
Treatment of Parkinson’s Disease with Cognitive Impairment: Current Approaches and Future Directions



Department of Neurology, University of Florida, Gainesville, FL 32611, USA
*
Author to whom correspondence should be addressed.
Behav. Sci. 2021, 11(4), 54; https://0-doi-org.brum.beds.ac.uk/10.3390/bs11040054
Submission received: 2 March 2021
/
Revised: 10 April 2021
/
Accepted: 14 April 2021
/
Published: 17 April 2021
(This article belongs to the Special Issue Parkinson’s Disease and Cognition)
Abstract
:Cognitive impairment risk in Parkinson’s disease increases with disease progression and poses a significant burden to the patients, their families and society. There are no disease-modifying therapies or preventative measures for Parkinson’s disease mild cognitive impairment (PD-MCI), or Parkinson’s disease dementia (PDD). This article reviews current and previously investigated treatments and those under investigation, including pharmacologic, non-pharmacologic and surgical procedures. There are currently no effective pharmacologic or non-pharmacologic treatments for PD-MCI. The only recommended treatment for PDD currently is rivastigmine, a cholinesterase inhibitor. Donepezil and galantamine—other cholinesterase inhibitors—are possibly useful. Memantine, a N-methyl-D-aspartate (NMDA) receptor antagonist, is considered investigational in PDD. Drug repurposing (atomoxetine, levodopa, insulin, atomoxetine for PD-MCI; ambroxol and ceftriaxone for PDD) and novel medications (SYN120, GRF6021, NYX-458 for PD-MCI; ANAVEX2-73, LY3154207, ENT-01, DAAOI-P for PDD) currently have insufficient evidence. There is growing research supporting exercise in the treatment of PD-MCI, but most non-pharmacological approaches have insufficient evidence for use in PD-MCI (cognitive rehabilitation, deep brain stimulation, transcranial direct current stimulation, transcranial ultrasound, vestibular nerve stimulation) and PDD (cognitive intervention, deep brain stimulation, transcranial alternating current stimulation, transcranial ultrasound, temporal blood brain barrier disruption). Research is needed for both disease-modifying and symptomatic treatments in PD cognitive impairment.
1. Introduction
Parkinson’s disease (PD) was historically classified as a movement disorder, but cognitive impairment is prevalent, especially later in the disease process. PD-related cognitive impairment is divided into two categories depending on severity and whether the level of cognitive impairment interferes with activities of daily living (ADLs). In PD mild cognitive impairment (PD-MCI), there is no impairment in ADLs. In PD dementia (PDD), ADLs are affected by cognition. The goal of this narrative review is to describe the therapeutic approaches studied for both PD-MCI and PDD, highlight the approaches recommended by the Movement Disorders Society, and provide a brief overview of therapies actively under investigation for treating cognitive symptoms in PD. To provide context for current and experimental approaches, we first briefly review the epidemiology and diagnosis of PD-MCI and PDD and the proposed mechanisms for cognitive impairment in PD.
1.1. Epidemiology and Clinical Significance
PD-MCI is present in 25–30% of persons with PD without dementia [1] and it increases the relative risk of dementia compared to those with PD without MCI (relative risk of 39.2 at 3 years) [2]. At 5 years, the risk of dementia is 6.5 times higher in individuals with PD-MCI, independent of sex, age, years of education and motor function [3]. Dementia is present in 24–31% of persons with PD [2,4]. The risk of dementia in persons with PD is 4 to 6 times higher than healthy individuals matched for age, sex, and education [5]. At least 75% of persons with PD who survive more than 10 years develop dementia [5]. PD-MCI and PDD are associated with decreased quality of life for persons with PD and caregivers and also increased nursing home admissions [6].
1.2. Diagnosis
Diagnoses of PD-MCI and PDD rely on the history provided by the patients and their caregivers, as well as cognitive testing. In contrast to Alzheimer’s disease (AD) dementia, the primary cognitive domains affected in PD are the executive, attentional and visuospatial domains [1]. The 2012 PD-MCI diagnostic criteria consist of level I (abbreviated) and level II (comprehensive) assessments [7]. For a diagnosis of PD-MCI, individuals must have a diagnosis of idiopathic PD, a gradual decline in cognitive abilities (noted by the patient, informant, or clinician), cognitive deficits upon testing, and preserved functional independence (with the exception of subtle difficulties with complex tasks). Level I assessment requires impairment on a scale of global cognition (e.g., the Montreal Cognitive Assessment (MoCA)) or at least two neuropsychological tests. Level II assessment requires full neuropsychological testing that includes all five cognitive domains, with impairment on two tests within one cognitive domain or on one test in two cognitive domains. The 2007 Movement Disorders Society PDD diagnostic criteria require a diagnosis of PD, the insidious onset and slow progression of a dementia syndrome (with impairment in more than one cognitive domain), decline from a premorbid level, and impaired ADLs beyond those attributed to motor and autonomic symptoms [8].
1.3. Risk Factors
The most consistently reported risk factors for PDD include more severe parkinsonism, increased age, and MCI [5], as well as other factors, including hallucinations, speech impairment, low level of education, depression and male sex [9]. Cognitive domains associated with higher risk of conversion from PD-MCI to PDD include poor baseline episodic memory, visuospatial function, semantic verbal fluency and cognitive flexibility [3].
1.4. Pathophysiology
The underlying mechanism of cognitive impairment in PD is not well understood and likely includes multiple factors. Proposed contributors include abnormal protein deposition, loss of dopaminergic neurons, neurotransmitter deficits, synaptic dysfunction, genetics [1], fatty acid oxidation [10], inflammation and oxidative stress [11,12,13], exosomal dysfunction [14], the gut microbiome and gut–brain axis involving the autonomic and enteric nervous systems [13], and prion-like aggregation of alpha-synuclein [13]. Many of these processes are also involved in other neurodegenerative diseases. The Braak hypothesis posits that aberrant alpha-synuclein starts in the gut and ascends via the vagus nerve to the brain, and that intraneuronal deposits made of α-synuclein fibrils (Lewy bodies) deposit in a caudal–cranial fashion, starting with the dorsal nucleus of the vagus and olfactory bulbs to the substantia nigra, then limbic, paralimbic and associative cortices [15]. The later stages are thought to cause cognitive dysfunctions in PD. Multiple abnormal proteins have been found in the postmortem brains of individuals with PD, including α-synuclein, tau and amyloid [11]. Individuals with PDD can have AD pathology, characterized by low CSF levels of amyloid β-42 (Aβ-42) and the cortical deposition of Aβ-42 in neuroimaging [11]. Individuals with dual PD and AD neuropathologies have more rapid disease progression (mean survival of 4.5 years, versus 10 years in those without AD neuropathology) [16]. This overlapping pathology presents as a diagnostic challenge in evaluating individuals with cognitive complaints. With regard to the gut microbiome, a significant alteration in gut bacterial species was found in individuals with PD-MCI as compared to PD with normal cognition and healthy controls [17]. Certain species correlated with worsening cognition.
Neurotransmitters implicated in cognitive changes and psychosis in PD include dopamine, serotonin, norepinephrine, acetylcholine, and N-methyl-D-aspartate (NMDA), prompting exploration of all of these targets for therapeutic drug development (Table 1). Additionally, several potential genetic risk factors have been identified for cognitive impairment in PD, including GBA (glucosylceremidase), MAPT (microtubule-associated protein tau), APOE (apolipoprotein E), LRRK2 (leucine-rich repeat serine/threonine-protein kinase 2), SNCA (α-synuclein), COMT (catechol-O-methyltransferase), BDNF (brain-derived neurotrophic factor), and various genes involved in inflammation/immune responses, such as IL10 (associated with lower risk of cognitive impairment), IL17A (associated with higher risk of cognitive impairment), IL18, and IFNG [1]. While the genetics associated with PD and PD cognitive impairment do not currently have treatment implications, precision medicine approaches applied to PD suggest that targeting specific genetics like GBA hold promise for future treatments [18].
2. Current Treatment and Therapies
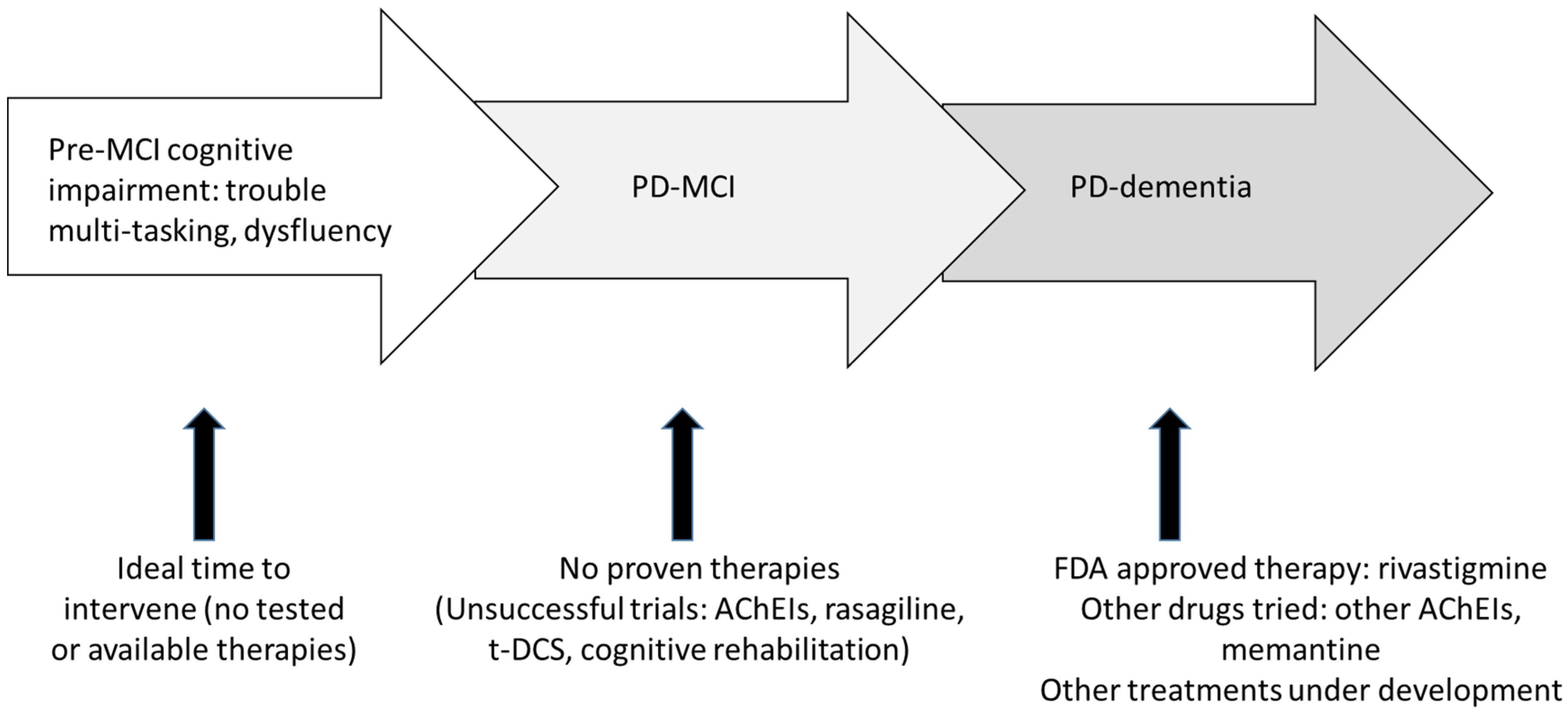
There are no current disease-modifying treatments for PD-MCI or PDD. There are no medications approved by the U.S. Food and Drugs Administration (FDA) or European Medicines Agency (EMA) for PD-MCI. Rivastigmine is the only FDA- and EMA-approved medication for PDD (Figure 1). Current treatments for PD-related cognitive impairment primarily focus on symptom management, such as treating mood disorders, behavioral disturbance, sleep disorder, and lifestyle modification to improve quality of life (e.g., physical activities, healthy diet and social engagement). While PD is more common in men than women, there currently exist no differences in treatment approaches in men and women with PD. Table 2 summarizes current pharmacologic treatments based on clinical evidence.
Treating cognitive changes in PD starts with an assessment for potentially reversible contributors to cognitive changes. Major pharmacologic culprits are anticholinergic medications (e.g., antihistamines, antispasmodics), benzodiazepines, and opioids (Table 3). Medications used to treat motor symptoms in PD can also contribute to cognitive symptoms. In the context of cognitive complaints, the general order in which PD medications are discontinued is as follows: anticholinergics, MAO-B inhibitors, amantadine, dopamine agonists, and COMT inhibitors, followed by reduced levodopa [19]. Laboratory assessment for contributors to cognitive impairment commonly includes a complete blood count, serum electrolytes, glucose, blood urea nitrogen/creatinine, folate, B12, and thyroid function testing [20]. Addressing depression and hearing loss are also part of a comprehensive approach to addressing cognitive impairment.
2.1. Studied Treatments for Parkinson’s Disease—Mild Cognitive Impairment
2.1.1. Pharmacologic Treatments for Parkinson’s Disease—Mild Cognitive Impairment
Research investigated the effects of four medications and two supplements for the treatment of PD-MCI, but no agent has consistently positive results. The transdermal (patch) form of rivastigmine, a cholinesterase inhibitor (4.6–9.5 mg/24h), had no statistically significant benefits in a 24-week randomized controlled trial (RCT) enrolling 28 individuals with PD-MCI [21]. The endpoints included the Alzheimer’s Disease Assessment Scale-clinicians’ global impression of change scales (ADCS-CGIC), the MoCA, NeuroTrax computerized cognitive testing, Dementia Rating Scale-2 (DRS-2), and the Gordon Diagnostics System. An initial RCT (n = 48) of rasagiline (1 mg daily), a monoamine oxidase B inhibitor, demonstrated significant improvement in digit span and verbal fluency tasks at 12 weeks in the rasagiline group [22]. However, a subsequent RCT (n = 151) showed no significant between-group differences in Change in Scales for Outcomes of Parkinson’s Disease-Cognition, MoCA, Penn Daily Activities Questionnaire, or ADCS-CGIC (MCI) scores at 24 weeks [23]. Clinicaltrials.gov lists a third study aiming to evaluate rasagiline’s effect on cognition in PD-MCI (NCT01497652, n = 34), but the study finished in 2015 and no results were published.
Researchers assessed atomoxetine, a selective norepinephrine reuptake inhibitor commonly used in attention deficit hyperactive disorder, in multiple studies of individuals with PD. In a small (n = 12) open-label, uncontrolled, flexible dose study involving individuals with PD and executive dysfunction without dementia (MMSE ≤ 25), atomoxetine (25–100 mg/day) improved executive function on the CGIC scale, Frontal Systems Behavior Scale (FrSBE), and Connors Adult Attention-Deficit/Hyperactivity Disorder Rating Scale (CAARS), a subjective measure of impulsivity and attention, at 8 weeks [24]. An RCT involving individuals with PD-MCI (n = 30), atomoxetine (80 mg/day) showed no difference between the treatment and control groups in the primary cognitive outcome, a composite score based on a battery of standardized executive function tests, but the atomoxetine group had significant improvement on CAARS [25]. In an RCT (n = 55) of atomoxetine for the treatment of depression in individuals with PD and a MMSE >14, those who received atomoxetine (target dose 80 mg/day) had a greater mean change in MMSE at 8 weeks compared to the placebo group (1.31, p = 0.003) [26]. A meta-analysis of these three studies concluded that atomoxetine improved global cognition (statistically significant large effect size), but changes in other categories (e.g., complex attention, executive function) were non-significant [27]. An RCT (n = 30) evaluating atomoxetine’s effect on cognition in PD-MCI was completed but no results were published (NCT01738191; last accessed on 17 January 2021).
Creatine and coenzyme Q10 are important substrates involved in energy conversion in the mitochondria and have an indirect antioxidant effect. A Chinese study (n = 75) found that creatine (5 g twice a day) and coenzyme Q10 (100 mg three times per day) improved MoCA scores in PD-MCI after 12 and 18 months [28]. The study did not adjust for baseline MoCA performance, however, and larger scale follow up studies have not been done to date.
2.1.2. Non-Pharmacologic Treatments for Parkinson’s Disease—Mild Cognitive Impairment
Cognitive Interventions
Cognitive interventions are divided into three types: cognitive stimulation, cognitive training, and cognitive rehabilitation [29]. Cognitive stimulation consists of non-specific stimulation of cognitive and social functioning. Cognitive training uses standardized cognitive tasks on the computer or on paper. Cognitive rehabilitation targets specific areas of difficulty in activities of daily living to improve function. A recent Cochrane systemic review evaluated seven RCTs on cognitive training for PD-MCI and PDD [29]. Four of the studies targeted persons with PD-MCI, two targeted individuals with PD without dementia (PD-MCI + PD-normal cognition), and one study included persons with PDD. Interventions varied from tailored exercises that stimulated executive function, attention, shifting ability, visuospatial function, multi-domain online computer-based training over 4–8 weeks. The review concluded that there was no significant improvement in global cognition with the investigated approaches. One RCT in the systematic review (n = 70) investigated a structured cognitive training program NEUROvitalis that focused on the cognitive domains frequently impaired in PD (attention, memory, executive functions). The study compared the treatment to unstructured training (“Mentally fit,” no specific targeted cognitive domains) and to a non-intervention control group. NEUROvitalis improved short-term memory and working memory in individuals with PD without dementia (MMSE ≥25), compared to the control group after 6 weeks (p < 0.01 and p < 0.05, respectively) [30]. Forty-seven individuals from the same study were reexamined at 1 year, and both the structured (NEUROvitalis) and non-structured (Mentally fit) cognitive training programs for 6 weeks improved overall cognitive function (MMSE and DemTect). The MCI risk was higher in the control group versus treatment groups (40.0%, versus 18.2% in NEUROvitalis and Mentally Fit, respectively) [31]. Other studies are underway, including an RCT that evaluates the effect of cognitive rehabilitation compared to standard supportive care (NCT03335150) and an RCT for targeted intervention strategy on prospective memory (NCT01469741) in PD-MCI and PD-normal cognition. Other studies in persons with PD-MCI without published data include the following: computer-based cognitive training (NCT02225314), neurocognitive and supportive therapy (NCT01646333), cognitive behavioral therapy (NCT02048605), and cognitive training (NCT04474379, NCT03582670).
Exercise and Physical Therapy
Different types of physical exercises have been evaluated for their effects on cognition, including treadmill training, dance, stationary bicycle, Wii Fit, and Tai chi. A systematic review of RCTs on the effects of physical exercise on cognition in PD (those with normal cognition and PD-MCI) showed that physical exercise improved global cognition, processing speed, attention and mental flexibility. Treadmill use 3 times per week for 60 min improved cognition with the most significance [32]. In persons with mild to moderate PD and a MMSE >24, treadmill walking (45 min, 3 days per week for 3 weeks) significantly improved executive function (measured by the Frontal Assessment Battery, trail-making and memory interference test) [33]. However, MoCA scores did not differ between the intervention and control groups. One RCT (n = 76) evaluated the effects of aerobic exercise (recumbent bicycle) and goal-based exercises (walking, muscle toning, and stretching exercises) for 60 min per session, 3 times per week for 12 weeks, compared to age-matched controls in individuals with PD with normal cognition and those with PD-MCI [34]. In both the cognitively normal and MCI groups, aerobic exercise improved executive function (Stroop test) compared to the goal-based group, but not better than the control group. In persons with PD-MCI, the aerobic group outperformed the control and goal-based groups on the trail-making test (a test of executive function and processing speed). There were no differences between groups in memory and language. A meta-analysis in Tai chi and Qigong exercises in PD, including two studies that assessed cognition, found that they improved most motor function, depression and quality of life, but not cognition [35]. Notably, study populations were heterogeneous, including persons with PD with normal cognition and PD-MCI. Two RCTs assessed Argentine tango dancing on cognition. One study (n = 33) showed that tango (90 min per session, 20 sessions over 12 weeks) improved spatial cognition (measured by Brook’s spatial task) in persons with PD without dementia (baseline MoCA > 24), but there was no difference in global cognition (measured by MoCA) between the treatment and control groups [36]. Another RCT (n = 33) found that tango (60 min per session, twice a week for 12 weeks) did not improve global cognition (measured by MoCA) in persons with PD without dementia compared to the home exercise control group [37]. A current RCT is investigating the effect of Rock Steady Boxing (versus sensory attention focused exercise) on motor and cognitive outcome in persons with idiopathic PD (NCT03618901).
An RCT (n = 40) found that intensive physical therapy (60 min per session, 6 times per week for 4 weeks, including aerobic exercises, treadmill training and exercise intervention program) improved global cognition (measured by MoCA) and attention/working memory (verbal and digit span) in persons with PD-MCI [38]. Other clinical trials are investigating the effects of certain types of exercise on cognition in persons with PD-MCI (NCT02267785) and some are utilizing home-based physical therapy (NCT02248649). A clinical trial is evaluating the roles of the supplement carnosine and physical exercise on working memory and motor functions in persons with MCI, early-stage PD, and subjective cognitive impairment (NCT03330470).
In summary, physical exercise shows some benefit on cognition in individuals with PD and normal cognition and those with PD-MCI, but the effects vary by exercise types. Aerobic exercises such as treadmill, recumbent bicycle, and tango most consistently improve executive function in the identified studies, but the effects on global cognition and other cognitive domains vary. Intensive physical therapy may improve global cognition, attention/working memory in persons with PD-MCI.
Device-Related Interventions
Transcranial magnetic stimulation (TMS) has been studied in PD for the treatment of motor, mood and cognitive symptoms. There is no definitive evidence for repetitive TMS (rTMS) in improving cognition in PD-associated cognitive impairment. One study showed that repeated intermittent “theta burst” stimulation of the left dorsolateral prefrontal cortex (DLPFC) improved cognition and visuospatial function lasting up to 1 month in persons with PD-MCI [39]. However, another study (n = 46) found that stimulation of the bilateral DLPFC did not improve overall cognition (primary outcome: DRS-2) or Clinical Global Impression of Improvement in persons with PD-MCI compared to the control group [40]. Clinical trials are ongoing to assess rTMS stimulation of bilateral (NCT02346708) and left DLPFC in PD-MCI (NCT03836950).
Transcranial direct current stimulation (tDCS) over the prefrontal cortex improved executive function, as measured in trail-making tasks, but not others (e.g., Stroop test, Wisconsin Card Sorting Test) in individuals with PD without dementia [41]. An RCT (n = 22) showed that the combination of cognitive training and transcranial direct current stimulation (tDCS) to the left DLPFC in individuals with PD-MCI (5 days/week for 2 weeks) improved phonemic verbal fluency compared to cognitive training alone, and this effect persisted at 3 months. However, there were no between-group differences in other primary outcome measures in language, attention, and executive functions [42]. Another RCT (n = 24) in individuals with PD-MCI showed that the combination of tDCS over the left DLPFC and cognitive training for 4 weeks did not improve memory and cognition at 16 weeks [43]. One RCT (n = 42) showed that cognitive training (45 min, 3 times per week for 4 weeks) and tDCS of the left DLPFC (20 min, once per week for 4 weeks) in isolation or combined both improved various cognitive and functional outcomes at 5 and 12 weeks, and combined interventions had greater effects [44]. The standard cognitive training group improved on memory, ADLs and quality of life. The tailored cognitive training group improved on attention/working memory and quality of life. The tDCS group improved on attention/working memory and memory. The standard cognitive training + tDCS group improved on executive function, attention/working memory and ADLs. The tailored cognitive training + tDCS group improved on executive function, attention/working memory and memory. Other clinical trials are ongoing to evaluate the effect of tDCS on cognition in PD-MCI (NCT03191916, NCT04171804) and individuals with PD without dementia (NCT03025334). Combination therapies in persons with PD-MCI, such as cognitive training with tDCS, have been heterogeneous and have shown mixed results [42,43,44]. An RCT (n = 20) showed that tDCS over the medial frontal cortex improved the Theory of Mind, the ability to understand and predict others’ behaviors in individuals with PD-MCI [45]. Pathologic oscillatory activities exist in the thalamo-cortical region in PD, thus transcranial alternating current stimulation (tACS) was investigated for potential disease modulation. An RCT (n = 15) using personalized transcranial alternating current stimulation, or tACS (location of stimulation was individually defined based on EEG data) 5 days/week for 2 weeks, did not show significant cognitive benefit in persons with PD with MMSE ≥ 23 [46].
Ongoing research is evaluating the role of vestibular nerve stimulation (NCT04450550), transcranial ultrasound (NCT04250376), and deep brain stimulation (DBS) of the globus pallidus interna (GPi) and the nucleus basalis of Meynert (NBM) (NCT04571112) or NBM alone (NCT02924194) in individuals with PD without dementia.
2.1.3. Clinical Treatment Approaches for PD-MCI
The 2019 Movement Disorders Society update on evidence-based treatments for non-motor symptoms of PD concluded that there is currently insufficient evidence to support any pharmacologic (rivastigmine, rasagiline) or non-pharmacologic (transcranial direct-current stimulation, cognitive rehabilitation) treatment for non-dementia cognitive impairment in PD. All reviewed approaches were labeled investigational [47]. However, research suggests that there may be a role for physical exercise and therapy in targeting cognitive outcomes in populations with PD without dementia [32]. Aerobic exercise (treadmill and recumbent bicycle) improved executive function in PD-MCI, while intensive physical therapy improved global cognition. More research is needed to identify pharmacologic and non-pharmacologic strategies for targeting PD-MCI, as well as combination approaches. In the meantime, particularly given the increasing research showing the benefits of exercise on PD more generally, it is reasonable for clinicians to recommend exercise as a strategy to target early cognitive changes in PD.
2.2. Studied Treatments for Parkinson’s Disease Dementia
2.2.1. Pharmacologic Treatments for Parkinson’s Disease Dementia
Cholinesterase inhibitors are the most frequently studied medications for PDD. Rivastigmine is the only cholinesterase inhibitor that is approved by the FDA for use in PDD. It is also approved for such use by the EMA, Canada and Japan. In an RCT of rivastigmine (3–12 mg) in individuals with mild-to-moderate PDD (n = 410), rivastigmine improved cognition (measured by ADAS-cog, MMSE, and Delis–Kaplan Executive Function System (D-KEFS) verbal fluency and ten-point clock drawing) as well as global function (ADCS-CGIC and ADCS-ADL) [48]. In a 76-week, open-label randomized study of rivastigmine capsule and patch formulations in individuals with mild-to-moderate PDD (n = 583), individuals receiving rivastigmine capsules had significantly better Mattis Dementia Rating Scale scores (weeks 24–76) and better ADCS-ADL scores at weeks 52 and 76 [49]. There were no differences in efficacy between the capsule and patch in persons with MMSE > 21, but individuals with lower MMSE scores benefited more from the capsules [49].
Donepezil showed conflicting results in PDD studies. An RCT (n = 16) found that donepezil 2.5–10 mg/day improved memory in persons with PD-MCI and PDD on the Dementia Rating Scale (DRS) but resulted in no significant changes in global cognitive status, attention, executive function, memory or visuospatial functions [50]. Another RCT (n = 22) showed that donepezil 2 to 10 mg/day for 10 weeks improved performance on the MMSE but not on the Mattis Dementia Rating Scale or ADAS-cog [51]. The EDON study (n = 550) found that donepezil 5 or 10 mg for 24 weeks did not improve its primary endpoints, ADAS-cog and Clinician’s Interview-based Impression of Change plus caregiver input (CIBIC+). After removing the treatment-by-country interaction from the model, 10 mg donepezil had a dose-dependent benefit in the CIBIC+ scores. Both 5 mg and 10 mg doses improved secondary endpoints: MMSE, D-KEFS, and Brief Test of Attention [52]. Galantamine (8 mg twice daily) was assessed in a single-open label study (n = 41). Participants reported improvements on the MMSE, ADAS-cog, clock drawing test, and Frontal Assessment Battery [53].
Memantine is an NMDA receptor antagonist considered investigational for use in PDD [47]. A metanalysis included three studies: one RCT specifically for PDD, and two for mixed dementia with Lewy bodies (DLB) and PDD [54]. There were no significant differences in the ADCS-CGIC scores in the memantine-treated group (20 mg/day) versus the control group for up to 24 weeks. One study showed improved attention and episodic memory in PDD [55].
2.2.2. Non-Pharmacologic Treatments for Parkinson’ Disease Dementia
Studies on the effects of non-pharmacologic approaches on cognition in individuals with PDD are scarce. One systemic review that examined the effect of exercise in Lewy body dementia (LBD) included five studies and only three included individuals with PDD (total of 10 individuals with PDD) [56].
Deep brain stimulation (DBS): An RCT (n = 6) evaluating bilateral NBM DBS in persons with PDD found no differences in the primary cognitive outcomes (California Verbal Learning Test, WAIS-III digit span, verbal fluency, Posner covert attention test, and simple and choice reaction times) between the treatment and control groups after 6 weeks [57]. Other RCTs are ongoing to evaluate subthalamic nucleus (STN) and NBM stimulation in treating motor and cognitive symptoms in PDD (NCT02589925). Other non-pharmacologic treatments being studied for PDD include transcranial ultrasound (NCT04250376) and temporary blood brain barrier (BBB) disruption using non-invasive ultrasound (NCT03608553).
2.2.3. Clinical Treatment Approaches for Parkinson’s Disease Dementia
The 2019 Movement Disorders Society update on evidence-based treatments for non-motor symptoms of PD concluded that there is only sufficient evidence to support rivastigmine as efficacious for PD dementia. There is insufficient evidence of the efficacy of donepezil, galantamine, or memantine. The update identified rivastigmine as clinically useful. The other cholinesterase inhibitors were classified as possibly useful, given their antidementia benefit outside PD. Memantine was labeled as investigational [47]. Research on non-pharmacologic approaches for PDD are lacking and there is insufficient evidence to support the use of non-pharmacological procedures (DBS, tACS) for PDD.
2.3. Treatments for Non-Cognitive Symptoms
A plethora of non-cognitive symptoms can manifest in PD-MCI and PDD, including fatigue, depression, anxiety, apathy, psychosis, REM sleep behavioral disorder, insomnia, and impulse control disorder. Treatments for these symptoms are a key part of management of cognitive impairment in PD but are beyond the scope of this review. Clinicians should screen for non-motor symptoms accompanying cognitive impairment in PD and treat them with pharmacologic and non-pharmacologic strategies, as needed.
3. Developing Research
In addition to aforementioned therapies in PD-MCI and PDD, studies are investigating treatments for cognitive impairment and dementia related to PD using various approaches, including (1) drug repurposing, (2) novel medications and (3) non-pharmacologic interventions. Clinical trials in pharmacologic and non-pharmacologic treatments are summarized in Table 4 and Table 5, respectively.
3.1. Drug Repurposing
Researchers are repurposing multiple pharmacologic agents for potential use in PD cognitive impairment. Ambroxol is an over-the-counter expectorant that is a pharmacological chaperone of B-glucocerebrosidase (GCase), coded by the gene GBA1. GBA1 mutations are a strong risk factor for PDD [58]. Ambroxol showed promise in mouse models and is being studied in a phase 2 RCT for persons with mild to moderate PDD (NCT02914366) [58]. Ceftriaxone, a third-generation cephalosporin antibiotic, is being studied in a phase 2 RCT in PDD given its potential neuroprotective effect by reducing glutamatergic hyperactivity and excitotoxicity (NCT03413384). Nilotinib is a tyrosine kinase Abelson inhibitor used to treat chronic myeloid leukemia, but it also increases dopamine levels. After a small proof-of-concept trial (n = 12) [59], a phase 2 RCT in persons with PD-MCI (MoCA score ≥ 22) found that nilotinib did not improve MoCA scores in the 150 mg group and significantly worsened in the 300 mg treatment group [60]. Intranasal insulin was previously shown to improve visuospatial and verbal working memory in persons with MCI and Alzheimer’s disease [61,62]. A proof-of-concept RCT (n = 16) in individuals with PD without dementia found that daily intranasal insulin (40 international units) improved letter fluency and Hoehn and Yahr scores but not MoCA scores [63]. No other neuropsychological assessment was performed outside of letter fluency.
One study evaluated the effects of atomoxetine (10–30 mg twice a day) and rivastigmine (1.5–4.5 mg twice a day) on attention in persons with PD without dementia (NCT01340885, n = 9). Results are not yet published.
3.2. Novel Medications
SYN120, a dual serotonin 5-HT6/5-HT2A antagonist, did not improve cognition (measured by Computerized Drug Research Cognition Battery, CDR episodic memory and ADAS-Cog) in persons with PDD compared to the placebo after 16 weeks in a proof-of-concept RCT (SYNAPSE trial; NCT02258152; n = 82) [64]. ANAVEX2-73 (Blarcamesine), an agonist of the intracellular sigma-1 chaperone protein, is in a phase 2 RCT in individuals with PDD (NCT03774459) as well as an open-label extension to evaluate for its safety and efficacy of daily treatment (NCT04575259). LY3154207 (mevidalen), a dopamine receptor D1 enhancer, is in a phase 2 trial to evaluate its effect on cognition in mild-to-moderate dementia due to LBD associated with idiopathic PD and DLB (NCT03305809). RO7046015/PRX002 (Prasinezumab) is an anti-α-synuclein monoclonal antibody (mAb) whose precursor reduced α-synuclein accumulation and improved cognition in animal models of PD [65]. Studies showed that intravenous PRX002 was safe in healthy adults [65] and in persons with mild to moderate idiopathic PD [66]. A trial is investigating its efficacy in early PD (primary outcome: change in UPDRS; secondary outcome includes change in MoCA score; NCT03100149). ENT-01 is in a phase 1 RCT to assess its effect on cognition in PDD (NCT03938922). GRF6021 is a plasma derivative being investigated for its safety and tolerability in persons with PD-MCI in a phase 2 RCT (NCT03713957). NMDA receptor modulators, NYX-458 and D-amino acid oxidase (DAAO) inhibitor (DAAOI-P), are under investigation for PD-MCI (NCT04148391) and PDD (NCT04470037).
3.3. Non-Pharmacologic Interventions
Active clinical trials for non-pharmacologic interventions for PD-MCI and PDD are reviewed in Section 2.1.2 and Section 2.2.2, respectively.
3.4. Challenges to Study Design in PD Cognitive Impairment
There are numerous challenges to clinical trials for individuals with PD and cognitive impairment. First, robust understanding of pathophysiologic mechanisms to guide intervention development is lacking. It is also possible that effective therapy will need to employ more than one type of treatment, such as combined pharmacologic cognitive interventions and exercise. From the perspective of study design, current studies sometimes mix populations (e.g., PD-MCI plus PD with normal cognition). It remains uncertain how best to identify populations for particular studies, such as whether to study PD without dementia (normal cognition and PD-MCI), PD with cognitive impairment (PD-MCI plus PDD), or the conditions separately. There are also debates regarding whether individuals with PDD should be combined with individuals with dementia with Lewy bodies for trials, as they both fall under the umbrella of Lewy body dementia [67]. Cognitive impairment in PD is a spectrum and how PD-MCI and PDD are operationalized for study design may affect results. Other aspects of PD cognitive impairment need also to be considered in trial design, such as whether researchers need to account for the presence or absence of concomitant AD pathology [67]. Features of PDD, such as fluctuations, can also negatively affect accurate clinical trial measurements, and study participation requirements (e.g., travel, study visit frequency) can affect trial enrollment, retention, and outcomes [67]. Finally, most measures used in studies of cognitive impairment in PD need further research to assess the validity, reliability, and clinically meaningful change of these measures when used in populations with PD and cognitive impairment [68].
4. Conclusions and Future Directions
Despite tremendous research efforts focused on PD-related cognitive impairment, current options are limited. When treating individuals with PD-MCI, clinicians should counsel patients regarding the absence of established pharmacologic therapies. Emerging research regarding the potential benefits of exercise in PD-MCI—in addition to research showing the benefits of exercise in PD more generally—suggest that clinicians should recommend exercise, especially the aerobic type, for individuals with PD and cognitive impairment. For individuals with PDD, rivastigmine is the only currently FDA-approved treatment for PDD, though other cholinesterase inhibitors are also sometimes used clinically. Memantine is labeled as investigational by the Movement Disorders Society Evidence Review, but is sometimes also tried in clinical practice. Current research approaches include both drug repurposing and identifying drugs with novel mechanisms of action. Additional non-pharmacological intervention studies are also needed, especially for PD dementia, where such research is particularly lacking.
Author Contributions
Writing—original draft preparation, C.S.; writing—review and editing, C.S. and M.J.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available in this article.
Conflicts of Interest
M.J.A. receives research support from the NIA (R01AG068128, P30AG047266), the Florida Department of Health (grant 20A08), and as the local PI of the Lewy Body Dementia Association Research Center of Excellence. She receives royalties from the publication of the book Parkinson’s Disease: Improving Patient Care and she has received honoraria for presenting at AAN and International Parkinson and Movement Disorder Society annual meetings. C.S. declares no conflicts of interest.
Abbreviations
| AD | Alzheimer’s disease |
| ADAS-cog | Alzheimer’s Disease Assessment Scale-Cognitive Subscale |
| ADCS-CGIC | Alzheimer’s Disease Assessment Scale-clinicians’ global impression of change scales |
| ADLs | Activities of daily living |
| DCS-ADL | Alzheimer’s Disease Assessment Scale-Activities of Daily Living scales |
| COMT | catechol-O-methyltransferase |
| DAD | disability assessment for dementia |
| D-KEFS | The Delis-Kaplan Executive Function System |
| MAO | monoamine oxidase |
| MMSE | Mini-Mental Status Exam |
| MoCA | Montreal Cognitive Assessment |
| NPI-10 | Neuropsychiatric Inventory-10 |
| PC-MCI | Parkinson’s disease mild cognitive impairment |
| PD | Parkinson’s disease |
| PDD | Parkinson’s dementia |
| SNc | substantia nigra pars compacta |
| STN | subthalamic nucleus |
| WAIS | Wechsler Adult Intelligence Scale |
References
- Aarsland, D.; Creese, B.; Politis, M.; Chaudhuri, K.R.; Ffytche, D.H.; Weintraub, D.; Ballard, C. Cognitive decline in parkinson disease. Nat. Rev. Neurol. 2017, 13, 217–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, K.F.; Larsen, J.P.; Tysnes, O.B.; Alves, G. Prognosis of mild cognitive impairment in early parkinson disease: The norwegian parkwest study. JAMA Neurol. 2013, 70, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Domellöf, M.E.; Ekman, U.; Forsgren, L.; Elgh, E. Cognitive function in the early phase of parkinson’s disease, a five-year follow-up. Acta. Neurol. Scand. 2015, 132, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Aarsland, D.; Zaccai, J.; Brayne, C. A systematic review of prevalence studies of dementia in parkinson’s disease. Mov. Disord. 2005, 20, 1255–1263. [Google Scholar] [CrossRef] [PubMed]
- Aarsland, D.; Kurz, M.W. The epidemiology of dementia associated with parkinson disease. J. Neurol. Sci. 2010, 289, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Emre, M. Dementia associated with parkinson’s disease. Lancet Neurol. 2003, 2, 229–237. [Google Scholar] [CrossRef]
- Litvan, I.; Goldman, J.G.; Troster, A.I.; Schmand, B.A.; Weintraub, D.; Petersen, R.C.; Mollenhauer, B.; Adler, C.H.; Marder, K.; Williams-Gray, C.H.; et al. Diagnostic criteria for mild cognitive impairment in parkinson’s disease: Movement disorder society task force guidelines. Mov. Disord. 2012, 27, 349–356. [Google Scholar] [CrossRef] [Green Version]
- Emre, M.; Aarsland, D.; Brown, R.; Burn, D.J.; Duyckaerts, C.; Mizuno, Y.; Broe, G.A.; Cummings, J.; Dickson, D.W.; Gauthier, S.; et al. Clinical diagnostic criteria for dementia associated with parkinson’s disease. Mov. Disord. 2007, 22, 1689–1707, quiz 1837. [Google Scholar] [CrossRef]
- Marinus, J.; Zhu, K.; Marras, C.; Aarsland, D.; van Hilten, J.J. Risk factors for non-motor symptoms in parkinson’s disease. Lancet Neurol. 2018, 17, 559–568. [Google Scholar] [CrossRef]
- Burté, F.; Houghton, D.; Lowes, H.; Pyle, A.; Nesbitt, S.; Yarnall, A.; Yu-Wai-Man, P.; Burn, D.J.; Santibanez-Koref, M.; Hudson, G. Metabolic profiling of parkinson’s disease and mild cognitive impairment. Mov. Disord. 2017, 32, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Brandão, P.R.P.; Munhoz, R.P.; Grippe, T.C.; Cardoso, F.E.C.; de Almeida, E.C.B.M.; Titze-de-Almeida, R.; Tomaz, C.; Tavares, M.C.H. Cognitive impairment in parkinson’s disease: A clinical and pathophysiological overview. J. Neurol. Sci. 2020, 419, 117177. [Google Scholar] [CrossRef]
- Pessoa Rocha, N.; Reis, H.J.; Vanden Berghe, P.; Cirillo, C. Depression and cognitive impairment in parkinson’s disease: A role for inflammation and immunomodulation? Neuroimmunomodulation 2014, 21, 88–94. [Google Scholar] [CrossRef]
- Nair, A.T.; Ramachandran, V.; Joghee, N.M.; Antony, S.; Ramalingam, G. Gut microbiota dysfunction as reliable non-invasive early diagnostic biomarkers in the pathophysiology of parkinson’s disease: A critical review. J. Neurogastroenterol. Motil. 2018, 24, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Sun, T.; An, J.; Wen, L.; Liu, F.; Bu, Z.; Cui, Y.; Feng, J. Potential roles of exosomes in parkinson’s disease: From pathogenesis, diagnosis, and treatment to prognosis. Front. Cell Dev. Biol. 2020, 8, 86. [Google Scholar] [CrossRef] [Green Version]
- Braak, H.; Del Tredici, K.; Bratzke, H.; Hamm-Clement, J.; Sandmann-Keil, D.; Rüb, U. Staging of the intracerebral inclusion body pathology associated with idiopathic parkinson’s disease (preclinical and clinical stages). J. Neurol. 2002, 249 (Suppl. 3), Iii/1-5. [Google Scholar] [CrossRef] [PubMed]
- Jellinger, K.A.; Seppi, K.; Wenning, G.K.; Poewe, W. Impact of coexistent alzheimer pathology on the natural history of parkinson’s disease. J. Neural Transm. (Vienna) 2002, 109, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Ren, T.; Gao, Y.; Qiu, Y.; Jiang, S.; Zhang, Q.; Zhang, J.; Wang, L.; Zhang, Y.; Nie, K. Gut microbiota altered in mild cognitive impairment compared with normal cognition in sporadic parkinson’s disease. Front. Neurol. 2020, 11, 137. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.A.; Alcalay, R.N. Precision medicine in parkinson’s disease: Emerging treatments for genetic parkinson’s disease. J. Neurol. 2020, 267, 860–869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, J.H.; Factor, S.A. Atypical antipsychotics in the treatment of drug-induced psychosis in parkinson’s disease. Mov. Disord. 2000, 15, 201–211. [Google Scholar] [CrossRef]
- Knopman, D.S.; DeKosky, S.T.; Cummings, J.L.; Chui, H.; Corey-Bloom, J.; Relkin, N.; Small, G.W.; Miller, B.; Stevens, J.C. Practice parameter: Diagnosis of dementia (an evidence-based review). Report of the quality standards subcommittee of the american academy of neurology. Neurology 2001, 56, 1143–1153. [Google Scholar] [CrossRef] [Green Version]
- Mamikonyan, E.; Xie, S.X.; Melvin, E.; Weintraub, D. Rivastigmine for mild cognitive impairment in parkinson disease: A placebo-controlled study. Mov. Disord. 2015, 30, 912–918. [Google Scholar] [CrossRef]
- Hanagasi, H.A.; Gurvit, H.; Unsalan, P.; Horozoglu, H.; Tuncer, N.; Feyzioglu, A.; Gunal, D.I.; Yener, G.G.; Cakmur, R.; Sahin, H.A.; et al. The effects of rasagiline on cognitive deficits in parkinson’s disease patients without dementia: A randomized, double-blind, placebo-controlled, multicenter study. Mov. Disord. 2011, 26, 1851–1858. [Google Scholar] [CrossRef]
- Weintraub, D.; Hauser, R.A.; Elm, J.J.; Pagan, F.; Davis, M.D.; Choudhry, A. Rasagiline for mild cognitive impairment in parkinson’s disease: A placebo-controlled trial. Mov. Disord. 2016, 31, 709–714. [Google Scholar] [CrossRef]
- Marsh, L.; Biglan, K.; Gerstenhaber, M.; Williams, J.R. Atomoxetine for the treatment of executive dysfunction in parkinson’s disease: A pilot open-label study. Mov. Disord. 2009, 24, 277–282. [Google Scholar] [CrossRef] [Green Version]
- Hinson, V.K.; Delambo, A.; Elm, J.; Turner, T. A randomized clinical trial of atomoxetine for mild cognitive impairment in parkinson’s disease. Mov. Disord. Clin. Pract. 2017, 4, 416–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weintraub, D.; Mavandadi, S.; Mamikonyan, E.; Siderowf, A.D.; Duda, J.E.; Hurtig, H.I.; Colcher, A.; Horn, S.S.; Nazem, S.; Ten Have, T.R.; et al. Atomoxetine for depression and other neuropsychiatric symptoms in parkinson disease. Neurology 2010, 75, 448–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, A.; Das, S.; Behera, S.K.; Ramakrishnan, K.; Selvarajan, S.; Kandasamy, P.; Nair, N.S. Atomoxetine does not improve complex attention in idiopathic parkinson’s disease patients with cognitive deficits: A meta-analysis. Parkinsons Dis. 2020, 2020, 4853590. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wang, P.; Yu, Z.; Cong, Y.; Sun, H.; Zhang, J.; Sun, C.; Zhang, Y.; Ju, X. The effect of creatine and coenzyme q10 combination therapy on mild cognitive impairment in parkinson’s disease. Eur. Neurol. 2015, 73, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Orgeta, V.; McDonald, K.R.; Poliakoff, E.; Hindle, J.V.; Clare, L.; Leroi, I. Cognitive training interventions for dementia and mild cognitive impairment in parkinson’s disease. Cochrane Database Syst. Rev. 2020, 2, Cd011961. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, A.; Kaesberg, S.; Barbe, M.T.; Timmermann, L.; Fink, G.R.; Kessler, J.; Kalbe, E. Effects of cognitive training in parkinson’s disease: A randomized controlled trial. Parkinsonism Relat. Disord. 2014, 20, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, A.; Kaesberg, S.; Barbe, M.T.; Timmermann, L.; Rosen, J.B.; Fink, G.R.; Kessler, J.; Kalbe, E. Cognitive training in parkinson’s disease reduces cognitive decline in the long term. Eur. J. Neurol. 2015, 22, 640–647. [Google Scholar] [CrossRef]
- da Silva, F.C.; Iop, R.D.R.; de Oliveira, L.C.; Boll, A.M.; de Alvarenga, J.G.S.; Gutierres Filho, P.J.B.; de Melo, L.; Xavier, A.J.; da Silva, R. Effects of physical exercise programs on cognitive function in parkinson’s disease patients: A systematic review of randomized controlled trials of the last 10 years. PLoS ONE 2018, 13, e0193113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picelli, A.; Varalta, V.; Melotti, C.; Zatezalo, V.; Fonte, C.; Amato, S.; Saltuari, L.; Santamato, A.; Fiore, P.; Smania, N. Effects of treadmill training on cognitive and motor features of patients with mild to moderate parkinson’s disease: A pilot, single-blind, randomized controlled trial. Funct. Neurol. 2016, 31, 25–31. [Google Scholar] [PubMed]
- Silveira, C.R.A.; Roy, E.A.; Intzandt, B.N.; Almeida, Q.J. Aerobic exercise is more effective than goal-based exercise for the treatment of cognition in parkinson’s disease. Brain Cogn. 2018, 122, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Song, R.; Grabowska, W.; Park, M.; Osypiuk, K.; Vergara-Diaz, G.P.; Bonato, P.; Hausdorff, J.M.; Fox, M.; Sudarsky, L.R.; Macklin, E.; et al. The impact of tai chi and qigong mind-body exercises on motor and non-motor function and quality of life in parkinson’s disease: A systematic review and meta-analysis. Parkinsonism Relat. Disord. 2017, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- McKee, K.E.; Hackney, M.E. The effects of adapted tango on spatial cognition and disease severity in parkinson’s disease. J. Mot. Behav. 2013, 45, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Rios Romenets, S.; Anang, J.; Fereshtehnejad, S.M.; Pelletier, A.; Postuma, R. Tango for treatment of motor and non-motor manifestations in parkinson’s disease: A randomized control study. Complement. Ther. Med. 2015, 23, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Avenali, M.; Picascia, M.; Minafra, B.; Tassorelli, C.; Sinforiani, E.; Bernini, S. Intensive physical therapy mitigates cognitive decline in people with parkinson’s disease. J. Alzheimers Dis. Parkinsonism 2019, 9, 475. [Google Scholar]
- Trung, J.; Hanganu, A.; Jobert, S.; Degroot, C.; Mejia-Constain, B.; Kibreab, M.; Bruneau, M.A.; Lafontaine, A.L.; Strafella, A.; Monchi, O. Transcranial magnetic stimulation improves cognition over time in parkinson’s disease. Parkinsonism Relat. Disord. 2019, 66, 3–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buard, I.; Sciacca, D.M.; Martin, C.S.; Rogers, S.; Sillau, S.H.; Greher, M.R.; Chen, R.; Kluger, B.M. Transcranial magnetic stimulation does not improve mild cognitive impairment in parkinson’s disease. Mov. Disord. 2018, 33, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Doruk, D.; Gray, Z.; Bravo, G.L.; Pascual-Leone, A.; Fregni, F. Effects of tdcs on executive function in parkinson’s disease. Neurosci Lett. 2014, 582, 27–31. [Google Scholar] [CrossRef]
- Manenti, R.; Cotelli, M.S.; Cobelli, C.; Gobbi, E.; Brambilla, M.; Rusich, D.; Alberici, A.; Padovani, A.; Borroni, B.; Cotelli, M. Transcranial direct current stimulation combined with cognitive training for the treatment of parkinson disease: A randomized, placebo-controlled study. Brain Stimul. 2018, 11, 1251–1262. [Google Scholar] [CrossRef] [PubMed]
- Biundo, R.; Weis, L.; Fiorenzato, E.; Gentile, G.; Giglio, M.; Schifano, R.; Campo, M.C.; Marcon, V.; Martinez-Martin, P.; Bisiacchi, P.; et al. Double-blind randomized trial of tdcs versus sham in parkinson patients with mild cognitive impairment receiving cognitive training. Brain Stimul. 2015, 8, 1223–1225. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, B.J.; Gasson, N.; Johnson, A.R.; Booth, L.; Loftus, A.M. Cognitive training and transcranial direct current stimulation for mild cognitive impairment in parkinson’s disease: A randomized controlled trial. Parkinsons Dis. 2018, 2018, 4318475. [Google Scholar] [CrossRef] [PubMed]
- Adenzato, M.; Manenti, R.; Enrici, I.; Gobbi, E.; Brambilla, M.; Alberici, A.; Cotelli, M.S.; Padovani, A.; Borroni, B.; Cotelli, M. Transcranial direct current stimulation enhances theory of mind in parkinson’s disease patients with mild cognitive impairment: A randomized, double-blind, sham-controlled study. Transl. Neurodegener. 2019, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Del Felice, A.; Castiglia, L.; Formaggio, E.; Cattelan, M.; Scarpa, B.; Manganotti, P.; Tenconi, E.; Masiero, S. Personalized transcranial alternating current stimulation (tacs) and physical therapy to treat motor and cognitive symptoms in parkinson’s disease: A randomized cross-over trial. Neuroimage Clin. 2019, 22, 101768. [Google Scholar] [CrossRef] [PubMed]
- Seppi, K.; Ray Chaudhuri, K.; Coelho, M.; Fox, S.H.; Katzenschlager, R.; Perez Lloret, S.; Weintraub, D.; Sampaio, C. Update on treatments for nonmotor symptoms of parkinson’s disease-an evidence-based medicine review. Mov. Disord. 2019, 34, 180–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emre, M.; Aarsland, D.; Albanese, A.; Byrne, E.J.; Deuschl, G.; De Deyn, P.P.; Durif, F.; Kulisevsky, J.; van Laar, T.; Lees, A.; et al. Rivastigmine for dementia associated with parkinson’s disease. N. Engl. J. Med. 2004, 351, 2509–2518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emre, M.; Poewe, W.; De Deyn, P.P.; Barone, P.; Kulisevsky, J.; Pourcher, E.; van Laar, T.; Storch, A.; Micheli, F.; Burn, D.; et al. Long-term safety of rivastigmine in parkinson disease dementia: An open-label, randomized study. Clin. Neuropharmacol. 2014, 37, 9–16. [Google Scholar] [CrossRef]
- Leroi, I.; Brandt, J.; Reich, S.G.; Lyketsos, C.G.; Grill, S.; Thompson, R.; Marsh, L. Randomized placebo-controlled trial of donepezil in cognitive impairment in parkinson’s disease. Int. J. Geriatr. Psychiatry 2004, 19, 1–8. [Google Scholar] [CrossRef]
- Ravina, B.; Putt, M.; Siderowf, A.; Farrar, J.T.; Gillespie, M.; Crawley, A.; Fernandez, H.H.; Trieschmann, M.M.; Reichwein, S.; Simuni, T. Donepezil for dementia in parkinson’s disease: A randomised, double blind, placebo controlled, crossover study. J. Neurol. Neurosurg. Psychiatry 2005, 76, 934–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubois, B.; Tolosa, E.; Katzenschlager, R.; Emre, M.; Lees, A.J.; Schumann, G.; Pourcher, E.; Gray, J.; Thomas, G.; Swartz, J.; et al. Donepezil in parkinson’s disease dementia: A randomized, double-blind efficacy and safety study. Mov. Disord. 2012, 27, 1230–1238. [Google Scholar] [CrossRef] [PubMed]
- Litvinenko, I.V.; Odinak, M.M.; Mogil’naya, V.I.; Emelin, A.Y. Efficacy and safety of galantamine (reminyl) for dementia in patients with parkinson’s disease (an open controlled trial). Neurosci. Behav. Physiol. 2008, 38, 937–945. [Google Scholar] [CrossRef] [PubMed]
- Stinton, C.; McKeith, I.; Taylor, J.P.; Lafortune, L.; Mioshi, E.; Mak, E.; Cambridge, V.; Mason, J.; Thomas, A.; O’Brien, J.T. Pharmacological management of lewy body dementia: A systematic review and meta-analysis. Am. J. Psychiatry 2015, 172, 731–742. [Google Scholar] [CrossRef] [PubMed]
- Wesnes, K.A.; Aarsland, D.; Ballard, C.; Londos, E. Memantine improves attention and episodic memory in parkinson’s disease dementia and dementia with lewy bodies. Int. J. Geriatr. Psychiatry 2015, 30, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Inskip, M.; Mavros, Y.; Sachdev, P.S.; Fiatarone Singh, M.A. Exercise for individuals with lewy body dementia: A systematic review. PLoS ONE 2016, 11, e0156520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gratwicke, J.; Zrinzo, L.; Kahan, J.; Peters, A.; Beigi, M.; Akram, H.; Hyam, J.; Oswal, A.; Day, B.; Mancini, L. , et al. Bilateral deep brain stimulation of the nucleus basalis of meynert for parkinson disease dementia: A randomized clinical trial. JAMA Neurol. 2018, 75, 169–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silveira, C.R.A.; MacKinley, J.; Coleman, K.; Li, Z.; Finger, E.; Bartha, R.; Morrow, S.A.; Wells, J.; Borrie, M.; Tirona, R.G.; et al. Ambroxol as a novel disease-modifying treatment for parkinson’s disease dementia: Protocol for a single-centre, randomized, double-blind, placebo-controlled trial. BMC Neurol. 2019, 19, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagan, F.; Hebron, M.; Valadez, E.H.; Torres-Yaghi, Y.; Huang, X.; Mills, R.R.; Wilmarth, B.M.; Howard, H.; Dunn, C.; Carlson, A.; et al. Nilotinib effects in parkinson’s disease and dementia with lewy bodies. J. Parkinsons Dis. 2016, 6, 503–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagan, F.L.; Hebron, M.L.; Wilmarth, B.; Torres-Yaghi, Y.; Lawler, A.; Mundel, E.E.; Yusuf, N.; Starr, N.J.; Anjum, M.; Arellano, J.; et al. Nilotinib effects on safety, tolerability, and potential biomarkers in parkinson disease: A phase 2 randomized clinical trial. JAMA Neurol. 2020, 77, 309–317. [Google Scholar] [CrossRef] [Green Version]
- Reger, M.A.; Watson, G.S.; Green, P.S.; Baker, L.D.; Cholerton, B.; Fishel, M.A.; Plymate, S.R.; Cherrier, M.M.; Schellenberg, G.D.; Frey, W.H., 2nd; et al. Intranasal insulin administration dose-dependently modulates verbal memory and plasma amyloid-beta in memory-impaired older adults. J. Alzheimers Dis. 2008, 13, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Craft, S.; Baker, L.D.; Montine, T.J.; Minoshima, S.; Watson, G.S.; Claxton, A.; Arbuckle, M.; Callaghan, M.; Tsai, E.; Plymate, S.R.; et al. Intranasal insulin therapy for alzheimer disease and amnestic mild cognitive impairment: A pilot clinical trial. Arch. Neurol. 2012, 69, 29–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novak, P.; Pimentel Maldonado, D.A.; Novak, V. Safety and preliminary efficacy of intranasal insulin for cognitive impairment in parkinson disease and multiple system atrophy: A double-blinded placebo-controlled pilot study. PLoS ONE 2019, 14, e0214364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syn120 Fails to Show Efficacy against Parkinson Dementia in Phase 2a SynapseTrial. Available online: https://consultqd.clevelandclinic.org/syn120-fails-to-show-efficacy-against-parkinson-dementia-in-phase-2a-synapse-trial/ (accessed on 13 February 2021).
- Schenk, D.B.; Koller, M.; Ness, D.K.; Griffith, S.G.; Grundman, M.; Zago, W.; Soto, J.; Atiee, G.; Ostrowitzki, S.; Kinney, G.G. First-in-human assessment of prx002, an anti-α-synuclein monoclonal antibody, in healthy volunteers. Mov. Disord. 2017, 32, 211–218. [Google Scholar] [CrossRef]
- Jankovic, J.; Goodman, I.; Safirstein, B.; Marmon, T.K.; Schenk, D.B.; Koller, M.; Zago, W.; Ness, D.K.; Griffith, S.G.; Grundman, M.; et al. Safety and tolerability of multiple ascending doses of prx002/rg7935, an anti-α-synuclein monoclonal antibody, in patients with parkinson disease: A randomized clinical trial. JAMA Neurol. 2018, 75, 1206–1214. [Google Scholar] [CrossRef]
- Goldman, J.G.; Forsberg, L.K.; Boeve, B.F.; Armstrong, M.J.; Irwin, D.J.; Ferman, T.J.; Galasko, D.; Galvin, J.E.; Kaufer, D.; Leverenz, J.; et al. Challenges and opportunities for improving the landscape for lewy body dementia clinical trials. Alzheimers Res. Ther. 2020, 12, 137. [Google Scholar] [CrossRef]
- Holden, S.K.; Jones, W.E.; Baker, K.A.; Boersma, I.M.; Kluger, B.M. Outcome measures for parkinson’s disease dementia: A systematic review. Mov. Disord. Clin. Pract. 2016, 3, 9–18. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Approach to treating cognitive impairment in Parkinson’s disease. AchEI: acetylcholinesterase inhibitors. T-DCS: transcranial direct current stimulation.
Figure 1.
Approach to treating cognitive impairment in Parkinson’s disease. AchEI: acetylcholinesterase inhibitors. T-DCS: transcranial direct current stimulation.


{kind=link}
Table 1.
Neurotransmitters targeted for pharmacologic treatments for Parkinson’s disease cognitive changes.
Table 1.
Neurotransmitters targeted for pharmacologic treatments for Parkinson’s disease cognitive changes.
| Target Neurotransmitter | Drugs | Status | |
|---|---|---|---|
| PD-MCI | PDD | ||
| Acetylcholine | Rivastigmine | Experimental | FDA-approved |
| Donepezil | Off-label | ||
| Galantamine | Off-label | ||
| NMDA | Memantine | Experimental | |
| NYX-458 | Experimental | ||
| D-amino acid oxidase inhibitor (DAAOI-P) | Experimental | ||
| Dopamine | MAO-B inhibitors (e.g., rasagiline) | Investigational | |
| Mevidalen (LY3154207) (D1 receptor positive allosteric modulator) | Experimental | ||
| Serotonin | SYN120 (dual 5-HT6/5-HT2A antagonist) | Experimental | |
| Norepinephrine | Experimental | ||
MAO: monoamine oxidase, NMDA: N-methyl-d-aspartate.
Table 2.
Clinically available pharmacologic treatments for cognition in Parkinson’s disease mild cognitive impairment and Parkinson’s disease dementia.
Table 2.
Clinically available pharmacologic treatments for cognition in Parkinson’s disease mild cognitive impairment and Parkinson’s disease dementia.
| Category | Specific Agents | MCI | Dementia | Most Common Adverse Effects | Severe but Rare Adverse Effects |
|---|---|---|---|---|---|
| Cholinesterase inhibitors | Rivastigmine | Investigational 3 | Clinically useful 1 | Capsules: Nausea, Vomiting, weight loss Patch: nausea, vomiting, falls | Capsules: atrial fibrillation, myocardial infarction, hypokalemia, transient ischemic attack, seizures. Patch: dehydration |
| Donepezil | Not studied | Possibly useful 2 | Nausea, diarrhea, vomiting | Gastrointestinal hemorrhage, heart block, torsades de pointes | |
| Galantamine | Not studied | Possibly useful 2 | Nausea, vomiting, diarrhea | Syncope, Stevens–Johnson syndrome, gastrointestinal hemorrhage, seizure | |
| NMDA Receptor Antagonist | Memantine | Not studied | Investigational 3 | Diarrhea, constipation, confusion, dizziness | Stroke, seizure, renal failure |
| Dopaminergic therapy | Rasagiline (monoamine oxidase B inhibitor) | Investigational 3 | Not studied | Orthostatic hypotension, headache, nausea | Serotonin syndrome |
| Selective norepinephrine reuptake inhibitor | Atomoxetine | Investigational | Not studied | Increased heart rate, nausea, decreased appetite, xerostomia | Sudden cardiac death, stroke |
1: Clinically useful as determined by the International Parkinson and Movement Disorder Society Evidence-Based Medicine Review. 2: Possibly useful as determined by the International Parkinson and Movement Disorder Society Evidence-Based Medicine Review. 3: Investigational as determined by the International Parkinson and Movement Disorder Society Evidence Based Medicine Review. Inclusion in the table indicates that the pharmacologic agent is clinically available but does not imply regulatory approval for any specific indication. Adverse effects obtained from Micromedex, last accessed on 17 January 2021.
Table 3.
Common medications associated with adverse cognitive effects.
| Drug Class | Examples |
|---|---|
| Anticholinergics | |
| Tricyclic antidepressants | Amitriptyline, nortriptyline |
| First generation antihistamines | Diphenhydramine, hydroxyzine |
| Bladder antimuscarinics | Oxybutynin, trospium |
| Antipsychotics | Fluphenazine |
| Antimuscarinic spasmolytic | Atropine, hyoscyamine |
| Antiemetics | Meclizine |
| Muscle relaxants | Tizanidine |
| Anti-Parkinson | Benztropine, trihexyphenidyl |
| Benzodiazepines | Alprazolam, clonazepam, diazepam, lorazepam |
| Opioids | Codeine, hydrocodone, morphine, oxycodone, tramadol, methadone, fentanyl |
This table is non-exhaustive.
Table 4.
Clinical trials on pharmacologic treatments for cognitive impairment in Parkinson’s disease.
Table 4.
Clinical trials on pharmacologic treatments for cognitive impairment in Parkinson’s disease.
| Condition | Study Title | Drug Name | Trial Number | Start Date | Status/Phase | Location | Last Accessed |
|---|---|---|---|---|---|---|---|
| Investigation of Current drugs | |||||||
| PD-MCI | A Double-Blind Placebo Controlled Trial Evaluating Rasagiline Effects on Cognition in Parkinson’s Disease Patients with Mild Cognitive Impairment Receiving Dopaminergic Therapy (RECOGNIZE) | Rasagiline | NCT01497652 | January 2012 | Completed/4 | USA | 17 January 2021 |
| PDD | Memantine for Treatment of Cognitive Impairment in Patients with Parkinson’s Disease and Dementia | Memantine | NCT00294554 | September 2008 | Completed/N/A | USA | 17 January 2021 |
| Drug Repurposing | |||||||
| PDD | Ambroxol as a Treatment for Parkinson’s Disease Dementia | Ambroxol | NCT02914366 | November 2015 | Recruiting/2 | Canada | 17 January 2021 |
| PDD | To Assess the Efficacy and Safety of Ceftriaxone in Patients with Mild to Moderate Parkinson’s Disease Dementia | Ceftriaxone | NCT03413384 | 15 February 2019 | Recruiting/2 | Taiwan | 17 January 2021 |
| PD without dementia | Cognitive Dysfunction in PD: Pathophysiology and Potential Treatments, a Pilot Study | Atomoxetine, rivastigmine | NCT01340885 | 2011 | Completed/4 | USA | 17 January 2021 |
| Novel Medications | |||||||
| PDD | SYN120 Study to Evaluate Its Safety, Tolerability and Efficacy in Parkinson’s Disease Dementia (SYNAPSE) | SYN120 | NCT02258152 | 22 December 2014 | Completed/2 | USA | 17 January 2021 |
| PDD | ANAVEX2-73 Study in Parkinson’s Disease Dementia | ANAVEX2-73 | NCT03774459 | 9 July 2018 | Completed/2 | Multiple, international | 17 January 2021 |
| PDD | OLE Study for Patients with Parkinson’s Disease with Dementia Enrolled in Study ANAVEX2-73-PDD-001 | ANAVEX2-73 | NCT04575259 | 10 October 2019 | Recruiting/2 | USA | 17 January 2021 |
| PDD | Effect of LY3154207 on Cognition in Mild-to-Moderate Dementia Due to Lewy Body Dementia (LBD) Associated with Idiopathic Parkinson’s Disease (PD) or Dementia with Lewy Bodies (DLB) | LY3154207 | NCT03305809 | November 2017 | Completed/2 | USA, Canada, Puerto Rico | 17 January 2021 |
| PD 1 | A Study to Evaluate the Efficacy of Prasinezumab (RO7046015/PRX002) in Participants with Early Parkinson’s Disease (PASADENA) | Prasinezumab | NCT03100149 | June 2017 | Active, not recruiting/2 | Multiple, international | 18 January 2021 |
| PDD | A Multicenter, Open Label Study to Evaluate Tolerability and Efficacy of Orally Administered ENT-01 for the Treatment of Parkinson’s Disease Dementia. | ENT-01 | NCT03938922 | 13 June 2019 | Active, not recruiting/1 | USA | 18 January 2021 |
| PD-MCI and probable or possible PDD | A Study to Assess the Safety of GRF6021 Infusions in Subjects with Parkinson’s Disease and Cognitive Impairment | GRF6021 | NCT03713957 | November 2018 | Completed/2 | Multiple, international | 18 January 2021 |
| PD-MCI | A Study to Evaluate NYX-458 in Subjects with Mild Cognitive Impairment Associated with Parkinson’s Disease | NYX-458 | NCT04148391 | November 2019 | Active, not recruiting/2 | USA | 18 January 2021 |
| PDD | Multidisciplinary Study of Novel NMDA Modulation for Neurodegenerative Disorder | DAAOI-P | NCT04470037 | April 2016 | Recruiting/2 | Taiwan | 18 January 2021 |
1: studies in individuals with Parkinson’s disease without specifying the presence of MCI or dementia.
Table 5.
Clinical trials on non-pharmacologic treatments for cognitive impairment in Parkinson’s disease.
Table 5.
Clinical trials on non-pharmacologic treatments for cognitive impairment in Parkinson’s disease.
| Condition | Study Title | Therapy | Trial Number | Start Date | Status/Phase | Location | Last Accessed |
|---|---|---|---|---|---|---|---|
| PD-MCI | Cognitive Rehabilitation for Individuals with Parkinson’s Disease and MCI | Cognitive training | NCT03335150 | November 2015 | Active, not recruiting/N/A | USA | 18 January 2021 |
| PD with normal cognition, PD-MCI | Rehabilitation of Everyday Memory Impairment in Parkinson’s Disease: A Pilot Study | Cognitive training | NCT01469741 | 2011 | Completed/N/A | USA | 18 January 2021 |
| PD-MCI | Computer-based Cognitive Training for Individuals with Parkinson’s Disease | Computer-based cognitive training | NCT02225314 | 2012 | Completed/N/A | USA | 18 January 2021 |
| PD-MCI | A Trial of Neurocognitive and Supportive Therapy Interventions for Individuals with Parkinson’s Disease | Cognitive rehabilitation | NCT01646333 | July 2012 | Completed/N/A | USA | 18 January 2021 |
| PD-MCI, mild PDD | Training of Psychosocial Skills Based on Cognitive Behavioral Therapy for Patients with Parkinson’s Disease (CBT) | Cognitive Behavioral Therapy | NCT02048605 | February 2014 | Active, not recruiting/N/A | Switzerland | 18 January 2021 |
| PD with normal cognition, PD-MCI | Prospective Memory Impairment in Parkinson’s Disease-related Cognitive Decline: Intervention and Mechanisms | Cognitive training | NCT04474379 | January 2021 | Not yet recruiting/N/A | USA | 18 January 2021 |
| PD-MCI | Prospective Memory Training in Parkinson’s Disease | Cognitive training | NCT03582670 | October 2017 | Completed/N/S | USA | 18 January 2021 |
| PD-MCI | Cognitive Rehabilitation for Veterans with Parkinson’s Disease | Cognitive training | NCT03836963 | January 2020 | Recruiting/N/A | USA | 18 January 2021 |
| PD-MCI | Exercise Targeting Cognitive Impairment in Parkinson’s Disease | Exercise | NCT02267785 | October 2014 | Active, not recruiting/N/A | USA | 18 January 2021 |
| PD-MCI | A Telemedicine Intervention to Improve Cognitive Function in Patients With PD | Exercise | NCT02248649 | December 2014 | Completed/N/A | USA | 18 January 2021 |
| PD, MCI 1 | Molecular Mediators of Physical Exercise and Carnosine Induced Effects in Patients with Preclinical and Early-Stage Neurodegenerative Disease | Exercise, carnosine | NCT03330470 | January 2017 | Unknown/N/A | Slovakia, Taiwan | 18 January 2021 |
| PDD 2 | Tailored Music Therapy for Dementia | Music | NCT03011723 | January 2017 | Active, not recruiting/N/A | Norway | 18 January 2021 |
| PD 3 | Double-blind, Randomized Controlled Trial to Demonstrate Efficacy of Celeste® Specialized Phototherapy in Treating Parkinson’s Disease. | Phototherapy | NCT04453033 | November 2020 | Not yet recruiting/N/A | N/A | 18 January 2021 |
| PDD | Combined Subthalamic and Nucleus Basalis Meynert Deep Brain Stimulation for Parkinson’s Disease with Dementia (Dempark-DBS) | DBS | NCT02589925 | October 2016 | Active, not recruiting/N/A | Germany | 18 January 2021 |
| PD-MCI | GPi+NBM DBS in Parkinson’s Disease with Mild Cognitive Impairment (2T-DBS) | DBS | NCT04571112 | December 2017 | Active, not recruiting/N/A | Canada | 18 January 2021 |
| PD-MCI | Deep Brain Stimulation of the NBM to Treat Mild Cognitive Impairment in Parkinson’s Disease | DBS | NCT02924194 | September 2016 | Recruiting/N/A | USA | 18 January 2021 |
| PD-MCI | Cortical Physiology as a Therapeutic Target in Parkinson’s Disease Related Dementia and Cognitive Dysfunction | TMS | NCT02346708 | December 2018 | Active, not recruiting/N/A | USA | 18 January 2021 |
| PD-MCI | rTMS as a Cognitive Rehabilitation Approach in Veterans with Parkinson’s Disease | TMS | NCT03836950 | April 2020 | Recruiting/1 & 2 | USA | 18 January 2021 |
| PD-MCI | Transcranial Direct Current Stimulation for Cognitive Improvement in Parkinson’s Mild Cognitive Impairment (tDCS) | tDCS | NCT03191916 | October 2015 | Recruiting/N/A | USA | 18 January 2021 |
| PD-MCI | Efficacy of Transcranial Direct Current Stimulation in Parkinson’s Disease MCI (PDMCIStim) | tDCS | NCT04171804 | January 2019 | Recruiting/N/A | Turkey | 18 January 2021 |
| PD with normal cognition, PD-MCI | tDCS on Parkinson’s Disease Cognition (tDCS-PD-fMRI) | tDCS | NCT03025334 | March 2017 | Recruiting/N/A | Canada | 18 January 2021 |
| PD-MCI, PDD | The Use of Transcranial Focused Ultrasound for the Treatment of Neurodegenerative Dementias | Transcranial ultrasound | NCT04250376 | November 2017 | Enrolling by invitation/N/A | USA | 18 January 2021 |
| PDD | A Study to Evaluate the Safety and Feasibility of Temporary Blood Brain Barrier Disruption (BBBD) Using Exablate MR Guided Focused Ultrasound in Patients with Parkinson’s Disease Dementia | Transcranial ultrasound | NCT03608553 | November 2018 | Recruiting/N/A | Spain | 18 January 2021 |
| PD with normal cognition, PD-MCI | Electrical Vestibular Stimulation (VeNS) in the Management of Parkinson’s Disease | Vestibular stimulation | NCT04450550 | September 2020 | Not yet recruiting/N/A | N/A | 18 January 2021 |
1: Recruited subjects include persons with subjective cognitive impairment (SCI), MCI, or early-stage PD (Hoehn-Yarh stage 1–2). 2: Recruited subjects include persons with Alzheimer’s dementia, vascular dementia, dementia with Lewy bodies, and PDD. 3: Recruited subjects include individuals with Parkinson’s disease, not specifically PD-MCI or PDD.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sun, C.; Armstrong, M.J. Treatment of Parkinson’s Disease with Cognitive Impairment: Current Approaches and Future Directions. Behav. Sci. 2021, 11, 54. https://0-doi-org.brum.beds.ac.uk/10.3390/bs11040054
AMA Style
Sun C, Armstrong MJ. Treatment of Parkinson’s Disease with Cognitive Impairment: Current Approaches and Future Directions. Behavioral Sciences. 2021; 11(4):54. https://0-doi-org.brum.beds.ac.uk/10.3390/bs11040054
Chicago/Turabian StyleSun, Chichun, and Melissa J. Armstrong. 2021. "Treatment of Parkinson’s Disease with Cognitive Impairment: Current Approaches and Future Directions" Behavioral Sciences 11, no. 4: 54. https://0-doi-org.brum.beds.ac.uk/10.3390/bs11040054
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.