
The Montreal Experience: A Retrospective Study Part I—Basic Principles and Treatment Algorithm

 , ,
, , 
Abstract
:1. Introduction
1.1. The First Pillar: Environmental Control
1.2. The Second Pillar: Binocular Vision Assessment
1.3. The Third Pillar: Control of the Blur
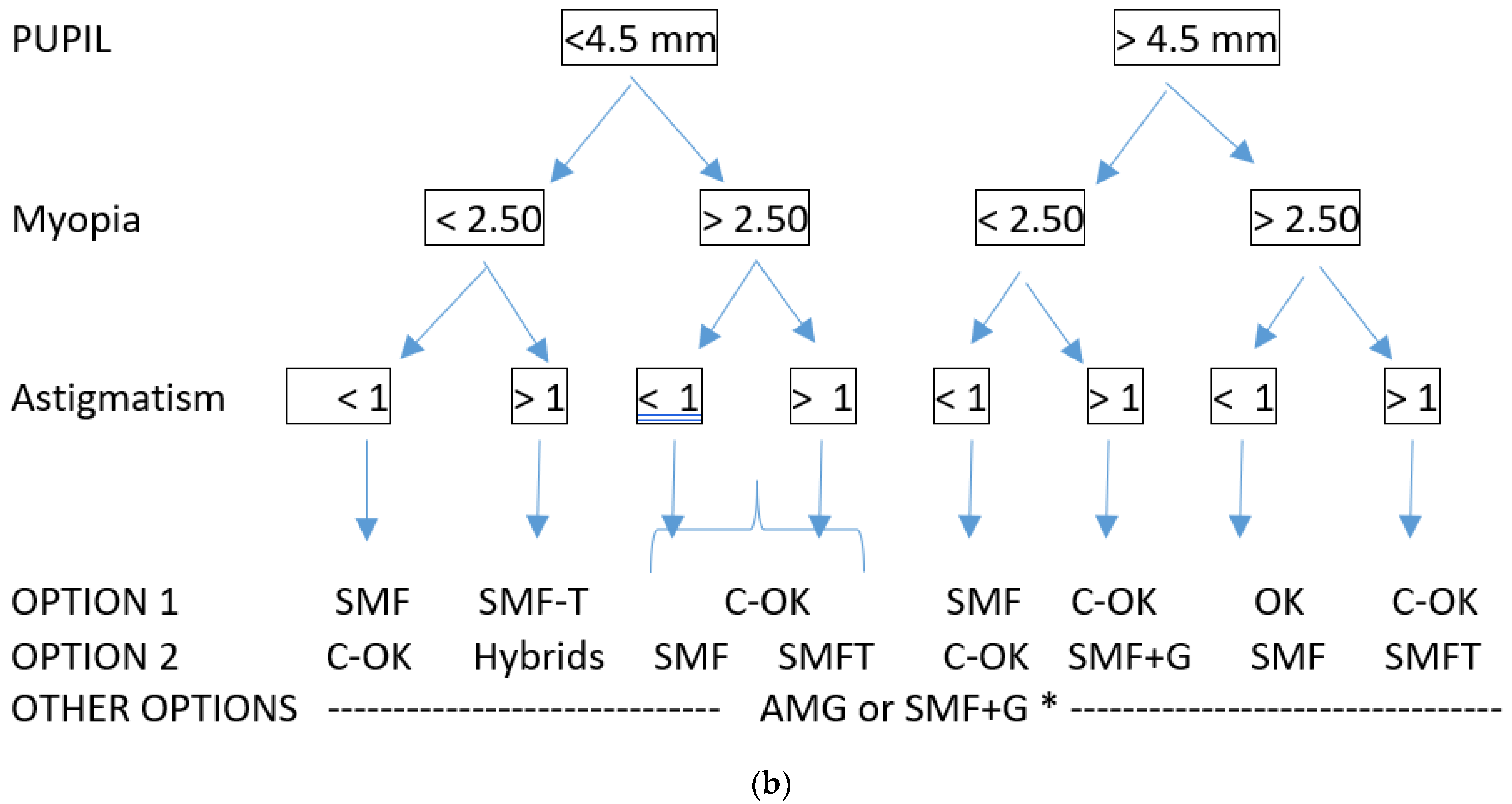
1.4. Selection of the Right Strategy
1.5. Importance of the Follow-Ups
1.6. Aim of the Study
2. Methods
Statistical Analysis
3. Results
3.1. Study Population
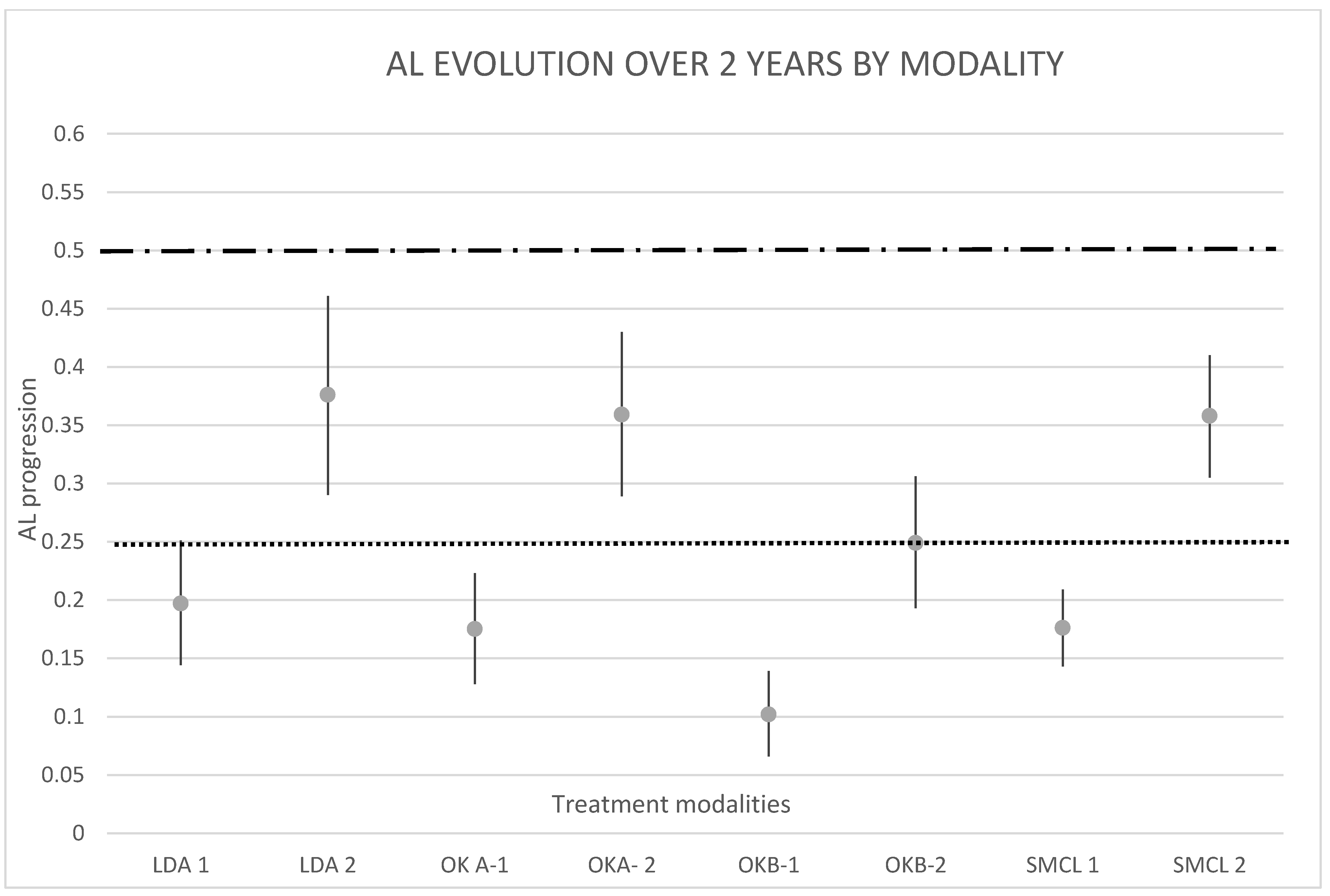
3.2. Axial Length Evolution over Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Resnikoff, S.; Jonas, J.B.; Friedman, D.; He, M.; Jong, M.; Nichols, J.J.; Ohno-Matsui, K.; Smith, E.L., III; Wildsoet, C.F.; Taylor, H.R.; et al. Myopia-A 21st Century Public Health Issue. Investig. Ophthalmol. Vis. Sci. 2019, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Optometry, W.C. Resolution: The Standard of Care for Myopia Management by Optometrists. 2021. Available online: https://worldcouncilofoptometry.info/resolution-the-standard-of-care-for-myopia-management-by-optometrists/ (accessed on 10 May 2021).
- Michaud, L.; Simard, P.; Marcotte-Collard, R. The Three pillars of Myopia Control in Practice. July 2020. Available online: https://www.pointsdevue.com/article/three-pillars-myopia-control-practice (accessed on 10 May 2021).
- Tedja, M.S.; Haarman, A.E.; Meester-Smoor, M.A.; Kaprio, J.; Mackey, D.A.; Guggenheim, J.A.; Hammond, C.J.; Verhoeven, V.J.; Klaver, C.C.; CREAM Consortium. IMI-Myopia Genetics Report. Investig. Ophthalmol. Vis. Sci. 2019, 60, M89–M105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, S.; Sankaridurg, P.; Naduvilath, T.; Zang, J.; Zou, H.; Zhu, J.; Lv, M.; He, X.; Xu, X. Time spent in outdoor activities in relation to myopia prevention and control: A meta-analysis and systematic review. Acta Ophthalmol. 2017, 95, 551–566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Guo, Y.; Xiao, Y.; Zhu, R.; Sun, W.; Huang, W.; Liang, D.; Tang, L.; Zhang, F.; Zhu, D. The Effects of Online Homeschooling on Children, Parents, and Teachers of Grades 1–9 during the COVID-19 Pandemic. Med. Sci. Monit. 2020, 26, e925591. [Google Scholar] [CrossRef]
- WHO. Guidelines on Physical Activity, Sedentary Behaviour and Sleep; World Health Organization: Geneva, Switzerland, 2019; p. 36. [Google Scholar]
- Kozeis, N. Impact of computer use on children’s vision. Hippokratia 2009, 13, 230–231. [Google Scholar]
- Rosenfield, M. Refractive error. Still the heart of optometry. Ophthalmic. Physiol. Opt. 2021, 41, 211–212. [Google Scholar] [CrossRef]
- Jiang, X.; Kurihara, T.; Torii, H.; Tsubota, K. Progress and Control of Myopia by Light Environments. Eye Contact Lens 2018, 44, 273–278. [Google Scholar] [CrossRef]
- Liu, X.N.; Naduvilath, T.J.; Wang, J.; Xiong, S.; He, X.; Xu, X.; Sankaridurg, P.R. Sleeping late is a risk factor for myopia development amongst school-aged children in China. Sci. Rep. 2020, 10, 17194. [Google Scholar] [CrossRef]
- Berticat, C.; Mamouni, S.; Ciais, A.; Villain, M.; Raymond, M.; Daien, V. Probability of myopia in children with high refined carbohydrates consumption in France. BMC Ophthalmol. 2020, 20, 337. [Google Scholar] [CrossRef] [PubMed]
- Mahto, H. Natural Ways of Myopia Control: A Public Health Approach for the Prevention of Myopia in College of Optometry; Pacific: Forest Grove, OR, USA, 2016. [Google Scholar]
- Mutti, D.O.; Mitchell, G.L.; Hayes, J.R.; Jones, L.A.; Moeschberger, M.L.; Cotter, S.A.; Kleinstein, R.N.; Manny, R.E.; Twelker, J.D.; Zadnik, K.; et al. Accommodative Lag before and after the Onset of Myopia. Investig. Ophthalmol. Vis. Sci. 2006, 47, 837–846. [Google Scholar] [CrossRef] [Green Version]
- Mutti, D.O.; Jones, L.A.; Moeschberger, M.L.; Zadnik, K. AC/A ratio, age, and refractive error in children. Investig. Ophthalmol. Vis. Sci. 2000, 41, 2469–2478. [Google Scholar] [CrossRef]
- Cheng, X.; Xu, J.; Brennan, N.A. Accommodation and its role in myopia progression and control with soft contact lenses. Ophthalmic. Physiol. Opt. 2019, 39, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Gwiazda, J.; Hyman, L.; Hussein, M.; Everett, D.; Norton, T.T.; Kurtz, D.; Leske, M.C.; Manny, R.; Marsh-Tootle, W.; Scheiman, M.; et al. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Investig. Ophthalmol. Vis. Sci. 2003, 44, 1492–1500. [Google Scholar] [CrossRef]
- Smith, E.L., 3rd; Hung, L.F.; Huang, J.; Arumugam, B. Effects of local myopic defocus on refractive development in monkeys. Optom. Vis. Sci. 2013, 90, 1176–1186. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.L., 3rd; Hung, L.F.; Huang, J.; Blasdel, T.L.; Humbird, T.L.; Bockhorst, K.H. Effects of optical defocus on refractive development in monkeys: Evidence for local, regionally selective mechanisms. Investig. Ophthalmol. Vis. Sci. 2010, 51, 3864–3873. [Google Scholar] [CrossRef]
- Bradley, A.; Nam, J.; Xu, R.; Harman, L.; Thibos, L. Impact of contact lens zone geometry and ocular optics on bifocal retinal image quality. Ophthalmic. Physiol. Opt. 2014, 34, 331–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauné, J.; Fonts, S.; Rodríguez, L.; Queirós, A. The Role of Back Optic Zone Diameter in Myopia Control with Orthokeratology Lenses. J. Clin. Med. 2021, 10, 336. [Google Scholar] [CrossRef] [PubMed]
- Walline, J.J.; Walker, M.K.; Mutti, D.O.; Jones-Jordan, L.A.; Sinnott, L.T.; Giannoni, A.G.; Bickle, K.M.; Schulle, K.L.; Nixon, A.; Pierce, G.E.; et al. Effect of High Add Power, Medium Add Power, or Single-Vision Contact Lenses on Myopia Progression in Children: The BLINK Randomized Clinical Trial. JAMA 2020, 324, 571–580. [Google Scholar] [CrossRef]
- Tse, D.Y.; To, C.H. Graded competing regional myopic and hyperopic defocus produce summated emmetropization set points in chick. Investig. Ophthalmol. Vis. Sci. 2011, 52, 8056–8062. [Google Scholar] [CrossRef] [Green Version]
- Kang, P.; McAlinden, C.; Wildsoet, C.F. Effects of multifocal soft contact lenses used to slow myopia progression on quality of vision in young adults. Acta Ophthalmol. 2017, 95, e43–e53. [Google Scholar] [CrossRef] [Green Version]
- Schulle, K.L.; Berntsen, D.A.; Sinnott, L.T.; Bickle, K.M.; Gostovic, A.T.; Pierce, G.E.; Jones-Jordan, L.A.; Mutti, D.O.; Walline, J.J.; Bifocal Lenses in Nearsighted Kids (BLINK) Study Group. Visual Acuity and Over-refraction in Myopic Children Fitted with Soft Multifocal Contact Lenses. Optom. Vis. Sci. 2018, 95, 292–298. [Google Scholar] [PubMed]
- Chung, K.; Mohidin, N.; O’Leary, D.J. Undercorrection of myopia enhances rather than inhibits myopia progression. Vision Res. 2002, 42, 2555–2559. [Google Scholar] [CrossRef] [Green Version]
- Fan, D.S.P.; Rao, S.K.; Cheung, E.Y.Y.; Islam, M.; Chew, S.; Lam, D.S.C. Astigmatism in Chinese preschool children: Prevalence, change, and effect on refractive development. BMJ 2004, 88, 938–941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franchi, C.; Longo, A.; Meslin, D. High Myopia: The specificities of refraction and optical equipment. Point. Int. Rev. Opht. Optics. 2016, 73, 34. [Google Scholar]
- Michaud, L.; Simard, P.; Marcotte-Collard, R. Defining a Strategy for Myopia Control. A systematic approach can help practitioners more effectively implement myopia control into practice. Contact Lens Spectr. 2016, 31, 36–42. [Google Scholar]
- Wang, J.; Li, Y.; Musch, D.C.; Wei, N.; Qi, X.; Ding, G.; Li, X.; Li, J.; Song, L.; Zhang, Y.; et al. Progression of Myopia in School-Aged Children After COVID-19 Home Confinement. JAMA Ophthalmol. 2021, 139, 293–300. [Google Scholar] [CrossRef]
- Glynn, R.J.; Rosner, B. Regression methods when the eye is the unit of analysis. Ophthalmic. Epidemiol. 2012, 19, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Tideman, J.W.L.; Polling, J.R.; Vingerling, J.R.; Jaddoe, V.W.V.; Williams, C.; Guggenheim, J.A.; Klaver, C.C.W. Axial length growth and the risk of developing myopia in European children. Acta Ophthalmol. 2018, 96, 301–309. [Google Scholar] [CrossRef]
- McCullough, S.; Adamson, G.; Breslin, K.M.; McClelland, J.F.; Doyle, L.; Saunders, K.J. Axial growth and refractive change in white European children and young adults: Predictive factors for myopia. Sci. Rep. 2020, 10, 15189. [Google Scholar] [CrossRef]
- Wong, H.B.; Machin, D.; Tan, S.B.; Wong, T.Y.; Saw, S.M. Ocular component growth curves among Singaporean children with different refractive error status. Investig. Ophthalmol. Vis. Sci. 2010, 51, 1341–1347. [Google Scholar] [CrossRef] [Green Version]
- Cho, P.; Cheung, S.W.; Boost, M.V. Categorisation of myopia progression by change in refractive error and axial elongation and their impact on benefit of myopia control using orthokeratology. PLoS ONE 2020, 15, e0243416. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.A.; Mitchell, G.L.; Mutti, D.O.; Hayes, J.R.; Moeschberger, M.L.; Zadnik, K. Comparison of ocular component growth curves among refractive error groups in children. Investig. Ophthalmol. Vis. Sci. 2005, 46, 2317–2327. [Google Scholar] [CrossRef] [Green Version]
- Cho, P.; Cheung, S.W. Retardation of myopia in Orthokeratology (ROMIO) study: A 2-year randomized clinical trial. Investig. Ophthalmol. Vis. Sci. 2012, 53, 7077–7085. [Google Scholar] [CrossRef] [PubMed]
- Carracedo, G.; Espinosa-Vidal, T.M.; Martínez-Alberquilla, I.; Batres, L. The Topographical Effect of Optical Zone Diameter in Orthokeratology Contact Lenses in High Myopes. J. Ophthalmol. 2019, 2019, 1082472. [Google Scholar] [CrossRef]
- Bullimore, M.A.; Richdale, K. Myopia Control 2020: Where are we and where are we heading? Ophthalmic. Physiol. Opt. 2020, 40, 254–270. [Google Scholar] [CrossRef] [PubMed]
- Christian, L.W.; Nandakumar, K.; Hrynchak, P.K.; Irving, E.L. Visual and binocular status in elementary school children with a reading problem. J. Optom. 2018, 11, 160–166. [Google Scholar] [CrossRef]
- Yam, J.C.; Li, F.F.; Zhang, X.; Tang, S.M.; Yip, B.H.; Kam, K.W.; Ko, S.T.; Young, A.L.; Tham, C.C.; Chen, L.J.; et al. Two-Year Clinical Trial of the Low-Concentration Atropine for Myopia Progression (LAMP) Study: Phase 2 Report. Ophthalmology 2020, 127, 910–919. [Google Scholar] [CrossRef] [PubMed]
- Moscato, V.; Picariello, A.; Sperli, G. An emotional recommender system for music. IEEE Intell. Syst. 2020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Lens Type | Brand Name | Treatment Zone (mm) | Jessen Factor (D) | Overall Diameter (mm) |
|---|---|---|---|---|
| OrthoK 1 | Paragon CRT (Cooper Vision) | 6.0 | 0.50 | 10.5 |
| OrthoK 2 | U de M design (custom; RGP designer software) | Variable vs. pupil Between 5.4 and 6.0 Average 5.6 | Variable. Average 0.75 | Variable. Covers 95% of the visible cornea, average 10.6 |
| OrthoK 3 | DRL (Precilens) | Variable vs. refraction Between 5.0 and 6.0 Average 5.5 | 1.5 | Variable. Covers 95% of the visible cornea, average 10.8 |
| OrthoK 4 | DreamLens (Bausch & Lomb) | 5.0 to 6.0 Average 5.0 | 0.75 | 10.6 |
| Brand | Add Power | Design | |
|---|---|---|---|
| Soft MF 1 | Oasys for presbyopia (Johnson & Johnson) | High add (= +1.75 D) | Concentric rings—alternating powers |
| Soft MF 2 | Biofinity D (Cooper Vision) | +2.00 D or +2.50 D | Centered distance—with 2 distinct zones. Central: 2.3 |
| Soft MF 3 | Proclear D (Cooper Vision) | +2.00 D or +2.50 D | Centered distance—with 2 distinct zones. Central: 2.3 |
| Soft MF 4 | Mi Sight (Cooper Vision) | +1.75 | Concentric rings—alternating powers |
| Month | Modality | Interaction of Month and Modality | Baseline SEQ | Interaction of Modality and SEQ | Gender | Age | Interaction of Month and Age | Interaction of Modality and Age |
|---|---|---|---|---|---|---|---|---|
| <0.001 | 0.852 | 0.006 | <0.001 | 0.008 | <0.001 | 0.002 | <0.001 | 0.040 |
| OrthoK 1 2 (N = 51) | OrthoK 2 (N = 49) | OrthoK 3 (N = 18) | OrthoK 4 (N = 22) | Atropine 3 (N = 42) | Overall (N = 182) | |
|---|---|---|---|---|---|---|
| Age (Mean ± SD) | 11.2 ± 2.0 | 11.6 ± 2.4 | 12 ± 2.2 | 11.7 ± 1.9 | 9.7 ± 2.3 | 11.1 ± 2.3 |
| Gender (N (%)) | ||||||
| Male | 27 (52.9%) | 11 (22.4%) | 7 (38.9%) | 12 (54.5%) | 17 (40.5%) | 74 (40.7%) |
| Female | 24 (47.1%) | 38 (77.6%) | 11 (61.1%) | 10 (45.5%) | 25 (59.5%) | 108 (59.3%) |
| Ethnicity (N (%)) | ||||||
| Caucasian | 17 (33.3%) | 13 (26.5%) | 5 (27.8%) | 9 (40.9%) | 19 (45.2%) | 63 (34.6%) |
| Asian | 25 (49%) | 25 (51%) | 12 (66.7%) | 10 (45.5%) | 9 (21.4%) | 81 (44.5%) |
| Other 1 | 9 (17.6%) | 11 (22.4%) | 1 (5.6%) | 3 (13.6%) | 14 (33.3%) | 38 (20.9%) |
| SEQ—Averaged across eyes (Mean ± SD) in Diopters | −3.2 ± 1.0 | −3.5 ± 1.4 | −4.2 ± 2.3 | −3.8 ± 1.2 | −4.3 ± 2.3 | −3.7 ± 1.7 |
| Pupil size—Averaged across eyes (Mean ± SD) in mm | 5.0 ± 0.6 | 5.2 ± 0.7 | 4.9 ± 0.8 | 5.3 ± 0.7 | 5.4 ± 0.9 | 5.1 ± 0.7 |
| SMCL 1 1 (N = 52) | SMCL 2 (N = 26) | SMCL 3 (N = 22) | SMCL 4 (N = 16) | Overall (N = 116) | |
|---|---|---|---|---|---|
| Age (Mean ± SD) | 11.6 ± 2.6 | 12.5 ± 2.0 | 11.8 ± 2.2 | 12.2 ± 2.0 | 11.9 ± 2.3 |
| Gender (N (%)) | |||||
| Male | 15 (28.8%) | 14 (53.8%) | 5 (22.7%) | 5 (31.3%) | 39 (33.6%) |
| Female | 37 (71.2%) | 12 (46.2%) | 17 (77.3%) | 11 (68.8%) | 77 (66.4%) |
| Ethnicity (N (%)) | |||||
| Caucasian | 14 (26.9%) | 12 (46.2%) | 5 (22.7%) | 8 (50%) | 39 (33.6%) |
| Asian | 25 (48.1%) | 4 (15.4%) | 7 (31.8%) | 6 (37.5%) | 42 (36.2%) |
| Other | 13 (25%) | 10 (38.5%) | 10 (45.5%) | 2 (12.5%) | 35 (30.2%) |
| SEQ—Averaged across eyes (Mean ± SD) in Diopters | −3.7 ± 2.0 | −4.5 ± 1.4 | −5.4 ± 2.2 | −3.2 ± 1.9 | −4.1 ± 2.0 |
| Pupil size—Averaged across eyes (Mean ± SD) in mm | 5.1 ± 0.8 | 4.7 ± 0.7 | 5 ± 0.7 | 5.4 ± 0.8 | 5 ± 0.8 |
| Eye | Eye | |||||
|---|---|---|---|---|---|---|
| Dataset | Time | Right | Left | Dataset | Right | Left |
| Ortho1 | Baseline | 24.97 ± 0.71 (N = 49) | 24.94 ± 0.75 (N = 51) | SMCL1 | 25.18 ± 1.03 (N = 50) | 25.19 ± 1.04 (N = 50) |
| 6 months | 25.10 ± 0.76 (N = 17) | 25.1 ± 0.82 (N = 17) | 25.03 ± 1.13 (N = 31) | 25.07 ± 1.14 (N = 30) | ||
| 12 months | 25.15 ± 0.72 (N = 40) | 25.11 ± 0.76 (N = 41) | 25.27 ± 1.00 (N = 43) | 25.28 ± 1.12 (N = 42) | ||
| 18 months | 25.31 ± 0.66 (N = 31) | 25.24 ± 0.68 (N = 33) | 25.43 ± 1.11 (N = 23) | 25.40 ± 1.06 (N = 25) | ||
| 24 months | 25.26 ± 0.75 (N = 36) | 25.20 ± 0.79 (N = 37) | 25.64 ± 1.08 (N = 22) | 25.64 ± 1.08 (N = 24) | ||
| Ortho2 | Baseline | 24.98 ± 0.77 (N = 49) | 25.02 ± 0.81 (N = 46) | SMCL2 | 25.18 ± 0.90 (N = 25) | 25.22 ± 0.88 (N = 25) |
| 6 months | 25.05 ± 0.75 (N = 40) | 25.02 ± 0.78 (N = 40) | 25.21 ± 1.08 (N = 13) | 25.38 ± 1.02 (N = 13) | ||
| 12 months | 25.00 ± 0.80 (N = 44) | 25.07 ± 0.81 (N = 42) | 25.09 ± 0.93 (N = 16) | 25.13 ± 0.89 (N = 16) | ||
| 18 months | 25.12 ± 0.83 (N = 46) | 25.16 ± 0.83 (N = 44) | 25.60 ± 0.93 (N = 10) | 25.72 ± 0.88 (N = 10) | ||
| 24 months | 25.20 ± 0.98 (N = 19) | 25.42 ± 0.90 (N = 17) | 25.54 ± 0.97 (N = 10) | 25.74 ± 0.93 (N = 10) | ||
| Ortho3 | Baseline | 25.13 ± 0.94 (N = 17) | 25.20 ± 1.04 (N = 18) | SMCL3 | 25.32 ± 1.03 (N = 22) | 25.38 ± 1.23 (N = 22) |
| 6 months | 25.26 ± 0.82 (N = 7) | 25.29 ± 0.86 (N = 7) | 25.49 ± 1.3 (N = 8) | 25.59 ± 1.68 (N = 8) | ||
| 12 months | 25.27 ± 0.90 (N = 16) | 25.34 ± 1.04 (N = 16) | 25.46 ± 1.06 (N = 18) | 25.48 ± 1.16 (N = 18) | ||
| 18 months | 25.45 ± 0.92 (N = 10) | 25.63 ± 1.07 (N = 10) | 25.76 ± 0.99 (N = 10) | 25.72 ± 1.17 (N = 10) | ||
| 24 months | 25.21 ± 0.88 (N = 11) | 25.27 ± 1.05 (N = 11) | 26.04 ± 1.39 (N = 9) | 26.23 ± 1.59 (N = 9) | ||
| Ortho4 | Baseline | 25.38 ± 0.69 (N = 21) | 25.35 ± 0.66 (N = 22) | SMCL4 | 25.05 ± 1.13 (N = 15) | 24.89 ± 1.13 (N = 16) |
| 6 months | 25.44 ± 0.74 (N = 4) | 25.39 ± 0.59 (N = 5) | 25.00 ± 0.94 (N = 9) | 24.92 ± 0.99 (N = 9) | ||
| 12 months | 25.72 ± 0.79 (N = 13) | 25.73 ± 0.76 (N = 13) | 25.30 ± 1.41 (N = 8) | 25.06 ± 1.39 (N = 9) | ||
| 18 months | 25.30 ± 0.40 (N = 5) | 25.23 ± 0.42 (N = 6) | 24.66 ± 0.72 (N = 7) | 24.57 ± 0.92 (N = 7) | ||
| 24 months | 25.52 ± 0.74 (N = 15) | 25.61 ± 0.72 (N = 15) | 25.30 ± 1.76 (N = 5) | 25.34 ± 1.75 (N = 5) | ||
| Atropine | Baseline | 24.90 ± 1.11 (N = 42) | 24.88 ± 1.15 (N = 42) | |||
| 6 months | 25.14 ± 1.06 (N = 32) | 25.17 ± 1.12 (N = 32) | ||||
| 12 months | 25.09 ± 1.07 (N = 34) | 25.04 ± 1.12 (N = 33) | ||||
| 18 months | 25.18 ± 1.06 (N = 24) | 25.22 ± 1.11 (N = 24) | ||||
| 24 months | 25.31 ± 1.12 (N = 19) | 25.39 ± 1.08 (N = 19) | ||||
| Change (mm) | OrthoK 1 | OrthoK 2-3-4 | SMCL | Atropine | Virtual Control |
|---|---|---|---|---|---|
| 1 year | 0.175 [0.128, 0.223] | 0.102 [0.066, 0.139] | 0.176 [0.143, 0.209] | 0.197 [0.144, 0.251] | 0.250 |
| 2 year | 0.359 [0.289, 0.430] | 0.249 [0.193, 0.306] | 0.358 [0.305, 0.410] | 0.376 [0.290, 0.461] | 0.500 |
| Time Interval | Modality 1 | Modality 2 | Mean Difference [95% CI] | p Value |
|---|---|---|---|---|
| One year change | Ortho K 1 | Atropine | −0.022 [−0.094, 0.050] | 0.543 |
| One year change | Ortho K 2,3,4 | Atropine | −0.095 [−0.161, −0.029] | 0.005 |
| One year change | SMCL | Atropine | −0.022 [−0.086, 0.043] | 0.505 |
| One year change | Ortho K 2,3,4 | Ortho K 1 | −0.073 [−0.133, −0.013] | 0.017 |
| One year change | SMCL | OrthoK 1 | 0.023 [−0.057, 0.058] | 0.988 |
| One year change | SMCL | Ortho K 2,3,4 | 0.073 [0.025, 0.122] | 0.003 |
| Two years change | OrthoK 1 | Atropine | −0.016 [−0.128, 0.095] | 0.776 |
| Two years change | Ortho K 2,3,4 | Atropine | −0.126 [−0.230, −0.022] | 0.018 |
| Two years change | SMCL | Atropine | −0.018 [−0.121, 0.085] | 0.730 |
| Two years change | Ortho K 2,3,4 | Ortho K 1 | −0.11 [−0.203, −0.021] | 0.017 |
| Two years change | SMCL | Ortho K 1 | −0.002 [−0.093, 0.086] | 0.967 |
| Two years change | SMCL | Ortho K 2,3,4 | 0.108 [0.032, 0.184] | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michaud, L.; Simard, P.; Marcotte-Collard, R.; Ouzzani, M.; Sinnott, L.T. The Montreal Experience: A Retrospective Study Part I—Basic Principles and Treatment Algorithm. Appl. Sci. 2021, 11, 7455. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167455
Michaud L, Simard P, Marcotte-Collard R, Ouzzani M, Sinnott LT. The Montreal Experience: A Retrospective Study Part I—Basic Principles and Treatment Algorithm. Applied Sciences. 2021; 11(16):7455. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167455
Chicago/Turabian StyleMichaud, Langis, Patrick Simard, Remy Marcotte-Collard, Mhamed Ouzzani, and Loraine T. Sinnott. 2021. "The Montreal Experience: A Retrospective Study Part I—Basic Principles and Treatment Algorithm" Applied Sciences 11, no. 16: 7455. https://0-doi-org.brum.beds.ac.uk/10.3390/app11167455