
Determination of the Vertical Dimension and the Position of the Occlusal Plane in a Removable Prosthesis Using Cephalometric Analysis and Golden Proportion

 ,
,  , , ,
, , , 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Target Questions
- –
- How to obtain a functional and aesthetic mobile prosthesis?
- –
- How to choose the correct vertical dimension for the patient and the correct occlusal plane of the prosthesis?
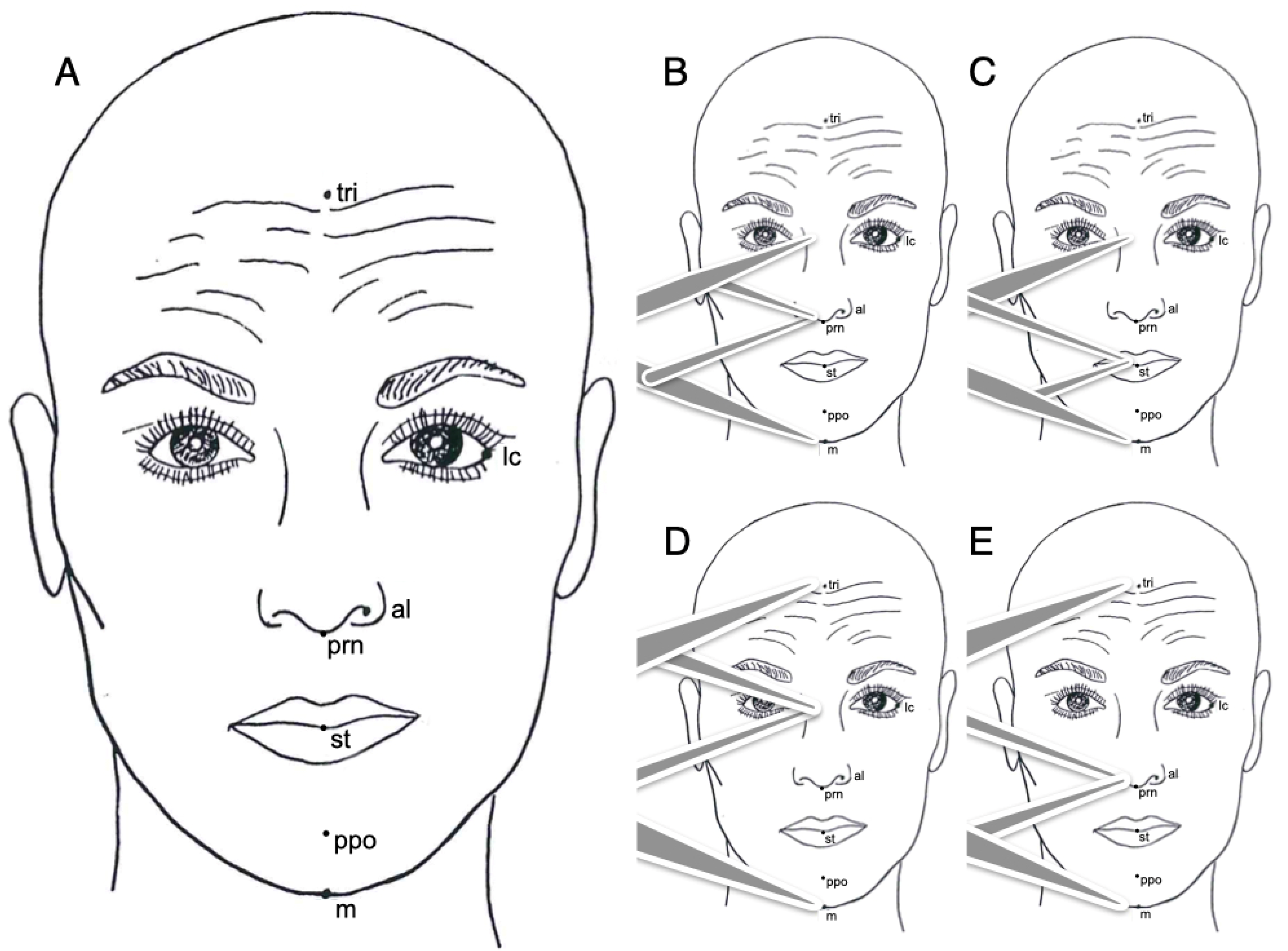
- Trichion (tri): is the point on the hairline in the midline of the forehead.
- Lateral canthus of the eyes (lc): is the point at the outer commissure of the eye fissure.
- Ala of the nose (al): the most lateral point on alar contour.
- Pronasalis (prn): the most anterior point of the tip of the nose.
- Stomion (st): the contact point of the upper and lower lips in the mid-sagittal line when the mouth is closed.
- Propogonion (ppo): the most anterior point of the chin profile.
- Menton (m): the lowest point in the midline on the lower border of the chin.
- Basion (Ba): located at the anterior border of the foramen magnun.
- Nasion (N): selected at the frontal margin of the fronto-nasal suture.
- Porion (P): selected at the center of the superior border of the ear canal.
- Orbitale (O): located at the lower rim of the orbit.
- Pterygoid point (Pt): selected at the lower border of the Foramen Rotundum at the origin of Pterygoid buttress.
- Center cranium (Cc): is the intersection between Frankfort Plane and Basion-Nasion Plane.
- Anterior Nasal Spine (ANS): is selected on the most forward point of maxillae bones.
- Point A (A): selected at the deepest curvature of the contour below the anterior nasal spine.
- Pogonion (Po): defined as the most anterior point on the outline of the chin.
- Protuberance menti (Pm): selected where the symphyseal cortical plate ends and where the supramental contour starts to recede into the alveolar process.
- Gnathion (Gn): selected cephalometrically and constructed by the intersection of the Facial Plane with the Mandibular Plane.
- Menton (M): is the lowest point on the inferior border of the symphysis.
- Xi: is selected as a centroid reference for the ramus.
- Subgonion (Sgo): is selected at the lower border of the angle of the mandible.
- Upper incisor (A1): representative position of the mean of the upper central incisors traced with the Ricketts template.
- Lower incisor (B1): representative position of the mean of the lower central incisors traced with the Ricketts template.
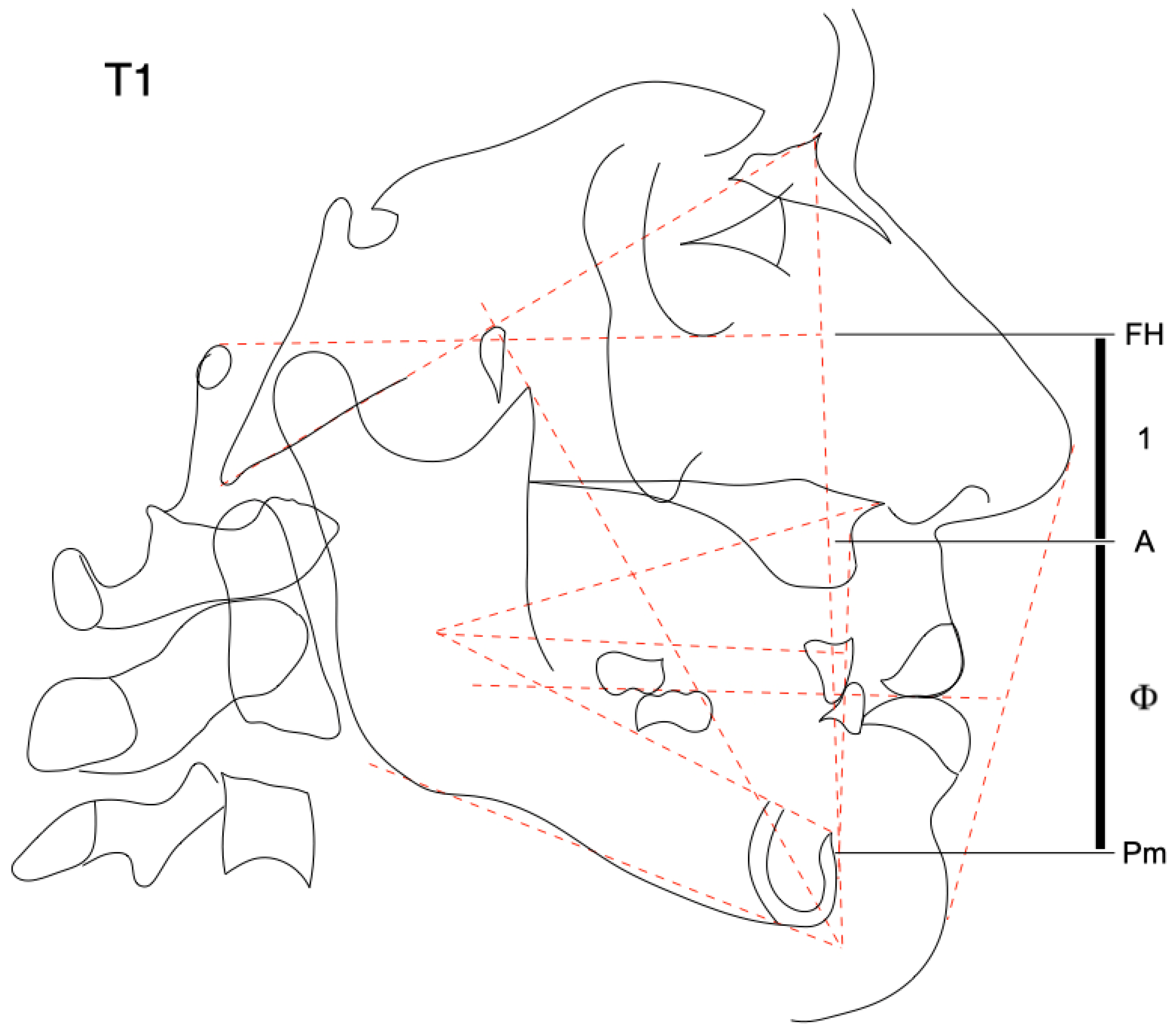
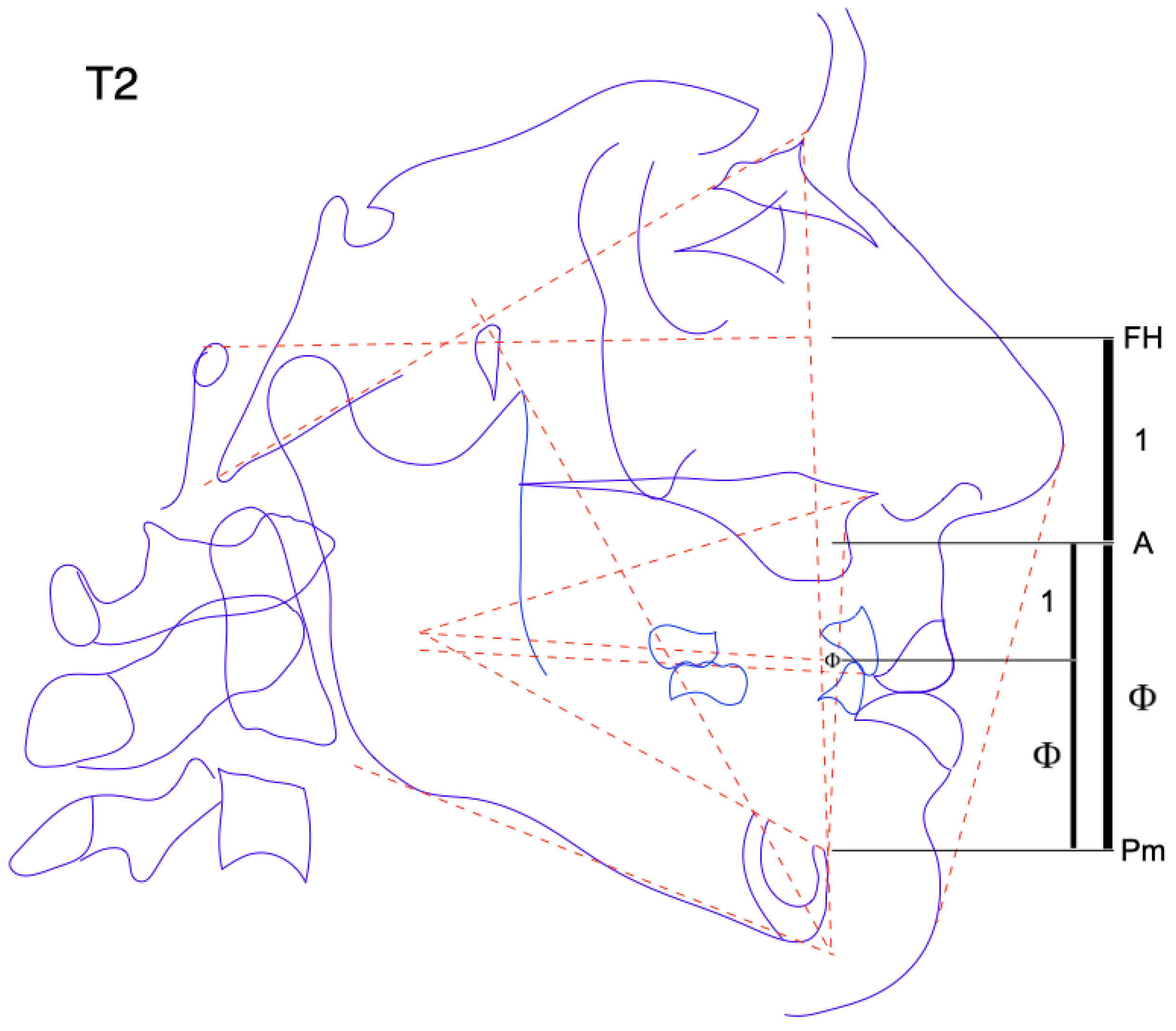
- Lower incisor divine point (Φ): selected in golden proportion between point A and Pm. The height from incisal edge to Pm should be 0.618.
- Upper first molar (A6): selected as the bisection of the two sides. Traced with the Ricketts template.
- Lower first molar (B6): selected as the mesial margin of the lower first molar for anterior reference and vertically as the bisection of the two sides and of the first molar occlusion. Traced with the Ricketts template.
- Lower second molar (B7): selected as the mesial margin of the lower second molar for anterior reference and vertically as the bisection of the two sides and of the second molar occlusion. Traced with the Ricketts template.
- Zygomatic arch point (Za): Zygomatic arch center.
- B6L: lower left first molar
- B6R: lower right first molar
- Basion-Nasion plane: Ba-N
- Frankfort Plane: P-O
- True Buccal Occlusal Plane (TBOP): line through the bisection of the buccal cusp of premolars and first molar.
- Divine Occlusal Plane (DOP): traced from Xi to Lower Incisor Divine point (Φ).
- Facial plane: N-Po
- Mandibular plane: Sgo-M
- Facial axis: Cc-Gn
- Corpus axis: Xi-Pm
- Org line: Xi-ANS
- Denture plane: A-Po
- Esthetic line: prn-ppo
- Central facial direction (Facial axis-BaNa plane) (degrees);
- Lower facial height (Corpus axis-Org line) (degrees);
- Incisor overjet (mm);
- Incisor overbite (mm);
- Horizontal B1 position (B1-denture plane) (mm);
- Lower lip protrusion (lower lip to E line) (mm)
- Zygomatic plane (ZA-ZA): represents a frontal Frankfort plane.
- Frontal occlusal plane (B6L to B6R): a bisection of the molar occlusion connection represents a fronto-occlusal plane.
3. Results
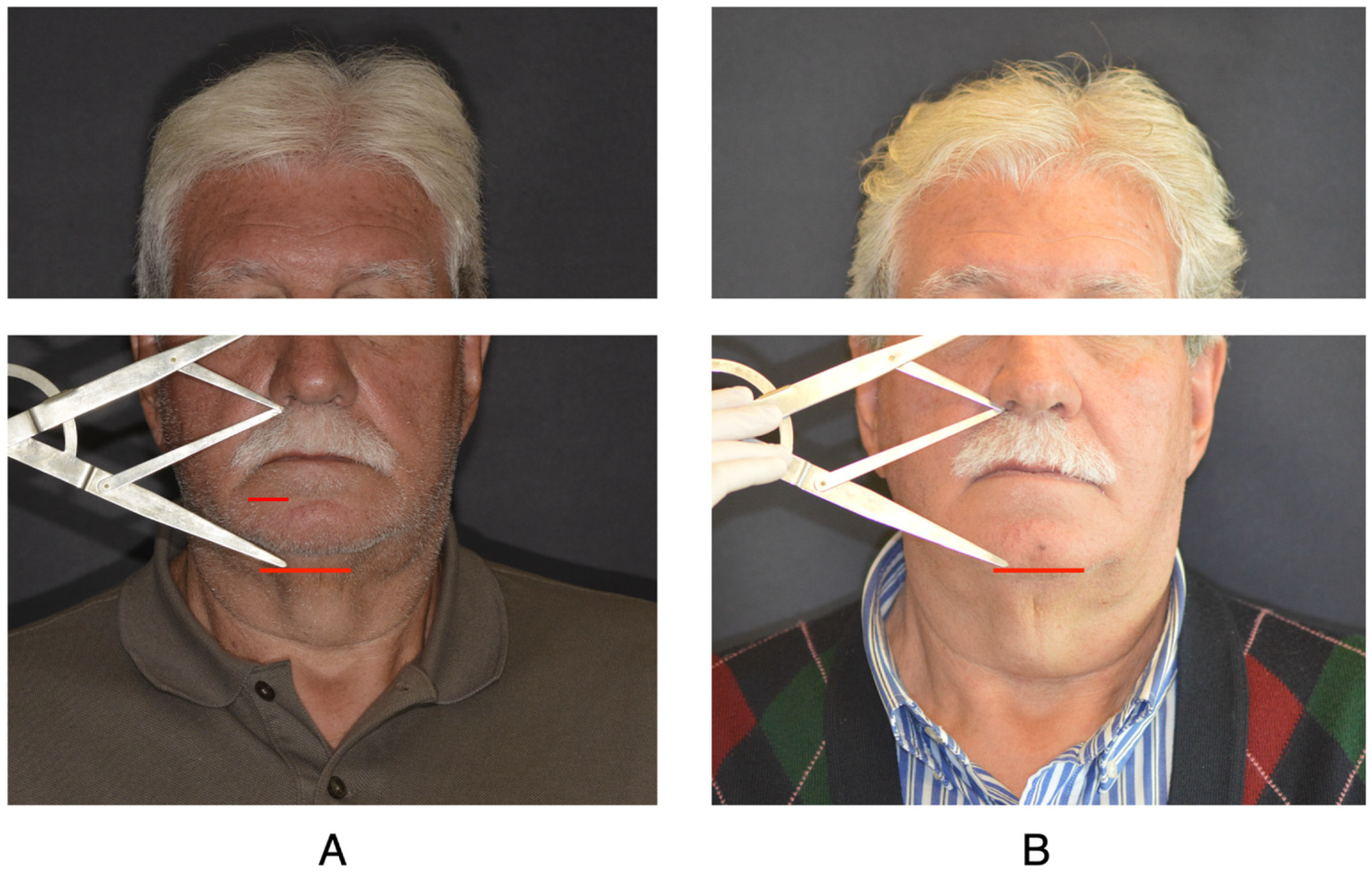
3.1. Step 1: Determination of the Vertical Dimension
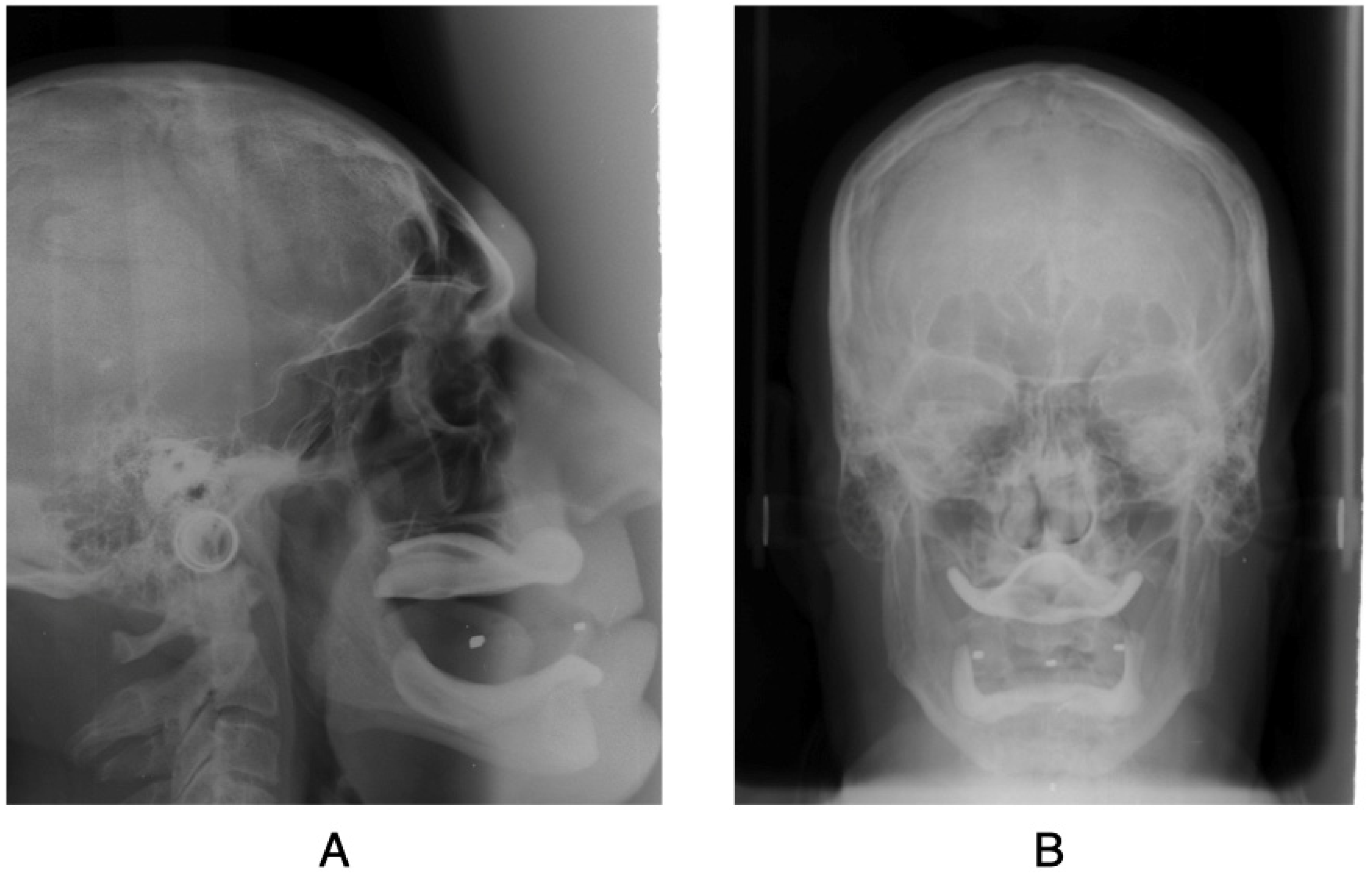
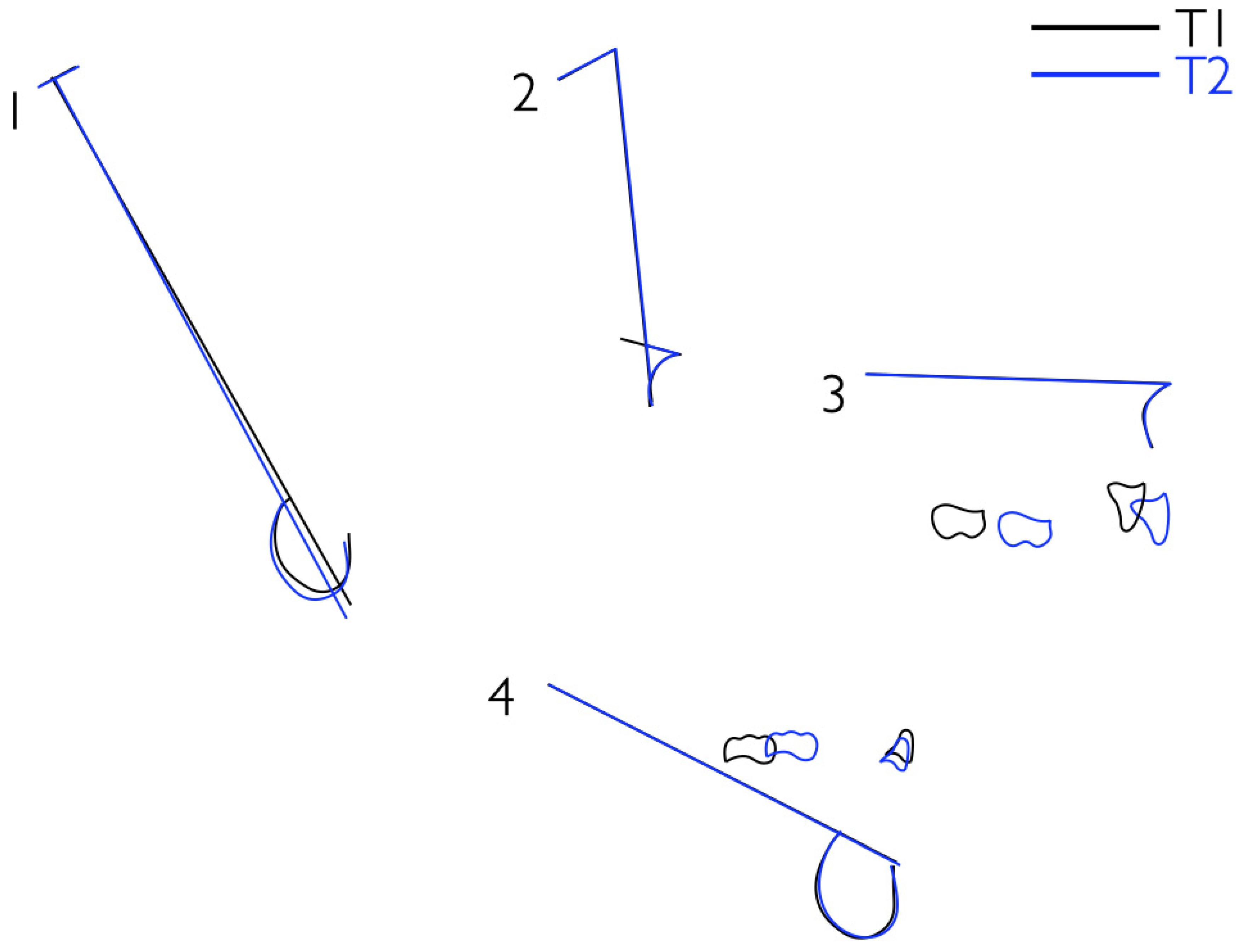
3.2. Step 2: Cephalometric Skeletal Verification of the Vertical Dimension and Determination of the Divine Occlusal Plane
3.3. Step 3: Phonetic Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Niswonger, M. Obtaining the Vertical Relation in Edentulous Cases That Existed Prior to Extraction. J. Am. Dent. Assoc. Dent. Cosm. 1938, 25, 1842–1847. [Google Scholar] [CrossRef]
- Available online: https://www.academyofprosthodontics.org/ (accessed on 10 July 2021).
- Glossary of prosthodontic terms. J. Prosthet Dent. The Academy of Prosthodontics Foundation 2017, 117, e1–e105.
- William, B.; Downs, D.D.S. Variations in facial relationships: Their significance in treatment and prognosis. Am. J. Orthod. 1948, 34, 812–840. [Google Scholar]
- Braun, S.; Kim, K.; Tomazic, T.; Legan, H.L. The relationship of the glenoid fossa to the functional occlusal plane. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 658–661. [Google Scholar] [CrossRef]
- Thayer, T.A. Effects of functional versus bisected occlusal planes on the Wits appraisal. Am. J. Orthod. Dentofac. Orthop. 1990, 97, 422–426. [Google Scholar] [CrossRef]
- Robert, M. Provocation and Perceptions in Cranio-Facial Orthopedics, 1st ed.; Rocky Mountain Orthodontics: Denver, CO, USA, 1989. [Google Scholar]
- Monteith, B.D. A cephalometric method to determine the angulation of the occlusal plane in edentulous patients. J. Prosthet. Dent. 1985, 54, 81–87. [Google Scholar] [CrossRef]
- Bhat, G. Reliability of determining vertical dimension of occlusion in complete denture: A clinical study. J. Prosthet. Dent. 2006, 6, 38. [Google Scholar] [CrossRef]
- Chirico, V.; Lacquaniti, A.; Vinci, S.; Piraino, B.; Manti, S.; Marseglia, L.; Salpietro, A.; Gitto, E.; Arrigo, T.; Salpietro, C.; et al. High-mobility group box 1 in allergic and non-allergic upper airway inflammation. J. Biol. Regul. Homeost. Agents 2015, 29, 55–57. [Google Scholar]
- Sambataro, S.; Cervino, G.; Fiorillo, L.; Cicciù, M. Upper First Premolar Positioning Evaluation for the Stability of the Dental Occlusion: Anatomical Considerations. J. Craniofacial Surg. 2018, 29, 1366–1369. [Google Scholar] [CrossRef]
- Militi, A.; Cicciù, M.; Sambataro, S.; Bocchieri, S.; Cervino, G.; De Stefano, R.; Fiorillo, L. Dental occlusion and sport performance. Minerva Stomatol. 2020, 69. [Google Scholar] [CrossRef]
- Sambataro, S.; Bocchieri, S.; Cervino, G.; La Bruna, R.; Cicciù, A.; Innorta, M.; Torrisi, B.; Cicciù, M. Correlations between Malocclusion and Postural Anomalies in Children with Mixed Dentition. J. Funct. Morphol. Kinesiol. 2019, 4, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sambataro, S.; Cervino, G.; Bocchieri, S.; La Bruna, R.; Cicciù, M. TMJ Dysfunctions Systemic Implications and Postural Assessments: A Review of Recent Literature. J. Funct. Morphol. Kinesiol. 2019, 4, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricketts, R.M. The golden divider. J. Clin. Orthod. 1981, 15, 752–759. [Google Scholar]
- Robert, M.R. Progressive Cephalometrics Paradigma 2000; American Institute for Bioprogressive Education (AIBE): Scottsdale, AZ, USA, 1996. [Google Scholar]
- Landa, J.S. Phonetic consideration in denture prosthesis. J. Prosthet. Dent. 1961, 11, 214–223. [Google Scholar]
- Allen, L.R. Improved phonetics in denture construction. J. Prosthet. Dent. 1958, 8, 753. [Google Scholar] [CrossRef]
- Grummons, D. Smile because of Dr Robert Murray Ricketts. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 368–373. [Google Scholar] [CrossRef]
- Ricketts, R.M. Advanced Orthodontic Syllabus. In Proceedings of the Advanced Orthodontic Seminar Institure for Bioprogressive Education, Scottsdale, AZ, USA, 1960. [Google Scholar]
- Chiche, J.G.; Pinault, A. Esthetics of Anterior Fixed Prosthodontics; Quintessence Pub Co.: Berlin, Germany, 1994. [Google Scholar]
- Calandriello, M.C.; Ricci, G. Parodontologia, Cides Odonto 1986 Italy.
- Silness, J. Fixed prosthodontics and periodontal health. Dent. Clin. N. Am. 1980, 24, 317–329. [Google Scholar]
- Jois, K.C. Altering Gingival Levels: The Restorative Connection. J. Prosthet. Dent. 1994, 6, 3–7. [Google Scholar]
- Garber, D.A.; Salama, M.A. The aesthetic smile: Diagnosis and treatment. Periodontology 1996, 11, 18–28. [Google Scholar] [CrossRef]
- Nevins, M.; Skurow, H.M. The intracrevicular restorative margin, the biologic width, and the maintenance of the gingival margin. Int. J. Periodontics Restor. Dent. 1984, 4, 30–49. [Google Scholar]
- Stacchi, C.; Lombardi, T.; Cusimano, P.; Berton, F.; Lauritano, F.; Cervino, G.; Di Lenarda, R.; Cicciù, M. Bone Scrapers Versus Piezoelectric Surgery in the Lateral Antrostomy for Sinus Floor Elevation. J. Craniofacial Surg. 2017, 28, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Kiel, R.A.; Anderhalden, K. Clinical and microbiological effects of subgingival restorations with overhanging or clinically perfect margins. J. Clin. Periodontol. 1983, 10, 563–578. [Google Scholar] [CrossRef] [PubMed]
- Chaconas, S.J.; Gonidis, D. A cephalometric technique for prosthodontic diagnosis and treatment planning. J. Prosthet. Dent. 1986, 56, 567–574. [Google Scholar] [CrossRef]
- Hofrath, H. Die Bedeutung der Röntgenfern- und Abstandsaufnahme für die Diagnostik der Kieferanomalien. J. Orofac. Orthop. Fortschr. der Kieferorthopädie 1931, 1, 232–258. [Google Scholar] [CrossRef]
- Broadbent, B.H. A new x-ray technique and its application to orthodontia. Angle Orthod. 1931, 1, 45–66. [Google Scholar]
- Bassi, F.; Deregibus, A.; Previgliano, V.; Bracco, P.; Preti, G. Evaluation of the utility of cephalometric parameters in constructing complete denture. Part I: Placement of posterior teeth. J. Oral. Rehabil. 2001, 28, 234–238. [Google Scholar] [CrossRef]
- Génin, G.; Helfer, M.; Chevalley, F. Conception et orientation de la surface occlusale en prothèse amovible complète [In French]. Stratégie Prothétique. 2012, 12, 109–120. [Google Scholar]
- Nissan, J.; Barnea, E.; Zeltzer, C.; Cardash, H.S. Relationship between occlusal plane determinants and craniofacial structures. J. Oral Rehabil. 2003, 30, 587–591. [Google Scholar] [CrossRef]
- Lo Giudice, G.; Lo Giudice, R.; Matarese, G.; Isola, G.; Cicciù, M.; Terranova, A.; Palaia, G.; Romeo, U. Evaluation of magnification systems in restorative dentistry. An in-vitro study. Dental Cadmos 2015, 83, 296–305. [Google Scholar] [CrossRef]
- Robert, M.; Ricketts, D.D.S. The role of cephalometrics in prosthetic diagnosis. J. Prosthet. Dent. 1956, 6, 488–503. [Google Scholar]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cervino, G.; Sambataro, S.; Stumpo, C.; Bocchieri, S.; Murabito, F.; Fiorillo, L.; Meto, A.; Zecca, P.A.; Caprioglio, A.; Cicciù, M. Determination of the Vertical Dimension and the Position of the Occlusal Plane in a Removable Prosthesis Using Cephalometric Analysis and Golden Proportion. Appl. Sci. 2021, 11, 6948. https://0-doi-org.brum.beds.ac.uk/10.3390/app11156948
Cervino G, Sambataro S, Stumpo C, Bocchieri S, Murabito F, Fiorillo L, Meto A, Zecca PA, Caprioglio A, Cicciù M. Determination of the Vertical Dimension and the Position of the Occlusal Plane in a Removable Prosthesis Using Cephalometric Analysis and Golden Proportion. Applied Sciences. 2021; 11(15):6948. https://0-doi-org.brum.beds.ac.uk/10.3390/app11156948
Chicago/Turabian StyleCervino, Gabriele, Sergio Sambataro, Chiara Stumpo, Salvatore Bocchieri, Fausto Murabito, Luca Fiorillo, Agron Meto, Piero Antonio Zecca, Alberto Caprioglio, and Marco Cicciù. 2021. "Determination of the Vertical Dimension and the Position of the Occlusal Plane in a Removable Prosthesis Using Cephalometric Analysis and Golden Proportion" Applied Sciences 11, no. 15: 6948. https://0-doi-org.brum.beds.ac.uk/10.3390/app11156948