
Reduction in Fatigue Symptoms Following the Administration of Nutritional Supplements in Patients with Multiple Sclerosis



 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Processing and Analysis of Blood Samples
2.3. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Serum Biochemical Parameters
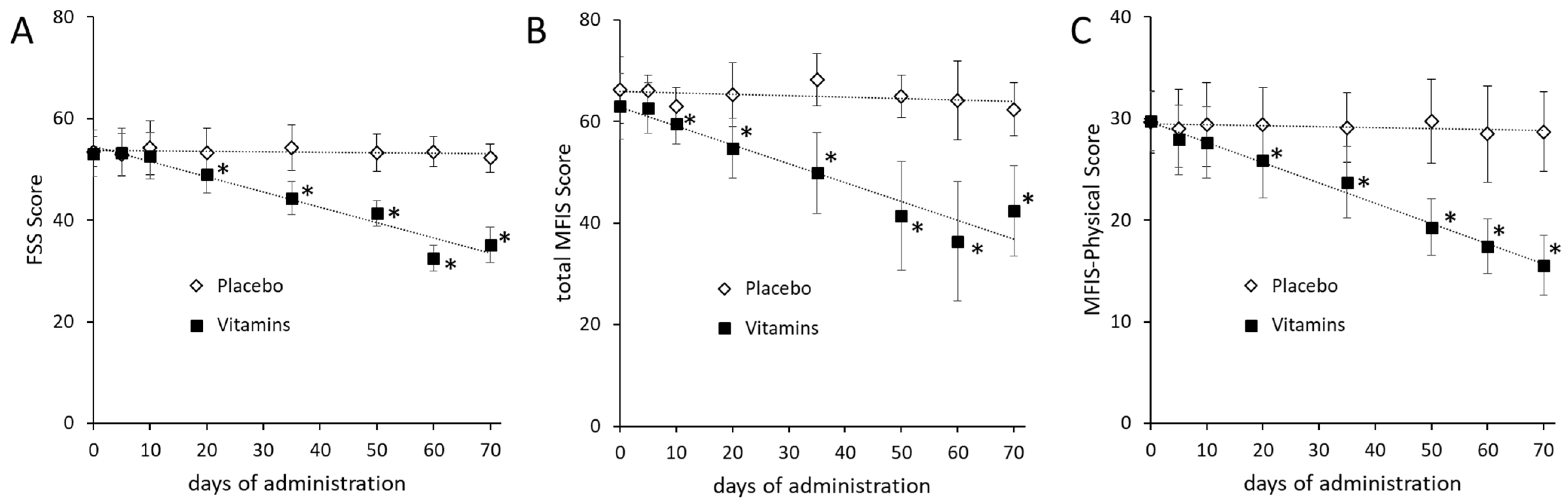
3.3. Effects of Nutritional Supplementation on Fatigue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Javed, A.; Khan, O. Acute disseminated encephalomyelitis. Handb. Clin. Neurol. 2014, 123, 705–717. [Google Scholar] [PubMed]
- Ascherio, A.; Munger, K.L. Environmental risk factors for multiple sclerosis, part II: Noninfectious factors. Ann. Neurol. 2007, 61, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Gilgun-Sherki, Y.; Melamed, E.; Offen, D. The role of oxidative stress in the pathogenesis of multiple sclerosis: The need for effective antioxidant therapy. J. Neurol. 2004, 251, 261–268. [Google Scholar]
- Lee, K.H.; Cha, M.; Lee, B.H. Neuroprotective Effect of Antioxidants in the Brain. Int. J. Mol. Sci. 2020, 21, 7152. [Google Scholar] [CrossRef]
- Bromley, L.; Horvath, P.J.; Bennett, S.E.; Weinstock-Guttman, B.; Ray, A.D. Impact of Nutritional Intake on Function in People with Mild-to-Moderate Multiple Sclerosis. Int. J. MS Care 2019, 21, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossman, P.; Kappos, L.; Gensicke, H.; D’Souza, M.; Mohr, D.C.; Penner, I.K.; Steiner, C. MS QOL, depression, and fatigue improve after mindfulness training: A randomized trial. Neurology 2010, 75, 1141–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newland, P.; Starkweather, A.; Sorenson, M. Central fatigue in multiple sclerosis: A review of the literature. J. Spinal Cord Med. 2016, 39, 386–399. [Google Scholar] [CrossRef]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.S.; LaRocca, N.G.; Miller, D.M.; Ritvo, P.G.; Andrews, H.; Paty, D. Recent developments in the assessment of QOL in multiple sclerosis (MS). Mult. Scler. 1999, 5, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Ayache, S.S.; Chalah, M.A. Fatigue in multiple sclerosis—Insights into evaluation and management. Neurophysiol. Clin. 2017, 47, 139–171. [Google Scholar] [CrossRef]
- Bagur, M.J.; Murcia, M.A.; Jiménez-Monreal, A.M.; Tur, J.A.; Bibiloni, M.M.; Alonso, G.L.; Martínez-Tomé, M. Influence of Diet in Multiple Sclerosis: A Systematic Review. Adv. Nutr. 2017, 8, 463–472. [Google Scholar] [CrossRef] [Green Version]
- Van Munster, C.E.; Uitdehaag, B.M. Outcome Measures in Clinical Trials for Multiple Sclerosis. CNS Drugs 2017, 31, 217–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckerman, H.; Eijssen, I.C.; van Meeteren, J.; Verhulsdonck, M.C.; de Groot, V. Fatigue Profiles in Patients with Multiple Sclerosis are Based on Severity of Fatigue and not on Dimensions of Fatigue. Sci. Rep. 2020, 10, 4167. [Google Scholar] [CrossRef]
- Schwarz, S.; Leweling, H. Multiple sclerosis and nutrition. Mult. Scler. 2005, 11, 24–32. [Google Scholar] [CrossRef]
- Flohé, L.; Günzler, W.A. Assays of glutathione peroxidase. Methods Enzymol. 1984, 105, 114–120. [Google Scholar] [PubMed]
- Oberley, L.W.; Spitz, D.R. Assay of superoxide dismutase activity in tumor tissue. Methods Enzymol. 1984, 105, 457–464. [Google Scholar] [PubMed]
- Flachenecker, P.; Kümpfel, T.; Kallmann, B.; Gottschalk, M.; Grauer, O.; Rieckmann, P.; Trenkwalder, C.; Toyka, K.V. Fatigue in multiple sclerosis: A comparison of different rating scales and correlation to clinical parameters. Mult. Scler. 2002, 8, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Gruszczak, A.; Bartosik-Psujek, H.; Pocińska, K.; Stelmasiak, Z. Validation analysis of selected psychometric features of Polish version of Modified Fatigue Impact Scale-preliminary findings. Neurol. Neurochir. Pol. 2009, 43, 148–154. [Google Scholar] [PubMed]
- Hernández-Ledesma, A.L.; Rodríguez-Méndez, A.J.; Gallardo-Vidal, L.S.; García-Gasca, T.; Alatorre-Cruz, J.M.; García-Solís, P.; Reyes, J.L.; Solís-Saínz, J.C. Lipid profile: Causal relationship on cognitive performance in multiple sclerosis? Mol. Biol. Rep. 2020, 47, 9667–9676. [Google Scholar] [CrossRef] [PubMed]
- Ascherio, A. Environmental factors in multiple sclerosis. Expert Rev. Neurother. 2013, 13 (Suppl. 12), 3–9. [Google Scholar] [CrossRef] [PubMed]
- Waubant, E.; Lucas, R.; Mowry, E.; Graves, J.; Olsson, T.; Alfredsson, L.; Langer-Gould, A. Environmental and genetic risk factors for MS: An integrated review. Ann. Clin. Transl. Neurol. 2019, 6, 1905–1922. [Google Scholar] [CrossRef] [PubMed]
- Tryfonos, C.; Mantzorou, M.; Fotiou, D.; Vrizas, M.; Vadikolias, K.; Pavlidou, E.; Giaginis, C. Dietary Supplements on Controlling Multiple Sclerosis Symptoms and Relapses: Current Clinical Evidence and Future Perspectives. Medicines 2019, 6, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sand, I.K. The Role of Diet in Multiple Sclerosis: Mechanistic Connections and Current Evidence. Curr. Nutr. Rep. 2018, 7, 150–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besler, H.T.; Comoğlu, S.; Okçu, Z. Serum levels of antioxidant vitamins and lipid peroxidation in multiple sclerosis. Nutr. Neurosci. 2002, 5, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Wesnes, K.; Myhr, K.M.; Riise, T.; Kvistad, S.S.; Torkildsen, Ø.; Wergeland, S.; Holmøy, T.; Midgard, R.; Bru, A.; Edland, A.; et al. Low vitamin D, but not tobacco use or high BMI, is associated with long-term disability progression in multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 50, 102801. [Google Scholar] [CrossRef] [PubMed]
- Feige, J.; Moser, T.; Bieler, L.; Schwenker, K.; Hauer, L.; Sellner, J. Vitamin D Supplementation in Multiple Sclerosis: A Critical Analysis of Potentials and Threats. Nutrients 2020, 12, 783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Carbonell, C.; Charvet, L.E.; Krupp, L.B. Enhancing Mood, Cognition, and Quality of Life in Pediatric Multiple Sclerosis. Pediatr. Drugs 2021, 23, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Simpson-Yap, S.; Jelinek, P.; Weiland, T.; Nag, N.; Neate, S.; Jelinek, G. Self-reported use of vitamin D supplements is associated with higher physical quality of life scores in multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 49, 102760. [Google Scholar] [CrossRef]
- Nemazannikova, N.; Mikkelsen, K.; Stojanovska, L.; Blatch, G.L.; Apostolopoulos, V. Is there a Link between Vitamin B and Multiple Sclerosis? Med. Chem. 2018, 14, 170–180. [Google Scholar] [CrossRef]
- Zhu, Y.; He, Z.Y.; Liu, H.N. Meta-analysis of the relationship between homocysteine, vitamin B12, folate, and multiple sclerosis. J. Clin. Neurosci. 2011, 18, 933–938. [Google Scholar] [CrossRef]
- Dardiotis, E.; Arseniou, S.; Sokratous, M.; Tsouris, Z.; Siokas, V.; Mentis, A.-F.A.; Michalopoulou, A.; Andravizou, A.; Dastamani, M.; Paterakis, K.; et al. Vitamin B12, folate, and homocysteine levels and multiple sclerosis: A meta-analysis. Mult. Scler. Relat. Disord. 2017, 17, 190–197. [Google Scholar] [CrossRef]
- Li, X.; Yuan, J.; Han, J.; Hu, W. Serum levels of Homocysteine, Vitamin B12 and Folate in Patients with Multiple Sclerosis: An Updated Meta-Analysis. Int. J. Med. Sci. 2020, 17, 751–761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nourbakhsh, B.; Julian, L.; Waubant, E. Fatigue and depression predict quality of life in patients with early multiple sclerosis: A longitudinal study. Eur. J. Neurol. 2016, 23, 1482–1486. [Google Scholar] [CrossRef] [PubMed]
- Braley, T.J.; Chervin, R.D. Fatigue in multiple sclerosis: Mechanisms, evaluation, and treatment. Sleep 2010, 33, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Morris, G.; Berk, M.; Walder, K.; Maes, M. Central pathways causing fatigue in neuro-inflammatory and autoimmune illnesses. BMC Med. 2015, 13, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottschalk, M.; Kümpfel, T.; Flachenecker, P.; Uhr, M.; Trenkwalder, C.; Holsboer, F.; Weber, F. Fatigue and regulation of the hypothalamo-pituitary-adrenal axis in multiple sclerosis. Arch. Neurol. 2005, 62, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Téllez, N.; Comabella, M.; Julià, E.; Río, J.; Tintoré, M.; Brieva, L.; Nos, C.; Montalban, X. Fatigue in progressive multiple sclerosis is associated with low levels of dehydroepiandrosterone. Mult. Scler. J. 2006, 12, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Nourbakhsh, B.; Revirajan, N.; Waubant, E. Association between glutamate blockade and fatigue in patients with multiple sclerosis. JAMA Neurol. 2015, 72, 1374–1375. [Google Scholar] [CrossRef] [Green Version]
- Sitar, M.E.; Aydin, S.; Cakatay, U. Human serum albumin and its relation with oxidative stress. Clin. Lab. 2013, 59, 945–952. [Google Scholar] [CrossRef]
- Prajapati, K.D.; Sharma, S.S.; Roy, N. Current perspectives on potential role of albumin in neuroprotection. Rev. Neurosci. 2011, 22, 355–363. [Google Scholar] [CrossRef]
- Zhang, S.Y.; Gui, L.N.; Liu, Y.Y.; Shi, S.; Cheng, Y. Oxidative Stress Marker Aberrations in Multiple Sclerosis: A Meta-Analysis Study. Front. Neurosci. 2020, 14, 823. [Google Scholar] [CrossRef] [PubMed]
- Sanoobar, M.; Dehghan, P.; Khalili, M.; Azimi, A.; Seifar, F. Coenzyme Q10 as a treatment for fatigue and depression in multiple sclerosis patients: A double blind randomized clinical trial. Nutr. Neurosci. 2016, 19, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Kouchaki, E.; Afarini, M.; Abolhassani, J.; Mirhosseini, N.; Bahmani, F.; Masoud, S.A.; Asemi, Z. High-dose ω-3 Fatty Acid Plus Vitamin D3 Supplementation Affects Clinical Symptoms and Metabolic Status of Patients with Multiple Sclerosis: A Randomized Controlled Clinical Trial. J. Nutr. 2018, 148, 1380–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krysko, K.M.; Bischof, A.; Nourbakhsh, B.; Henry, R.G.; Revirajan, N.; Manguinao, M.; Nguyen, K.; Akula, A.; Li, Y.; Waubant, E. A pilot study of oxidative pathways in MS fatigue: Randomized trial of N-acetyl cysteine. Ann. Clin. Transl. Neurol. 2021, 8, 811–824. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.Y.; Lee, P.; Adany, P.; Hughes, A.J.; Belliston, S.; Denney, D.R.; Lynch, S.G. In vivo evidence of oxidative stress in brains of patients with progressive multiple sclerosis. Mult. Scler. J. 2018, 24, 1029–1038. [Google Scholar] [CrossRef] [PubMed]
- Giacci, M.K.; Bartlett, C.A.; Smith, N.M.; Iyer, K.S.; Toomey, L.M.; Jiang, H.; Guagliardo, P.; Kilburn, M.R.; Fitzgerald, M. Oligodendroglia are particularly vulnerable to oxidative damage after neurotrauma in vivo. J. Neurosci. 2018, 38, 6491–6504. [Google Scholar] [CrossRef] [Green Version]
- Maggi, P.; Kuhle, J.; Schädelin, S.; van der Meer, F.; Weigel, M.; Galbusera, R.; Mathias, A.; Lu, P.J.; Rahmanzadeh, R.; Benkert, P.; et al. Chronic white matter inflammation and serum neurofilament levels in multiple sclerosis. Neurology 2021, 4, 10–12. [Google Scholar]
- Torricelli, P.; Antonelli, F.; Ferorelli, P.; De Martino, A.; Shevchenko, A.; Beninati, S. Multiple Sclerosis: Effect of oral administration of an antioxidant dietary supplement in C57BL6/N induced model of experimental autoimmune encephalomyelitis. Am. J. Clin. Exp. Med. 2015, 3, 83–87. [Google Scholar]
- Ansar, W.; Ghosh, S. Inflammation and Inflammatory Diseases, Markers, and Mediators: Role of CRP in Some Inflammatory Diseases. Biol. C React. Protein Health Dis. 2016, 24, 67–107. [Google Scholar]
- Dionyssiotis, Y. Bone loss and fractures in multiple sclerosis: Focus on epidemiologic and physiopathological features. Int. J. Gen. Med. 2011, 4, 505–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beavers, K.M.; Brinkley, T.E.; Nicklas, B.J. Effect of exercise training on chronic inflammation. Clin. Chim. Acta 2010, 411, 785–793. [Google Scholar] [CrossRef] [Green Version]
- Cui, C.; Sun, J.; Pawitan, Y.; Piehl, F.; Chen, H.; Ingre, C.; Wirdefeldt, K.; Evans, M.; Andersson, J.; Carrero, J.J.; et al. Creatinine and C-reactive protein in amyotrophic lateral sclerosis, multiple sclerosis and Parkinson’s disease. Brain Commun. 2020, 2, fcaa152. [Google Scholar] [CrossRef] [PubMed]
- Pandhi, P.; Streng, K.W.; Anker, S.D.; Cleland, J.G.; Damman, K.; Dickstein, K.; Pellicori, P.; Lang, C.C.; Ng, L.; Samani, N.J.; et al. The value of spot urinary creatinine as a marker of muscle wasting in patients with new-onset or worsening heart failure. J. Cachexia Sarcopenia Muscle. 2021, 12, 555–567. [Google Scholar] [CrossRef] [PubMed]
- Fragoso, Y.D.; Stoney, P.N.; McCaffery, P.J. The evidence for a beneficial role of vitamin A in multiple sclerosis. CNS Drugs 2014, 28, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Bitarafan, S.; Saboor-Yaraghi, A.; Sahraian, M.A.; Nafissi, S.; Togha, M.; Beladi Moghadam, N.; Roostaei, T.; Siassi, F.; Eshraghian, M.R.; Ghanaati, H.; et al. Impact of vitamin A supplementation on disease progression in patients with multiple sclerosis. Arch. Iran. Med. 2015, 18, 435–440. [Google Scholar] [PubMed]
- Racke, M.K.; Burnett, D.; Pak, S.H.; Albert, P.S.; Cannella, B.; Raine, C.S.; McFarlin, D.E.; Scott, D.E. Retinoid treatment of experimental allergic encephalomyelitis. IL-4 production correlates with improved disease course. J. Immunol. 1995, 154, 450–458. [Google Scholar] [PubMed]
- Ruschil, C.; Dubois, E.; Stefanou, M.I.; Kowarik, M.C.; Ziemann, U.; Schittenhelm, M.; Krumbholz, M.; Bischof, F. Treatment of progressive multiple sclerosis with high-dose all-trans retinoic acid—No clear evidence of positive disease modifying effects. Neurol. Res. Pract. 2021, 3, 25–35. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | All Sample N = 50 | Supplemented Group N = 25 | Placebo Group N = 25 | p-Value |
|---|---|---|---|---|
| age (years) | 39.60 (6.06) | 40.16 (5.73) | 39.04 (6.32) | 0.4715 * |
| height (m) | 1.69 (0.07) | 1.69 (0.08) | 1.69 (0.07) | 0.9840 * |
| weight (kg) | 69.04 (9.00) | 68.64 (7.53) | 69.44 (10.25) | 0.6384 * |
| BMI (kg/m2) | 24.11 (3.11) | 24.03 (2.86) | 24.20 (3.34) | 0.8259 * |
| duration MS (years) | 16.46 (2.87) | 16.04 (2.85) | 16.88 (2.82) | 0.2420 * |
| Placebo Group | Supplemented Group | |||
|---|---|---|---|---|
| TAS (U/mg protein) | 0.32 (0.20) | [0.24–0.40] | 0.89 (0.30) | [0.77–1.01] |
| SOD (U/mg protein) | 3.84 (1.80) | [3.10–4.58] | 6.43 (0.60) | [6.18–6.68] |
| GPx (U/mg protein) | 2.95 (0.56) | [2.72–3.18] | 4.95 (0.67) | [4.67–5.23] |
| CAT (U/mg protein) | 2.34 (1.37) | [1.77–2.91] | 5.24 (1.27) | [4.72–5.76] |
| Placebo Group | Supplemented Group | |||
|---|---|---|---|---|
| Glycemia (mg/dL) | 84.52 (10.37) | [80.24–88.80] | 94.61 (6.30) | [92.01–97.21] |
| Total Cholesterol (mg/dL) | 182.70 (42.88) | [165.00–200.40] | 232.84 (52.22) | [211.28–254.39] |
| Triglycerides (mg/dL) | 104.75 (52.72) | [82.99–126.51] | 112.73 (32.24) | [99.42–126.04] |
| Total Lipids (mg/dL) | 632.82 (130.42) | [578.98–686.65] | 732.86 (100.20) | [691.50–774.22] |
| Albumin (g/dL) | 4.45 (0.52) | [4.23–4.66] | 7.45 (0.32) | [7.32–7.58] |
| Creatinine (mg/dL) | 0.35 (0.02) | [0.34–0.36] | 0.83 (0.25) | [0.73–0.93] |
| RBP (mg/dL) | 2.12 (1.50) | [1.60–2.64] | 5.82 (1.92) | [5.03–6.61] |
| CRP (mg/L) | 18.45 (9.53) | [14.52–22.38] | 9.22 (6.42) | [6.57–11.87] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferorelli, P.; Antonelli, F.; Shevchenko, A.; Mischiati, C.; Doepp, M.; Lenzi, S.; Borromeo, I.; Feriotto, G.; Beninati, S. Reduction in Fatigue Symptoms Following the Administration of Nutritional Supplements in Patients with Multiple Sclerosis. Med. Sci. 2021, 9, 52. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci9030052
Ferorelli P, Antonelli F, Shevchenko A, Mischiati C, Doepp M, Lenzi S, Borromeo I, Feriotto G, Beninati S. Reduction in Fatigue Symptoms Following the Administration of Nutritional Supplements in Patients with Multiple Sclerosis. Medical Sciences. 2021; 9(3):52. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci9030052
Chicago/Turabian StyleFerorelli, Pasquale, Francesco Antonelli, Anna Shevchenko, Carlo Mischiati, Manfred Doepp, Stefano Lenzi, Ilaria Borromeo, Giordana Feriotto, and Simone Beninati. 2021. "Reduction in Fatigue Symptoms Following the Administration of Nutritional Supplements in Patients with Multiple Sclerosis" Medical Sciences 9, no. 3: 52. https://0-doi-org.brum.beds.ac.uk/10.3390/medsci9030052