1. Introduction
Frequent reasons for restoration failure on posterior teeth include restoration fractures (8%), secondary carious lesions (6%), and cusp fractures (5%) [
1]. Although dental fractures on posterior teeth are relatively common in dentistry, their frequency and associated factors are still not well established.
Some studies have investigated fractures on posterior teeth [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14] reporting different prevalence/incidence rates, varying from 20.5 per 1000 people/year [
11] to 69.9 per 1000 people/year [
10]. These incidence estimations, although different, show posterior teeth fractures are a frequent and relevant problem due to a lack of scientific knowledge [
1,
8,
10,
11,
12,
13,
14,
15]. One retrospective study has shown that most teeth lost were nonvital teeth (92%), and the most common cause of tooth loss was tooth fracture (62%). A statistically significant risk factor for tooth loss was the number of remaining teeth at the start of maintenance [
16]. There is also a lack of consensus regarding the aetiology of both complete (with dental fragment detachment) and incomplete fractures (cracked or fissured), being linked to several individual and multifactorial variations and their association with other factors such as structure loss (cavity preparation and cervical lesions), epidemiological data, dental characteristics, restorative materials, diet, and parafunctional habits [
2,
3,
4,
5,
6,
7,
8,
9,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21].
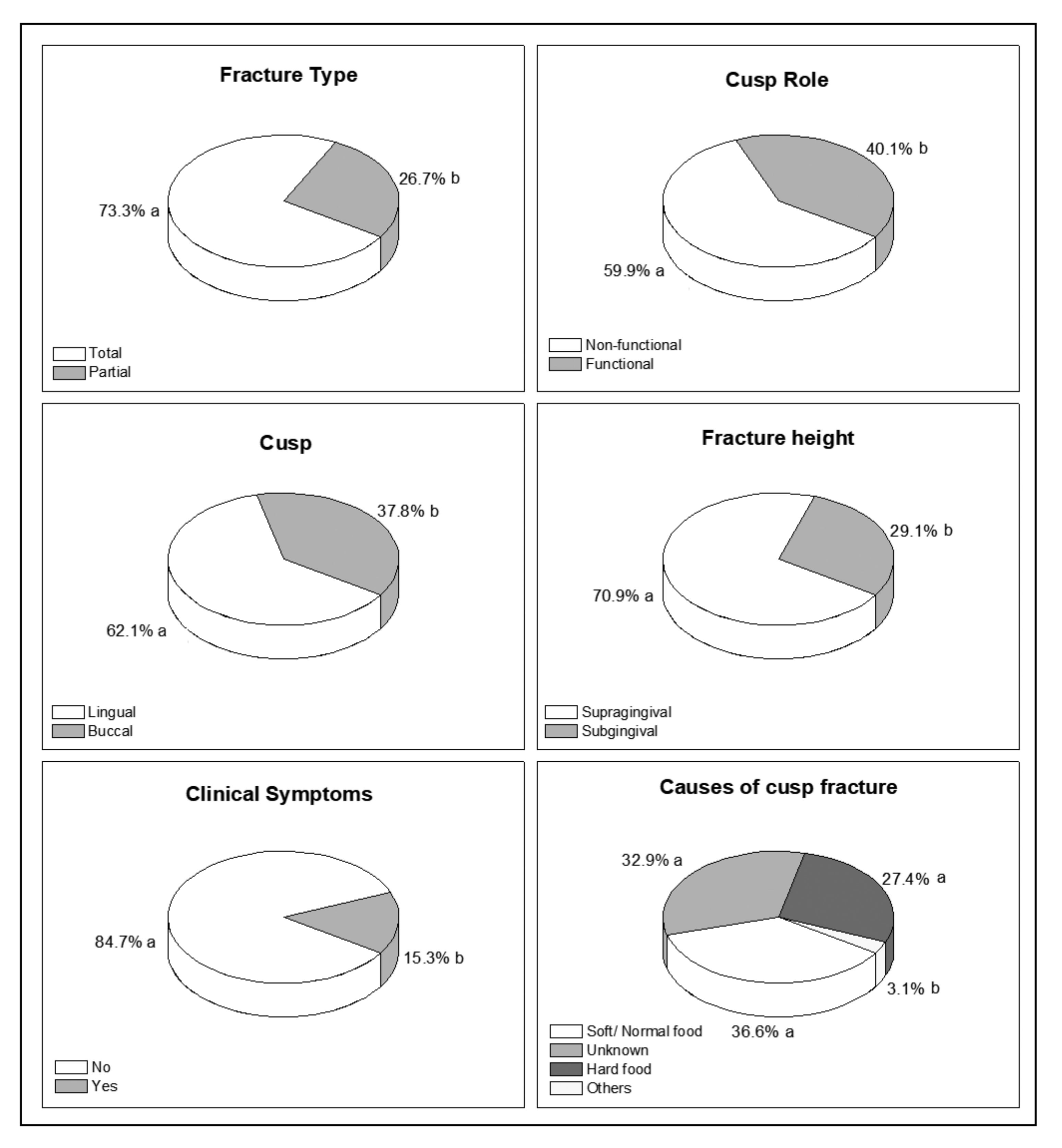
The well-established rule that functional cusps (LUBL—lingual cusps for upper teeth and buccal cusps for lower teeth) are more prone to fractures since they are responsible for food crushing (together with the antagonist pits) and contention in centric occlusion needs to be better confirmed [
7,
13,
15,
18].
Previous works have provided scientific literature with important data about cusp fractures on posterior teeth [
1,
3,
4,
5,
6,
7,
8,
9,
10,
13,
14]. However, factors related to memory; performed interventions before data collection; inexperienced personnel for information recording; the use of self-report questionnaires unable to differentiate the type of fractures, etc., could have biased obtained results [
13,
20].
Bader et al. (2001) [
10] critically assessed conceptual and collected data from several studies, concluding that their work was only capable to collect adequate data regarding the incidence of fractures on posterior teeth. Bader et al. (1995) [
8] affirmed that the literature is almost silent regarding the above-mentioned issue, presenting little information about dental fracture severity. It was not possible to identify, therefore, any systematic review analyzing cusp fractures on posterior tooth studies.
Several issues in restorative dentistry have been recently raised in the literature, such as the influence of different parameters in cavity preparation, new treatment paradigms for posterior teeth, the increase of adhesive procedures at the expense of the reduction of amalgam indication, the signs and symptoms prior tooth fractures, the influence of root canal treatment, and the rule of LUBL [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
15,
16,
17,
18,
19,
20,
21,
22,
23]. Although a large number of factors associated with cusp fracture have been identified, their magnitude has not been quantified. Therefore, already reported risk indicators need to be better explored [
10,
13,
14,
22], since prevention and management may only be implemented after the establishment of condition/failure causalities [
24].
Given the gaps in the previous study methodologies, the main purpose of this cross-sectional study was to assess the associated risk factors of posterior permanent tooth fractures. As secondary objectives, this project sought to evaluate whether functional cusps are the ones that fracture the most in accordance with the rule of LUBL; whether there are signs or symptoms that could predict such an event; and whether amalgam, cavity preparation, or endodontic treatment are directly associated with dental fractures. The null hypothesis was that both functional and nonfunctional cusps fracture at the same frequency.
2. Materials and Methods
This study was approved by the Ibirapuera University Ethics Committee (protocol CAAE nº 56415416.9.0000.5597) and followed the STROBE guidelines for observational studies [
25]. All patients received emergency treatment in the presence of pain and then referred to dental specialists (restorative treatment, periodontics, and/or prosthesis).
Patients presented cusp fractures on posterior permanent teeth, clinically assessed up to 7 days after the event; dental treatment requested at two public services (university and public dentistry clinics) was included in this cross-sectional study. One examiner (SM) collected fracture data (1998–2007); after this (2008–2016), two examiners (SM and DYN) were individually trained and then calibrated following the assessment of 10 images of cavities and restorations and 10 images of fractured teeth compared to a benchmark examiner. Kappa values were 0.9, and all possible discordances were solved by consensus. Isthmus in cavity preparation was standardised as follows: less than 1/4, between 1/3 and 1/4, and more than 1/3 of the intercuspid distance. The evaluation of the patients was performed independently, and the final result was decided by consensus. Clinical evaluation was made under dental operating light with an oral mirror, a dental probe, and a three-way syringe, and periapical radiographic examination was assessed by the examiners for all the patients. Only one tooth was included per patient. Periodontal condition was based on scores: A—bleeding on probing and/or calculus, B—pocket 4 to 5 mm without recession, and C—pocket 4 to 5 mm with recession or pockets ≥6 mm [
26]. From 2010, self-reported questionnaire about the presence of parafunctional habits (bruxism/clench) was included, based on the international consensus on the assessment of bruxism (Lobbezoo et al. 2018) [
27].
Data collection was set at a maximum of 7 days after the fracture episode to avoid memory bias and ensure clinical examination fidelity with minimal dental structure modification from the injury event. Thus, inclusion criteria included only patients assessed up to 7 days after presenting complete fractures on molar and/or pre-molar cusps. Patients were excluded when presenting fractured teeth with absence of the antagonist teeth or with a prosthesis (total and/or removable), as well as when already treated.
Demographic and clinical data were collected to draw the patient profiles and establish how teeth were affected individually. Hence, a clinical chart including demographic aspects (age/gender); teeth (FDI classification, molar/pre-molar, upper/lower); tooth characteristics (restoration presence and number of involved surfaces, restorative material, endodontic treatment–after periapical radiographic assessment, and cavity width); referred symptoms; fractured cusps characteristics (total/partial, buccal/lingual, sub/supragingival, and functional/non-functional); and fracture cause (food–hard or normal/soft, unknown, or accidental). Third molars were not considered in this study due to their many variations (anodontia and shape, position, and size anomalies). Regarding the height of the cusp fractures, it was considered supragingival when the inferior level of the fracture was up to the height of the free gingival margin and subgingival when the fracture line invaded the intrasulcular/intraosseous space. Regarding the total volume of the cusp, it was called partial cusp fracture when the fragment did not cover this volume, the remainder of which was a part of this cusp. Furthermore, it was considered as a total fracture when it covered the equivalent of the total volume of this cusp.
Sample size was calculated with a significance level of 95% and power of 80%. The main outcome for sample size calculation was the difference between the functional cusp fractures and nonfunctional cusp fractures, with the inclusion of 134 teeth being necessary. Data analysis was conducted using Minitab (Minitab Inc., State College, PA, USA). Descriptive analyses of relative frequencies per related case were performed, and comparisons among relative frequencies and each variable level were established by the Fisher exact test with a significance level of 95% (α = 0.05). Chi-square test was used to assess the associations between “teeth group” and “fractured cusp”; “endodontically-treated teeth” and “fracture height”; and “restorative material” and “isthmus”, also having a 95% (α = 0.05) significance level. Univariate logistic regression was performed to analyze the association of all variables in isolation with the fact that the fracture is in the lingual cusp, and multiple logistic regression was also used to analyze the variables that presented potential for statistical significance in conjunction, to verify what would actually be associated with fractures in lingual cusps. The outcome considered was the fracture being in the lingual cusp, having as reference the fractures in the vestibular cusp. Firstly, univariate analyses with odds ratio (OR) and confidence intervals (CI-95%) were performed. Then, a multiple model with all variables with p < 0.20 in the univariate analysis was tested.
4. Discussion
Lingual cusps were the most fractured, and showed a significant association with severe fractures, regardless of their functional or nonfunctional role. These data were based on the results here obtained, since fracture type and fracture height were the only factors significantly associated with fractures on lingual cusps. Total and subgingival fractures were more likely to occur on lingual cusps than partial and supragingival fractures.
Indications of classic protection on functional cusps (LUBL), covering of all cusps for weakened teeth and for endodontically treated teeth [
5,
6,
7,
11,
13,
20,
21], were also assessed in this study, since, theoretically, functional cusp would fracture more than nonfunctional ones and, therefore, should be covered [
14]. However, obtained results question this statement, since in lower molars the majority of fractures occurred on non-functional cusps (lingual), and for the upper molars and lower premolars, there were no differences between functional and non-functional cusps fractures. Maxillary premolars were the only teeth showing a higher frequency of fractures on functional cusps (lingual). Given that, when a cusp is already weakened by cavity preparation, lingual are generally the most involved in fractures, deserving special attention [
4,
5,
6,
7,
15]. Possible explanations rely on Wilson curve of occlusion, in which the posterior teeth are lingually oriented and, thus, the occlusal force components favor these cusp fractures. Nevertheless, the most adopted and disseminated reason is based on the fact that functional cusps are more voluminous, except for the upper premolars. These data support the idea that fractures do not occur due to the cusp role (functional or nonfunctional), but under the assumption that smaller cusps are weaker and more likely to fracture. Authors also observed that nonfunctional molar cusps and the upper premolars were the most inclined, and this might also contribute as a correlating factor. Thickness of the enamel was also related to fractures. In addition, functional cusps lie between two other cusps during intercuspation, which may avoid fractures [
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15].
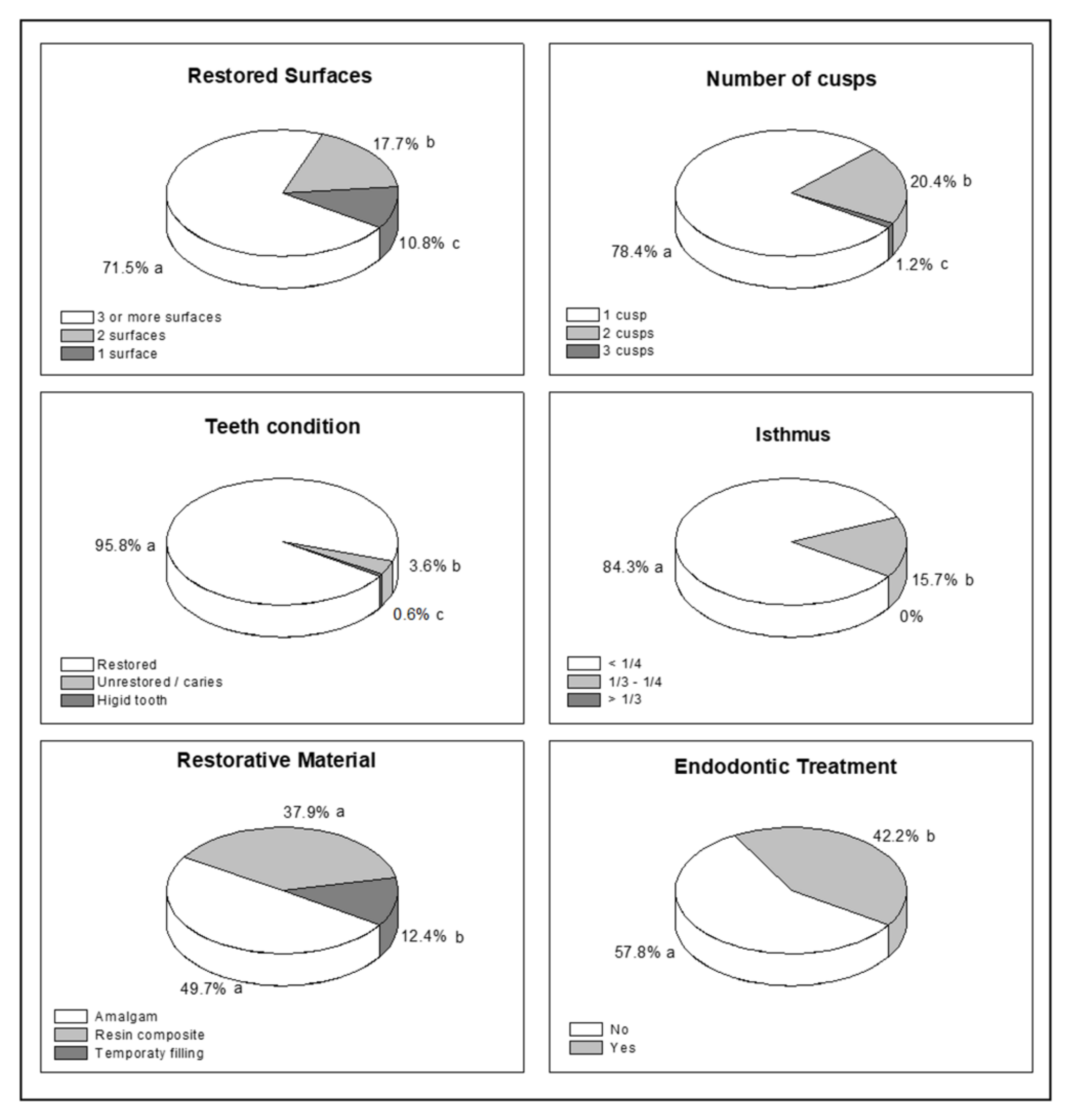
Fractures were more common in teeth where the restoration had an isthmus wider than 1/3 of the intercuspid distance and/or involved more than and/or involved more than 3 restored surfaces. Overall, less than 1% of sound teeth fractured, reinforcing the notion that teeth undergoing cavity preparation are weakened and prone to fracture [
2,
13]. In this sense, Bader et al. (2001) [
10] reported that 97% of fractures involved teeth with restorations. This may be related to the fact that cusp deflection increases with cavity size, causing fatigue of the dental structures over time, resulting in microleakage and dental fractures [
3,
11,
28,
29]. Proximal box preparation significantly weakens the entire dental structure and further potentiates fractures due to the marginal ridge loss.
Cavity preparation has been reported as one of the numerous risk factors for dental fractures [
5,
6,
7,
10,
11,
12,
13,
15], yet more than 500 million restorations are annually placed worldwide [
19]. Dentistry coexists with these paradoxical data since restorative interventions in the management of dental caries is often unavoidable. Besides, placing this relevant information together with the other 49 described risk factors for tooth fractures may be leading the practitioner to underestimate the relevance of cavity preparation, not knowing what really matters and believing that, due to restoration, the tooth is recovering. However, this is not what actually occurs.
Lower molars were the most fractured teeth, followed by upper molars and upper premolars. This could be explained by the tooth eruption chronology since the lower 1st permanent molars are the first posterior teeth to erupt and thus they could be affected earlier by caries, receiving restorations and becoming more vulnerable to fractures.
Generally, patients did not refer symptomatology before experiencing fractures (85%) and, consequently, the presence of symptoms cannot be taken as an indication to start preventive measures. However, these data reinforce the importance of frequent dental visits since the absence of sensitivity alone cannot be considered relevant for the diagnosis; clinical observation of the presence of cracks or fracture lines is also relevant, among others indicators [
2,
13,
17,
21,
29]. Here, when symptoms were present (15%), they were often inaccurate. However, pain during mastication was the most frequently reported, followed by nonspecific pain and after-cold stimulus.
Although endodontic treatment is not a fracture determinant, it might be associated with its severity since the present is more subgingival. In vital teeth, fractures often reach the level of the bone crest, whereas in nonvital teeth, they are usually subgingival since the fracture line may propagate to the root portion. Fractures begin at the dihedral of the cavity preparation involving the pulp wall and its surrounding ones, mainly buccal and lingual, and the deeper the pulp wall, the more subgingival the fractures tend to be [
6]. Although endodontic treatment is not a fracture determinant, it might be associated with its severity, since the present is more subgingival. Usually, teeth that require root canals have undergone successive structure losses, numerous cavity preparations, and restoration placements. These factors really weaken the structure integrity and not necessarily the pulp removal and endodontic access as an isolated cause. Reeh et al. (1989) [
18] stated that accessing the pulp chamber reduces dental stiffness by only 5%, whereas the preparation of a mesial-occlusal-distal cavity reduces it by up to 63%. Hansen and Asmussen (1990) [
19] observed retrospectively that the survival of endodontically treated teeth restored with amalgam was 74% (teeth with mesial-occlusal/distal-occlusal preparation), 38% (mesial-occlusal-distal), and only 28% of upper premolars (mesial-occlusal-distal) remained intact after 20 years. These data suggest, as do the findings in this study, that cavity preparation is an important factor for dental fractures in comparison to endodontic treatment itself.
Individual and multifactorial variations such as sex, age, race, cusp height, pit and fissure depth, enamel thickness, tooth size, structure loss (i.e., cavity preparation, caries, and cervical lesions), restorative material, type of food, occlusal contact, and parafunctional habits have been cited as failure predictors [
1,
2,
5,
6,
7,
9,
11,
13,
14,
15]. Nevertheless, some of these can be considered as possible confounding factors, such as the restoration size and restorative material. In a case-control study, Bader et al. (2004) [
13] observed two risk indicators for dental fractures: presence of fracture lines and the crown volume of a tooth filled by a restoration. However, a critical analysis [
20] questions these indicators since the fracture lines could be interpreted as the beginning of the fracture per se, especially regarding the accuracy of the restoration volume calculation in cases where the restoration had been lost.
To date, no study has been able to quantify such risk and dissociate the main factors associated with variables in the binomial cavity preparation/restorative material. What is the number of faces involved? What is the cavity width? Or, perhaps, what is the restorative material? Questions raised given the change in the dentistry scene, and the use of adhesive systems in posterior teeth, have reached considerable proportions in the last decades [
19,
28,
29].
Regarding restorative materials, teeth restored with resin or amalgam fractured equally. It is normally believed that teeth with amalgam restorations are more associated with fractures than those restored with composites. However, given the increased indication of composites restorations in posterior teeth associated with etching and the use of last generation adhesives, the assessing of these premises was important for this study [
1,
12,
15,
20,
28,
29]. Nevertheless, the results pointed out the restorative material did not influence the fractures’ development, reinforcing, once again, that cavity preparation is a more important factor than restoration material. Consequently, no restorative material would restore cusp stiffness and cusp deflection would increase at the expense of cavity extension, allowing failure, microleakage at the restorative interface, and tooth fatigue over time [
17]. One previous study evaluated 10.082 teeth restored with amalgam and 787 with composite. Authors observed that the frequency of fractured cusps in each group was not considered statistically different, both of which were considered acceptable from the point of view of restoration and tooth durability [
12].
Based on the analyses here performed, sex, age, arch, restorative material (amalgam or resin), endodontic treatment, or type of food were not factors that were directly associated with dental fractures, although they have been considered previously [
1,
2,
5,
6,
7,
9,
11,
13,
15]. On the other hand, fractures were more common in teeth where the restoration was 1/3 wider than their distance and/or involved more than three restored surfaces. Among patients with fractured teeth, only 20% reported bruxism/clench.
The idea of covering functional cusps or even all cusps was left opened for discussion: how can we be protecting the cusps by wearing them? To preemptively cover the cusps would today be an analogy for the “Extension for Prevention” by Black (1910) [
30], which established the philosophy of “wearing to prevent”? Moreover, even if the dentist chooses to cover them, he/she should know the lingual cusps are most prone to fractures, not necessarily the LUBL. In this way, the null hypothesis in this project was rejected since even non-functional cusps fractured more than the functional cusps.
Data from this study strongly encourage earlier and minimally invasive preventive approaches preserving unsupported enamel and restricted to selective caries removal, with special attention to marginal ridge preservation since they are joists joining the buccal and lingual cusps. For those compromised teeth, with the classic indication of cusp coverage, randomized studies based on adhesive procedures and ceramic and resin restorations should be established, restoring only the missing parts since many principles were established based on cast restorations.
This study, following a cross-sectional design, required a rigorous data collection and compilation, including clinical observations, examiner training and calibration, and establishment of inclusion and exclusion criteria, among other methodological characteristics, ensuring data reliability. The development of new epidemiological surveys is essential, as well as the conduction of systematic reviews on that matter. Among the limitations of this study, we can mention the need to assess malocclusions and bruxism. In this study, we relied solely on self-reporting since studies [
27] state that it can be employed to assess bruxism; however, studies more focused on these factors are recommended.


 ,
, 


{kind=link}
{kind=link}