The Evaluation of a Mind-Body Intervention (MBT-T) for Stress Reduction in Academic Settings: A Pilot Study



{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
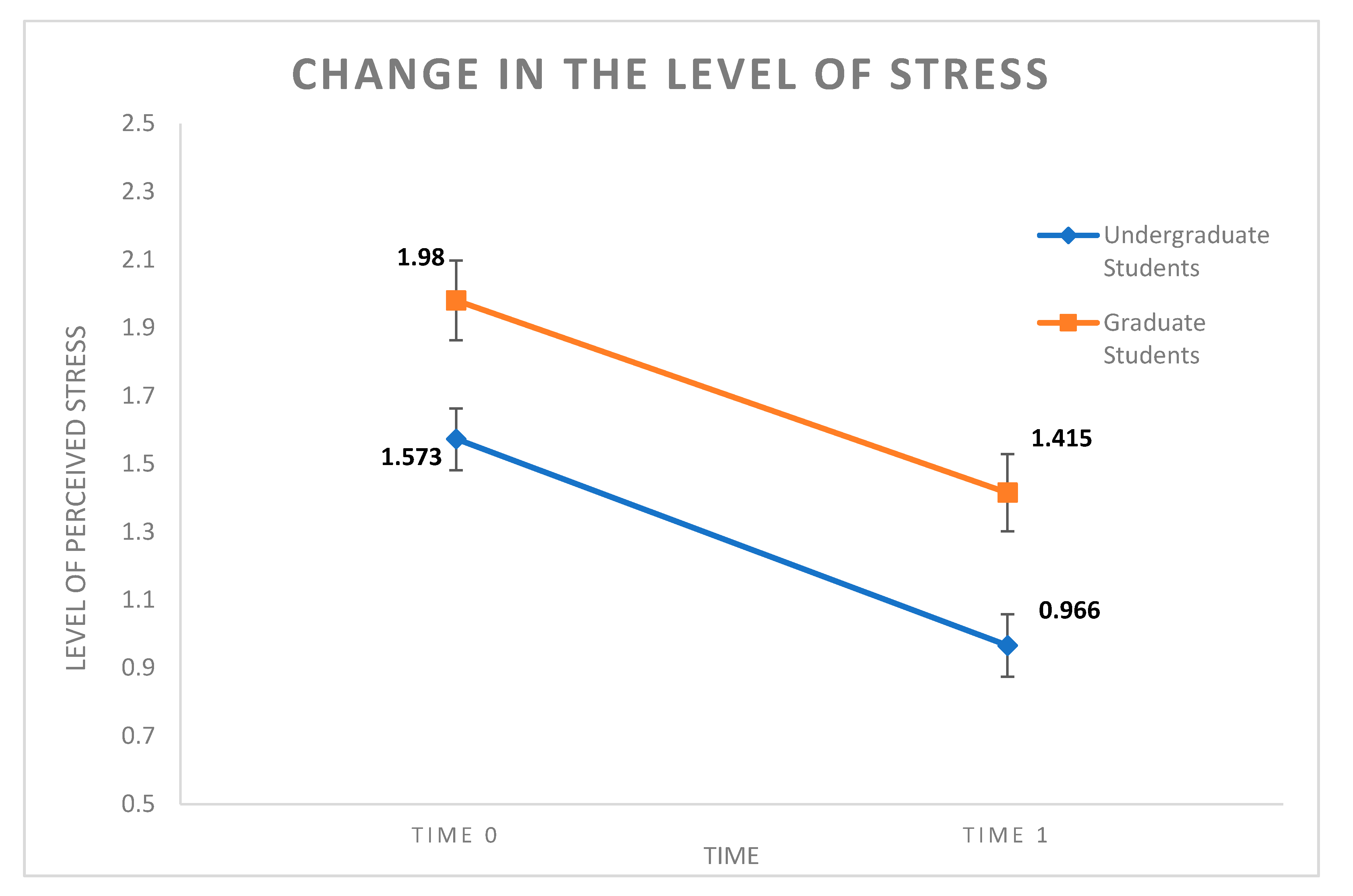
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. The Creative Psychosocial Genomic Healing Experience: A Brief Protocol
References
- Joshi, A.R.; Nagpal, M. Assessment of Perceived Stress in Postgraduate Medical Students during Training Programme. J. Clin. Diagnostic Res. 2018, 12, 1–4. [Google Scholar] [CrossRef]
- Grover, S.; Dua, D.; Shouan, A.; Nehra, R.; Avasthi, A. Perceived stress and barriers to seeking help from mental health professionals among trainee doctors at a tertiary care centre in North India. Asian J. Psychiatr. 2019, 39, 143–149. [Google Scholar] [CrossRef]
- Jiang, Y.; Guan, Y.; Dai, D.; Huang, W.; Huang, Z. Prevalence of stress and its determinants among residents enrolled in china standardized training program for resident doctor (C-STRD) program: A cross-sectional study. PLoS ONE 2019, 1. [Google Scholar] [CrossRef]
- Vanheusden, K.; Mulder, C.L.; van der Ende, J.; van Lenthe, F.J.; Mackenbach, J.P.; Verhulst, F.C. Young adults face major barriers to seeking help from mental health services. Patient Educ. Couns. 2008, 73, 97–104. [Google Scholar] [CrossRef]
- Jennings, K.S.; Goguen, K.N.; Britt, T.W.; Jeffirs, S.M.; Wilkes, J.R.; Brady, A.R.; Pittman, R.A.; DiMuzio, D.J. The role of personality traits and barriers to mental health treatment seeking among college students. Psychol. Serv. 2017, 14, 513–523. [Google Scholar] [CrossRef]
- Girelli, L.; Alivernini, F.; Salvatore, S.; Cozzolino, M.; Sibilio, M.; Lucidi, F. Coping with the first exams: Motivation, autonomy support and perceived control predict the performance of first-year university students. J. Educ. Cult. Psychol. Stud. 2018, 2018, 165–185. [Google Scholar] [CrossRef]
- Venuleo, C.; Mangeli, G.; Mossi, P.; Amico, A.F.; Cozzolino, M.; Distante, A.; Ignone, G.; Savarese, G.; Salvatore, S. The Cardiac Rehabilitation Psychodynamic Group intervention (CR-PGI): An explorative study. Front. Psychol. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Rocco, D.; Pastore, M.; Gennaro, A.; Salvatore, S.; Cozzolino, M.; Scorza, M. Beyond verbal behavior: An empirical analysis of speech rates in psychotherapy sessions. Front. Psychol. 2018, 9, 978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, E.L.; Rossi, K.L.; Yount, G.; Cozzolino, M.; Iannotti, S. The Bioinformatics of Integrative Medical Insights: Proposals for an International Psycho-Social and Cultural Bioinformatics Project. Integr. Med. Insights 2006, 1, 7–26. [Google Scholar] [CrossRef]
- Rossi, E.L.; Cozzolino, M.; Mortimer, J.; Atkinson, D.; Rossi, K.L. A Brief Protocol for the Creative Psychosocial Genomic Healing Experience: The 4-Stage Creative Process in Therapeutic Hypnosis and Brief Psychotherapy. Am. J. Clin. Hypn. 2011, 54, 133–152. [Google Scholar] [CrossRef] [PubMed]
- Cozzolino, M.; Girelli, L.; Vivo, D.R.; Limone, P.; Celia, G. A mind-body intervention for stress reduction as an adjunct to an information session on stress management in university students. Brain Behav. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein-Fox, L.; Park, C.L.; Riley, K.E. Mindfulness and emotion regulation: Promoting well-being during the transition to college. Anxiety, Stress Coping 2018, 31, 639–653. [Google Scholar] [CrossRef] [PubMed]
- Gallego, J.; Aguilar-Parra, J.M.; Cangas, A.J.; Rosado, A.; Langer, Á.I. Efecto de intervenciones mente/cuerpo sobre los niveles de ansiedad, estrés y depresión en futuros docentes de edu. Rev. Psicodidact. 2016, 21, 87–101. [Google Scholar] [CrossRef] [Green Version]
- Meier, N.F.; Welch, A.S. Walking versus biofeedback: A comparison of acute interventions for stressed students. Anxiety Stress Coping 2016, 29, 463–478. [Google Scholar] [CrossRef]
- Running, A.; Hildreth, L. A Pilot Study: The Effect of Bio-Energy on Stress for University Faculty, Staff, and Students During Finals Week. J. Holist. Nurs. 2017, 35, 25–32. [Google Scholar] [CrossRef]
- Saoji, A.; Mohanty, S.; Vinchurkar, S.A. Effect of a Single Session of a Yogic Meditation Technique on Cognitive Performance in Medical Students: A Randomized Crossover Trial. J. Relig. Health 2017, 56, 141–148. [Google Scholar] [CrossRef]
- Cozzolino, M.; Cicatelli, A.; Fortino, V.; Guarino, F.; Tagliaferri, R.; Castiglione, S.; De Luca, P.; Napolitano, F.; Celia, G.; Iannotti, S.; et al. The Mind-Body Healing Experience (MHE) Is associated with Gene Expression in Human Leukocytes. Int. J. Phys. Soc. Sci. 2015, 5, 361–374. [Google Scholar]
- Hsieh, J.; Eisch, A.J. Epigenetics, hippocampal neurogenesis, and neuropsychiatric disorders: Unraveling the genome to understand the mind. Neurobiol. Dis. 2010, 39, 73–84. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, D.; Rossi, E.L. Ultradian rhythms from molecules to mind: A new vision of life; Springer: Dordrecht, The Netherlands, 2008; ISBN 9781402083518. [Google Scholar]
- Buric, I.; Farias, M.; Jong, J.; Mee, C.; Brazil, I.A. What is the molecular signature of mind-body interventions? A systematic review of gene expression changes induced by meditation and related practices. Front. Immunol. 2017, 8, 670. [Google Scholar] [CrossRef] [Green Version]
- Kanherkar, R.R.; Stair, S.E.; Bhatia-Dey, N.; Mills, P.J.; Chopra, D.; Csoka, A.B. Epigenetic Mechanisms of Integrative Medicine. Evidence-Based Complement. Altern. Med. 2017, 2017, 1–19. [Google Scholar] [CrossRef]
- Kuan, P.-F.; Waszczuk, M.A.; Kotov, R.; Marsit, C.J.; Guffanti, G.; Gonzalez, A.; Yang, X.; Koenen, K.; Bromet, E.; Luft, B.J. An epigenome-wide DNA methylation study of PTSD and depression in World Trade Center responders. Transl. Psychiatry 2017, 7, e1158. [Google Scholar] [CrossRef]
- Miller, M.W.; Maniates, H.; Wolf, E.J.; Logue, M.W.; Schichman, S.A.; Stone, A.; Milberg, W.; McGlinchey, R. CRP polymorphisms and DNA methylation of the AIM2 gene influence associations between trauma exposure, PTSD, and C-reactive protein. Brain. Behav. Immun. 2018, 67, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Niles, H.; Mehta, D.H.; Corrigan, A.A.; Bhasin, M.K.; Denninger, J.W. Functional genomics in the study of mind-body therapies. Ochsner J. 2014, 14, 681–695. [Google Scholar] [PubMed]
- Stillwell, S.B.; Vermeesch, A.L.; Scott, J.G. Interventions to reduce perceived stress among graduate students: A systematic review. Worldviews Evidence-Based Nurs. 2017, 00, 1–7. [Google Scholar]
- Upchurch, D.M.; Gill, M.; Jiang, L.; Prelip, M.; Slusser, W. Use of Mind–Body Therapies Among Young Adults Aged 18–24 Years: Findings From the 2012 National Health Interview Survey. J. Adolesc. Heal. 2018, 63, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Nanthakumar, C. The benefits of yoga in children. J. Integr. Med. 2018, 16, 14–19. [Google Scholar] [CrossRef]
- Wang, D.; Hagins, M. Perceived benefits of yoga among urban school students: A qualitative analysis. Evidence-Based Complement. Altern. Med. 2016, 2016, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Qin, S.; Zhou, Y.; Meng, L.; Su, H.; Zhang, J.; Qin, S.; Zhou, Y.; Meng, L.; Su, H.; et al. A randomized controlled trial of mindfulness-based tai chi chuan for subthreshold depression adolescents. Neuropsychiatr. Dis. Treat. 2018, 14, 2313–2321. [Google Scholar] [CrossRef] [Green Version]
- Sarkissian, M. Building Spiritual Capital: The Effects of Kundalini Yoga on Adolescent Stress, Emotional Affect, and Resilience. Ph.D. Thesis, Loyola Marymount University, Los Angeles, CA, USA, 2012. [Google Scholar]
- Soares, D.S.; Chan, L. Stress and wellbeing of junior doctors in Australia: A comparison with American doctors and population norms. BMC Med. Educ. 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Birtwell, K.; Williams, K.; van Marwijk, H.; Armitage, C.J.; Sheffield, D. An Exploration of Formal and Informal Mindfulness Practice and Associations with Wellbeing. Mindfulness (N. Y). 2019, 10, 89–99. [Google Scholar] [CrossRef] [Green Version]
- Bennett, K.; Dorjee, D. The Impact of a Mindfulness-Based Stress Reduction Course (MBSR) on Well-Being and Academic Attainment of Sixth-form Students. Mindfulness (N. Y). 2016, 7, 105–114. [Google Scholar] [CrossRef]
- AAP Section on Integrative Medicine. Mind-Body Therapies in Children and Youth. Pediatrics 2016, 138, e20161896. [Google Scholar] [CrossRef] [Green Version]
- Brancaleone, F. TBA: Terapia bionomico-autogena: Fondamenti, principi, tecniche e applicazioni; Franco Angeli: Milan, Italy, 2010; ISBN 8856822237. [Google Scholar]
- Dobkin, P.L.; Irving, J.A.; Amar, S. For whom may participation in a mindfulness-based stress reduction program be contraindicated? Mindfulness (N. Y.) 2012, 3, 44–50. [Google Scholar] [CrossRef]
- Guo, Y.; Xu, M.; Ji, M.; Wei, Z.; Zhang, J.; Hu, Q.; Yan, J.; Chen, Y.; Lyu, J.; Shao, X.; et al. The effect of Imaginary Working Qigong on the psychological well-being of college students. Medicine (Baltimore) 2018, 97, e13043. [Google Scholar] [CrossRef]
- Wielgosz, J.; Goldberg, S.B.; Kral, T.R.A.; Dunne, J.D.; Davidson, R.J. Mindfulness Meditation and Psychopathology. Annu. Rev. Clin. Psychol. 2019, 15, 285–316. [Google Scholar] [CrossRef]
- Cozzolino, M.; Tagliaferri, R.; Castiglione, S.; Fortino, V.; Cicatelli, A.; Guarino, F.; Napolitano, F.; Raiconi, G.; Celia, G.; De Luca, P.; et al. The Creative Psychosocial and Cultural Genomic Healing Experience: A new top-down epigenomic psychotherapeutic protocol. Int. J. Psychosoc. Cult. Genomics, Conscious. Heal. Res. 2014, 1, 18–26. [Google Scholar]
- Cozzolino, M.; Guarino, F.; Castiglione, S.; Cicatelli, A.; Celia, G. Pilot Study on Epigenetic Response to A Mind-Body Treatment. Transl. Med. @ UniSa 2017, 17, 40. [Google Scholar]
- Celia, G. Les styles narratifs du groupe comme indicateurs de changement. Rev. Psychother. Psychanal. Groupe 2020, 74, 157. [Google Scholar]
- Rossi, K.; Mortimer, J.; Rossi, E. Mind-Body Transformations Therapy (MBT-T). A single case study of trauma and rehabilitation. Int. J. Psychosoc. Genomics Conscious. Heal. Res. 2013, 1, 32–40. [Google Scholar]
- Rossi, E.; Rossi, K. The Creative Psychosocial Genomic Healing Experience©: An Open Invitation to Mind-Body Psychotherapy, Clinical & Experimental Research! Available online: [email protected] (accessed on 5 May 2020).
- Regehr, C.; Glancy, D.; Pitts, A. Interventions to reduce stress in university students: A review and meta-analysis. J. Affect. Disord. 2013, 148, 1–11. [Google Scholar] [CrossRef]
- Snowden, A.; White, C.A.; Christie, Z.; Murray, E.; McGowan, C.; Scott, R. The clinical utility of the Distress Thermometer: A review. Br. J. Nurs. 2014, 20, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, P.B.; Donovan, K.A.; Trask, P.C.; Fleishman, S.B.; Zabora, J.; Baker, F.; Holland, J.C. Screening for psychologic distress in ambulatory cancer patients: A multicenter evaluation of the distress thermometer. Cancer 2005, 103, 1494–1502. [Google Scholar] [CrossRef] [PubMed]
- Cutillo, A.; O’Hea, E.; Person, S.D.; Lessard, D.; Harralson, T.L.; Boudreaux, E. The distress thermometer: Cutoff points and clinical use. Oncol. Nurs. Forum 2017, 44, 329–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donovan, K.A.; Grassi, L.; McGinty, H.L.; Jacobsen, P.B. Validation of the Distress Thermometer worldwide: State of the science. Psychooncology. 2014, 23, 241–250. [Google Scholar] [CrossRef]
- Goebel, S.; Mehdorn, H.M. Measurement of psychological distress in patients with intracranial tumours: The NCCN distress thermometer. J. Neurooncol. 2011, 104, 357–364. [Google Scholar] [CrossRef]
- Gunnarsdottir, S.; Thorvaldsdottir, G.H.; Fridriksdottir, N.; Bjarnason, B.; Sigurdsson, F.; Skulason, B.; Smari, J. The psychometric properties of the Icelandic version of the Distress Thermometer and Problem List. Psychooncology. 2012, 21, 730–736. [Google Scholar] [CrossRef]
- Salkind, N.J. Encyclopedia of Research Design: Grounded Theory. Encycl. Res. Des. 2010, 181–186. [Google Scholar] [CrossRef]
- Beiter, R.; Nash, R.; McCrady, M.; Rhoades, D.; Linscomb, M.; Clarahan, M.; Sammut, S. The prevalence and correlates of depression, anxiety, and stress in a sample of college students. J. Affect. Disord. 2015, 173, 90–96. [Google Scholar] [CrossRef]
- Chaló, P.; Pereira, A.; Batista, P.; Sancho, L. Brief Biofeedback Intervention on Anxious Freshman University Students. Appl. Psychophysiol. Biofeedback 2017, 42, 163–168. [Google Scholar] [CrossRef]
- Alexander, A.; Barnett-Cowan, M.; Bartmess, E.; Bosco, F.A.; Brandt, M.; Carp, J.; Chandler, J.J.; Clay, R.; Cleary, H.; Cohn, M.; et al. An open, large-scale, collaborative effort to estimate the reproducibility of psychological science. Perspect. Psychol. Sci. 2012, 7, 657–660. [Google Scholar] [CrossRef] [Green Version]
- Simons, D.J. The Value of Direct Replication. Perspect. Psychol. Sci. 2014, 9, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Kahneman, D. A new etiquette for replication. Soc. Psychol. (Gott) 2014, 45, 310–311. [Google Scholar]
- Makel, M.C.; Plucker, J.A.; Hegarty, B. Replications in Psychology Research: How Often Do They Really Occur? Perspect. Psychol. Sci. 2012, 7, 537–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cozzolino, M.; Vivo, D.R.; Girelli, L.; Limone, P.; Celia, G. The Evaluation of a Mind-Body Intervention (MBT-T) for Stress Reduction in Academic Settings: A Pilot Study. Behav. Sci. 2020, 10, 124. https://0-doi-org.brum.beds.ac.uk/10.3390/bs10080124
Cozzolino M, Vivo DR, Girelli L, Limone P, Celia G. The Evaluation of a Mind-Body Intervention (MBT-T) for Stress Reduction in Academic Settings: A Pilot Study. Behavioral Sciences. 2020; 10(8):124. https://0-doi-org.brum.beds.ac.uk/10.3390/bs10080124
Chicago/Turabian StyleCozzolino, Mauro, Deborah R. Vivo, Laura Girelli, Pierpaolo Limone, and Giovanna Celia. 2020. "The Evaluation of a Mind-Body Intervention (MBT-T) for Stress Reduction in Academic Settings: A Pilot Study" Behavioral Sciences 10, no. 8: 124. https://0-doi-org.brum.beds.ac.uk/10.3390/bs10080124