
Monitoring Radon Levels in Hospital Environments. Findings of a Preliminary Study in the University Hospital of Sassari, Italy

 ,
,  , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design
2.3. Radon Concentration Measurement
2.4. Statistical Analysis
3. Results
3.1. Buildings Characteristics
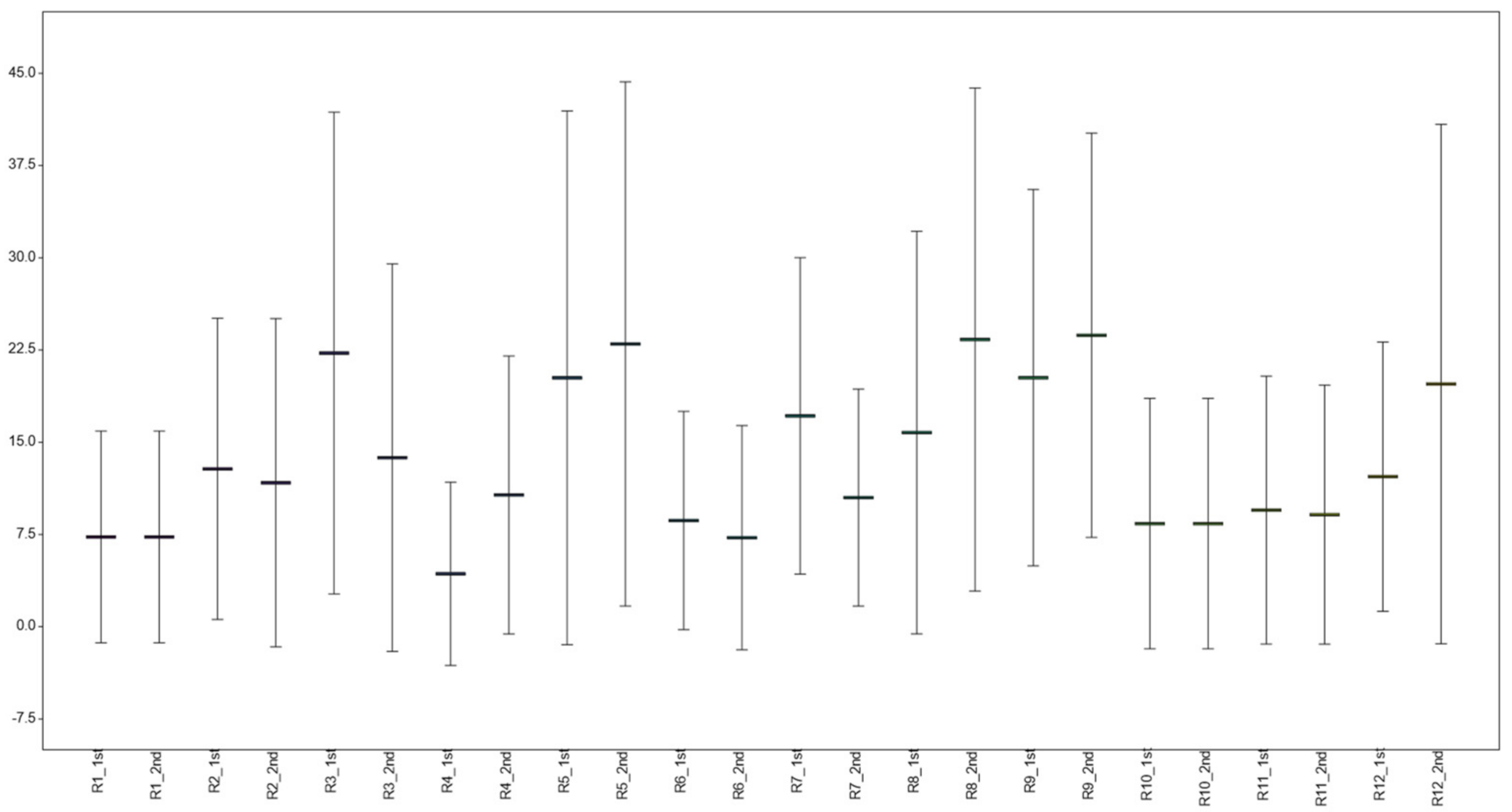
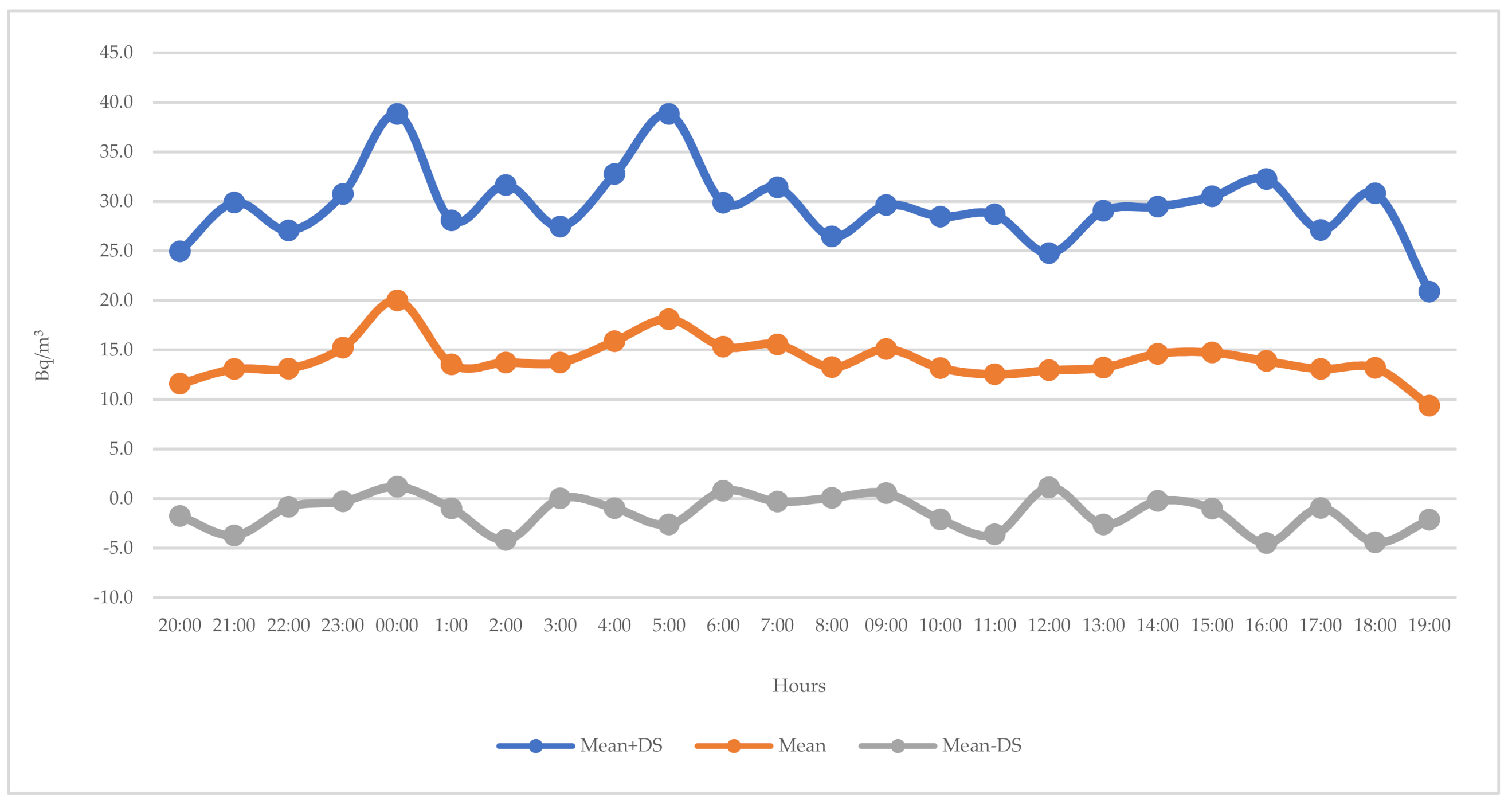
3.2. Radon Baseline Detection
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- World Health Organisation. Handbook on Indoor Radon—A Public Health Perspective; World Health Organization: Geneva, Switzerland, 2009; Available online: http://apps.who.int/iris/bitstream/handle/10665/44149/9789241547673_eng.pdf (accessed on 5 March 2021).
- National Research Council (US). Committee on Health Risks of Exposure to Radon (BEIR VI); National Academies Press (US): Washington, DC, USA, 1999; ISBN 0-309-05645-4. [Google Scholar]
- National Cancer Institute Radon and Cancer. 2016. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/substances/radon/radon-fact-sheet (accessed on 5 March 2021).
- International Agency for Research on Cancer. Man-Made Mineral Fibres and Radon. 1988. Available online: http://bases.bireme.br/cgi-bin/wxislind.exe/iah/online/?IsisScript=iah/iah.xis&src=google&base=WHOLIS&lang=p&nextAction=lnk&exprSearch=9283212436&indexSearch=ID (accessed on 5 March 2021).
- US Environmental Protection Agency Health Risk of Radon. 2016. Available online: https://www.epa.gov/radon/health-risk-radon (accessed on 5 March 2021).
- Oh, S.S.; Koh, S.; Kang, H.; Lee, J. Radon exposure and lung cancer: Risk in nonsmokers among cohort studies. Ann. Occup. Environ. Med. 2016, 28, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baeza, A.; García-Paniagua, J.; Guillén, J.; Montalbán, B. Influence of architectural style on indoor radon concentration in a radon prone area: A case study. Sci. Total Environ. 2018, 610–611, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Darby, S.; Hill, D.; Auvinen, A.; Baros-Dios, J.M.; Baysson, H.; Bochicchio, F.; Deo, H.; Falk, R.; Forastiere, F.; Hakama, M.; et al. Radon in homes and risk of lung cancer: Collaborative analysis of individual data from 13 European case-control studies. BMJ 2005, 330, 223. [Google Scholar] [CrossRef] [Green Version]
- Franci, D.; Aureli, T. Long- and short-term indoor radon survey in the Ardea municipality, south Rome. Radiat. Prot. Dosim. 2014, 162, 625–629. [Google Scholar] [CrossRef]
- Council Directive 2013/59/Euratom of 5 December 2013. Laying down Basic Safety Standards for Protection against the Dangers Arising from Exposure to Ionising Radiation, and Repealing Directives 89/618/Euratom, 90/641/Euratom, 96/29/Euratom, 97/43/Euratom and 2003/122/Euratom. Available online: https://ec.europa.eu/energy/sites/ener/files/documents/CELEX-32013L0059-EN-TXT.pdf (accessed on 5 March 2021).
- Commission Recommendation 90/143/Euratom of 21 February 1990 on the Protection of the Public against Indoor Exposure to Radon. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:31990H0143&from=SV (accessed on 5 March 2021).
- Decreto Legislativo del Governo n. 101 del 31/07/2020. D.Lgs. 241/2000. Attuazione della Direttiva 2013/59/Euratom, che Stabilisce Norme Fondamentali di Sicurezza Relative alla Protezione Contro i Pericoli Derivanti dall’esposizione alle Radiazioni Ionizzanti, e che Abroga le Direttive 89/618/Euratom, 90/641/Euratom, 96/29/Euratom, 97/43/Euratom e 2003/122/Euratom e Riordino della Normativa di Settore in Attuazione dell’articolo 20, Comma 1, Lettera a), della Legge 4 Ottobre 2019, n. 117. Available online: https://www.gazzettaufficiale.it/eli/id/2020/08/12/20G00121/sg (accessed on 9 February 2021).
- Decreto Legislativo del Governo n. 81 del 09/04/2008. D.Lgs. 81/2008. Attuazione dell’articolo 1 della Legge 3 Agosto 2007, n. 123, in Materia di Tutela della Salute e della Sicurezza nei Luoghi di Lavoro. Available online: http://www.parlamento.it/parlam/leggi/deleghe/08081dl.htm (accessed on 5 March 2021).
- Ministero della Salute. Piano Nazionale Radon. 2002. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2436_allegato.pdf (accessed on 5 March 2021).
- Regione Autonoma della Sardegna. Classificazione del Territorio Regionale della Sardegna con Individuazione delle Aree a Rischio Radon. 2019. Available online: http://www.sardegnaambiente.it/documenti/21_393_20190417132602.pdf (accessed on 5 March 2021).
- Samet, J.M.; Avila-Tang, E.; Boffetta, P.; Hannan, L.M.; Olivo-Marston, S.; Thun, M.J.; Rudin, C.M. Lung cancer in never smokers: Clinical epidemiology and environmental risk factors. Clin. Cancer Res. 2009, 15, 5626–5645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundy, A.; Brand, K.; Khandwala, F.; Poirier, A.; Tamminen, S.; Friedenreich, C.M.; Brenner, D.R. Lung cancer incidence attributable to residential radon exposure in Alberta in 2012. CMAJ Open. 2017, 5, E529–E534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Abente, G.; Núñez, O.; Fernández-Navarro, P.; Barros-Dios, J.M.; Martín-Méndez, I.; Bel-Lan, A.; Locutura, J.; Quindós, L.; Sainz, C.; Ruano-Ravina, A. Residential radon and cancer mortality in Galicia, Spain. Sci. Total Environ. 2018, 610–611, 1125–1132. [Google Scholar] [CrossRef] [PubMed]
- Bochicchio, F.; Žunić, Z.S.; Carpentieri, C.; Antignani, S.; Venoso, G.; Carelli, V.; Cordedda, C.; Veselinovic, N.; Tollefsen, T.; Bossew, P. Radon in indoor air of primary schools: A systematic survey to evaluate factors affecting radon concentration levels and their variability. Indoor Air 2014, 24, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Quarto, M.; Pugliese, M.; La Verde, G.; Loffredo, F.; Roca, V. Radon Exposure Assessment and Relative Effective Dose Estimation to Inhabitants of Puglia Region, South Italy. Int. J. Environ. Res. Public Health 2015, 12, 14948–14957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vimercati, L.; Fucilli, F.; Cavone, D.; Maria, L.D.; Birtolo, F.; Ferri, G.; Soleo, L.; Lovreglio, P. Radon Levels in Indoor Environments of the University Hospital in Bari-Apulia Region Southern Italy. Int. J. Environ. Res. Public Health 2018, 15, 694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Branco, P.T.B.S.; Nunes, R.A.O.; Alvim-Ferraz, M.C.M.; Martins, F.G.; Sousa, S.I.V. Children’s Exposure to Radon in Nursery and Primary Schools. Int. J. Environ. Res. Public Health 2016, 13, 386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vukotic, P.; Stojanovska, Z.; Antovic, N. Developing a method for predicting radon concentrations above a reference level in new montenegrin buildings. J Environ. Radioact. 2021, 227, 106500. [Google Scholar] [CrossRef] [PubMed]
- Stanley, F.K.T.; Irvine, J.L.; Jacques, W.R.; Salgia, S.R.; Innes, D.G.; Winquist, B.D.; Torr, D.; Brenner, D.R.; Goodarzi, A.A. Radon exposure is rising steadily within the modern North American residential environment, and is increasingly uniform across seasons. Sci. Rep. 2019, 9, 18472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firenze, A.; Calamusa, G.; Amodio, E.; Morici, M.; Di Paquale, M.; Mazzucco, W.; Azara, A.; Muresu, E.; Dettori, M.; Maida, G.; et al. Evaluation of radon levels in indoor gymnasia of Palermo (Sicily) and Sassari (Sardinia). Ital. J. Public Health 2009, 6, 316–322. [Google Scholar]
- Azara, A.; Dettori, M.; Castiglia, P.; Piana, A.; Durando, P.; Parodi, V.; Salis, G.; Saderi, L.; Sotgiu, G. Indoor Radon Exposure in Italian Schools. Int. J. Environ. Res. Public Health 2018, 15, 749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Istituto Superiore di Sanità (ISS). EpiCentro. Radon—Aspetti Epidemiologici. Available online: https://www.epicentro.iss.it/radon/epidemiologia (accessed on 5 March 2021).
- Istituto Superiore per la Prevenzione e la Sicurezza del Lavoro (ISPESL). Il Radon in Italia: Guida Per il Cittadino. 2007. Available online: http://www.salute.gov.it/imgs/C_17_opuscoliPoster_160_allegato.pdf (accessed on 5 March 2021).
- Barros, N.G.; Steck, D.J.; Field, R.W. A comparison of winter short-term and annual average radon measurements in basements of a radon-prone region and evaluation of further radon testing indicators. Health Phys. 2014, 106, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Mnich, Z.; Karpińska, M.; Kapała, J.; Kozak, K.; Mazur, J.; Birula, A.; Antonowicz, A. Radon concentration in hospital buildings erected during the last 40 years in Białystok, Poland. J. Environ. Radioact. 2004, 75, 225–232. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Building Characteristics | Number (%) | |
|---|---|---|
| Construction period | <1900 | 0/14 (0.0) |
| 1900–1950 | 3/14 (21.4) | |
| 1951–1964 | 0/14 (0.0) | |
| 1965–1979 | 6/14 (42.9) | |
| ≥1980 | 5/14 (35.7) | |
| Underground renovation | 6/14 (42.9) | |
| Type of structure | Floor below ground level | 3/14 (21.4) |
| Partially underground | 2/14 (14.3) | |
| 2 basement walls | 9/14 (64.3) | |
| Wall material | Cement | 12/14 (85.7) |
| Stone | 1/14 (7.1) | |
| Wood | 0/14 (0.0) | |
| Coated metal | 1/14 (7.1) | |
| Flooring material | Cement | 8/14 (57.1) |
| Floor tiles | 4/14 (28.6) | |
| Wood | 0/14 (0.0) | |
| Earth | 0/14 (0.0) | |
| Linoleum | 2/14 (14.3) | |
| Floor in direct contact with ground | 14/14 (100.0) | |
| External entrance doors | 3/14 (21.4) | |
| Windows | 7/14 (50.0) | |
| Underground walls adjacent to a cavity wall | Totally | 3/14 (21.4) |
| Partially | 3/14 (21.4) | |
| None | 7/14 (50.0) | |
| Underground rocky walls | 0/14 (0.0) | |
| Water infiltration/Damp | 4/14 (28.6) | |
| Wind exposure | Low | 2/14 (14.3) |
| Medium | 3/14 (21.4) | |
| High | 1/14 (7.1) | |
| Nil | 8/14 (57.1) | |
| Sun exposure | Low | 1/14 (7.1) |
| Medium | 6/14 (42.9) | |
| High | 0/14 (0.0) | |
| Nil | 7/14 (50.0) | |
| Exposed Piping | None | 3/11 (21.4) |
| In side wall | 10/11 (90.9) | |
| In ceiling | 1/11 (9.1) | |
| Rooms | Average Values (Bq/m3) | Standard Deviation (Bq/m3) | Highest Levels (Bq/m3) |
|---|---|---|---|
| Bunker 1 | 464.2 | 1843.8 | 12,136.0 |
| Bunker 2 | 1670.5 | 6232.2 | 36,963.0 |
| Rooms | Average Values (Bq/m3) | Standard Deviation (Bq/m3) | Highest Levels (Bq/m3) |
|---|---|---|---|
| Post-operative room | 7.3 | 8.6 | 48.1 |
| Storage room | 12.3 | 12.8 | 59.2 |
| Outpatients cinic | 18.8 | 18.6 | 74.0 |
| Pre-MRI scan room | 7.5 | 10.0 | 37.0 |
| Dentistry department | 21.6 | 21.5 | 88.8 |
| Laboratory 1 | 7.8 | 9.0 | 37.0 |
| Laboratory 2 | 14.8 | 12.0 | 48.1 |
| Laboratory 3 | 18.4 | 18.2 | 85.1 |
| Archive 1 | 21.6 | 15.8 | 74.0 |
| Archive 2 | 8.4 | 10.1 | 37.0 |
| Glassware washing room | 9.3 | 10.7 | 37.0 |
| Disposal room | 15.2 | 16.2 | 85.1 |
| Variable | p-Value |
|---|---|
| Contruction period | 0.779 |
| Underground renovation | 0.438 |
| Type of structure | 0.856 |
| Wall material | 0.584 |
| Flooring material | 0.366 |
| External entrance doors | 0.186 |
| Presence of windows | 0.035 |
| Underground walls | 0.406 |
| Water infiltration/Damp | 0.066 |
| Wind exposure | 0.196 |
| Sun exposure | 0.035 |
| Exposed piping | 0.051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deiana, G.; Dettori, M.; Masia, M.D.; Spano, A.L.; Piana, A.; Arghittu, A.; Castiglia, P.; Azara, A. Monitoring Radon Levels in Hospital Environments. Findings of a Preliminary Study in the University Hospital of Sassari, Italy. Environments 2021, 8, 28. https://0-doi-org.brum.beds.ac.uk/10.3390/environments8040028
Deiana G, Dettori M, Masia MD, Spano AL, Piana A, Arghittu A, Castiglia P, Azara A. Monitoring Radon Levels in Hospital Environments. Findings of a Preliminary Study in the University Hospital of Sassari, Italy. Environments. 2021; 8(4):28. https://0-doi-org.brum.beds.ac.uk/10.3390/environments8040028
Chicago/Turabian StyleDeiana, Giovanna, Marco Dettori, Maria Dolores Masia, Antonio Lorenzo Spano, Andrea Piana, Antonella Arghittu, Paolo Castiglia, and Antonio Azara. 2021. "Monitoring Radon Levels in Hospital Environments. Findings of a Preliminary Study in the University Hospital of Sassari, Italy" Environments 8, no. 4: 28. https://0-doi-org.brum.beds.ac.uk/10.3390/environments8040028