
Biomechanical Consequences of Tibial Insert Thickness after Total Knee Arthroplasty: A Musculoskeletal Simulation Study



Abstract
:Featured Application
Abstract
1. Introduction
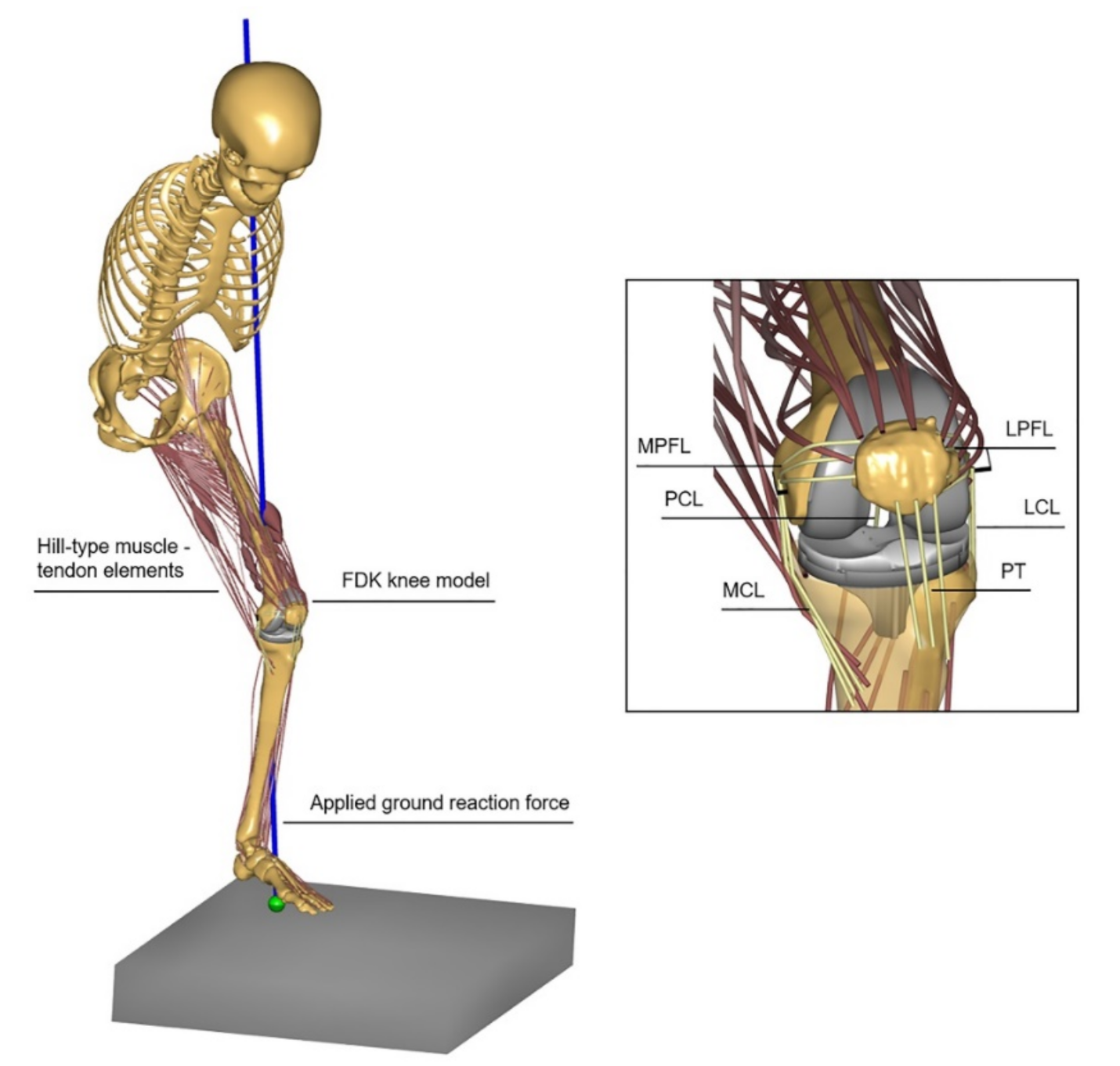
2. Materials and Methods
3. Results
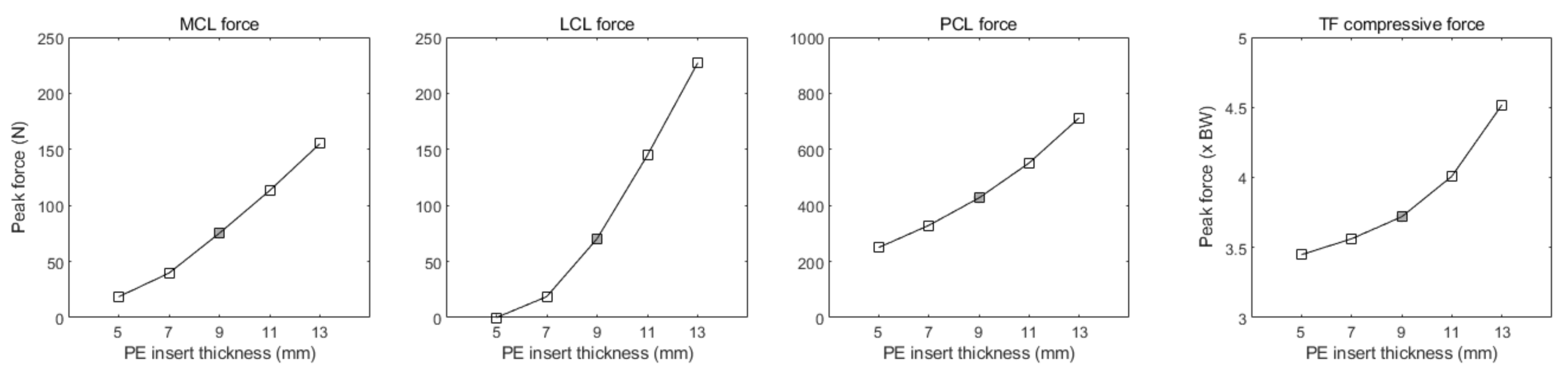
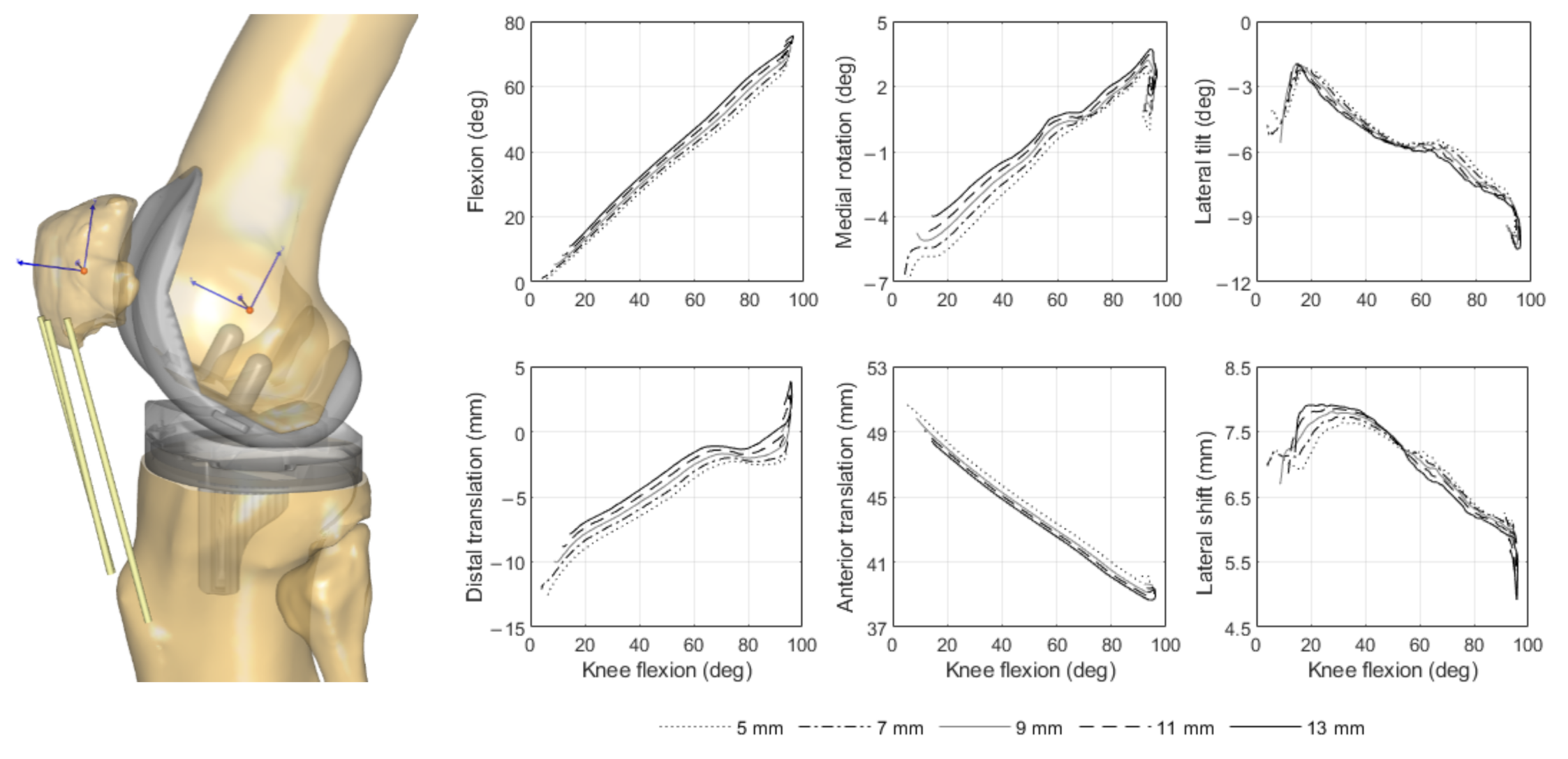
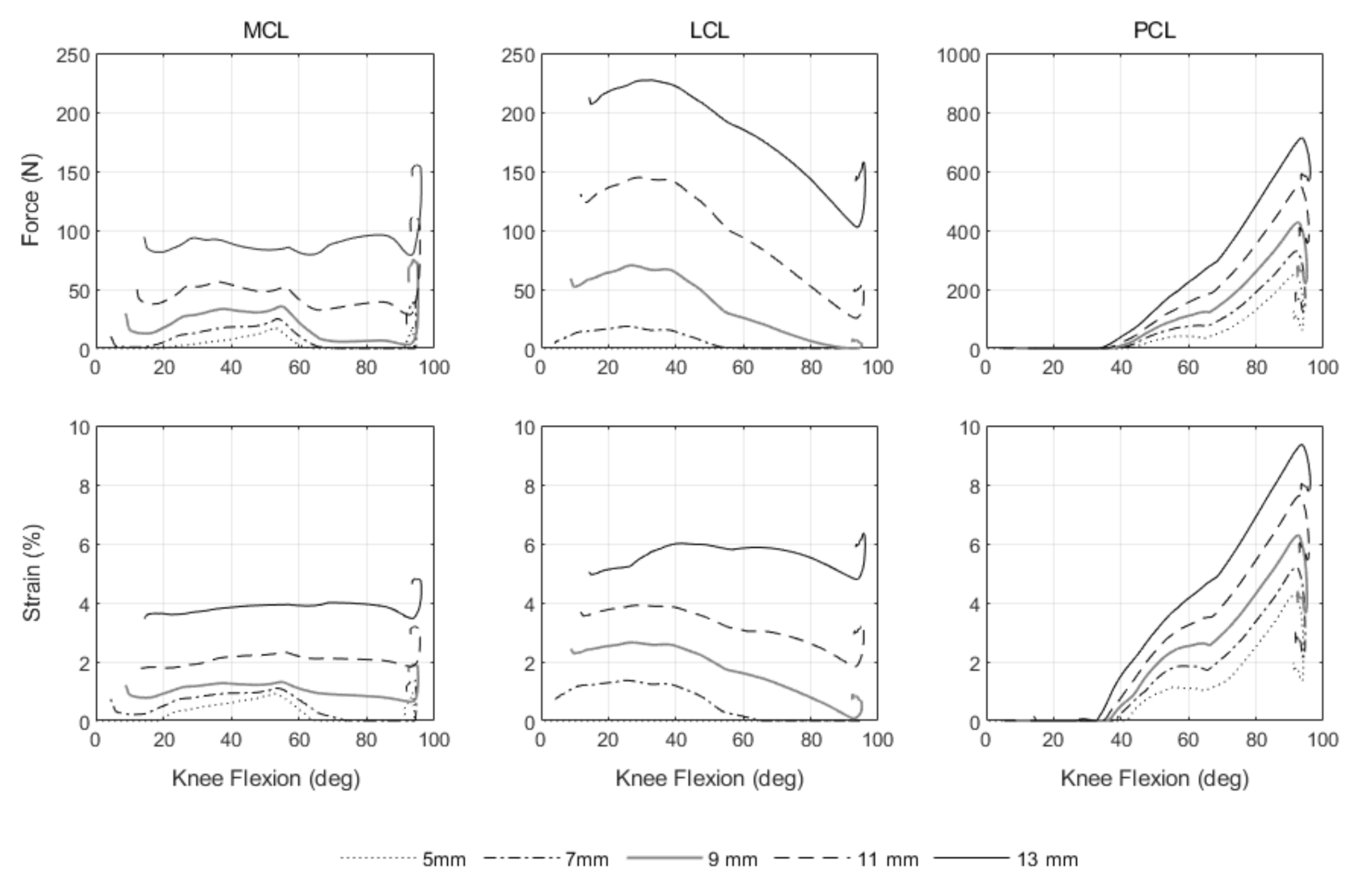
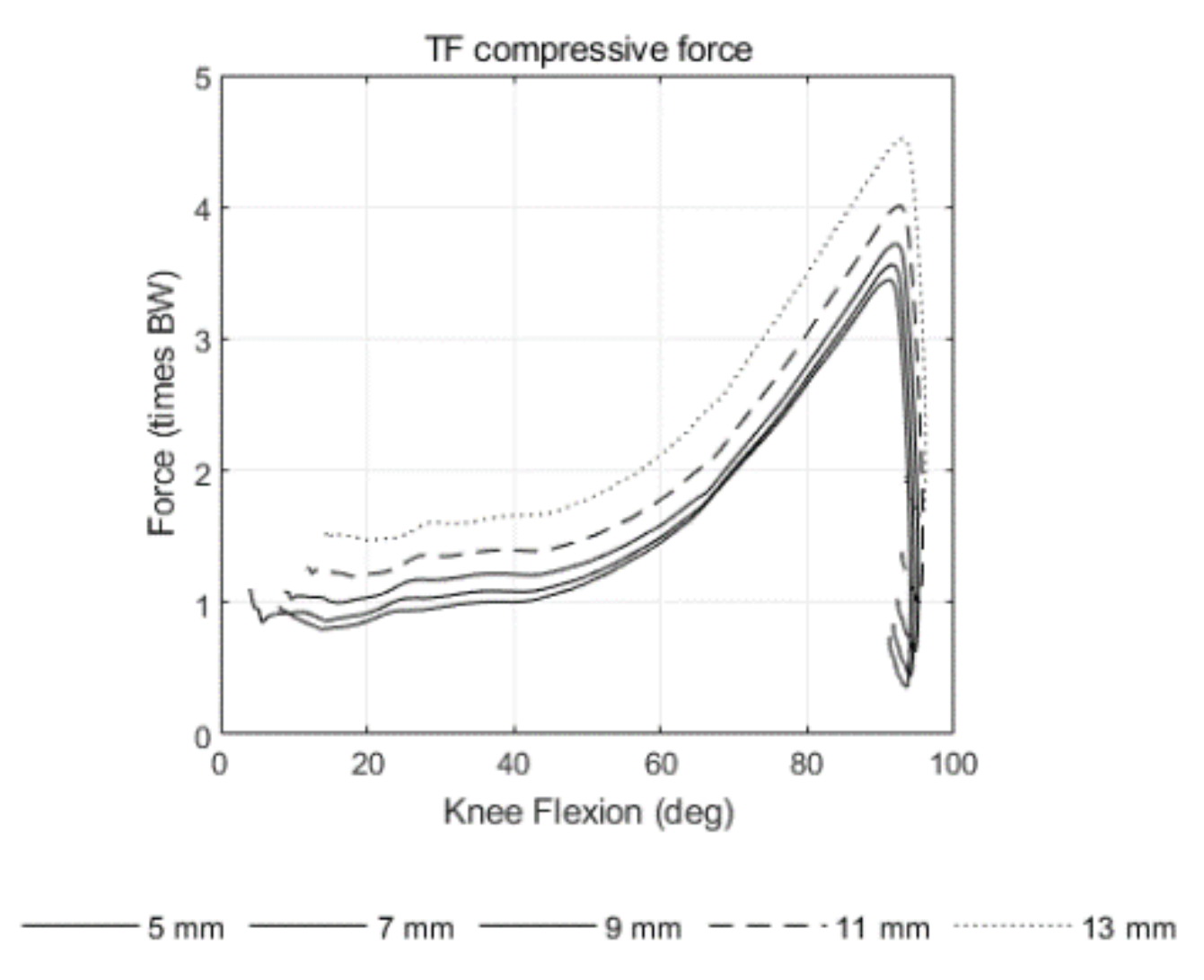
3.1. Tibiofemoral Joint
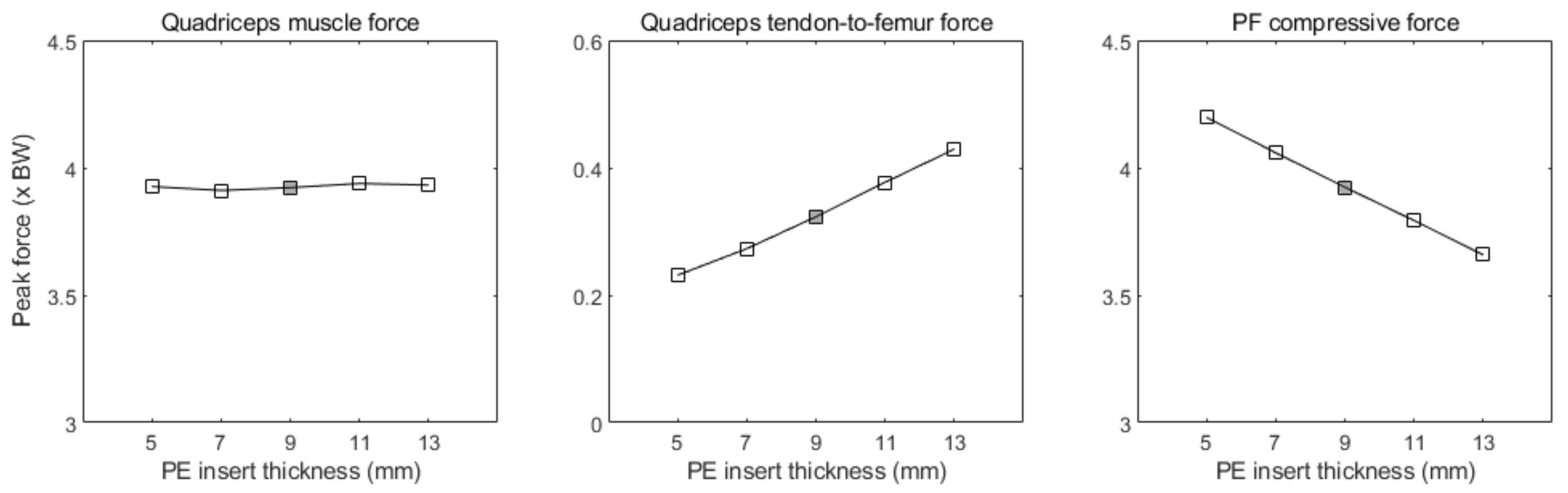
3.2. Patellofemoral Joint
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A



References
- Carr, A.J.; Robertsson, O.; Graves, S.; Price, A.J.; Arden, N.K.; Judge, A.; Beard, D.J. Knee replacement. Lancet 2012, 379, 1331–1340. [Google Scholar] [CrossRef]
- Hamilton, D.; Burnett, R.; Patton, J.; Howie, C.; Moran, M.; Simpson, A.; Gaston, P. Implant design influences patient outcome after total knee arthroplasty: A prospective double-blind randomised controlled trial. Bone Jt. J. 2015, 97, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Bonnin, M.P.; Schmidt, A.; Basiglini, L.; Bossard, N.; Dantony, E. Mediolateral oversizing influences pain, function, and flexion after TKA. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2314–2324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longstaff, L.M.; Sloan, K.; Stamp, N.; Scaddan, M.; Beaver, R. Good alignment after total knee arthroplasty leads to faster rehabilitation and better function. J. Arthroplast. 2009, 24, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, P.F.; Hozack, W.J.; Rothman, R.H.; Shastri, S.; Jacoby, S.M. Why are total knee arthroplasties failing today? Clin. Orthop. Relat. Res. 2002, 404, 7–13. [Google Scholar] [CrossRef]
- Edwards, S.; Pandit, H.; Ramos, J.; Grover, M. Analysis of polyethylene thickness of tibial components in total knee replacement. J. Bone Jt. Surg. Am. 2002, 84, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Lanting, B.A.; Snider, M.G.; Chess, D.G. Effect of polyethylene component thickness on range of motion and stability in primary total knee arthroplasty. J. Orthop. 2012, 35, e170–e174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartel, D.L.; Bicknell, V.; Wright, T.J.J. The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J. Bone Jt. Surg. Am. 1986, 68, 1041–1051. [Google Scholar] [CrossRef]
- Pijls, B.G.; Van der Linden-Van, H.M.; Nelissen, R.G. Polyethylene thickness is a risk factor for wear necessitating insert exchange. Int. Orthop. 2012, 36, 1175–1180. [Google Scholar] [CrossRef] [Green Version]
- Yoo, J.Y.; Cai, J.; Chen, A.F.; Austin, M.S.; Sharkey, P.F. Modular Polyethylene Inserts for Total Knee Arthroplasty: Can Surgeons Detect 1-mm Thickness Increments? J. Arthroplast. 2016, 31, 968–970. [Google Scholar] [CrossRef] [PubMed]
- Mueller, J.K.P.; Wentorf, F.A.; Moore, R.E. Femoral and tibial insert downsizing increases the laxity envelope in TKA. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 3003–3011. [Google Scholar] [CrossRef] [Green Version]
- Engh, G.A.; Dwyer, K.A.; Hanes, C.K. Polyethylene wear of metal-backed tibial components in total and unicompartmental knee prostheses. J. Bone Jt. Surg. Br. 1992, 74, 9–17. [Google Scholar] [CrossRef]
- Greco, N.J.; Crawford, D.A.; Berend, K.R.; Adams, J.B.; Lombardi, A.V., Jr. “Thicker” polyethylene bearings are not associated with higher failure rates in primary total knee arthroplasty. J. Arthroplast. 2018, 33, 2810–2814. [Google Scholar] [CrossRef] [PubMed]
- Berend, M.E.; Davis, P.J.; Ritter, M.A.; Keating, E.M.; Faris, P.M.; Meding, J.B.; Malinzak, R.A. “Thicker” polyethylene bearings are associated with higher failure rates in primary total knee arthroplasty. J. Arthroplast. 2010, 25, 17–20. [Google Scholar] [CrossRef]
- Ding, Z.; Nolte, D.; Kit Tsang, C.; Cleather, D.J.; Kedgley, A.E.; Bull, A.M. In vivo knee contact force prediction using patient-specific musculoskeletal geometry in a segment-based computational model. J. Biomech. Eng. 2016, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peersman, G.; Slane, J.; Dirckx, M.; Vandevyver, A.; Dworschak, P.; Heyse, T.J.; Scheys, L. The influence of polyethylene bearing thickness on the tibiofemoral kinematics of a bicruciate retaining total knee arthroplasty. Knee 2017, 24, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Marra, M.A.; Vanheule, V.; Fluit, R.; Koopman, B.; Rasmussen, J.; Verdonschot, N.; Andersen, M.S. A subject-specific musculoskeletal modeling framework to predict in vivo mechanics of total knee arthroplasty. J. Biomech. Eng. 2015, 137. [Google Scholar] [CrossRef] [PubMed]
- Carbone, V.; Fluit, R.; Pellikaan, P.; Van Der Krogt, M.; Janssen, D.; Damsgaard, M.; Vigneron, L.; Feilkas, T.; Koopman, H.F.; Verdonschot, N. TLEM 2.0–A comprehensive musculoskeletal geometry dataset for subject-specific modeling of lower extremity. J. Biomech. 2015, 48, 734–741. [Google Scholar] [CrossRef] [Green Version]
- Fregly, B.J.; Besier, T.F.; Lloyd, D.G.; Delp, S.L.; Banks, S.A.; Pandy, M.G.; D’lima, D.D. Grand challenge competition to predict in vivo knee loads. J. Orthop. Res. 2012, 30, 503–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skipper Andersen, M.; De Zee, M.; Damsgaard, M.; Nolte, D.; Rasmussen, J. Introduction to force-dependent kinematics: Theory and application to mandible modeling. J. Biomech. Eng. 2017, 139. [Google Scholar] [CrossRef] [PubMed]
- Damsgaard, M.; Rasmussen, J.; Christensen, S.T.; Surma, E.; De Zee, M. Analysis of musculoskeletal systems in the AnyBody Modeling System. Simul. Model. Pract. Theory 2006, 14, 1100–1111. [Google Scholar] [CrossRef]
- Butler, D.L.; Kay, M.D.; Stouffer, D.C. Comparison of material properties in fascicle-bone units from human patellar tendon and knee ligaments. J. Biomech. 1986, 19, 425–432. [Google Scholar] [CrossRef]
- Cook, L.E.; Klika, A.K.; Szubski, C.R.; Rosneck, J.; Molloy, R.; Barsoum, W.K. Functional outcomes used to compare single radius and multiradius of curvature designs in total knee arthroplasty. J. Knee Surg. 2012, 25, 249–254. [Google Scholar] [CrossRef]
- Rivière, C.; Iranpour, F.; Auvinet, E.; Howell, S.; Vendittoli, P.-A.; Cobb, J.; Parratte, S. Alignment options for total knee arthroplasty: A systematic review. Orthop. Traumatol. Surg. Res. 2017, 103, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Cohen, Z.A.; Mccarthy, D.M.; Kwak, S.D.; Legrand, P.; Fogarasi, F.; Ciaccio, E.J.; Ateshian, G.A. Knee cartilage topography, thickness, and contact areas from MRI: In-vitro calibration and in-vivo measurements. Osteoarthr. Cartil. 1999, 7, 95–109. [Google Scholar] [CrossRef] [Green Version]
- Blankevoort, L.; Kuiper, J.; Huiskes, R.; Grootenboer, H. Articular contact in a three-dimensional model of the knee. J. Biomech. 1991, 24, 1019–1031. [Google Scholar] [CrossRef] [Green Version]
- Ellis, M.; Seedhom, B.; Wright, V. Forces in the knee joint whilst rising from a seated position. J. Biomed. Eng. 1984, 6, 113–120. [Google Scholar] [CrossRef]
- Nagura, T.; Matsumoto, H.; Kiriyama, Y.; Chaudhari, A.; Andriacchi, T.P. Tibiofemoral joint contact force in deep knee flexion and its consideration in knee osteoarthritis and joint replacement. J. Appl. Biomech. 2006, 22, 305–313. [Google Scholar] [CrossRef] [Green Version]
- Schnurr, C.; Csécsei, G.; Nessler, J.; Eysel, P.; König, D.P. How much tibial resection is required in total knee arthroplasty? Int. Orthop. 2011, 35, 989–994. [Google Scholar] [CrossRef] [Green Version]
- Kebbach, M.; Grawe, R.; Geier, A.; Winter, E.; Bergschmidt, P.; Kluess, D.; D’Lima, D.; Woernle, C.; Bader, R. Effect of surgical parameters on the biomechanical behaviour of bicondylar total knee endoprostheses–A robot-assisted test method based on a musculoskeletal model. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Onishi, Y.; Hino, K.; Watanabe, S.; Watamori, K.; Kutsuna, T.; Miura, H. The influence of tibial resection on the PCL in PCL-retaining total knee arthroplasty: A clinical and cadaveric study. J. Orthop. Sci. 2016, 21, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Marra, M.A.; Strzelczak, M.; Heesterbeek, P.J.; van de Groes, S.A.; Janssen, D.W.; Koopman, B.F.; Wymenga, A.B.; Verdonschot, N.J. Anterior referencing of tibial slope in total knee arthroplasty considerably influences knee kinematics: A musculoskeletal simulation study. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1540–1548. [Google Scholar] [CrossRef] [PubMed]
- Scott, C.; Howie, C.; MacDonald, D.; Biant, L. Predicting dissatisfaction following total knee replacement: A prospective study of 1217 patients. J. Bone Jt. Surg. Br. 2010, 92, 1253–1258. [Google Scholar] [CrossRef]
- Petersen, W.; Rembitzki, I.V.; Brüggemann, G.-P.; Ellermann, A.; Best, R.; Gösele-Koppenburg, A.; Liebau, C. Anterior knee pain after total knee arthroplasty: A narrative review. Int. Orthop. 2014, 38, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Laubach, M.; Hellmann, J.T.; Dirrichs, T.; Gatz, M.; Quack, V.; Tingart, M.; Betsch, M. Anterior knee pain after total knee arthroplasty: A multifactorial analysis. J. Orthop. Surg. 2020, 28. [Google Scholar] [CrossRef]
- Chonko, D.J.; Lombardi, A.V., Jr.; Berend, K.R. Patella baja and total knee arthroplasty (TKA): Etiology, diagnosis, and management. Surg. Technol. Int. 2004, 12, 231–238. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference PE Insert Thickness 9 mm | ||||||||
|---|---|---|---|---|---|---|---|---|
| −4 mm | −2 mm | +2 mm | +4 mm | |||||
| Average Difference | Peak Difference | Average Difference | Peak Difference | Average Difference | Peak Difference | Average Difference | Peak Difference | |
| Tibiofemoral joint | ||||||||
| MCL force | −89% | −75% | −59% | −47% | +100% | +51% | +251% | +106% |
| LCL force | −100% | −100% | −83% | −73% | +210% | +106% | +554% | +223% |
| PCL force | −53% | −41% | −31% | −23% | +43% | +29% | +104% | +67% |
| Compressive force | −21% | −7% | −9%% | −4% | +17% | +8% | +44% | +21% |
| Patellofemoral joint | ||||||||
| Quadriceps muscle force | +4% | 0% | +1% | 0% | 0% | 0% | −1% | 0% |
| Quadriceps tendon-to-femur force | −30% | −28% | −15% | −15% | +15% | +17% | +29% | +33% |
| Compressive force | +3% | +7% | +3% | +3% | −3% | −3% | −8% | −7% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tzanetis, P.; Marra, M.A.; Fluit, R.; Koopman, B.; Verdonschot, N. Biomechanical Consequences of Tibial Insert Thickness after Total Knee Arthroplasty: A Musculoskeletal Simulation Study. Appl. Sci. 2021, 11, 2423. https://0-doi-org.brum.beds.ac.uk/10.3390/app11052423
Tzanetis P, Marra MA, Fluit R, Koopman B, Verdonschot N. Biomechanical Consequences of Tibial Insert Thickness after Total Knee Arthroplasty: A Musculoskeletal Simulation Study. Applied Sciences. 2021; 11(5):2423. https://0-doi-org.brum.beds.ac.uk/10.3390/app11052423
Chicago/Turabian StyleTzanetis, Periklis, Marco A. Marra, René Fluit, Bart Koopman, and Nico Verdonschot. 2021. "Biomechanical Consequences of Tibial Insert Thickness after Total Knee Arthroplasty: A Musculoskeletal Simulation Study" Applied Sciences 11, no. 5: 2423. https://0-doi-org.brum.beds.ac.uk/10.3390/app11052423