
Potential New Treatments for Knee OA: A Prospective Review of Registered Trials

Abstract
:1. Introduction
2. Materials and Methods
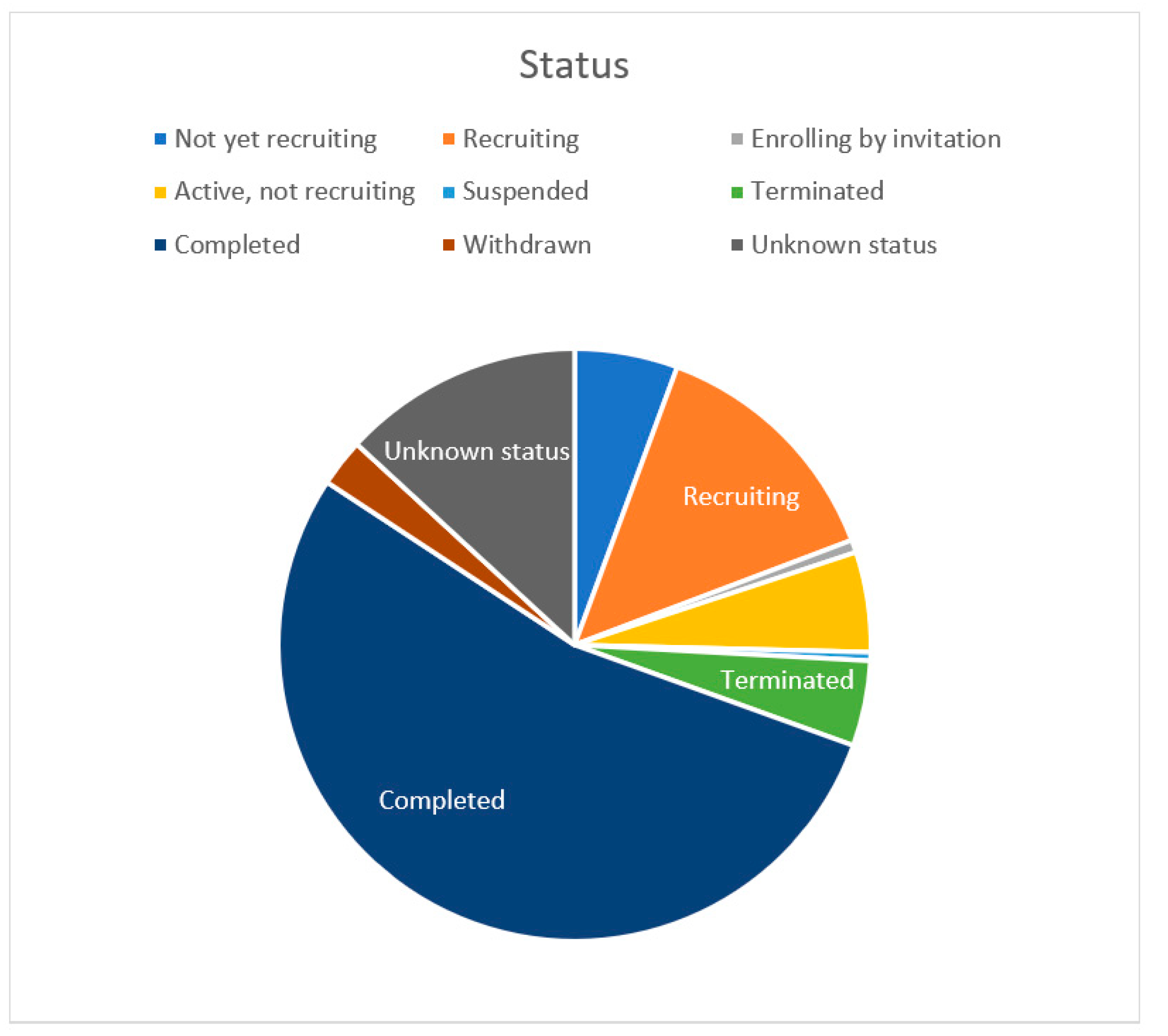
- Not yet recruiting 156.
- Recruiting 377.
- Enrolling by invitation 19.
- Active, not recruiting 151.
- Suspended 13.
- Terminated 129.
- Completed 1488.
- Withdrawn 72.
- Unknown status 364.
3. Results
- ○
- Behavioral 53.
- ○
- Biological 62.
- ○
- Combination product 6.
- ○
- Device 185.
- ○
- Diagnostic test 7.
- ○
- Dietary supplement 13.
- ○
- Drug 112.
- ○
- Other 121.
- ○
- Genetic 1.
- ○
- Procedure 95.
- ○
- No specification 26.
- ✓
- 79 device.
- ✓
- 18 drug.
- ✓
- 45 procedure.
- ✓
- 6 other.
- ✓
- 59 biological.
- ✓
- 4 combination.
- ✓
- 18 device.
- ✓
- 21 drug.
- ✓
- 9 procedure.
- ✓
- 1 other.
- ✓
- 1 combination.
- ✓
- 37 device.
- ✓
- 51 other.
- ✓
- 2 procedure.
- ✓
- 2 biological.
- ✓
- 13 dietary supplement.
- ✓
- 67 drug.
- ✓
- 1 genetic.
- ✓
- 50 behavioral.
- ✓
- 1 device.
- ✓
- 4 other.
- ✓
- 1 biological.
- ✓
- 18 device..
- ✓
- 2 diagnostic test
- ✓
- 3 drug.
- ✓
- 26 other.
- ✓
- 22 procedure.
- ✓
- 2 radiation.
4. Discussion
4.1. Knee Replacement
4.2. Intraarticular Injections
4.3. Physical Therapy
4.4. Drugs
4.5. Behavioral Interventions
4.6. Other
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharma, L. Osteoarthritis of the Knee. N. Engl. J. Med. 2021, 384, 51–59. [Google Scholar] [CrossRef]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef]
- Primorac, D.; Molnar, V.; Rod, E.; Jeleč, Ž.; Čukelj, F.; Matišić, V.; Vrdoljak, T.; Hudetz, D.; Hajsok, H.; Borić, I. Knee Osteoarthritis: A Review of Pathogenesis and State-Of-The-Art Non-Operative Therapeutic Considerations. Genes 2020, 11, 854. [Google Scholar] [CrossRef] [PubMed]
- Khella, C.M.; Asgarian, R.; Horvath, J.M.; Rolauffs, B.; Hart, M.L. An Evidence-Based Systematic Review of Human Knee Post-Traumatic Osteoarthritis (PTOA): Timeline of Clinical Presentation and Disease Markers, Comparison of Knee Joint PTOA Models and Early Disease Implications. Int. J. Mol. Sci. 2021, 22, 1996. [Google Scholar] [CrossRef]
- Belluzzi, E.; Macchi, V.; Fontanella, C.G.; Carniel, E.L.; Olivotto, E.; Filardo, G.; Sarasin, G.; Porzionato, A.; Granzotto, M.; Pozzuoli, A.; et al. Infrapatellar Fat Pad Gene Expression and Protein Production in Patients with and without Osteoarthritis. Int. J. Mol. Sci. 2020, 21, 6016. [Google Scholar] [CrossRef]
- Rim, Y.A.; Ju, J.H. The Role of Fibrosis in Osteoarthritis Progression. Life 2021, 11, 3. [Google Scholar] [CrossRef]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and Treatment of Hip and Knee Osteoarthritis: A Review. JAMA 2021, 9, 568–578. [Google Scholar] [CrossRef]
- Biehl, C.; Heinrich, M.; Biehl, L.; Knapp, G.; Heiss, C.; Thormann, U. Biomechanical Particularities in the Therapy of the Rheumatic Knee. Appl. Sci. 2020, 10, 8600. [Google Scholar] [CrossRef]
- American Academy of Orthopaedic Surgeons Surgical Management of the Knee Evidence-Based Clinical Practice Guideline. Published 4 September 2015. Available online: https://www.aaos.org/globalassets/quality-and-practice-resources/surgical-management-knee/smoak-cpg_4.22.2016.pdf (accessed on 14 October 2021).
- American Academy of Orthopaedic Surgeons Management of Osteoarthritis of the Knee (Non-Arthroplasty) Evidence-Based Clinical Practice Guideline (3rd ed.). Published 31 August 2021. Available online: https://www.aaos.org/oak3cpg (accessed on 14 October 2021).
- Grässel, S.; Muschter, D. Recent advances in the treatment of osteoarthritis. F1000Research 2020, 9, F1000. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Robertson, W.B.; Zhao, J.; Chen, W.; Xu, J. Emerging Trend in the Pharmacotherapy of Osteoarthritis. Front. Endocrinol. 2019, 10, 431. [Google Scholar] [CrossRef]
- Available online: https://clinicaltrials.gov/ct2/results?cond=Osteoarthritis%2C+Knee&flds=bgijkopv&recrs=b&recrs=a&recrs=f&recrs=d&age_v=&gndr=&type=Intr&rslt=&Search=Apply (accessed on 23 September 2021).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.; Mavrogenis, A.F.; Scarlat, M.M. The growth of scientific publications in 2020: A bibliometric analysis based on the number of publications, keywords, and citations in orthopaedic surgery. Int. Orthop. 2021, 45, 1905–1910. [Google Scholar] [CrossRef] [PubMed]
- Todor, A.; Vermesan, D.; Haragus, H.; Patrascu, J.M., Jr.; Timar, B.; Cosma, D.I. Cross-cultural adaptation and validation of the Romanian International Knee Documentation Committee-subjective knee form. PeerJ 2020, 8, e8448. [Google Scholar] [CrossRef] [PubMed]
- Batailler, C.; Swan, J.; Sappey Marinier, E.; Servien, E.; Lustig, S. New Technologies in Knee Arthroplasty: Current Concepts. J. Clin. Med. 2020, 10, 47. [Google Scholar] [CrossRef]
- Kim, J.; Min, K.D.; Lee, B.I.; Kim, J.B.; Kwon, S.W.; Chun, D.I.; Kim, Y.B.; Seo, G.W.; Lee, J.S.; Park, S.; et al. Comparison of functional outcomes between single-radius and multi-radius femoral components in primary total knee arthroplasty: A meta-analysis of randomized controlled trials. Knee Surg. Relat. Res. 2020, 32, 1–12. [Google Scholar] [CrossRef]
- Ene, R.; Nica, M.; Ene, D.; Cursaru, A.; Cirstoiu, C. Review of calcium-sulphate-based ceramics and synthetic bone substitutes used for antibiotic delivery in PJI and osteomyelitis treatment. EFORT Open Rev. 2021, 6, 297–304. [Google Scholar] [CrossRef]
- Prasad, A.K.; Tan, J.H.S.; Bedair, H.S.; Dawson-Bowling, S.; Hanna, S.A. Cemented vs. cementless fixation in primary total knee arthroplasty: A systematic review and meta-analysis. EFORT Open Rev. 2020, 5, 793–798. [Google Scholar] [CrossRef]
- Siddiqi, A.; Mont, M.A.; Krebs, V.; Piuzzi, N.S. Not All Robotic-assisted Total Knee Arthroplasty Are the Same. J. Am. Acad. Orthop. Surg. 2021, 29, 45–59. [Google Scholar] [CrossRef]
- Tandogan, R.N.; Kort, N.P.; Ercin, E.; van Rooij, F.; Nover, L.; Saffarini, M.; Hirschmann, M.T.; Becker, R.; Dejour, D. European Knee Associates (EKA). Computer-assisted surgery and patient-specific instrumentation improve the accuracy of tibial baseplate rotation in total knee arthroplasty compared to conventional instrumentation: A systematic review and meta-analysis. Knee Surg. Sports Traumatol. Arthrosc. 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Boia, E.S.; David, V.L. The Financial Burden of Setting up a Pediatric Robotic Surgery Program. Medicina 2019, 55, 739. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Liu, W.; Hou, J.; Hu, X.; Zhang, W. Does robotic-assisted unicompartmental knee arthroplasty have lower complication and revision rates than the conventional procedure? A systematic review and meta-analysis. BMJ Open 2021, 11, e044778. [Google Scholar] [CrossRef]
- Predescu, V.; Grosu, A.M.; Gherman, I.; Prescura, C.; Hiohi, V.; Deleanu, B. Early experience using patient-specific instrumentation in opening wedge high tibial osteotomy. Int. Orthop. 2021, 45, 1509–1515. [Google Scholar] [CrossRef]
- Kon, E.; Di Matteo, B.; Verdonk, P.; Drobnic, M.; Dulic, O.; Gavrilovic, G.; Patrascu, J.M.; Zaslav, K.; Kwiatkowski, G.; Altschuler, N.; et al. Aragonite-Based Scaffold for the Treatment of Joint Surface Lesions in Mild to Moderate Osteoarthritic Knees: Results of a 2-Year Multicenter Prospective Study. Am. J. Sports Med. 2021, 49, 588–598. [Google Scholar] [CrossRef]
- Cofaru, N.F.; Roman, M.D.; Cofaru, I.I.; Oleksik, V.S.; Fleaca, S.R. Medial Opening Wedge High Tibial Osteotomy in Knee Osteoarthritis—A Biomechanical Approach. Appl. Sci. 2020, 10, 8972. [Google Scholar] [CrossRef]
- Hussain, N.; Brull, R.; Sheehy, B.; Dasu, M.; Weaver, T.; Abdallah, F.W. Does the addition of iPACK to adductor canal block in the presence or absence of periarticular local anesthetic infiltration improve analgesic and functional outcomes following total knee arthroplasty? A systematic review and meta-analysis. Reg. Anesth. Pain Med. 2021, 46, 713–721. [Google Scholar] [CrossRef]
- Levy, D.M.; Petersen, K.A.; Scalley Vaught, M.; Christian, D.R.; Cole, B.J. Injections for Knee Osteoarthritis: Corticosteroids, Viscosupplementation, Platelet-Rich Plasma, and Autologous Stem Cells. Arthrosc. J. Arthrosc. Relat. Surg. 2018, 34, 1730–1743. [Google Scholar] [CrossRef] [PubMed]
- Radu, F.; Valentin, O.; Adrian, P.; Mihaela, C.M.; Mihai, R. Properties and Behaviour of Distal Femur to Axial Loading in Osteochondral Autologous Transplantation. Rom. Biotechnol. Lett. 2014, 2, 9141–9147. [Google Scholar]
- Chu, C.R.; Rodeo, S.; Bhutani, N.; Goodrich, L.R.; Huard, J.; Irrgang, J.; LaPrade, R.F.; Lattermann, C.; Lu, Y.; Mandelbaum, B.; et al. Optimizing Clinical Use of Biologics in Orthopaedic Surgery: Consensus Recommendations From the 2018 AAOS/NIH U-13 Conference. J. Am. Acad Orthop. Surg. 2019, 27, e50–e63. [Google Scholar] [CrossRef] [PubMed]
- Hernigou, P.; Hernigou, J.; Scarlat, M. Mesenchymal stem cell therapy improved outcome of early post-traumatic shoulder osteonecrosis: A prospective randomized clinical study of fifty patients with over ten year follow-up. Int. Orthop. 2021, 45, 2643–2652, epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, N.; Mak, C.; Bojanic, C.; To, K.; Khan, W. Meta-Analysis of Adipose Tissue Derived Cell-Based Therapy for the Treatment of Knee Osteoarthritis. Cells 2021, 10, 1365. [Google Scholar] [CrossRef]
- Gobbi, A.; Dallo, I.; Rogers, C.; Striano, R.D.; Mautner, K.; Bowers, R.; Rozak, M.; Bilbool, N.; Murrell, W.D. Two-year clinical outcomes of autologous microfragmented adipose tissue in elderly patients with knee osteoarthritis: A multi-centric, international study. Int. Orthop. 2021, 45, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Matas, J.; Orrego, M.; Amenabar, D.; Infante, C.; Tapia-Limonchi, R.; Cadiz, M.I.; Alcayaga-Miranda, F.; González, P.L.; Muse, E.; Khoury, M.; et al. Umbilical Cord-Derived Mesenchymal Stromal Cells (MSCs) for Knee Osteoarthritis: Repeated MSC Dosing Is Superior to a Single MSC Dose and to Hyaluronic Acid in a Controlled Randomized Phase I/II Trial. Stem Cells Transl. Med. 2019, 8, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.Y.; Song, E.K.; Kang, S.J.; Kwak, W.K.; Kang, J.K.; Seon, J.K. Allogenic umbilical cord blood-derived mesenchymal stromal cell implantation was superior to bone marrow aspirate concentrate augmentation for cartilage regeneration despite similar clinical outcomes. Knee Surg. Sports Traumatol. Arthrosc. 2021, 25, 1–11, epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Ren, B.; Lv, X.; Tu, C.; Li, Z. Research trends of platelet-rich plasma application in orthopaedics from 2002 to 2020: A bibliometric analysis. Int. Orthop. 2021, 45, 2773–2790. [Google Scholar] [CrossRef] [PubMed]
- Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Goodrich, J.A.; Dragoo, J.L.; McCarty, E.C. Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Am. J. Sports Med. 2021, 49, 249–260. [Google Scholar] [CrossRef]
- Onofrei, R.R.; Amaricai, E.; Suciu, O.; David, V.L.; Rata, A.L.; Hogea, E. Smartphone Use and Postural Balance in Healthy Young Adults. Int. J. Environ. Res. Public Health 2020, 17, 3307. [Google Scholar] [CrossRef]
- Bobes Álvarez, C.; Issa-Khozouz Santamaría, P.; Fernández-Matías, R.; Pecos-Martín, D.; Achalandabaso-Ochoa, A.; Fernández-Carnero, S.; Martínez-Amat, A.; Gallego-Izquierdo, T. Comparison of Blood Flow Restriction Training versus Non-Occlusive Training in Patients with Anterior Cruciate Ligament Reconstruction or Knee Osteoarthritis: A Systematic Review. J. Clin. Med. 2021, 10, 68. [Google Scholar] [CrossRef] [PubMed]
- Novak, S.; Guerron, G.; Zou, Z.; Cheung, G.; Berteau, J.P. New Guidelines for Electrical Stimulation Parameters in Adult Patients With Knee Osteoarthritis Based on a Systematic Review of the Current Literature. Am. J. Phys. Med. Rehabil. 2020, 99, 682–688. [Google Scholar] [CrossRef]
- Latourte, A.; Kloppenburg, M.; Richette, P. Emerging pharmaceutical therapies for osteoarthritis. Nat. Rev. Rheumatol. 2020, 16, 673–688. [Google Scholar] [CrossRef]
- Rice, D.; McNair, P.; Huysmans, E.; Letzen, J.; Finan, P. Best Evidence Rehabilitation for Chronic Pain Part 5: Osteoarthritis. J. Clin. Med. 2019, 8, 1769. [Google Scholar] [CrossRef] [Green Version]
- Torkian, P.; Golzarian, J.; Chalian, M.; Clayton, A.; Rahimi-Dehgolan, S.; Tabibian, E.; Talaie, R. Osteoarthritis-Related Knee Pain Treated With Genicular Artery Embolization: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2021, 9, 23259671211021356. [Google Scholar] [CrossRef]
- Chen, A.F.; Mullen, K.; Casambre, F.; Visvabharathy, V.; Brown, G.A. Thermal Nerve Radiofrequency Ablation for the Nonsurgical Treatment of Knee Osteoarthritis: A Systematic Literature Review. J. Am. Acad. Orthop Surg. 2021, 29, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.H.; Shen, P.C.; Lu, C.C.; Liu, Z.M.; Tien, Y.C.; Huang, P.J.; Chou, C.M.; Shih, C.L. Comparison of Efficacy among Three Radiofrequency Ablation Techniques for Treating Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 7424. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
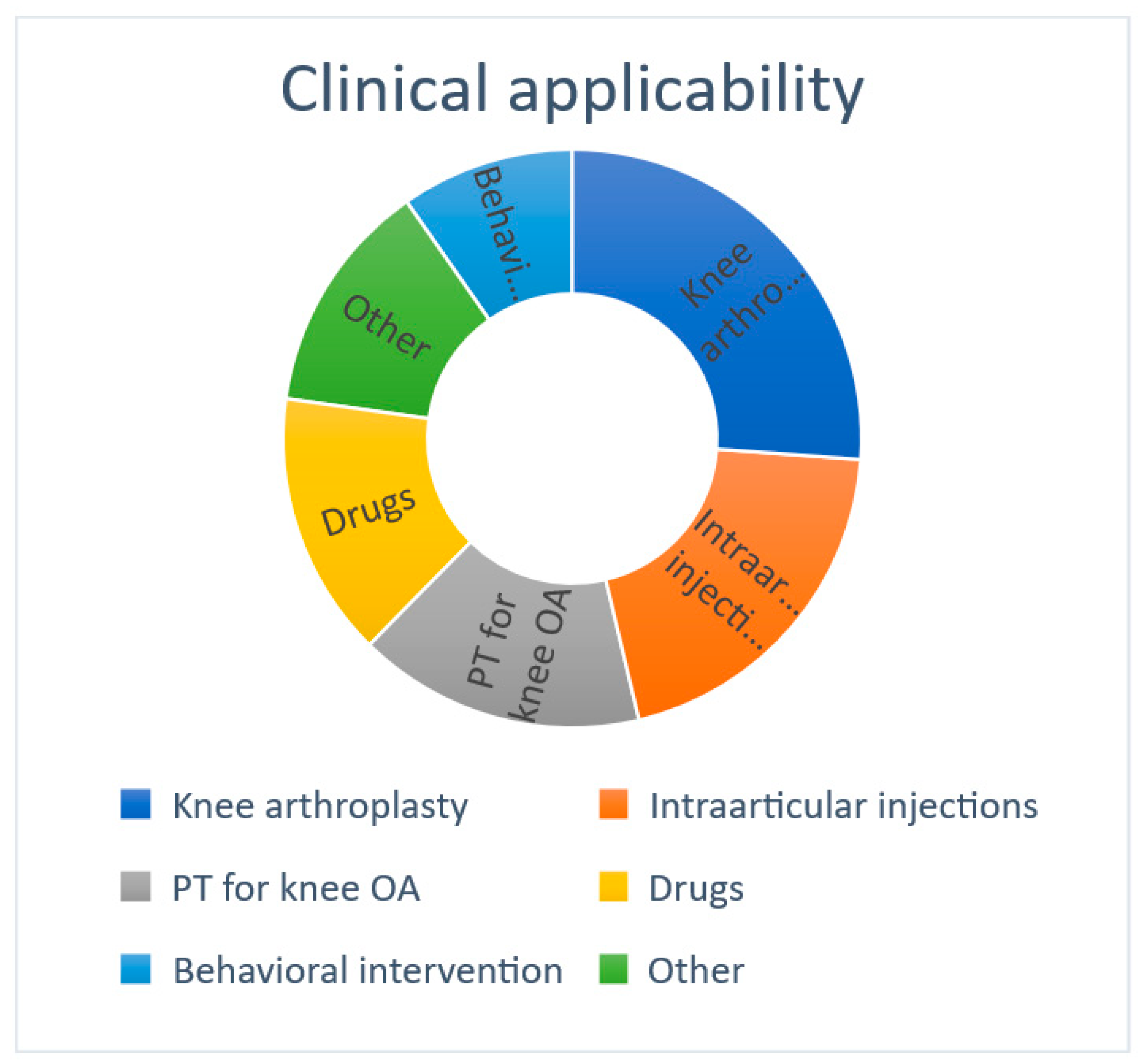
| Clinical Applicability | Number of Studies | % of Total Analyzed | Number of Subjects |
|---|---|---|---|
| Knee arthroplasty | 148 | 26.2 | 28,915 |
| Intraarticular injections | 114 | 20.2 | 15,269 |
| Physical therapy | 91 | 16.1 | 18,260 |
| Drugs | 84 | 14.9 | 18,608 |
| Behavioral intervention | 55 | 9.7 | 7804 |
| Other | 74 | 13.1 | 24,432 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ioniţescu, M.; Vermeşan, D.; Andor, B.; Dumitrascu, C.; Al-Qatawneh, M.; Bloanca, V.; Dumitrascu, A.; Prejbeanu, R. Potential New Treatments for Knee OA: A Prospective Review of Registered Trials. Appl. Sci. 2021, 11, 11049. https://0-doi-org.brum.beds.ac.uk/10.3390/app112211049
Ioniţescu M, Vermeşan D, Andor B, Dumitrascu C, Al-Qatawneh M, Bloanca V, Dumitrascu A, Prejbeanu R. Potential New Treatments for Knee OA: A Prospective Review of Registered Trials. Applied Sciences. 2021; 11(22):11049. https://0-doi-org.brum.beds.ac.uk/10.3390/app112211049
Chicago/Turabian StyleIoniţescu, Marius, Dinu Vermeşan, Bogdan Andor, Cristian Dumitrascu, Musab Al-Qatawneh, Vlad Bloanca, Andrei Dumitrascu, and Radu Prejbeanu. 2021. "Potential New Treatments for Knee OA: A Prospective Review of Registered Trials" Applied Sciences 11, no. 22: 11049. https://0-doi-org.brum.beds.ac.uk/10.3390/app112211049