-M.; Liu, S.; Yang, J.-K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Alahdal, H.M.; Alotaibi, R.M.; Sonbol, H.S.; Almaghrabi, R.H.; Alsofayan, Y.M.; Althunayyan, S.M.; Alsaif, F.A.; Almudarra, S.S.; Alabdulkareem, K.I.; et al. Controlling COVID-19 Pandemic: A Mass Screening Experience in Saudi Arabia. Front. Public Health 2021, 8, 606385. [Google Scholar] [CrossRef] [PubMed]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 23. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Month | Number of Patients Screened with PCR for SARS-CoV-2 | Number SARS-CoV-2 Positive Tests | ||
|---|---|---|---|---|
| Healthcare Workers n (%) | Patients n (%) | Total n (%) | ||
| March | 7 | 0 (0) | 0 (0) | 0 (0) |
| April | 43 | 0 (0) | 0 (0) | 0 (0) |
| May | 111 | 14 (12.6) | 4 (3.6) | 18 (16.2) |
| June | 403 | 74 (18.4) | 24 (5.9) | 98 (24.3) |
| July | 452 | 36 (7.9) | 17 (3.8) | 53 (11.7) |
| August | 639 | 25 (3.9) | 33 (5.2) | 58 (9.1) |
| September | 715 | 18 (2.5) | 30 (4.2) | 48 (6.7) |
| October | 769 | 7 (0.9) | 16 (2.1) | 23 (3) |
| November | 808 | 15 (1.9) | 16 (1.9) | 31 (3.8) |
| December | 515 | 14 (2.7) | 15 (2.9) | 29 (5.6) |
| Total | 4462 | 203 (4.5) | 155 (3.5) | 358 (8.0) |
| Demographic Variables | Frequency (n = 203) | Percentage |
|---|---|---|
| Gender | ||
| Male | 125 | 61.6 |
| Female | 78 | 38.4 |
| Age | ||
| <40 years | 130 | 64 |
| ≥40 years | 73 | 36 |
| Mean Age | 37.3 ± 9.1 (range 21–62) | |
| Nationality | ||
| Saudi | 75 | 36.9 |
| Filipino | 49 | 24.1 |
| Indian | 35 | 17.2 |
| Malaysian | 17 | 8.4 |
| Pakistan | 11 | 5.4 |
| Sudanese | 5 | 2.5 |
| Egyptian | 4 | 2 |
| Bangladesh | 2 | 1 |
| Palestinian | 2 | 1 |
| South African | 1 | 0.5 |
| Tunisian | 1 | 0.5 |
| Yemeni | 1 | 0.5 |
| Travel History Overseas | ||
| Yes | 2 | 1 |
| No | 201 | 99 |
| Mortality | ||
| Yes | 0 | 0 |
| No | 203 | 100 |
| Symptoms | Frequency (n = 203) | Percentage |
|---|---|---|
| Fever | 128 | 63.1 |
| Dry cough | 123 | 60.6 |
| Sore throat | 97 | 47.8 |
| Body aches | 124 | 61.8 |
| Loss of appetite | 73 | 36 |
| Chills | 57 | 28.1 |
| Fatigue | 94 | 46.3 |
| Headache | 113 | 55.7 |
| Vomiting | 18 | 8.9 |
| Diarrhea | 41 | 20.2 |
| Loss of taste | 76 | 37.4 |
| Loss of smell | 73 | 36 |
| Shortness of breath | 50 | 24.6 |
| Runny nose | 65 | 32 |
| Body weakness | 97 | 47.8 |
| Asymptomatic | 6 | 2.9 |
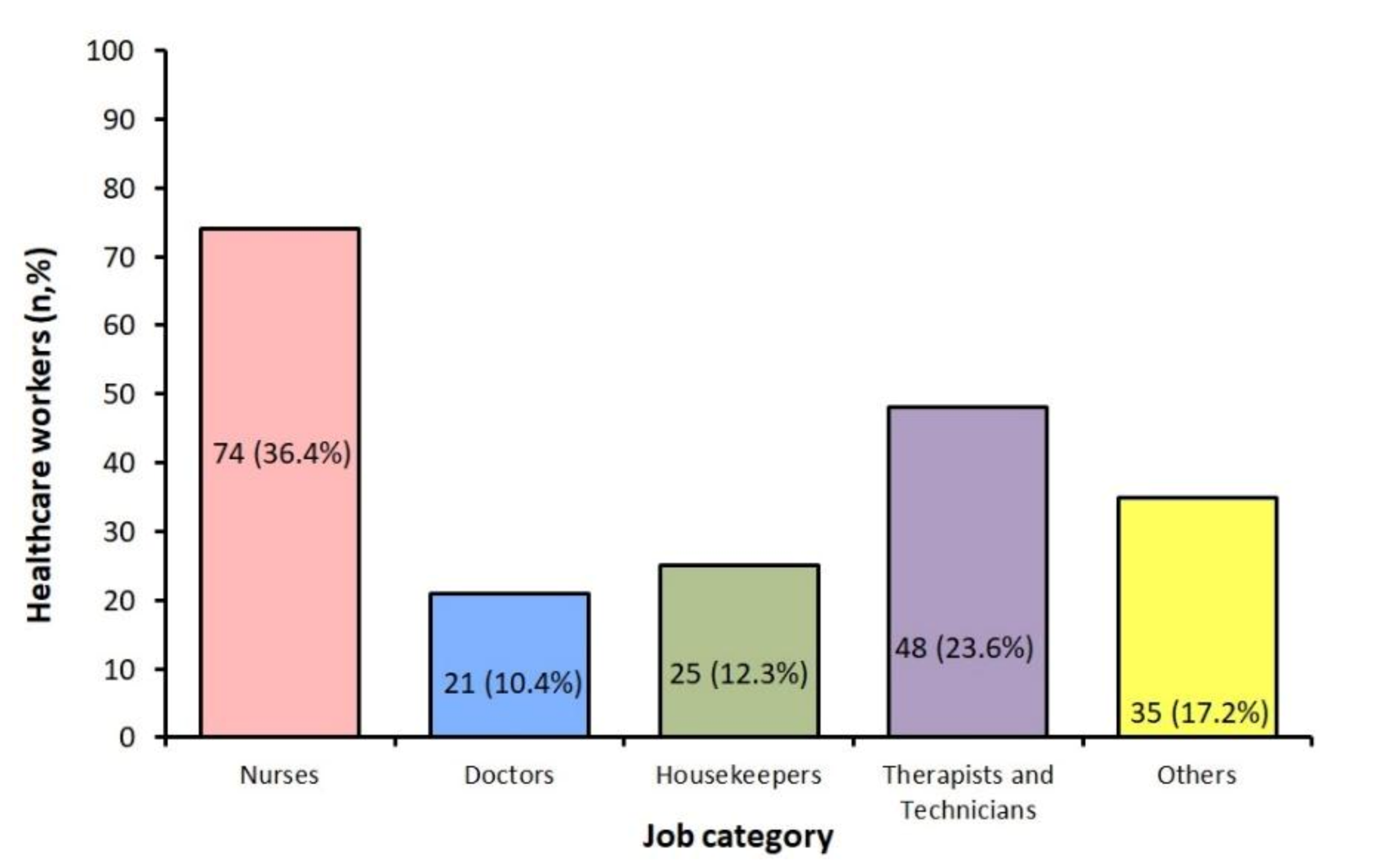
| Total N = 203 n (%) | Nurses N = 74 n (%) | Doctors N = 21 n (%) | Housekeepers N = 25 n (%) | Therapists and Technicians N = 48 n (%) | Others N = 35 n (%) | |
|---|---|---|---|---|---|---|
| Gender | ||||||
| Male | 125 (61.6) | 15 (20.3) | 19 (90.5) | 25 (100) | 37 (77.1) | 29 (82.9) |
| Female | 78 (38.4) | 59 (79.7) (p < 0.0001) | 2 (9.5) (p < 0.0001) | 0 | 11 (22.9) (p < 0.0001) | 6 (17.1) (p < 0.0001) |
| Age | ||||||
| <40 years | 130 (64) | 49 (66.2) | 7 (33.3) | 15 (60) | 34 (70.8) | 25 (71.4) |
| ≥40 years | 73 (36) | 25 (33.8) (p = 0.005) | 14 (66.7) (p = 0.127) | 10 (40) (p = 0.317) | 14 (29.2) (p = 0.004) | 10 (28.6) (p = 0.114) |
| Nationality | ||||||
| Saudi | 75 (36.9) | 19 (25.7) | 6 (28.6) | 0 | 30 (62.5) | 20 (57.1) |
| Non-Saudi | 128 (63.1) | 55 (74.3) (p < 0.0001) | 15 (71.4) (p = 0.050) | 25 (100) | 18 (37.5) (p = 0.083) | 15 (42.9) (p = 0.398) |
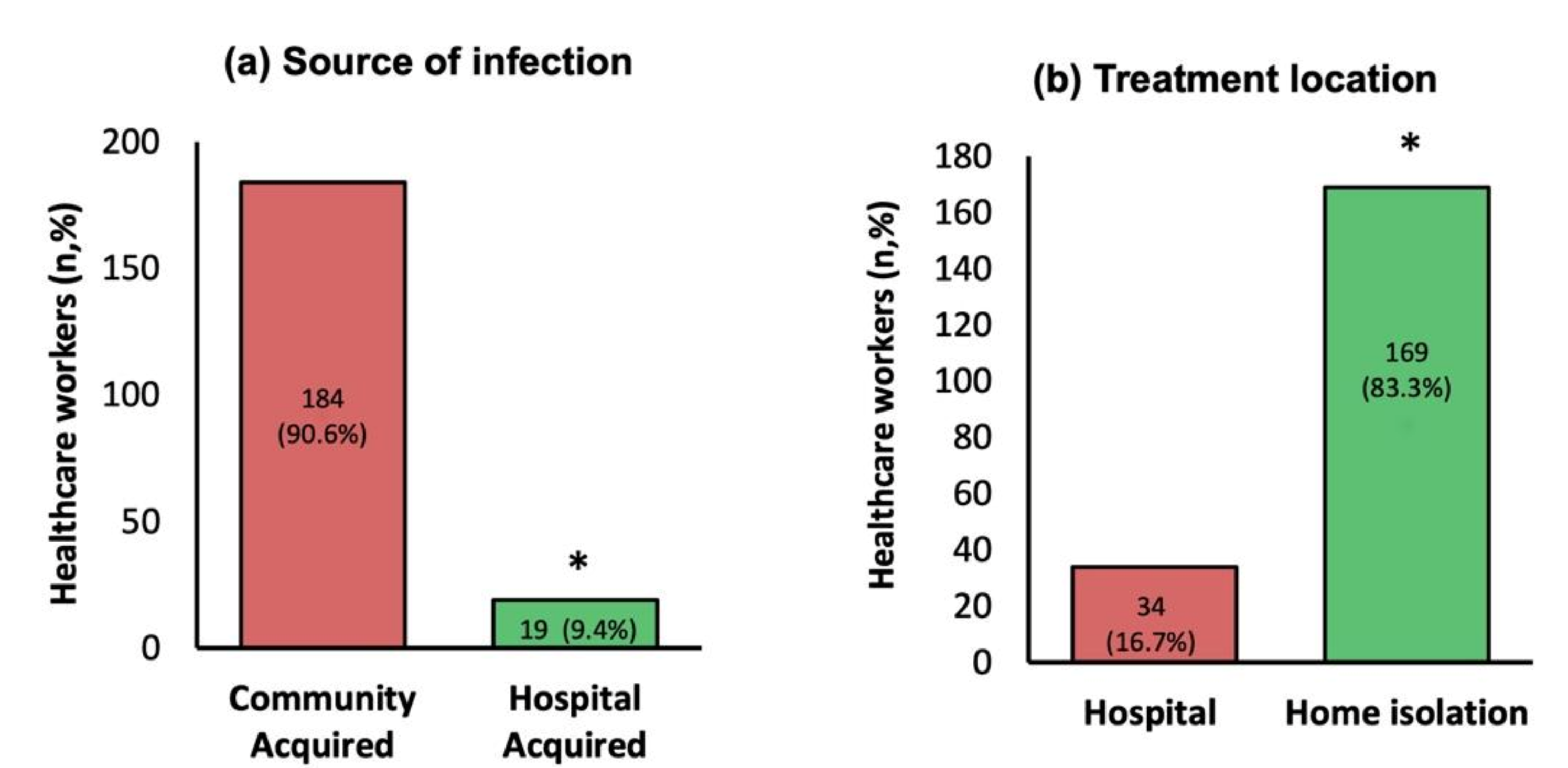
| Treatment Location | ||||||
| Home | 169 (83.3) | 72 (97.3) | 21 (100) | 1 (4) | 44 (91.7) | 31 (88.6) |
| Hospital | 34 (16.7) | 2 (2.7) (p < 0.0001) | 0 | 24 (96) (p < 0.0001) | 4 (8.3) (p < 0.0001) | 4 (11.4) (p < 0.0001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barry, M.; Robert, A.A.; Temsah, M.-H.; Abdul Bari, S.; Akhtar, M.Y.; Al Nahdi, F.; Erlandez, R.; Al-Tawfiq, J.A.; Al Khushail, A.; Al Hebaishi, Y. COVID-19 Community Transmission among Healthcare Workers at a Tertiary Care Cardiac Center. Med. Sci. 2021, 9, 49. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci9030049
Barry M, Robert AA, Temsah M-H, Abdul Bari S, Akhtar MY, Al Nahdi F, Erlandez R, Al-Tawfiq JA, Al Khushail A, Al Hebaishi Y. COVID-19 Community Transmission among Healthcare Workers at a Tertiary Care Cardiac Center. Medical Sciences. 2021; 9(3):49. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci9030049
Chicago/Turabian StyleBarry, Mazin, Asirvatham Alwin Robert, Mohamad-Hani Temsah, Syed Abdul Bari, Muhammad Yasin Akhtar, Faizah Al Nahdi, Richilda Erlandez, Jaffar A. Al-Tawfiq, Abdullah Al Khushail, and Yahya Al Hebaishi. 2021. "COVID-19 Community Transmission among Healthcare Workers at a Tertiary Care Cardiac Center" Medical Sciences 9, no. 3: 49. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci9030049