Postoperative Quality of Life after Single-Visit Root Canal Treatment Performed with Reciprocating Shaping Systems: An Observational Study

 , , ,
, , ,  , ,
, ,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Size Calculation
2.2. Clinical Intervention
- (1)
- During canal scouting with a size #10 stainless-steel K-file,
- (2)
- At the end of glide path with a size #15 stainless-steel K-file, and
- (3)
- 3 mm before reaching the WL during shaping with a size #15 stainless-steel K-file.
2.3. Outcomes
2.4. Statistical Methods
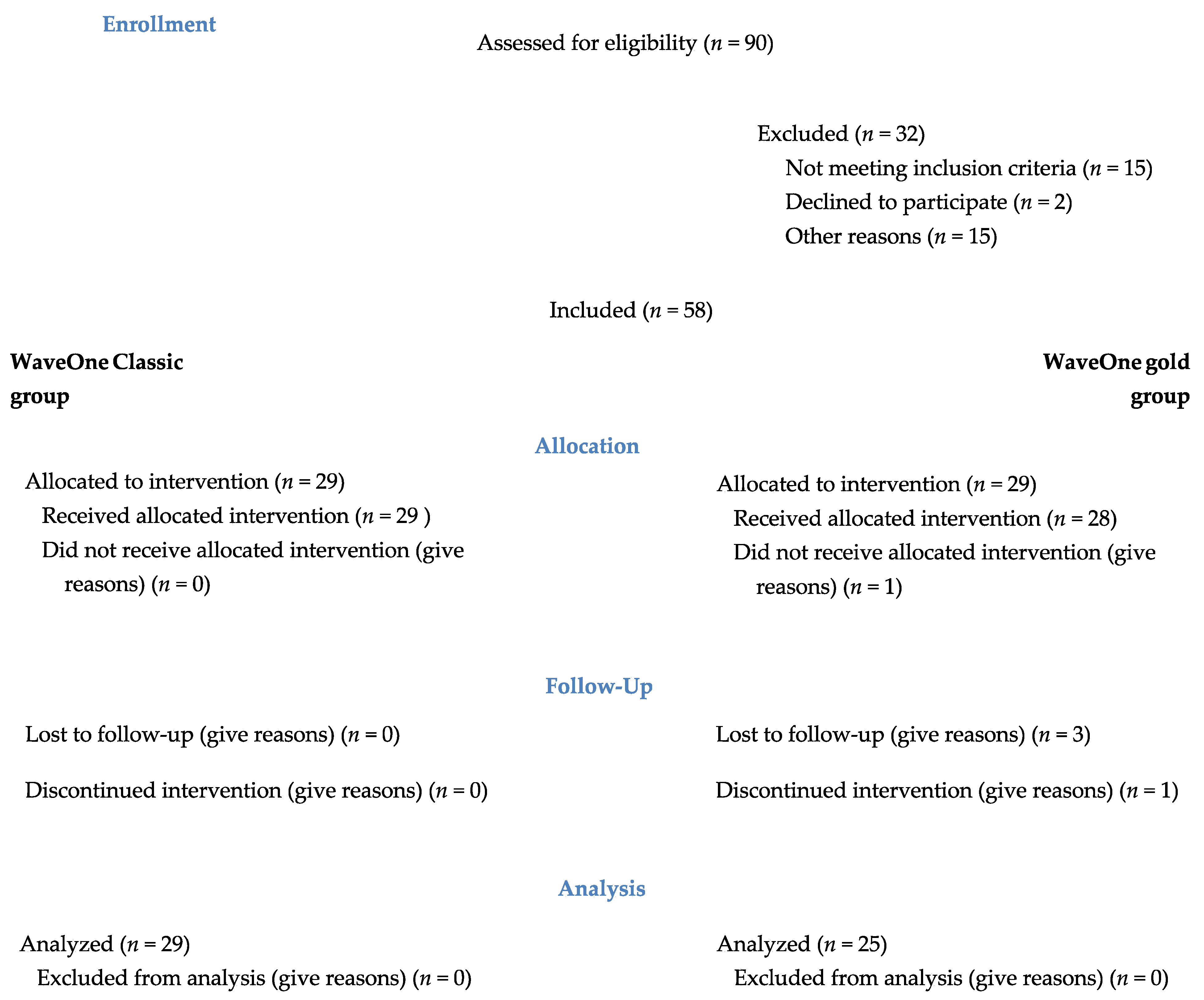
3. Results
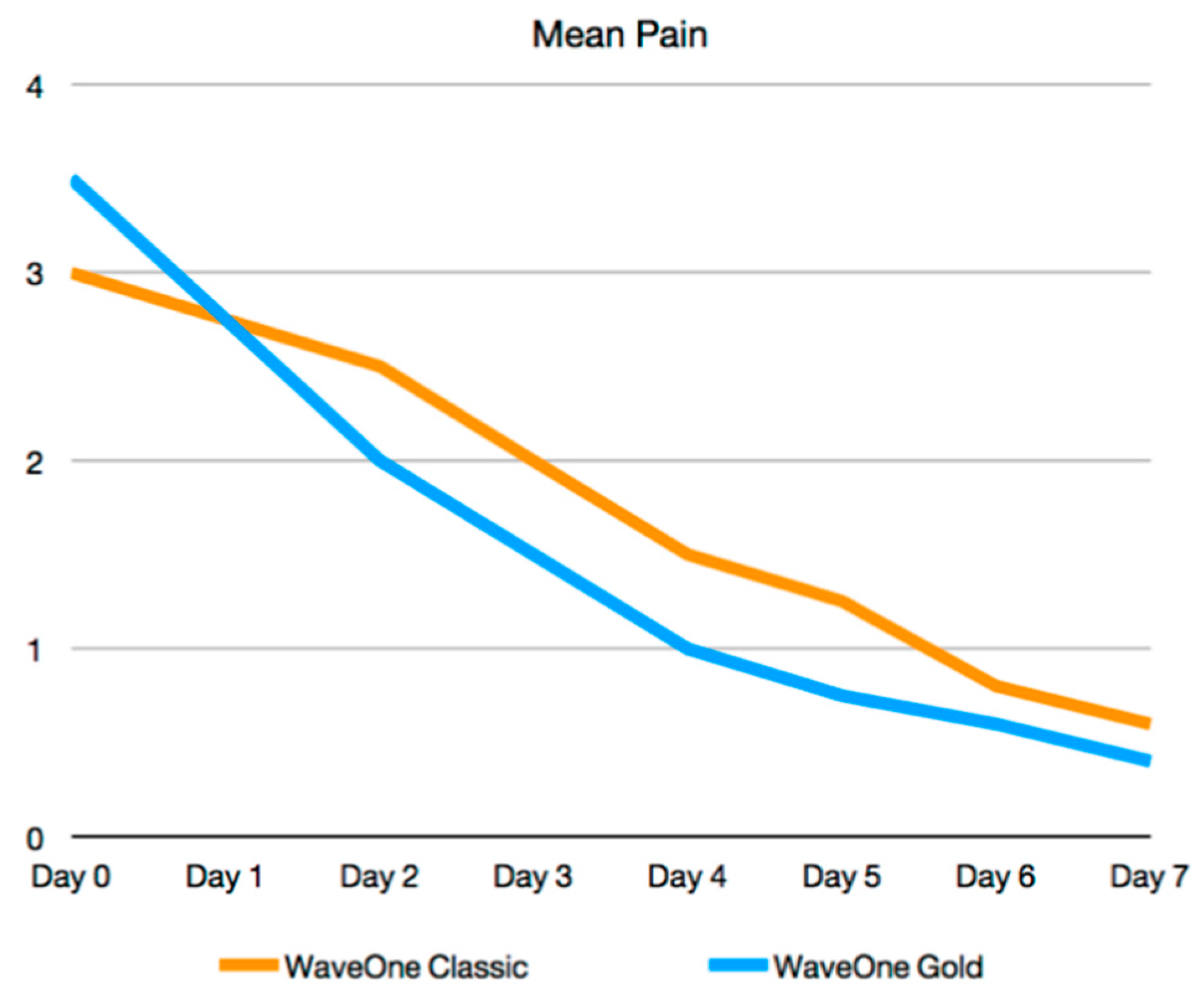
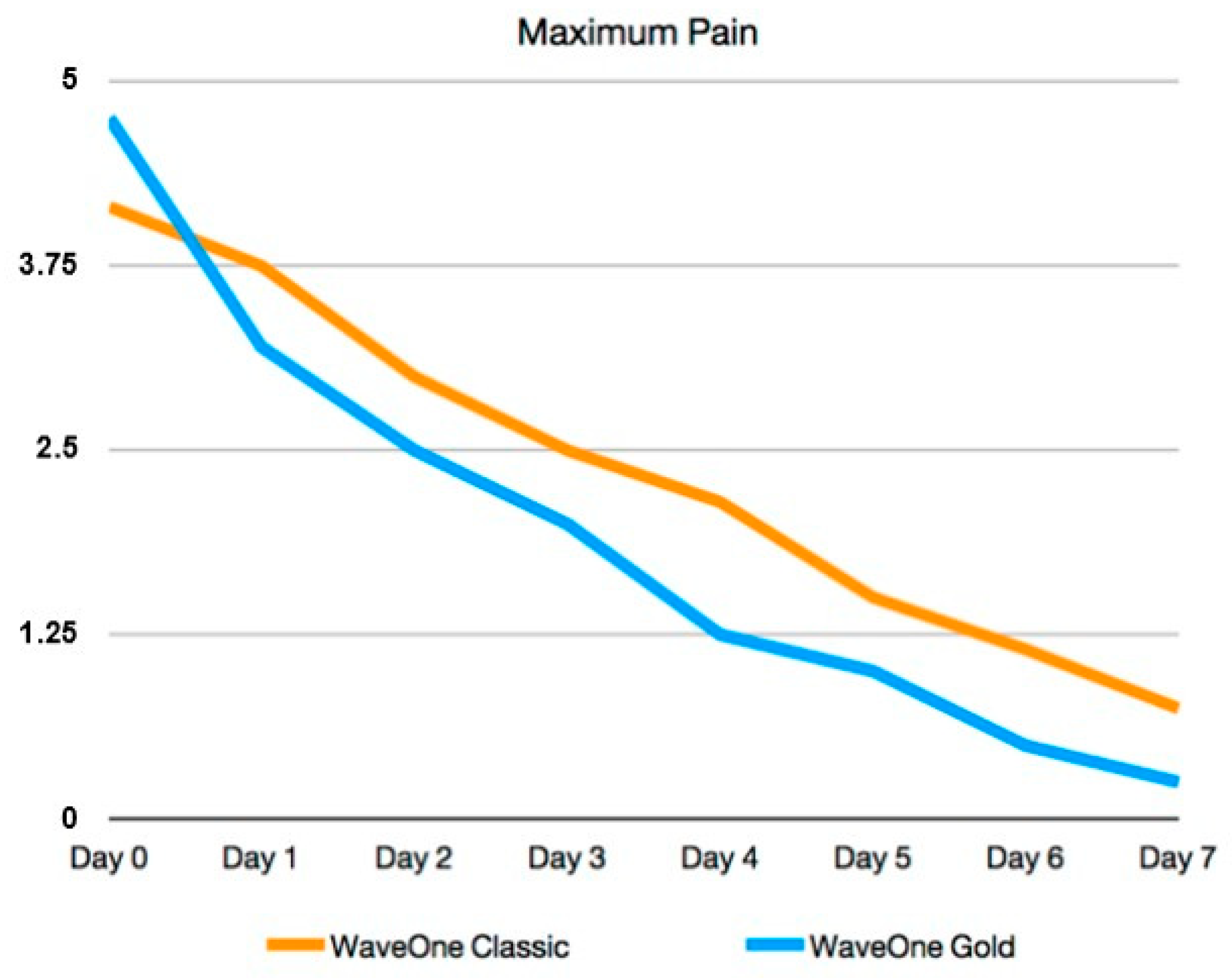
3.1. Postoperative Pain, Analgesic Intake, and Pain Stop Value
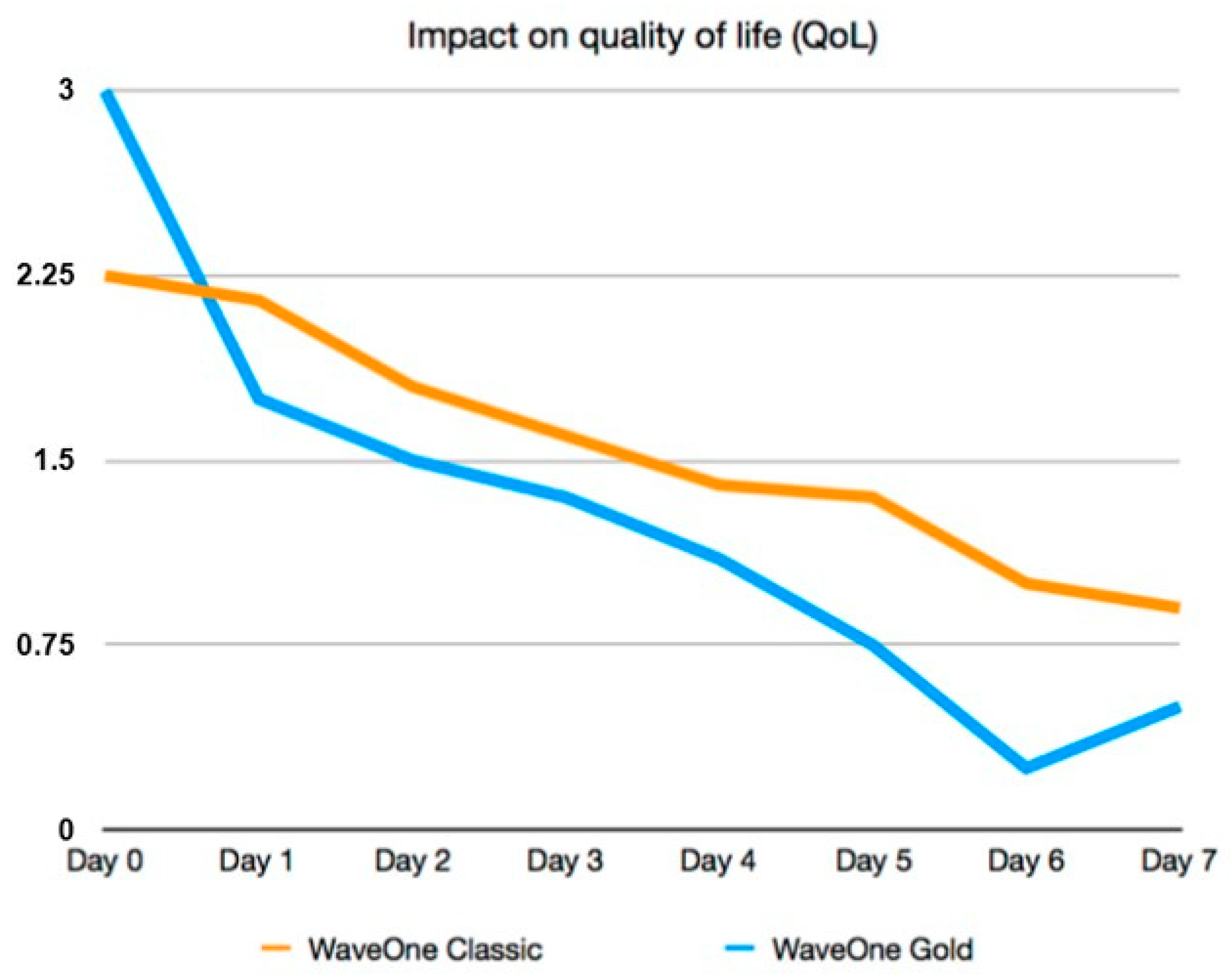
3.2. Postoperative Qualty of Life Indicators
3.3. Number of Pecking Motions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
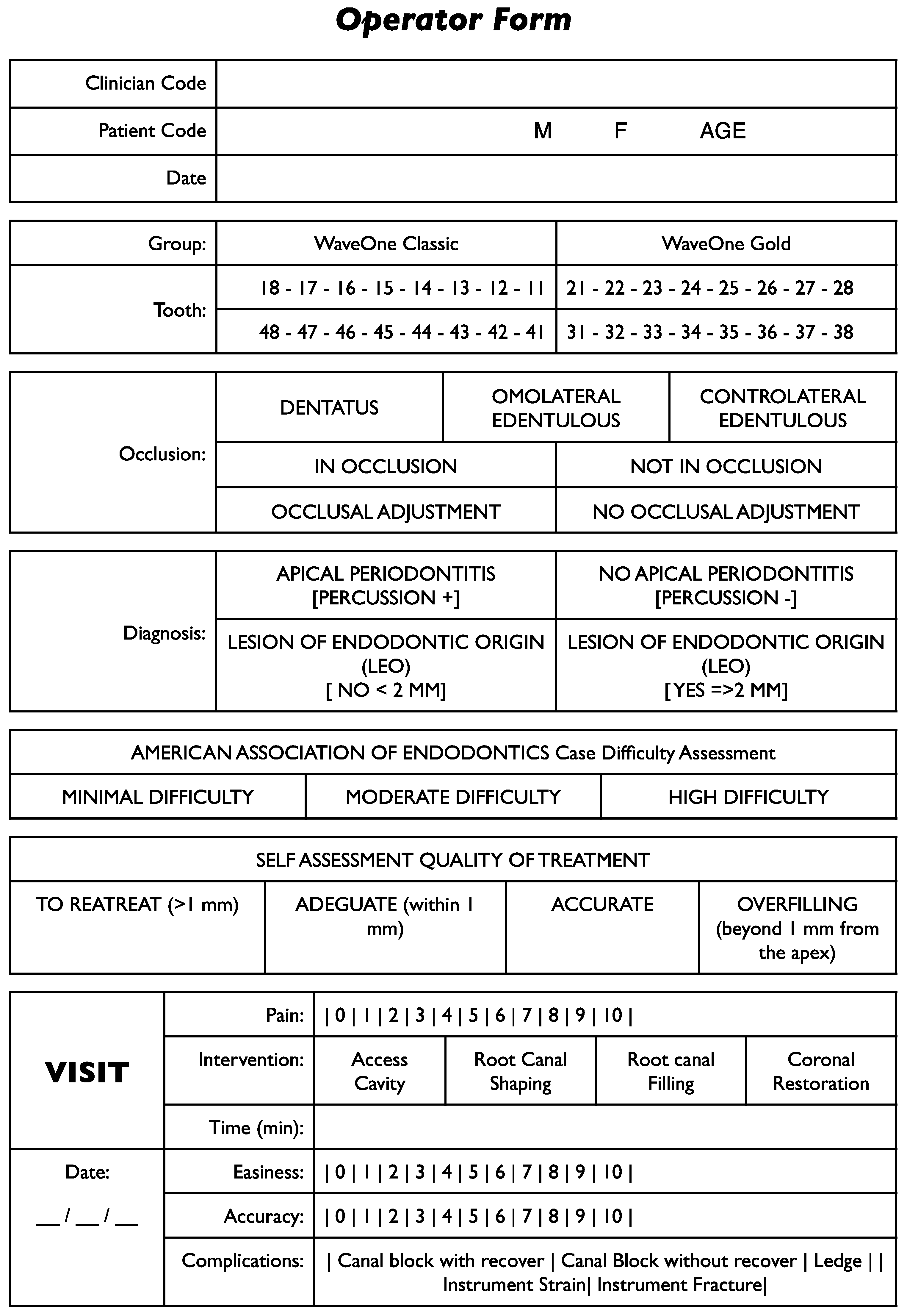
Appendix A


Appendix B

Appendix C

References
- WHOQOL. The world health organization quality of life assessment. Position paper from the world health organization. Soc. Sci. Med. 1995, 41, 1405. [Google Scholar]
- McGrath, C.; Newson, P.R. Patient centred measures in dental practice: Quality of life. Dent. Update 2007, 34, 41–42. [Google Scholar] [CrossRef] [PubMed]
- Dugas, N.N.; Lawrence, H.P.; Teplitsky, P.; Friedman, S. Quality of life and satisfaction outcomes of endodontic treatment. J. Endod. 2002, 28, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Gatten, D.L.; Riedy, C.A.; Hong, S.K.; Johnson, J.D.; Cohenca, N. Quality of life od endodontically treated versus implant treated patients: A University-based qualitative research study. J. Endod. 2011, 37, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Tsesis, I.; Shoshani, Y.; Givol, N.; Yahalom, R.; Fuss, Z.; Taicher, S. Comparison of quality of life after surgical endodontic treatment using two techniques: A prospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 99, 367–371. [Google Scholar] [CrossRef]
- Taschieri, S.; Corbella, S.; Tsesis, I.; Del Fabbro, M. Impact of the use of plasma rich in growth factors (PRGF) on the quality of life of patients treated with endodontic surgery when a perforation of sinus membrane occurred. A comparative study. Oral Maxillofac. Surg. 2014, 18, 43–52. [Google Scholar] [CrossRef]
- AAE. Public Education Report: Surveys Document More People Choosing Root Canal Therapy over Extraction; American Association of Endodontics: Chicago, IL, USA, 1987. [Google Scholar]
- Friedman, S. Prognosis of initial endodontic therapy. Endod. Top. 2002, 2, 59–88. [Google Scholar] [CrossRef] [Green Version]
- Pak, J.G.; White, S.N. Pain prevalence and severity before, during, and after root canal treatment: A systematic review. J. Endod. 2011, 37, 32–36. [Google Scholar] [CrossRef]
- Di Renzo, A.; Gresla, T.; Johnson, B.R.; Rogers, M.; Tucker, D.; Be Gole, E.A. Postoperative pain after 1- and 2-visit root canal therapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 93, 605–610. [Google Scholar] [CrossRef] [Green Version]
- Torabinejad, M.; Cymerman, J.J.; Frankson, M.; Lemon, R.R.; Maggio, J.D.; Schilder, H. Effectiveness of various medications on postoperative pain following complete instrumentation. J. Endod. 2005, 31, 171–176. [Google Scholar] [CrossRef]
- Liu, P.; McGrath, C.; Cheung, G. What are the key endodontic factors associated with oral health-related quality of life? Int. Endod. J. 2014, 47, 238–245. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; McGrath, C.; Cheung, G. Quality of life and psychological well-being among endodontic patients: A case control study. Aust. Dent. J. 2012, 57, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Pasqualini, D.; Mollo, L.; Soctti, N.; Cantatore, G.; Castellucci, A.; Migliaretti, G.; Berutti, E. Postoperative pain after manual and mechanical glide path: A randomized clinical trial. J. Endod. 2012, 38, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Siqueira, J.F., Jr.; Rocas, I.N.; Favieri, A.; Machado, A.G.; Gahyva, S.G.; Oliceira, J.C.M.; Abad, E.C. Incidence of postoperative pain after intracanal procedures based on an antimicrobial strategy. J. Endod. 2002, 28, 457–460. [Google Scholar] [CrossRef]
- Tanalp, J.; Güngör, T. Apical extrusion of debris: A literature review of an inherent occurrence during root canal treatment. Int. Endod. J. 2014, 47, 211–221. [Google Scholar] [CrossRef]
- Berutti, E.; Chiandussi, G.; Paolino, D.S.; Scotti, N.; Cantatore, G.; Castellucci, A.; Pasqualini, D. Canal Shaping with WaveOne Primary reciprocating file and ProTaper system: A comparative study. J. Endod. 2012, 28, 505–509. [Google Scholar] [CrossRef] [Green Version]
- Bürklein, S.; Schäfer, E. Apically extruded debris with reciprocating single-file and full sequence rotary instrumentation system. J. Endod. 2012, 38, 850–852. [Google Scholar] [CrossRef]
- Nekoofar, M.H.; Sheykhrezae, M.S.; Meraji, N.; Jamee, A.; Shirvani, A.; Jamee, J.; Dummer, P.M. Comparison of the effect of root canal preparation by using WaveOne and ProTaper on postoperative pain: A randomized clinical trial. J. Endod. 2015, 41, 575–578. [Google Scholar] [CrossRef]
- Bürklein, S.; Hinschitza, K.; Dammaschke, T.; Schäfer, E. Shaping ability and cleaning effectiveness of two single file systems in severely curved root canals of extracted teeth: Reciproc and WaveOne versus Mtwo and ProTaper. Int. Endod. J. 2012, 45, 449–461. [Google Scholar] [CrossRef]
- Caviedes-Bucheli, J.; Castellanos, F.; Vasquez, N.; Ulate, E.; Munoz, H.R. The influence of two reciprocating single file and two rotary-file systems on the apical extrusion of debris and its biological relationship with symptomatic apical periodontitis. A systematic review and meta-analysis. Int. Endod. J. 2015, 49, 255–270. [Google Scholar] [CrossRef]
- Pasqualini, D.; Corbella, S.; Alovisi, M.; Taschieri, S.; Del Fabbro, M.; Migliaretti, G.; Carpegna, G.C.; Scotti, N.; Berutti, E. Postoperative quality of life following single-visit root canal treatment performed by rotary or reciprocating instrumentation: A randomized clinical trial. Int. Endod. J. 2015, 49, 1030–1039. [Google Scholar] [CrossRef]
- Hou, X.M.; Su, Z.; Hou, B.X. Post endodontic pain following single-visit root canal preparation with rotary vs reciprocating instruments: A meta-analysis of randomized clinical trials. BMC Oral Health 2017, 17, 86. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Med. Assoc. 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- American Association of Endodontists. AAE Endodontic Case Difficulty Assessment Form and Guidelines. 2006. [WWW document]. Available online: https://www.aae.org/specialty/wp-content/uploads/sites/2/2019/02/19AAE_CaseDifficultyAssessmentForm.pdf (accessed on 16 November 2020).
- Torabinejad, M.; Anderson, P.; Bader, J.; Brown, L.J.; Chen, L.H.; Goodacre, C.J.; Kattadiyil, M.T.; Kutsenko, D.; Lozada, J.; Patel, R.; et al. Outcomes of root canal treatment and restoration, implant-supported single crowns, fixed partial dentures, and extraction without replacement: A systematic review. J. Prosthet. Dent. 2007, 98, 285–311. [Google Scholar] [CrossRef]
- McGrath, C.; Lam, O.; Lang, N. An evidence-based review of patient-reported outcome measures in dental implant research among dentate subjects. J. Clin. Periodontol. 2012, 39 (Suppl. 12), 193–201. [Google Scholar] [CrossRef]
- Arias, A.; de la Macorra, J.C.; Hidalgo, J.J.; Azabal, M. Predictive models of pain following root canal treatment: A prospective clinical study. Int. Endod. J. 2013, 46, 784–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caviedes-Bucheli, J.; Moreno, J.O.; Carreno, C.P.; Delgado, R.; Garcia, D.J.; Solano, J.; Dia, E.; Munoz, H.R. The effect of single-file reciprocating systems on Substance P and Calcitonin gene-related peptide expression in human periodontal ligament. Int. Endod. J. 2013, 46, 419–426. [Google Scholar] [CrossRef]
- Ibrahim, E.Y.; Kurnaz, S.; Tunca, Y.M. Maintaining apical patency does not increase postoperative pain in molars with necrotic pulp and apical periodontitis: A randomized clinical trial. J. Endod. 2019, 44, 335–340. [Google Scholar]
- Hamasha, A.A.; Hatiwsh, A. Quality of life and satisfaction of patients after nonsurgical primary root canal treatment provided by undergraduate students, graduate students and endodontic specialists. Int. Endod. J. 2013, 46, 1131–1139. [Google Scholar] [CrossRef]
- Caviedes-Bucheli, J.; Azuero-Holguin, M.M.; Gutierrez-Sanchez, L.; Higuerey-Bermudez, F.; Pereira-Nava, V.; Lombana, N.; Munoz, H.R. The effect of three different rotary instrumentation systems on Substance P and Calcitonin gene-related peptide expression in human periodontal ligament. J. Endod. 2010, 36, 1938–1942. [Google Scholar] [CrossRef]
- Wong, A.W.-Y.; Zhang, S.; Li, S.K.-Y.; Zhang, C.; Chu, C.H. Clinical studies on core-carrier obturation: Asystematic review and metanalysis. BMC Oral Health 2017, 17, 167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figini, L.; Lodi, G.; Gorni, F.; Gagliani, M. Single versus multiple visits for endodontic treatment of permanent teeth: A Cochrane systematic review. J. Endod. 2008, 34, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Manfredi, M.; Figini, L.; Gagliani, M.; Lodi, G. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst. Rev. 2016, 12, CD005296. [Google Scholar] [CrossRef] [PubMed]
- Keskin, C.; Sarıyılmaz, E. Apically extruded debris and irrigants during root canal filling material removal using Reciproc Blue, WaveOne Gold, R-Endo and ProTaper Next systems. J. Dent. Res. Dent. Clin. Dent. Prospect. 2018, 12, 272–276. [Google Scholar] [CrossRef]
- Stringheta, C.P.; Bueno, C.E.S.; Kato, A.S.; Freire, L.G.; Iglecias, E.F.; Santos, M.; Pelegrine, R.A. Micro-computed tomographic evaluation of the shaping ability of four instrumentation systems in curved root canals. Int. Endod. J. 2019, 52, 908–916. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 | Group 2 | |
|---|---|---|
| Canal Scouting | K-File #10 | K-File #10 |
| Mechanical Glide Path | Proglider #16.02 | Proglider #16.02 |
| Irrigants | NaOCl 5% EDTA 10% | NaOCl 5% EDTA 10% |
| Root Canal Shaping | WaveOne Classic Primary (25.08) | WaveOne Gold Primary (25.07) |
| WL Measurement | Electronic and Radiographic | Electronic and Radiographic |
| Root Canal Filling | Thermafil Technique | Thermafil Technique |
| Pre-Operative Status | Group 1 (n = 29) WOC | Group 2 (n = 25) WOG | p |
|---|---|---|---|
| AAE difficulty (minimal/moderate/high) (n) | 8/20/1 | 6/18/1 | NS |
| Type of tooth (maxillary molars/mandibular molars) | 18/11 | 10/15 | NS |
| Pulp necrosis | 100% | 100% | NS |
| Symptomatic apical periodontitis | 54.2% | 48.0% | NS |
| LEO prevalence | 25.0% | 20.0% | NS |
| Pain prevalence | 83.3% | 80.0% | NS |
| Mean pain score (VAS) | 3.84 ± 3.12 | 2.90 ± 2.51 | NS |
| Maximum pain score (VAS) | 5.24 ± 3.76 | 4.28 ± 3.30 | NS |
| Quality of life (LS) | 2.92 ± 2.60 | 2.10 ± 2.92 | NS |
| Group 1 (n = 29) WOC | Group 2 (n = 25) WOG | p | |
|---|---|---|---|
| Age (<30/30–45/45–60/>60) | 9/10/7/3 | 8/9/6/2 | NS |
| Gender (M/F) | 12/17 | 10/15 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Multari, S.; Alovisi, M.; Berutti, E.; Corbella, S.; Taschieri, S.; Carpegna, G.; Scotti, N.; Comba, A.; Pasqualini, D. Postoperative Quality of Life after Single-Visit Root Canal Treatment Performed with Reciprocating Shaping Systems: An Observational Study. Appl. Sci. 2021, 11, 273. https://0-doi-org.brum.beds.ac.uk/10.3390/app11010273
Multari S, Alovisi M, Berutti E, Corbella S, Taschieri S, Carpegna G, Scotti N, Comba A, Pasqualini D. Postoperative Quality of Life after Single-Visit Root Canal Treatment Performed with Reciprocating Shaping Systems: An Observational Study. Applied Sciences. 2021; 11(1):273. https://0-doi-org.brum.beds.ac.uk/10.3390/app11010273
Chicago/Turabian StyleMultari, Stefania, Mario Alovisi, Elio Berutti, Stefano Corbella, Silvio Taschieri, Giorgia Carpegna, Nicola Scotti, Allegra Comba, and Damiano Pasqualini. 2021. "Postoperative Quality of Life after Single-Visit Root Canal Treatment Performed with Reciprocating Shaping Systems: An Observational Study" Applied Sciences 11, no. 1: 273. https://0-doi-org.brum.beds.ac.uk/10.3390/app11010273