
Occurrence of P. aeruginosa in Water Intended for Human Consumption and in Swimming Pool Water

 ,
,  , , , and
, , , and 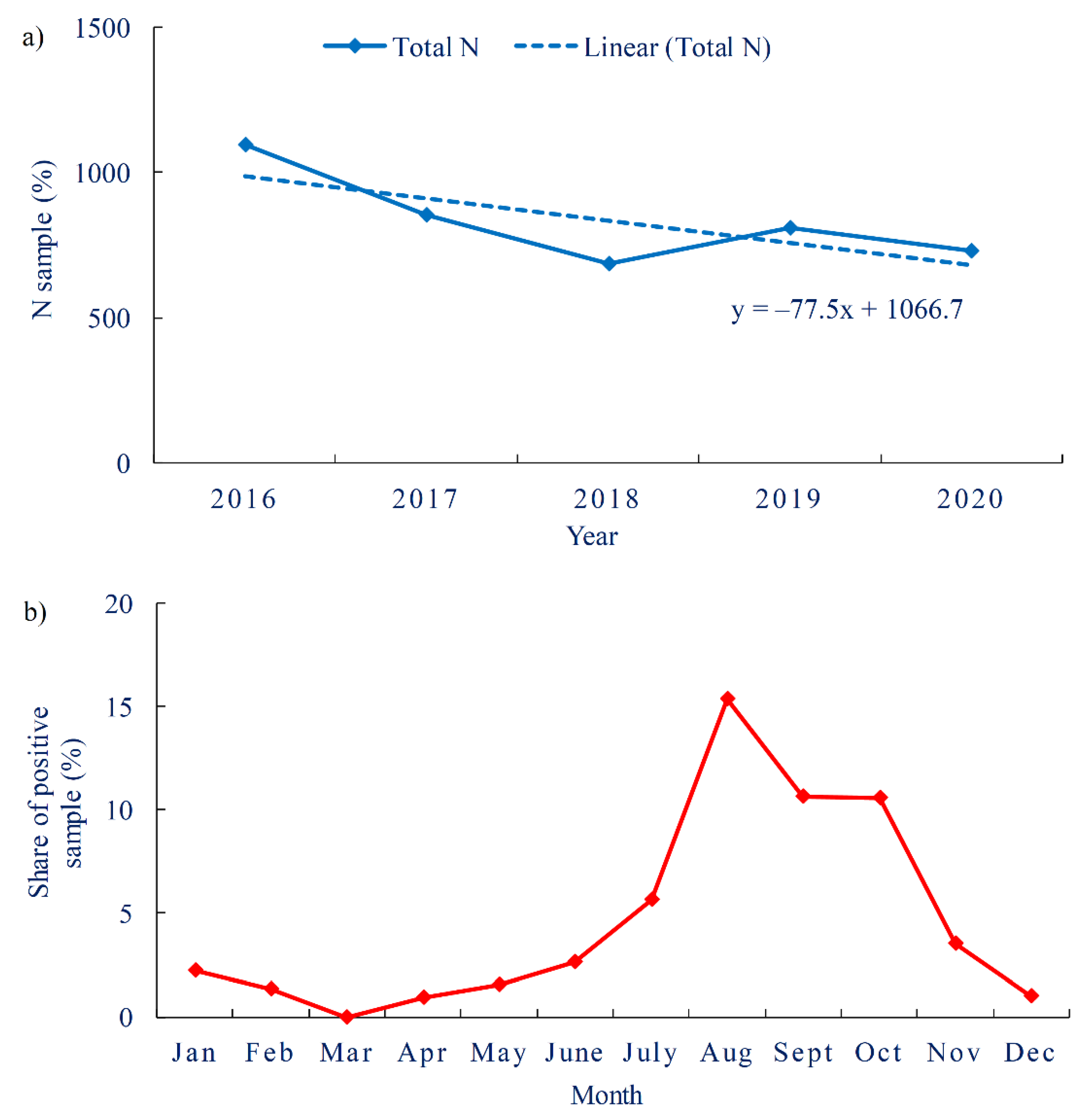{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results and Discussion
3.1. Drinking Water
3.1.1. Occurrence of P. aeruginosa in Drinking Water
3.1.2. Drinking Water Legislation
3.2. Swimming Pool Water
3.2.1. Occurrence of P. aeruginosa in Swimming Pool Water
3.2.2. Swimming Pool Water Legislation
4. Conclusions
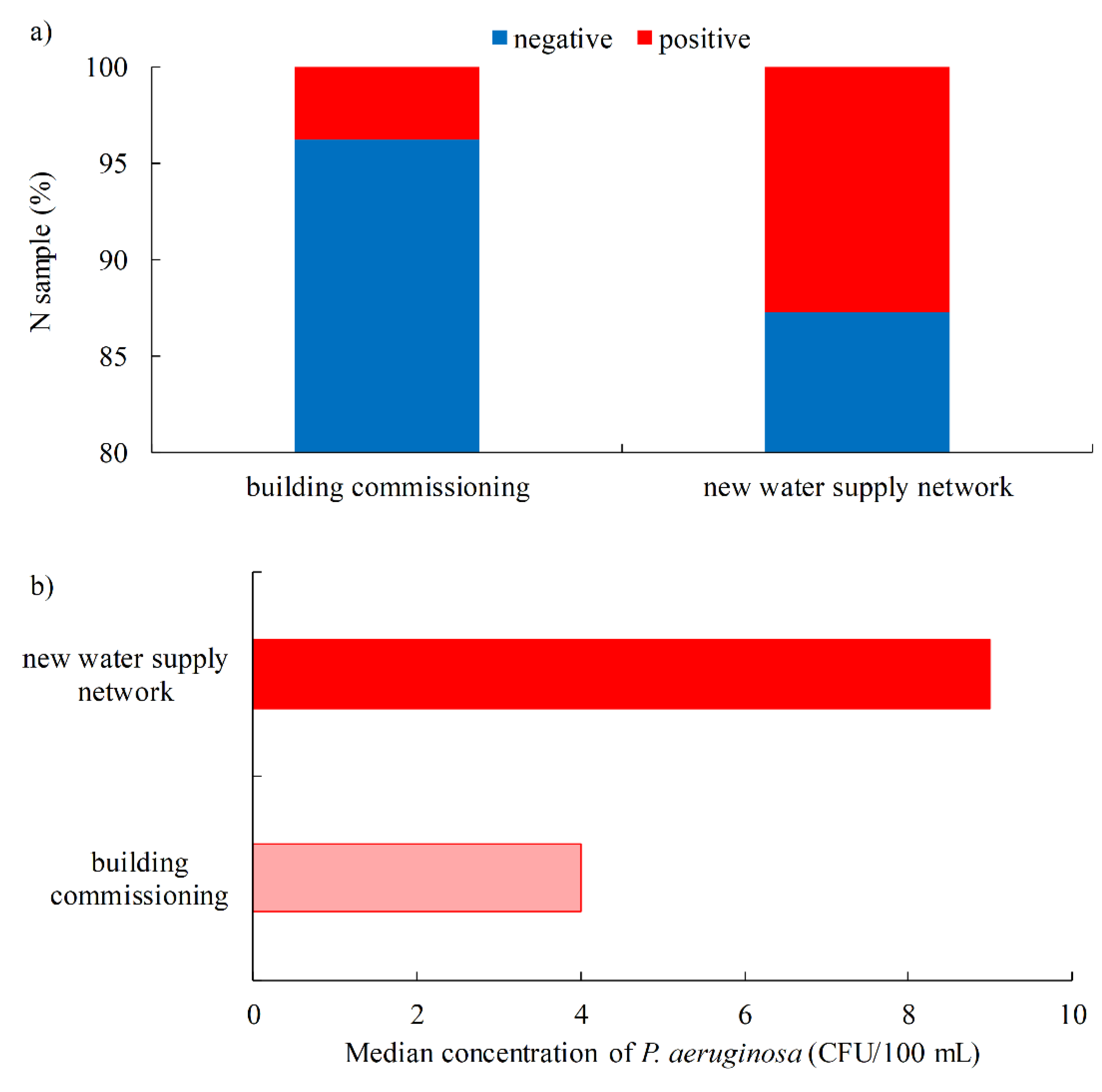
- In total, 3.9% of drinking water samples were positive for the presence of P. aeruginosa, mainly during the commissioning of buildings or the construction of a new water supply network.
- There is no general agreement on whether it is appropriate to routinely test drinking water in public water systems for the presence of P. aeruginosa, as the prevailing opinion is that this bacterium does not pose a health risk to the general population.
- Some countries restrict surveillance for P. aeruginosa by national guidelines to hospitals and other health care facilities, nursing homes and other public facilities housing the elderly. Croatia is one of these countries which, in our opinion, has raised the level of health protection for the most vulnerable population groups, although the standard set does not require the absence of this bacterium in the public water supply, which would be difficult to achieve in real conditions.
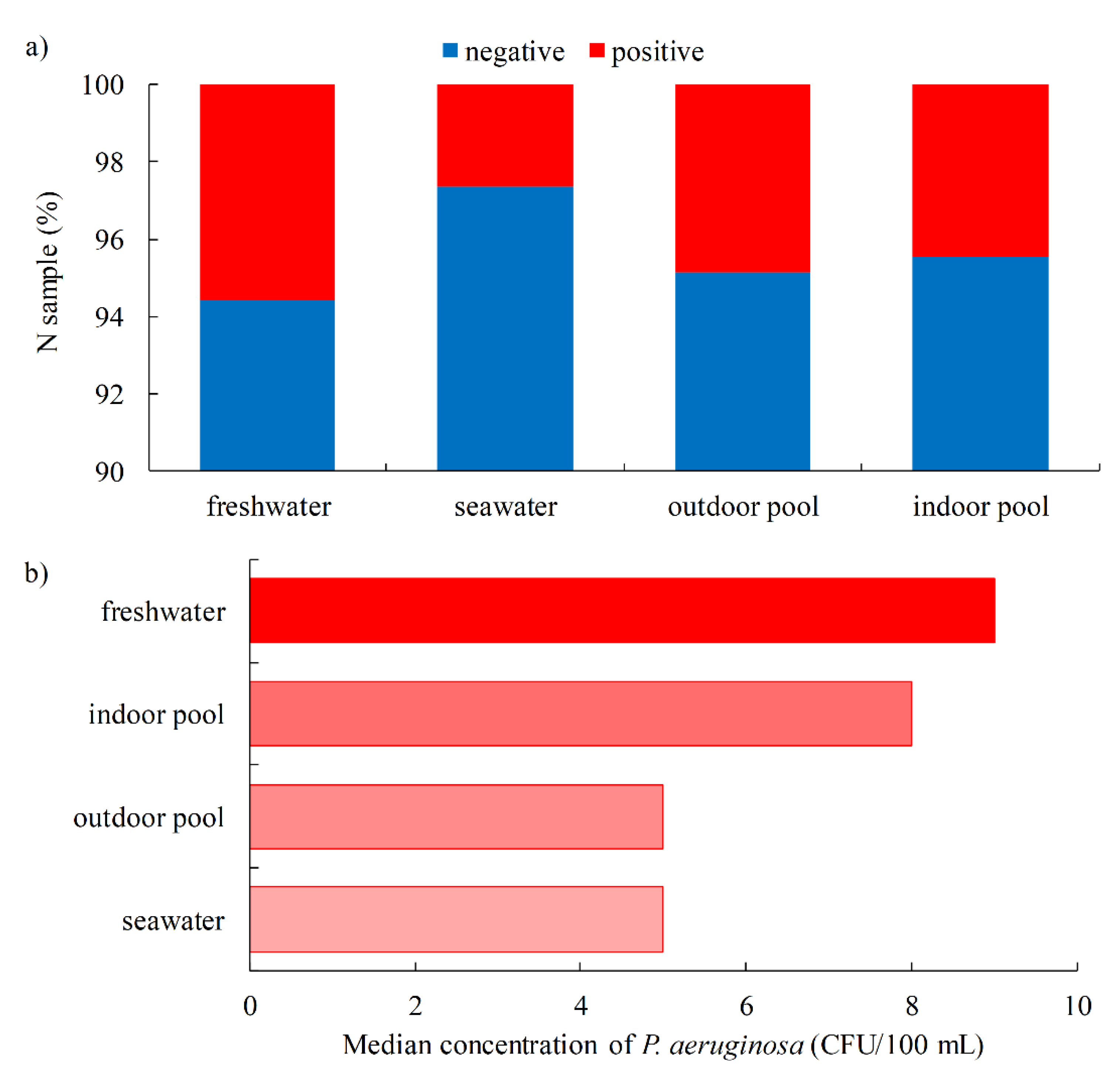
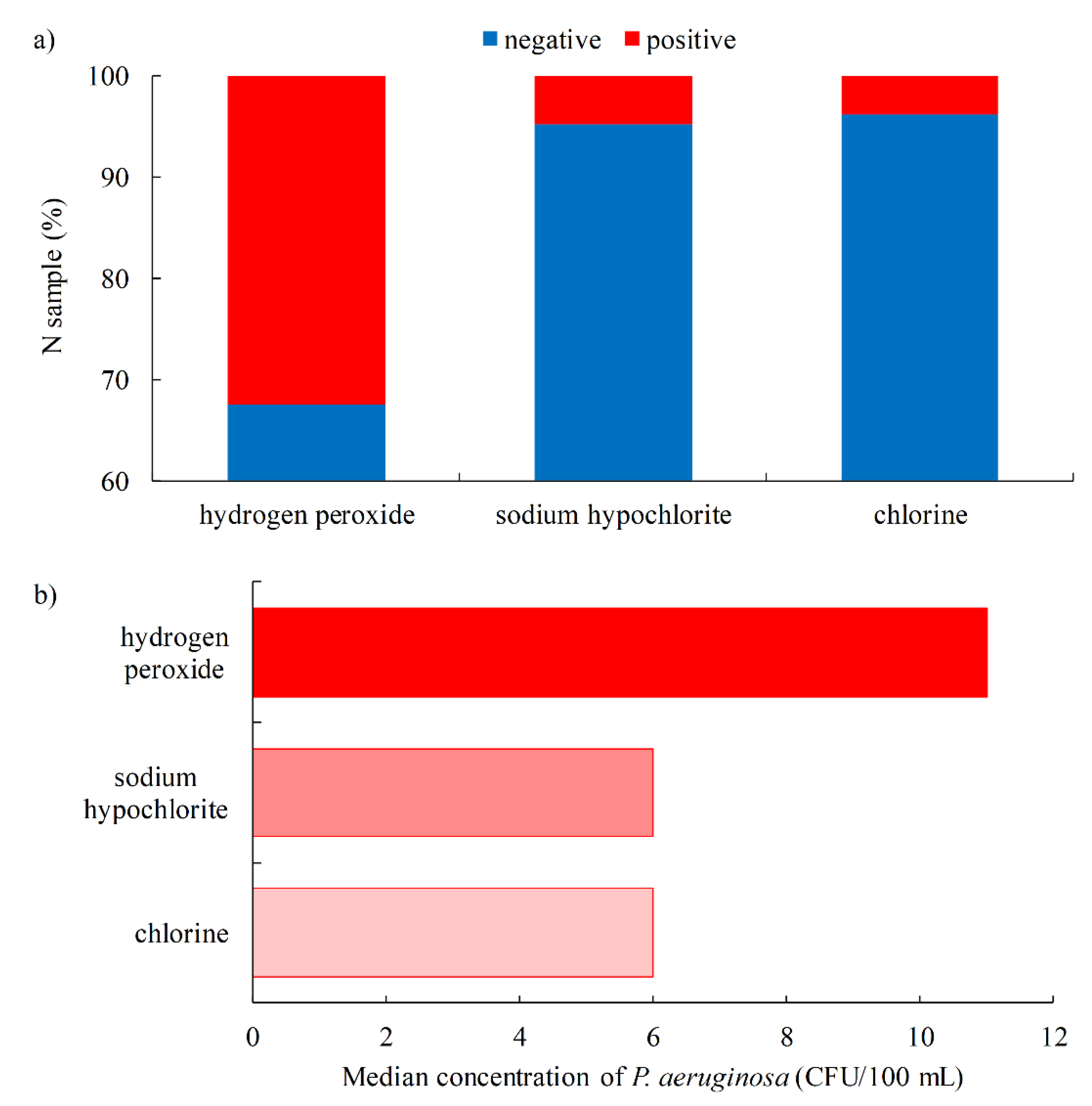
- P. aeruginosa was detected more frequently: in outdoor pools (4.9%) vs. indoor pools (4.5%); freshwater pools (5.6%) vs. seawater pools (2.7%); entertainment pools (13.8%) and spa/hydromassage pools (4.8%) vs. children (3.9%), recreational (3.9%), rehabilitation (2.1%) and sports pools (1.2%); when hydrogen peroxide (32.4%) is used as a disinfectant vs. sodium hypochlorite (4.8%) and chlorine (3.8%).
- Unlike water intended for human consumption, the testing of P. aeruginosa in swimming pool water is consistent in all countries covered by this study, where P. aeruginosa is a mandatory parameter for testing of the safety of swimming pool water.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bédard, E.; Prévost, M.; Déziel, E. Pseudomonas aeruginosa in premise plumbing of large buildings. Microbiologyopen 2016, 5, 937–956. [Google Scholar] [CrossRef] [PubMed]
- Science Direct. Pseudomonas aeruginosa. 2021. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/topics/medicine-and-dentistry/pseudomonas-aeruginosa (accessed on 18 October 2021).
- European Commission. Directive (EU) 2020/2184 of the European Parliament and of the Council of 16 December 2020 on the quality of water intended for human consumption (recast). Off. J. Eur. Union 2020, 435, 1–62. [Google Scholar]
- Liu, S.; Gunawan, C.; Barraud, N.; Rice, S.A.; Harry, E.J.; Amal, R. Understanding, monitoring, and controlling biofilm growth in drinking water distribution systems. Environ. Sci. Technol. 2016, 50, 8954–8976. [Google Scholar] [CrossRef] [PubMed]
- Lutz, J.K.; Lee, J. Prevalence and antimicrobial-resistance of Pseudomonas aeruginosa in swimming pools and hot tubs. Int. J. Environ. Res. Public Health 2011, 8, 554–564. [Google Scholar] [CrossRef] [Green Version]
- Lehtola, M.J.; Nissinen, T.K.; Miettinen, I.T.; Martikainen, P.J.; Vartiainen, T. Removal of soft deposits from the distribution system improves the drinking water quality. Water Res. 2004, 38, 601–610. [Google Scholar] [CrossRef]
- Eschbach, M.; Schreiber, K.; Trunk, K.; Buer, J.; Jahn, D.; Schobert, M. Long-term anaerobic survival of the opportunistic pathogen Pseudomonas aeruginosa via pyruvate fermentation. J. Bacteriol. 2004, 186, 4596–4604. [Google Scholar] [CrossRef] [Green Version]
- Diggle, S.P.; Whiteley, M. Microbe Profile: Pseudomonas aeruginosa: Opportunistic pathogen and lab rat. Microbiology 2020, 166, 30–33. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Guidelines for Drinking-Water Quality, 4th ed.; Incorporating the 1st Addendum; WHO: Geneva, Switzerland, 2017; Available online: https://www.who.int/publications/i/item/9789241549950 (accessed on 18 November 2021).
- Penna, V.T.; Martins, S.A.; Mazzola, P.G. Identification of bacteria in drinking and purified water during the monitoring of a typical water purification system. BMC Public Health 2002, 2, 13. [Google Scholar] [CrossRef] [Green Version]
- ISO 16266:2008. Detection and Enumeration of Pseudomonas aeruginosa—Method by Membrane Filtration; International Organization for Standardization (ISO): Geneva, Switzerland, 2008. [Google Scholar]
- ISO 9308-1:2014/AMD 1:2016. Water Quality—Enumeration of Escherichia coli and Coliform Bacteria—Part 1: Membrane Filtration Method for Waters with Low Bacterial Background Flora—Amendment 1; (ISO 9308-1:2014/AMD 1:2016; EN ISO 9308-1:2014/AMD 1:2016); International Organization for Standardization: Geneva, Switzerland, 2014. [Google Scholar]
- Baird, R.; Bridgewater, L. Standard Methods for the Examination of Water and Wastewater, 23rd ed.; American Public Health Association: Washington, DC, USA, 2017. [Google Scholar]
- ISO 11731:2017. Water Quality—Enumeration of Legionella; International Organization for Standardization (ISO): Geneva, Switzerland, 2017.
- ISO 6222:1999. Water Quality—Enumeration of Culturable Micro-Organisms—Colony Count by Inoculation in a Nutrient Agar Culture Medium; International Organization for Standardization (ISO): Geneva, Switzerland, 1999.
- Standard Method 2550 B. Temperature of Water. Standard Methods for the Examination of Water and Waste Water, 23rd ed.; American Public Health Association (APHA): Washington, DC, USA, 2017.
- ISO 7027-1:2016. Water Quality—Determination of Turbidity—Part 1: Quantitative Methods; International Organization for Standardization (ISO): Geneva, Switzerland, 2016.
- ISO 7888:1985. Water Quality—Determination of Electrical Conductivity; International Organization for Standardization (ISO): Geneva, Switzerland, 1985.
- ISO 7393-2:2018. Water Quality—Determination of Free Chlorine and Total Chlorine—Part 2: Colorimetric Method Using N,N-Diethyl-1,4-Phenylenediamine, for Routine Control Purposes; International Organization for Standardization (ISO): Geneva, Switzerland, 2018.
- ISO 10523:2008. Water Quality—Determination of pH.; International Organization for Standardization (ISO): Geneva, Switzerland, 2008.
- ISO 10301:1997. Water Quality—Determination of Highly Volatile Halogenated Hydrocarbons—Gas-Chromatographic Methods; International Organization for Standardization (ISO): Geneva, Switzerland, 1997.
- ISO 7150-1:1984. Water Quality—Determination of Ammonium—Part 1: Manual Spectrometric Method; International Organization for Standardization (ISO): Geneva, Switzerland, 1984.
- ISO 9297:1989 Modified. Water Quality—Determination of Chloride—Silver Nitrate Titration with Chromate Indicator (Mohr’s Method); International Organization for Standardization (ISO): Geneva, Switzerland, 1989.
- ISO 10304-1:2007. Water Quality—Determination of Dissolved Anions by Liquid Chromatography of Ions—Part 1: Determination of Bromide, Chloride, Fluoride, Nitrate, Nitrite, Phosphate and Sulfate; International Organization for Standardization (ISO): Geneva, Switzerland, 2007.
- Mena, K.D.; Gerba, C.P. Risk assessment of Pseudomonas aeruginosa in water. Rev. Environ. Contam. Toxicol. 2009, 201, 71–115. [Google Scholar] [CrossRef]
- Anversa, L.; Arantes Stancari, R.C.; Garbelotti, M.; da Silva Ruiz, L.; Pereira, V.B.R.; Nogueira Nascentes, G.A.; Alves Dantas, S.T.; Mores Rall, V.L. Pseudomonas aeruginosa in public water supply. Water Pract. Technol. 2019, 14, 732–737. [Google Scholar] [CrossRef]
- De Victorica, J.; Galván, M. Pseudomonas aeruginosa as an indicator of health risk in water for human consumption. Water Sci. Technol. 2001, 43, 49–52. [Google Scholar] [CrossRef] [Green Version]
- Wen, X.; Chen, F.; Lin, Y.; Zhu, H.; Yuan, F.; Kuang, D.; Jia, Z.; Yuan, Z. Microbial indicators and their use for monitoring drinking water quality—A review. Sustainability 2020, 12, 2249. [Google Scholar] [CrossRef] [Green Version]
- Camilla, B.; Daverio, E.; Michela, G. Microbiology Dimension in EU Water Directives; EUR 20787 EN. JRC25814; European Commission: Brussels, Belgium, 2003; Available online: https://publications.jrc.ec.europa.eu/repository/handle/JRC25814 (accessed on 20 September 2021).
- World Health Organization (WHO). Heterotrophic Plate Counts and Drinking-Water Safety; IWA Publishing: London, UK, 2006; Available online: https://www.who.int/water_sanitation_health/dwq/HPCFull.pdf (accessed on 6 November 2021).
- Moritz, M.M.; Flemming, H.-C.; Wingender, J. Integration of Pseudomonas aeruginosa and Legionella pneumophila in drinking water biofilms grown on domestic plumbing materials. Int. J. Hyg. Environ. Health 2010, 213, 190–197. [Google Scholar] [CrossRef]
- Exner, M.; Kramer, A.; Lajoie, L.; Gebel, J.; Engelhart, S.; Hartemann, P. Prevention and control of health care–associated waterborne infections in health care facilities. Am. J. Infect. Control 2005, 33, S26–S40. [Google Scholar] [CrossRef]
- Loveday, H.P.; Wilson, J.A.; Kerr, K.; Pitchers, R.; Walker, J.T.; Browne, J. Association between healthcare water systems and Pseudomonas aeruginosa infections: A rapid systematic review. J. Hosp. Infect. 2014, 86, 7–15. [Google Scholar] [CrossRef]
- Xue, Z.; Hessler, C.M.; Panmanee, W.; Hassett, D.J.; Seo, Y. Pseudomonas aeruginosa inactivation mechanism is affected by capsular extracellular polymeric substances reactivity with chlorine and monochloramine. FEMS Microbiol. Ecol. 2013, 83, 101–111. [Google Scholar] [CrossRef] [Green Version]
- Official Gazette of the Republic of Croatia 125/2017 and 39/2020. Ordinance on Compliance Parameters and Methods of Analysis, Monitoring and Water Safety Plans of Water for Human Consumption and the Manner of Keeping a Register of Legal Entities Performing Public Water Supply Activities; Ministry of Health: Zagreb, Croatia, 2017. [Google Scholar]
- Department of Health Estates & Facilities. HTM 04-01—Addendum: Pseudomonas aeruginosa—Advice for Augmented Care Units. 2013. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/140105/Health_Technical_Memorandum_04-01_Addendum.pdf (accessed on 5 October 2021).
- The French Society for Hospital Hygiene (SFHH). Recommandations Nationales. Préventionde la Transmission Croisée: Précautions Complémentaires Contact. 2009. Available online: https://www.sf2h.net/wp-content/uploads/2009/01/SF2H_prevention-transmission-croisee-2009.pdf (accessed on 18 October 2021).
- Official Gazette of the Republic of Montenegro 24/2012 and 32/2015. The Rulebook on Detailed Safety Requirements for Drinking Water; Ministry of Health: Podgorica, Montenegro, 2012; Available online: http://www.podaci.net/_gCGO/propis/Pravilnik_o_blizim/P-bzpbti04v1224.html (accessed on 20 November 2021).
- Official Gazette of the Federation of Bosnia and Herzegovina 40/10; 43/10; 30/12 and 62/2017. Regulation on Health Safety of Drinking Water; Official Gazette of the Federation of Bosnia and Herzegovina: Sarajevo, Bosnia and Herzegovina, 2010. [Google Scholar]
- Official Gazette of the Republic of Slovenia 19/04; 35/04; 26/06; 92/06; 25/09; 74/15; 51/17. Rules on Drinking Water; Uradni List Republike Slovenije: Ljubljana, Slovenia, 2004. [Google Scholar]
- U.S. Environmental Protection Agency (U.S. EPA). National Primary Drinking Water Regulations. Microorganisms. 2017. Available online: https://www.epa.gov/ground-water-and-drinking-water/national-primary-drinking-water-regulations#Microorganisms (accessed on 22 August 2021).
- Hardalo, C.; Edberg, S.C. Pseudomonas aeruginosa: Assessment of risk from drinking water. Crit. Rev. Microbiol. 1997, 23, 47–75. [Google Scholar] [CrossRef]
- Firuzi, P.; Asl Hashemi, A.; Samadi Kafil, H.; Gholizadeh, P.; Aslani, H. Comparative study on the microbial quality in the swimming pools disinfected by the ozone-chlorine and chlorine processes in Tabriz, Iran. Environ. Monit. Assess. 2020, 192, 516. [Google Scholar] [CrossRef]
- Hajjartabar, M. Poor-quality water in swimming pools associated with a substantial risk of otitis externa due to Pseudomonas aeruginosa. Water Sci. Technol. 2004, 50, 63–67. [Google Scholar] [CrossRef]
- Abd El-Salam, M.M. Assessment of water quality of some swimming pools: A case study in Alexandria, Egypt. Environ. Monit. Assess. 2012, 184, 7395–7406. [Google Scholar] [CrossRef]
- Aboulfotoh Hashish, N.M.; Gawad Abbass, A.A.; Khamis Amine, A.E. Pseudomonas aeruginosa in swimming pools. Cogent Environ. Sci. 2017, 3, 1328841. [Google Scholar] [CrossRef]
- Dallolio, L.; Belletti, M.; Agostini, A.; Teggi, M.; Bertelli, M.; Bergamini, C.; Chetti, L.; Leoni, E. Hygienic surveillance in swimming pools: Assessment of the water quality in Bologna facilities in the period 2010–2012. Microchem. J. 2013, 110, 624–628. [Google Scholar] [CrossRef]
- Moore, J.E.; Heaney, N.; Millar, B.C.; Crowe, M.; Elborn, J.S. Incidence of Pseudomonas aeruginosa in recreational and hydrotherapy pools. Commun. Dis. Public Health 2002, 5, 23–26. [Google Scholar]
- Wei, X.; Li, J.; Hou, S.; Xu, C.; Zhang, H.; Atwill, E.R.; Li, X.; Yang, Z.; Chen, S. Assessment of microbiological safety of water in public swimming pools in Guangzhou, China. Int. J. Environ. Res. Public Health 2018, 15, 1416. [Google Scholar] [CrossRef] [Green Version]
- Croatian Bureau of Statistic. CBS Databases. 2021. Available online: https://www.dzs.hr (accessed on 15 August 2021).
- Papadopoulou, C.; Economou, V.; Sakkas, H.; Gousia, P.; Giannakopoulos, X.; Dontorou, C.; Filioussis, G.; Gessouli, H.; Karanis, P.; Leveidiotou, S. Microbiological quality of indoor and outdoor swimming pools in Greece: Investigation of the antibiotic resistance of the bacterial isolates. Int. J. Hyg. Environ. Health 2008, 211, 385–397. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Guidelines for Safe Recreational Water Environments. Volume 2 Swimming Pools and Similar Environments; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Ujević Bošnjak, M.; Gajšak, F.; Antičević, M.; Štiglić, J. Pool water safety in Republic of Croatia in year 2017. In Proceedings of the XXII Scientific and Professional Conference Water and Public Water Supply, Sisak, Croatia, 2–5 October 2018; pp. 23–31. [Google Scholar]
- Ríos-Castillo, A.G.; González-Rivas, F.; Rodríguez-Jerez, J.J. Bactericidal efficacy of hydrogen peroxide-based disinfectants against gram-positive and gram-negative bacteria on stainless steel surfaces. J. Food. Sci. 2017, 82, 2351–2356. [Google Scholar] [CrossRef]
- Borgmann-Strahsen, R. Comparative assessment of different biocides in swimming pool water. Int. Biodeterior. Biodegrad. 2003, 51, 291–297. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. The Model Aquatic Health Code ANNEX Draft Posted for Public Comment. Disinfection and Water Quality 2012. Available online: https://www.cdc.gov/healthywater/pdf/swimming/pools/mahc/structure-content/mahc-disinfection-water-quality-annex.pdf (accessed on 20 November 2021).
- Rice, S.A.; van den Akker, B.; Pomati, F.; Roser, D. A risk assessment of Pseudomonas aeruginosa in swimming pools: A review. J Water Health 2012, 10, 181–196. [Google Scholar] [CrossRef] [Green Version]
- Corre, M.-H.; Delafont, V.; Legrand, A.; Berjeaud, J.-M.; Verdon, J. Exploiting the richness of environmental waterborne bacterial species to find natural Legionella pneumophila competitors. Front. Microbiol. 2019, 9, 3360. [Google Scholar] [CrossRef]
- Borella, P.; Montagna, M.T.; Romano-Spica, V.; Stampi, S.; Stancanelli, G.; Triassi, M.; Neglia, R.; Marchesi, I.; Fantuzzi, G.; Tatò, D.; et al. Legionella infection risk from domestic hot water. Emerg. Infect. Dis. 2004, 10, 457–464. [Google Scholar] [CrossRef]
- Leoni, E.; Legnani, P.P.; Bucci Sabattini, M.A.; Righi, F. Prevalence of Legionella spp. in swimming pool environment. Water Res. 2001, 35, 3749–3753. [Google Scholar] [CrossRef]
- Bilajac, L.; Vukić Lušić, D.; Doko Jelinić, J.; Rukavina, T. Microbiological and chemical indicators of water quality in indoor hotel swimming pools before and after training of swimming pool operators. J. Water Health 2011, 10, 108–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Official Gazette of the Republic of Croatia 59/2020. Regulation on Sanitary-Technical and Hygienic Conditions of Swimming Pools and on the Health Safety of Pool Waters; Ministry of Health: Zagreb, Croatia, 2020. [Google Scholar]
- Official Gazette of the Republic of Serbia 30/2017 and 97/2017. The Rulebook on Swimming Pool Water Quality; Ministry of Health: Belgrade, Serbia, 2018. [Google Scholar]
- Official Gazette of the Republic of Montenegro 57/2018 and 112/2020. Regulation on Sanitary-Technical and Hygienic Conditions, as Well as Conditions for Health Safety of Water for Recreational Needs and Other Waters of Public Health Interest; Ministry of Health: Podgorica, Montenegro, 2018. [Google Scholar]
- Official Gazette of the Federation of Bosnia and Herzegovina 50/2018. Regulation on Sanitary-Technical and Hygienic Conditions of Swimming Pools and Health Safety of Pool Waters; Ministry of Health: Sarajevo, Bosnia and Herzegovina, 2018. [Google Scholar]
- Official Gazette of the Republic of Slovenia 59/15; 86/15 and Amendments 52/18. Rules on the Minimum Hygiene Requirements for Bathing and Bathing Water in Swimming Pools; Ministry of Health: Ljubljana, Slovenia, 2015. [Google Scholar]
- American National Standards Institute. American National Standard for Water Quality in Public Pools and Spas ANSI/APSP/ICC-11 2019; American National Standards Institute: Washington, DC, USA, 2020; Available online: https://issuu.com/thephta/docs/apsp-11_2019 (accessed on 6 November 2021).








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vukić Lušić, D.; Maestro, N.; Cenov, A.; Lušić, D.; Smolčić, K.; Tolić, S.; Maestro, D.; Kapetanović, D.; Marinac-Pupavac, S.; Tomić Linšak, D.; et al. Occurrence of P. aeruginosa in Water Intended for Human Consumption and in Swimming Pool Water. Environments 2021, 8, 132. https://0-doi-org.brum.beds.ac.uk/10.3390/environments8120132
Vukić Lušić D, Maestro N, Cenov A, Lušić D, Smolčić K, Tolić S, Maestro D, Kapetanović D, Marinac-Pupavac S, Tomić Linšak D, et al. Occurrence of P. aeruginosa in Water Intended for Human Consumption and in Swimming Pool Water. Environments. 2021; 8(12):132. https://0-doi-org.brum.beds.ac.uk/10.3390/environments8120132
Chicago/Turabian StyleVukić Lušić, Darija, Nerma Maestro, Arijana Cenov, Dražen Lušić, Katarina Smolčić, Sonja Tolić, Daniel Maestro, Damir Kapetanović, Sandra Marinac-Pupavac, Dijana Tomić Linšak, and et al. 2021. "Occurrence of P. aeruginosa in Water Intended for Human Consumption and in Swimming Pool Water" Environments 8, no. 12: 132. https://0-doi-org.brum.beds.ac.uk/10.3390/environments8120132