
IoT and Deep Learning Based Approach for Rapid Screening and Face Mask Detection for Infection Spread Control of COVID-19

 ,
,  ,
, 
 , and
, and
Abstract
:1. Introduction
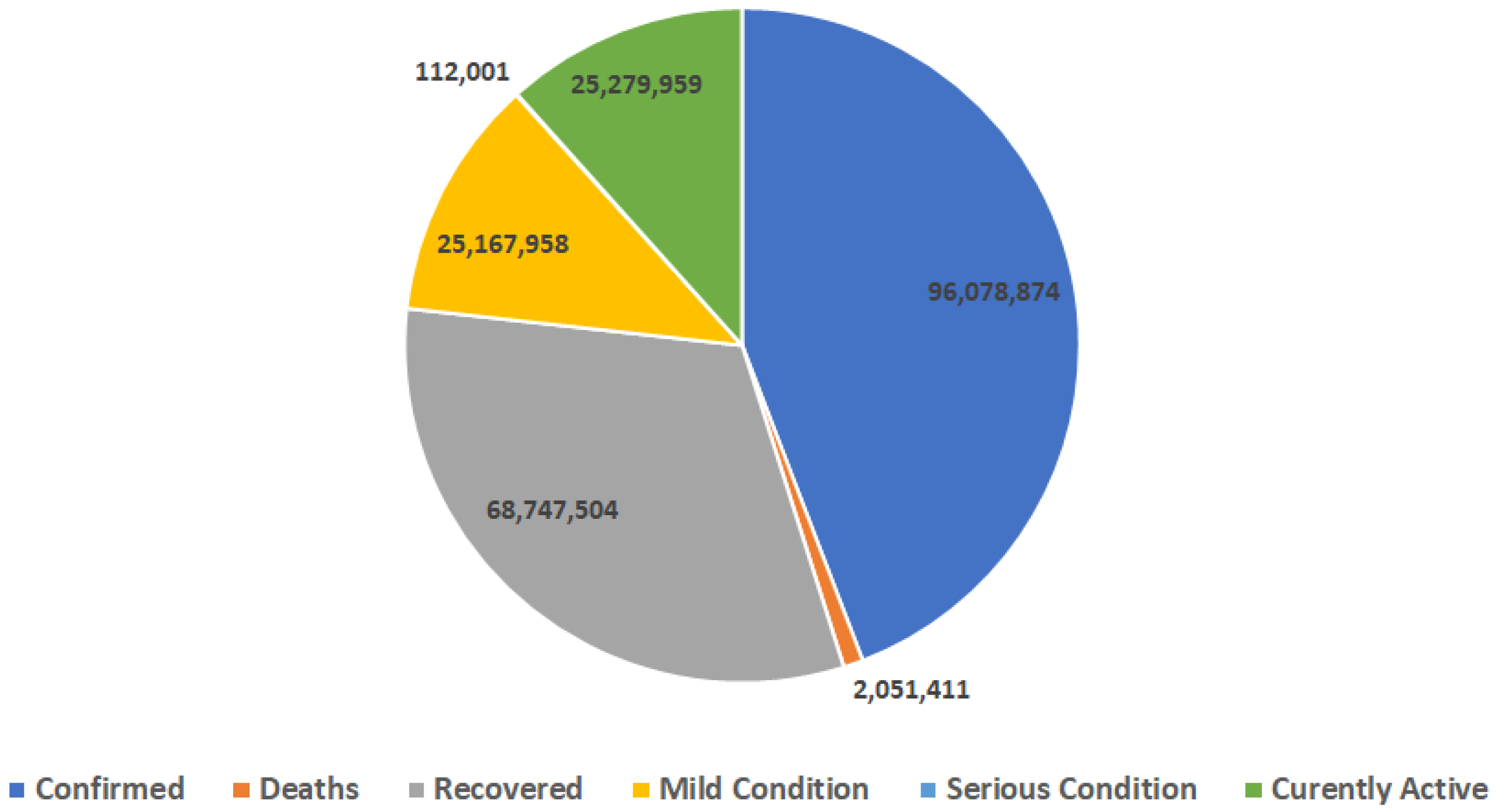
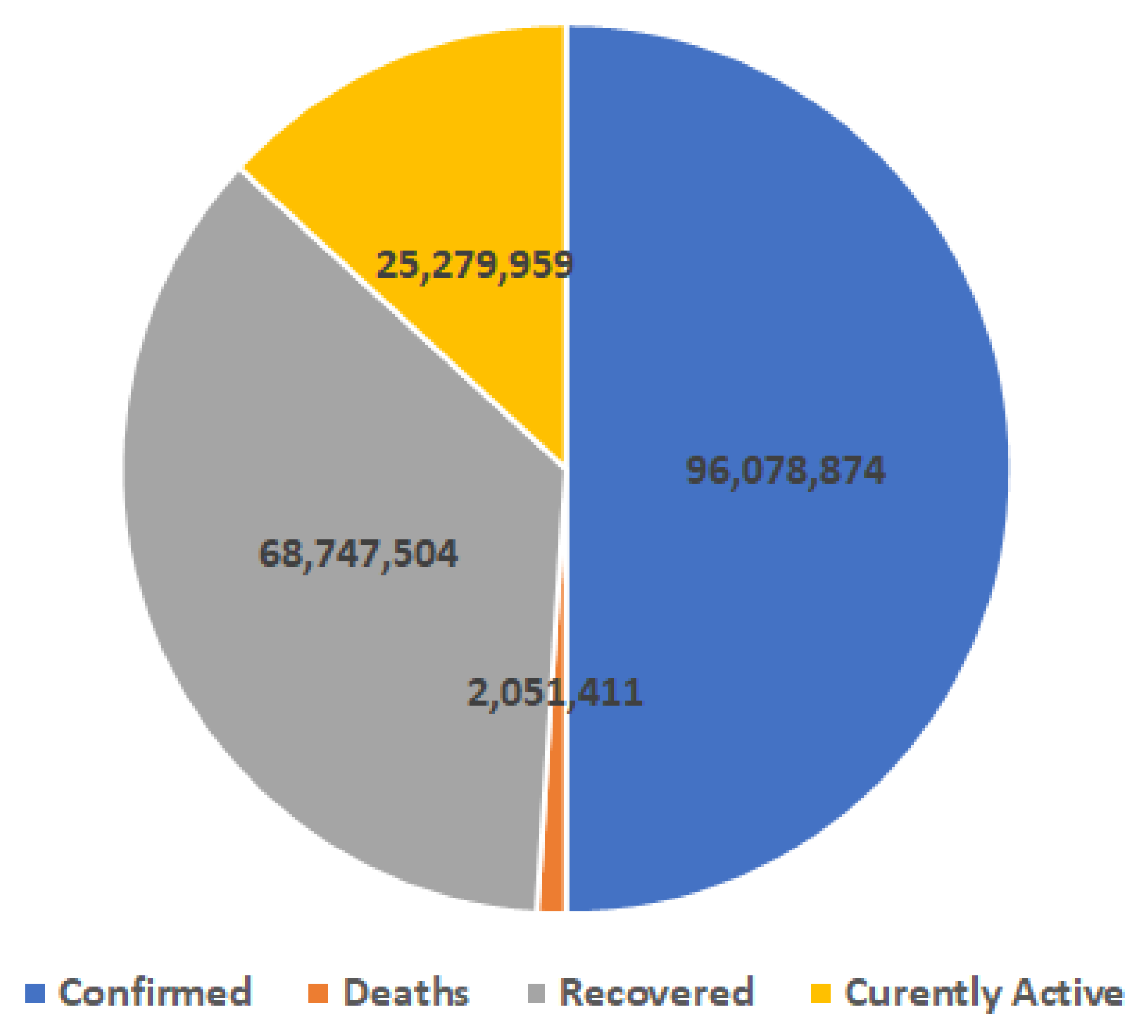
1.1. Worldwide Situation of COVID-19
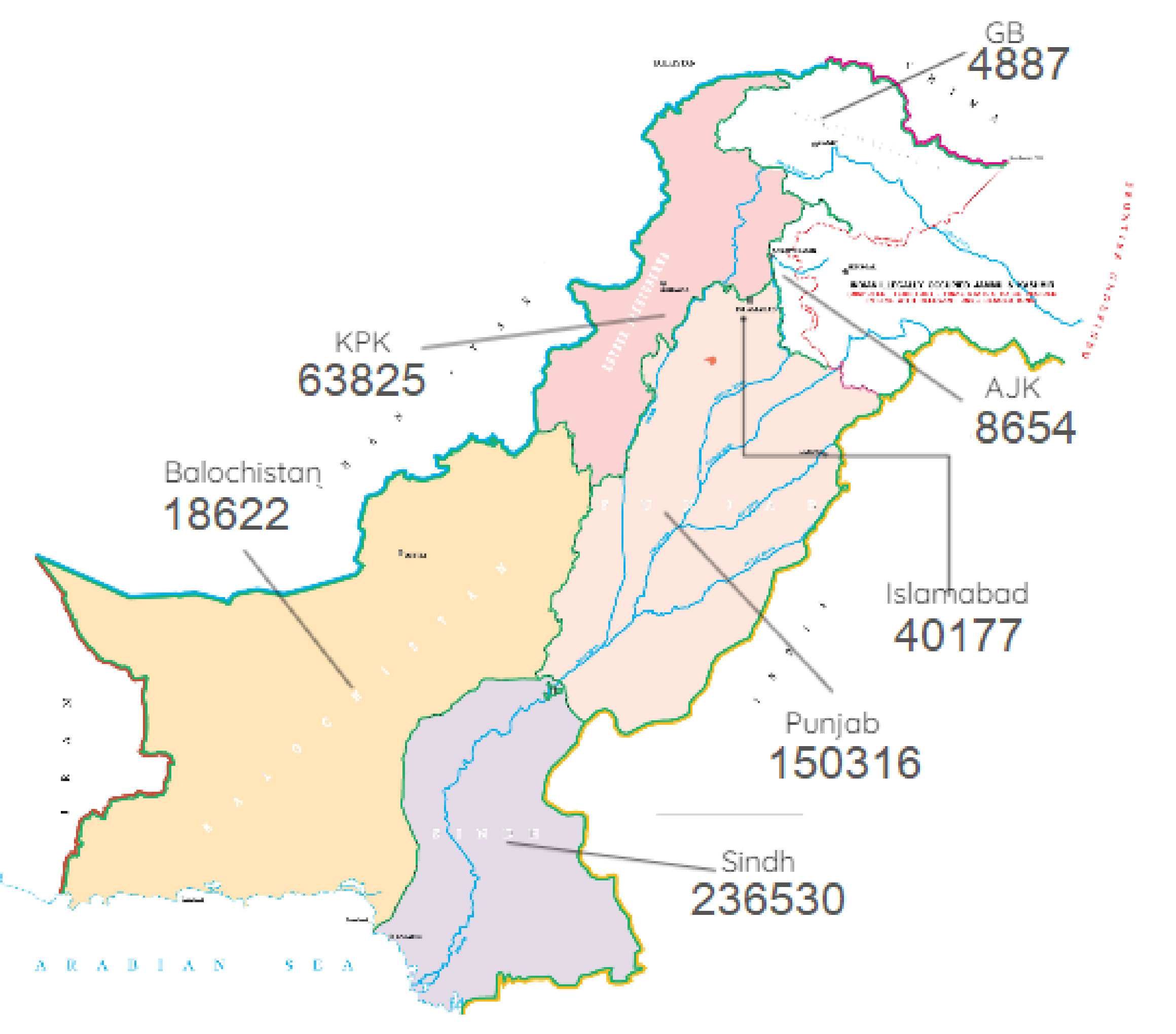
1.2. Pakistan’s Situation of COVID-19
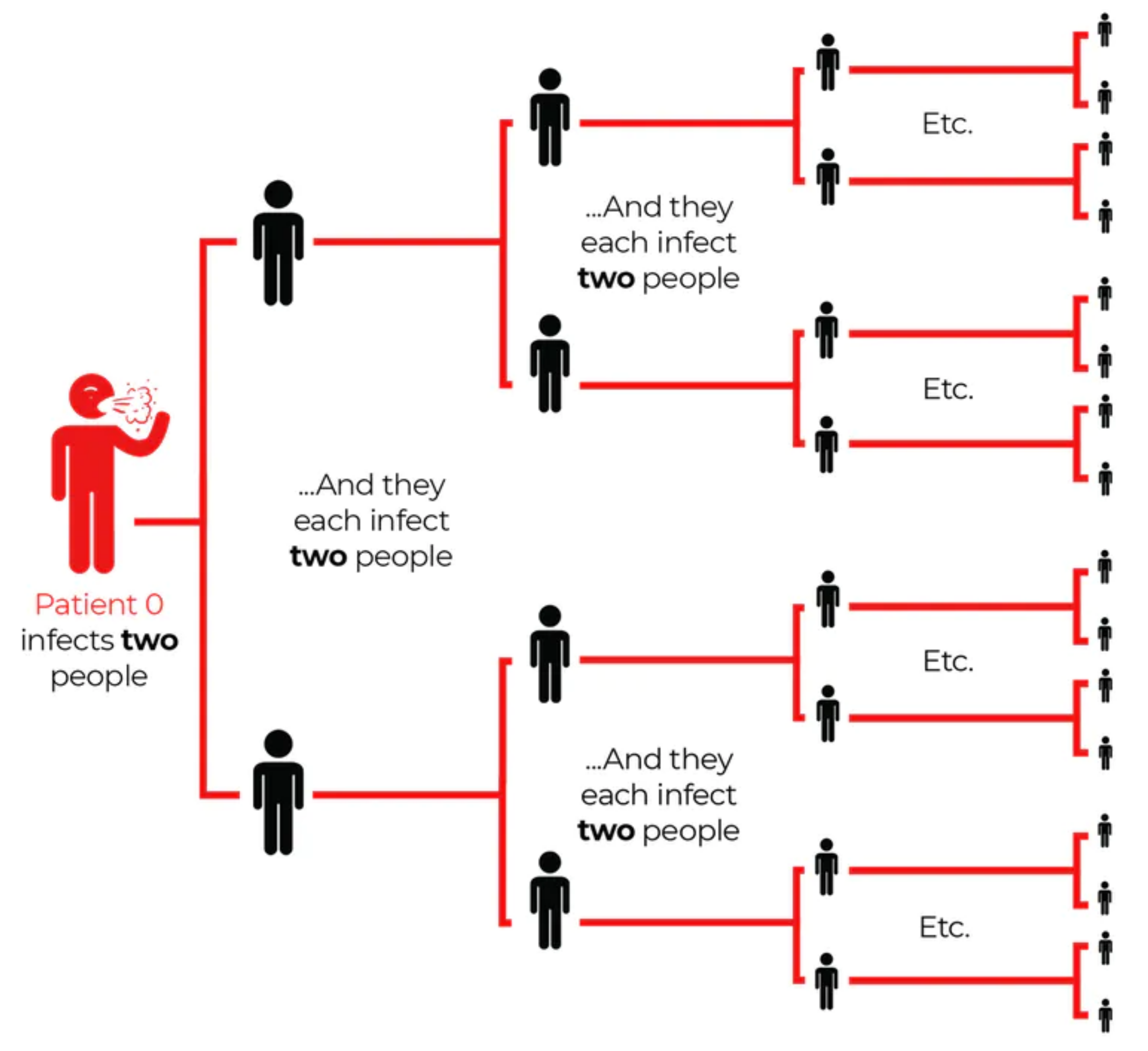
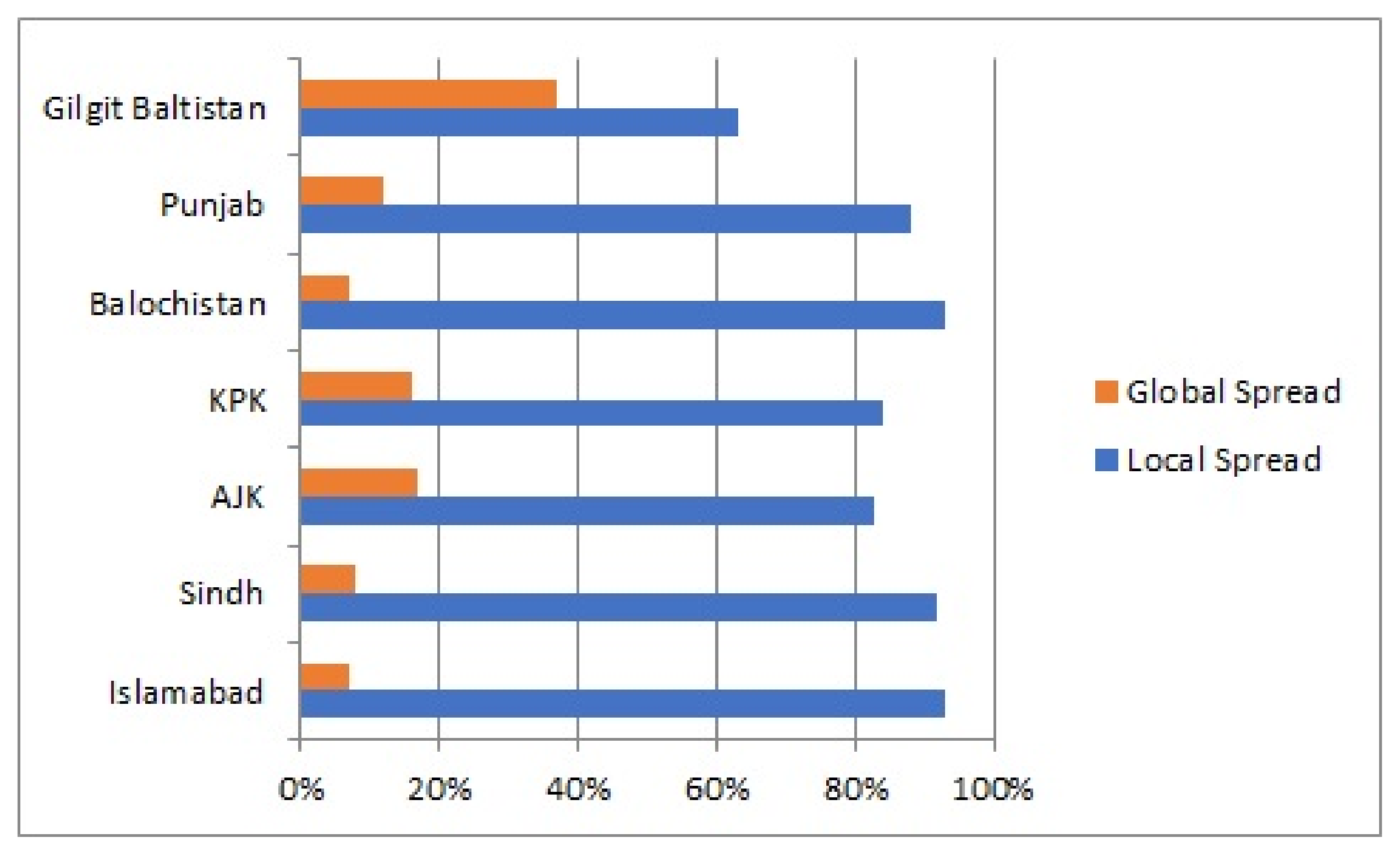
1.3. Local Transmission in Pakistan
1.4. Motivation and Contribution
- Our proposed SSDWG includes multi-features to disinfect many people from the COVID-19 without using a manual disinfection system.
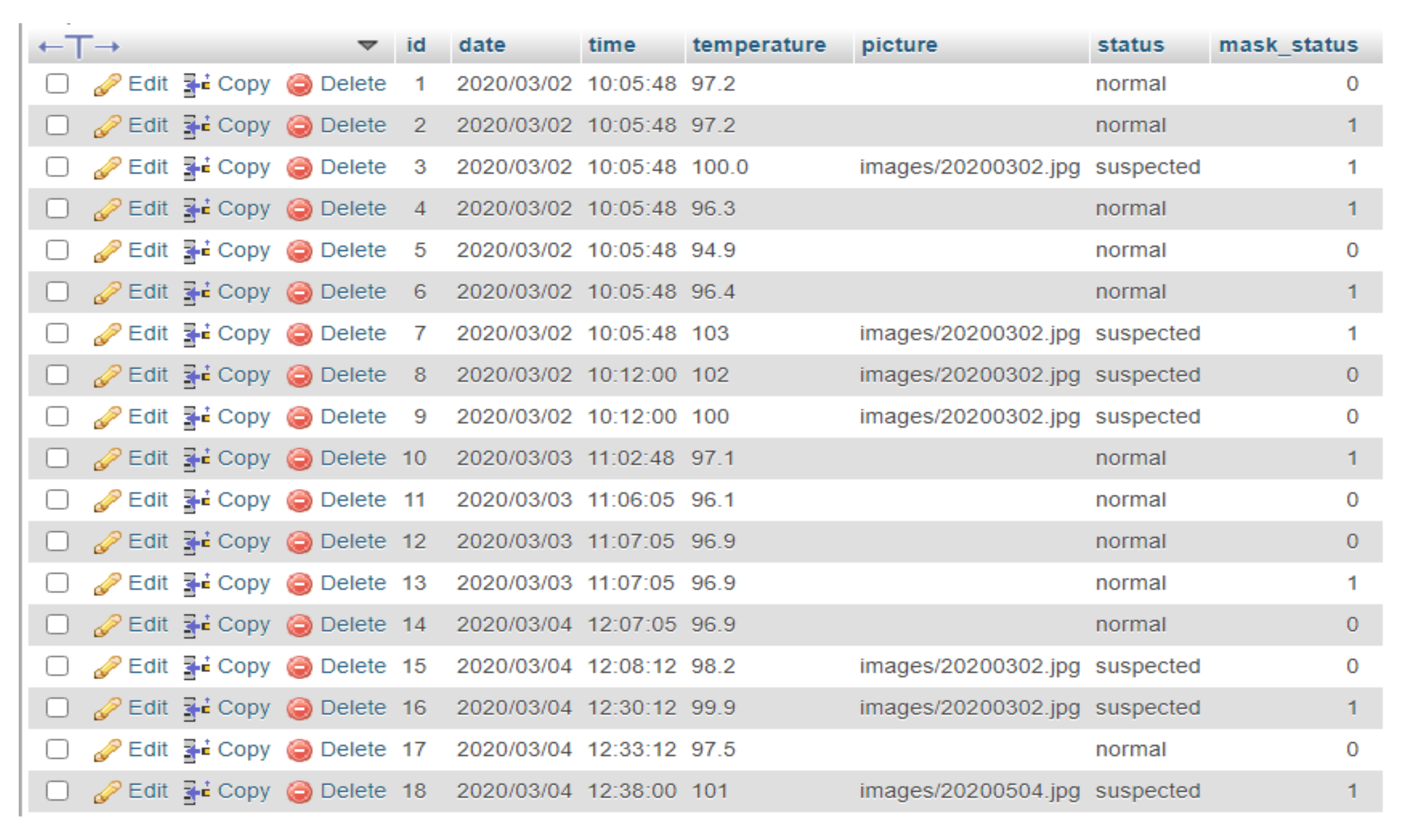
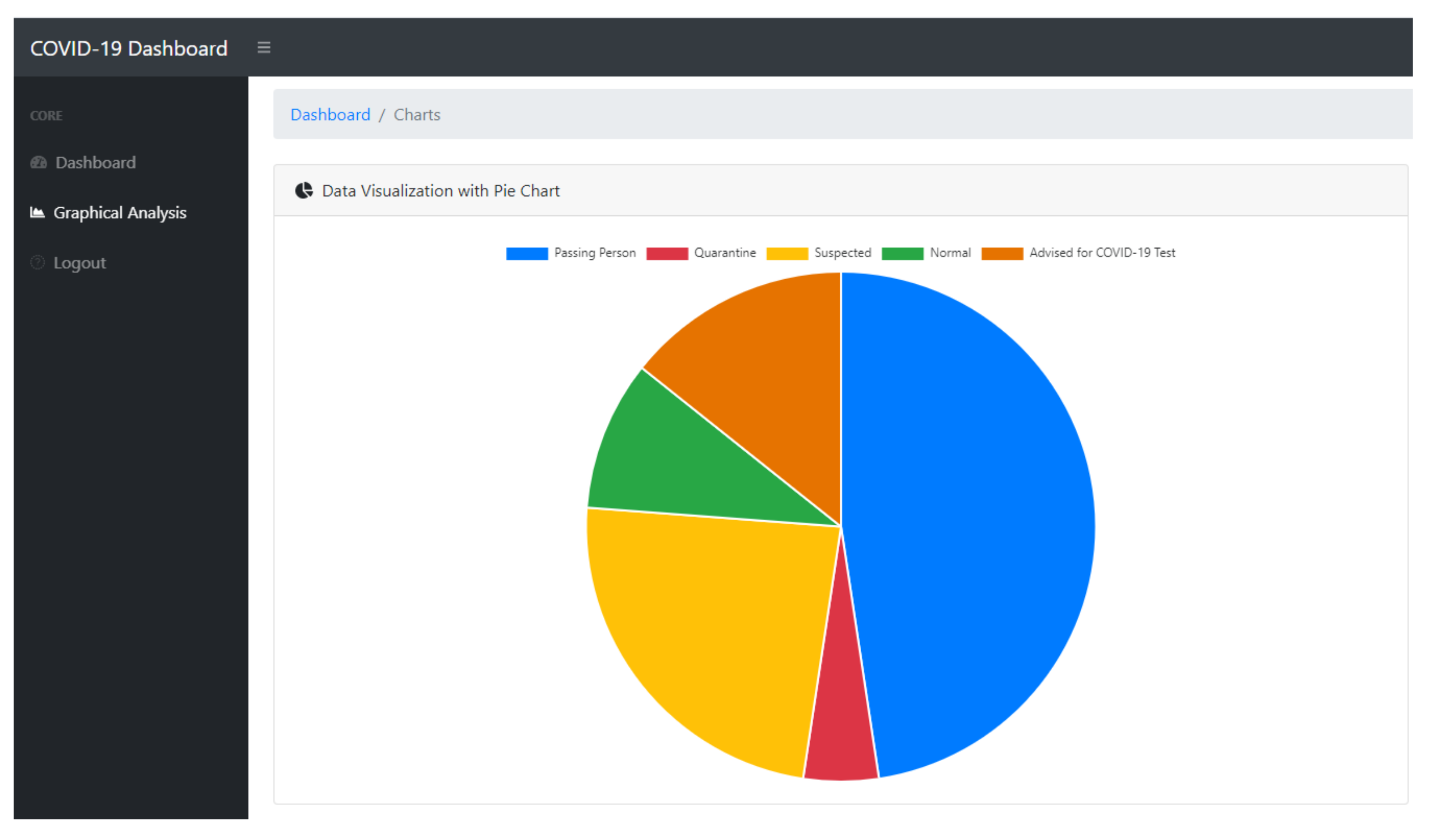
- Our proposed system can help to track vulnerable individuals’ records for further trace and control.
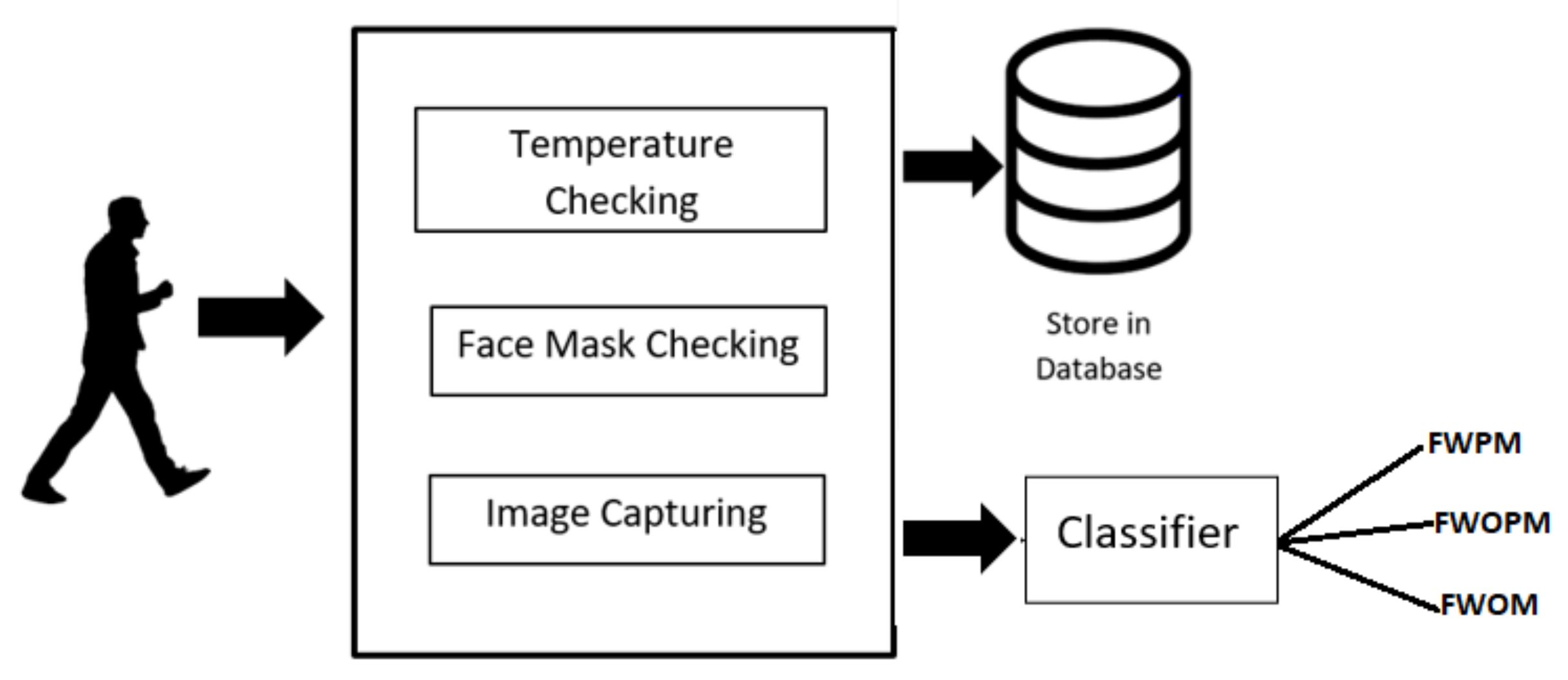
- The proposed model also includes the module to check an individual’s temperature while using a contact-free temperature sensor without any human intervention and store the temperature in the database.
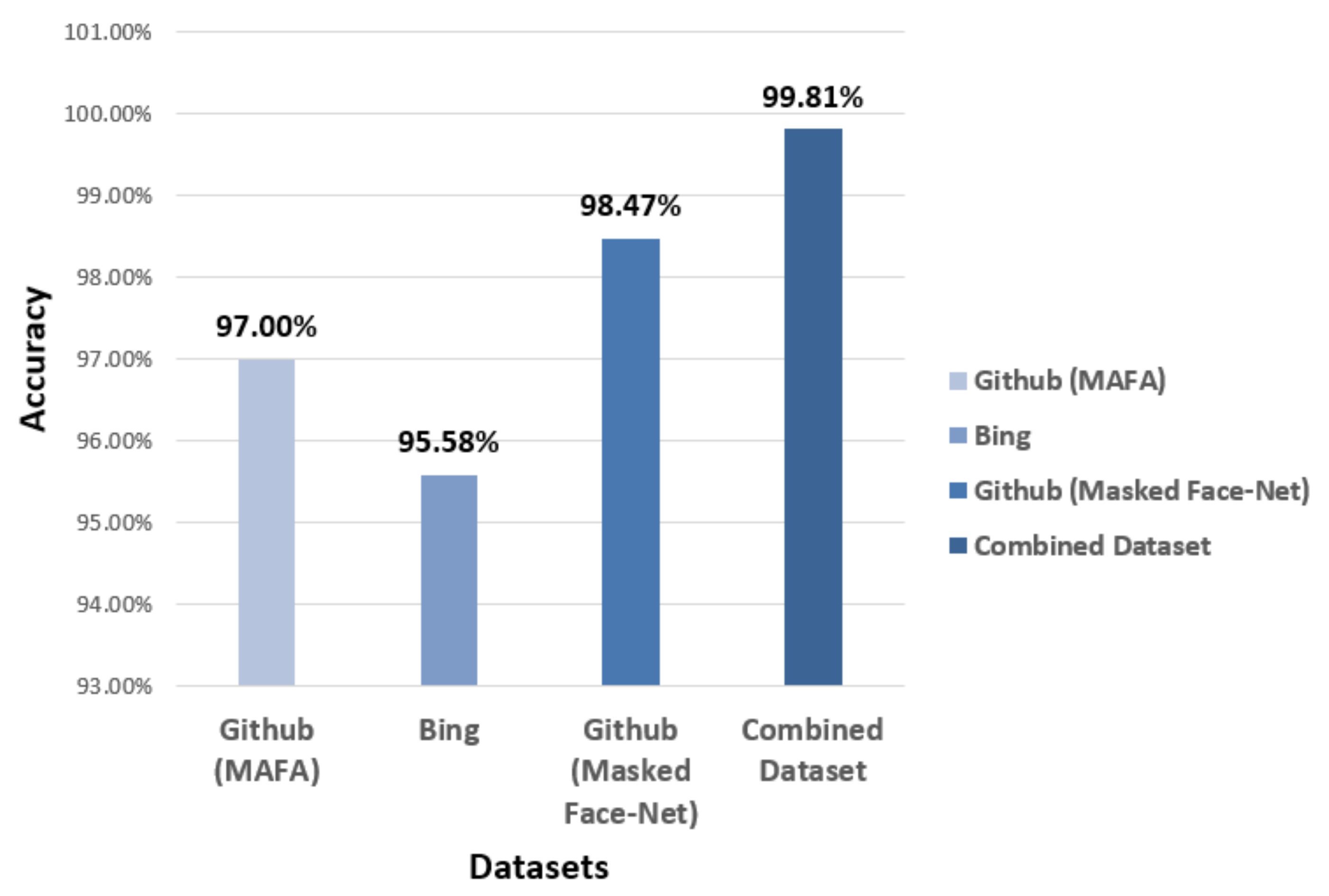
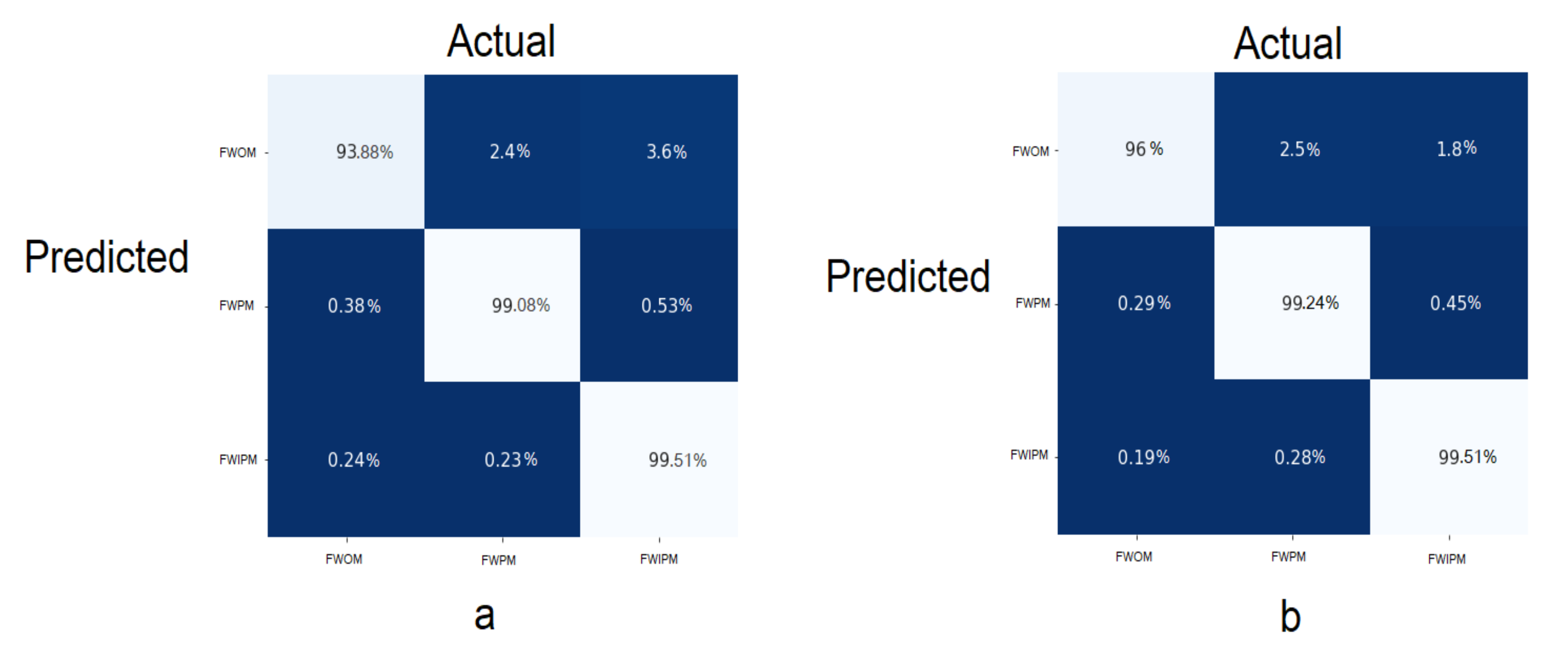
- According to the WHO, wearing a face mask in public places can protect an individual from COVID-19, as evidenced by experiments. The second module of SSDWG is to detect individuals wearing a mask or not and classify individuals in three classes, which are face with proper mask (FWPM), face with improper mask (FWIPM), and face without a mask (FWOM). In this module, we trained our machine learning models using three datasets, and we attained significant accuracy.
- The sub-module of our face mask identification system is to identify the types of face masks, either N-95 or surgical masks.
2. Related Work
2.1. IoT Healthcare Systems
2.2. Role of Artificial Intelligence (AI) in COVID-19 Pandemic
3. Materials and Methods
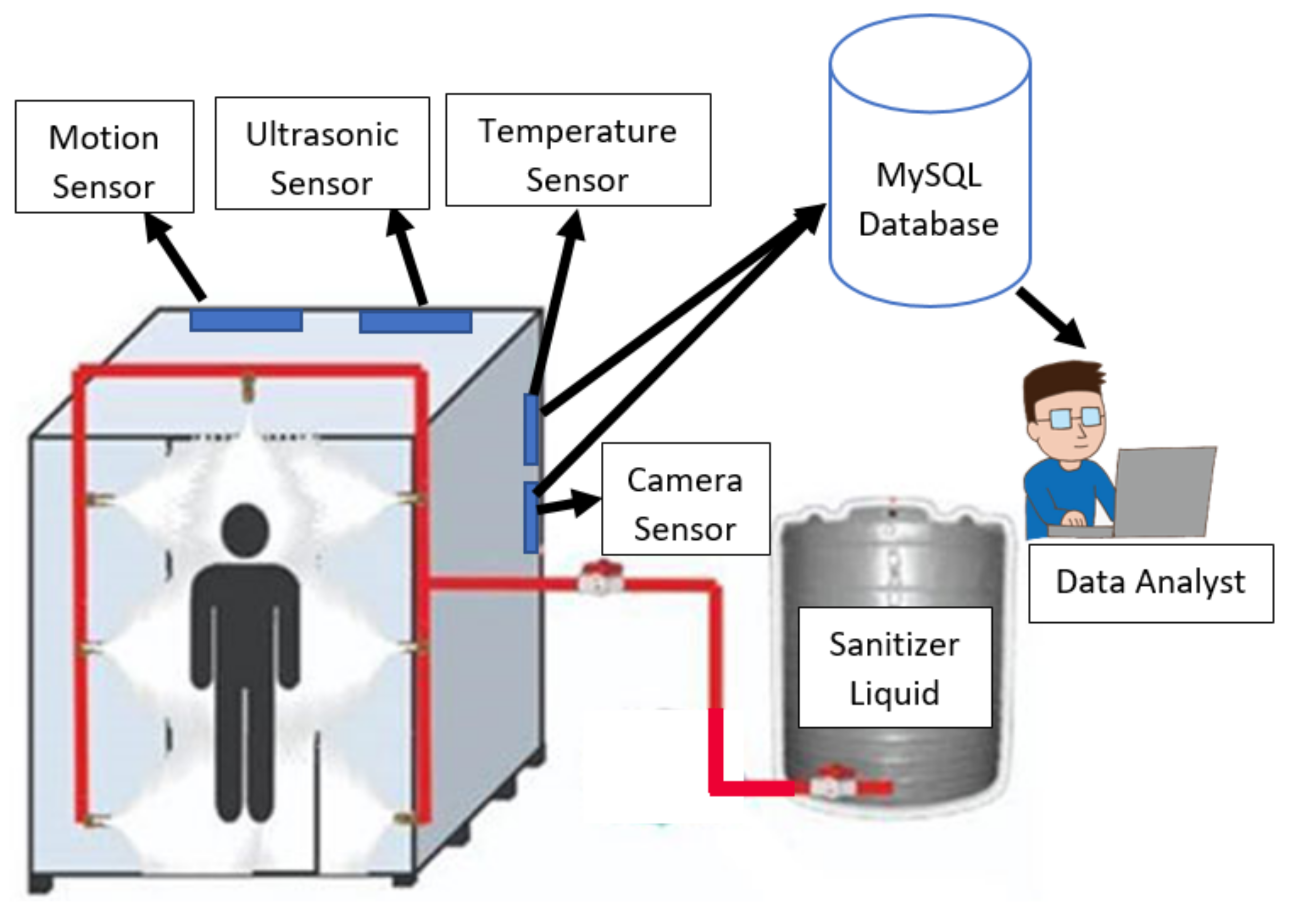
3.1. IoT Based Smart Screening and Disinfection Walkthrough Gate (SSDWG)
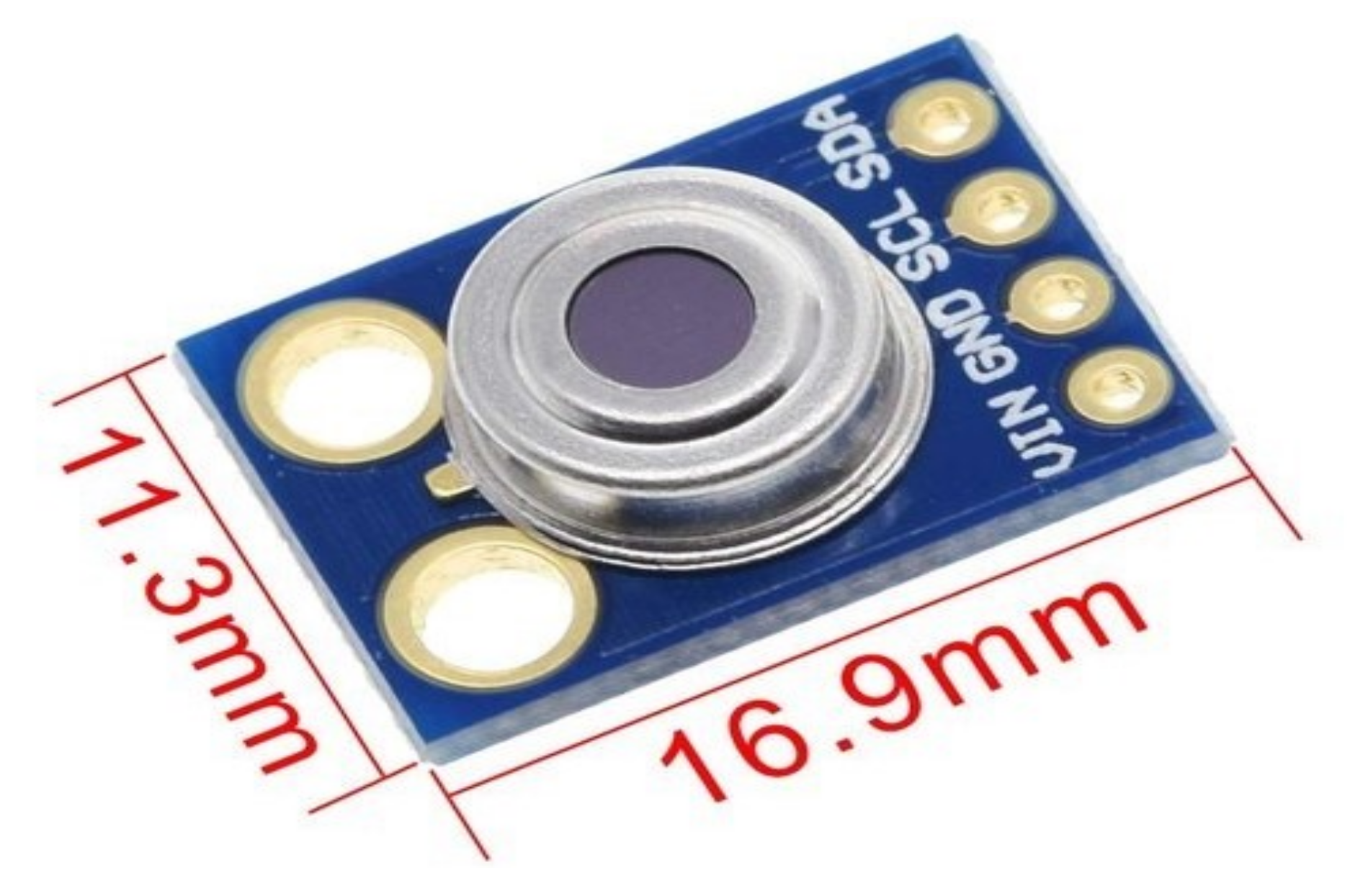
3.2. Body Temperature Detection
3.3. Mask Detection Module
3.3.1. Dataset
3.3.2. Fine-Tuning with Transfer Learning
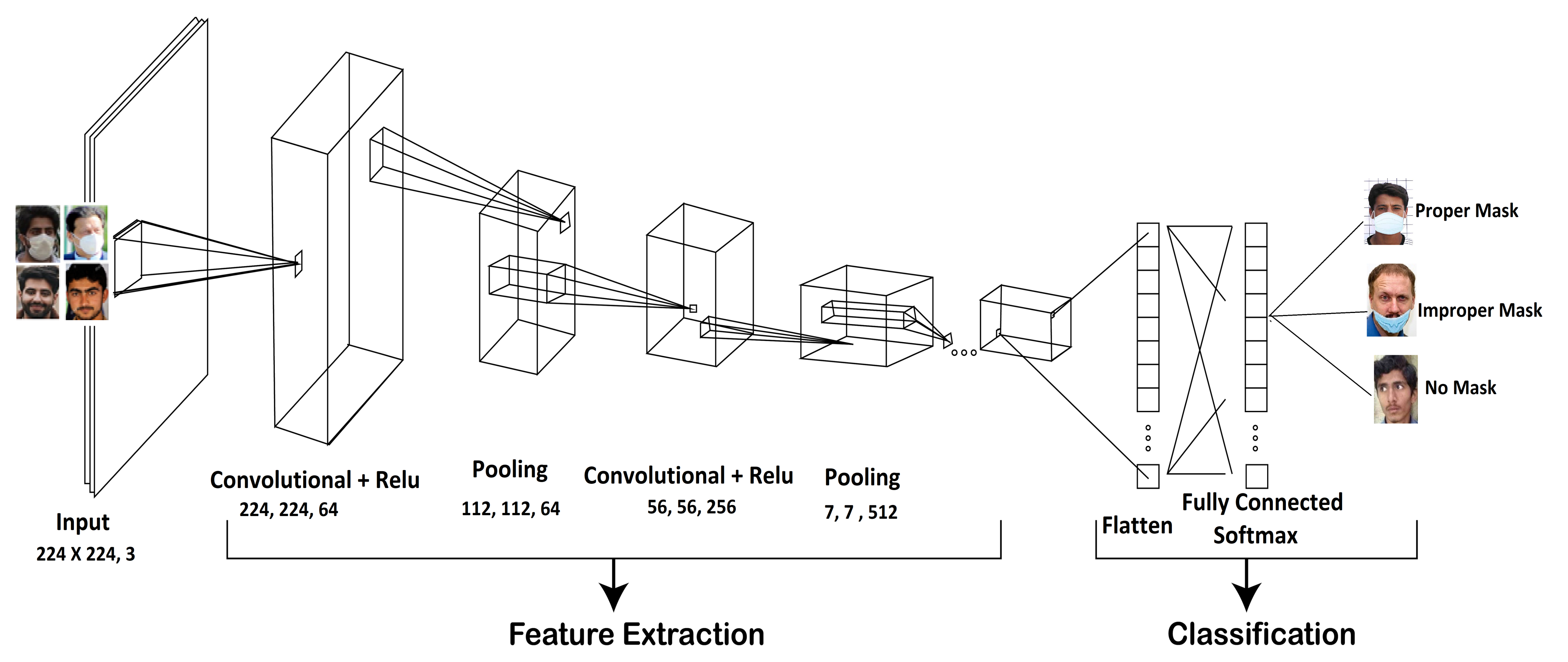
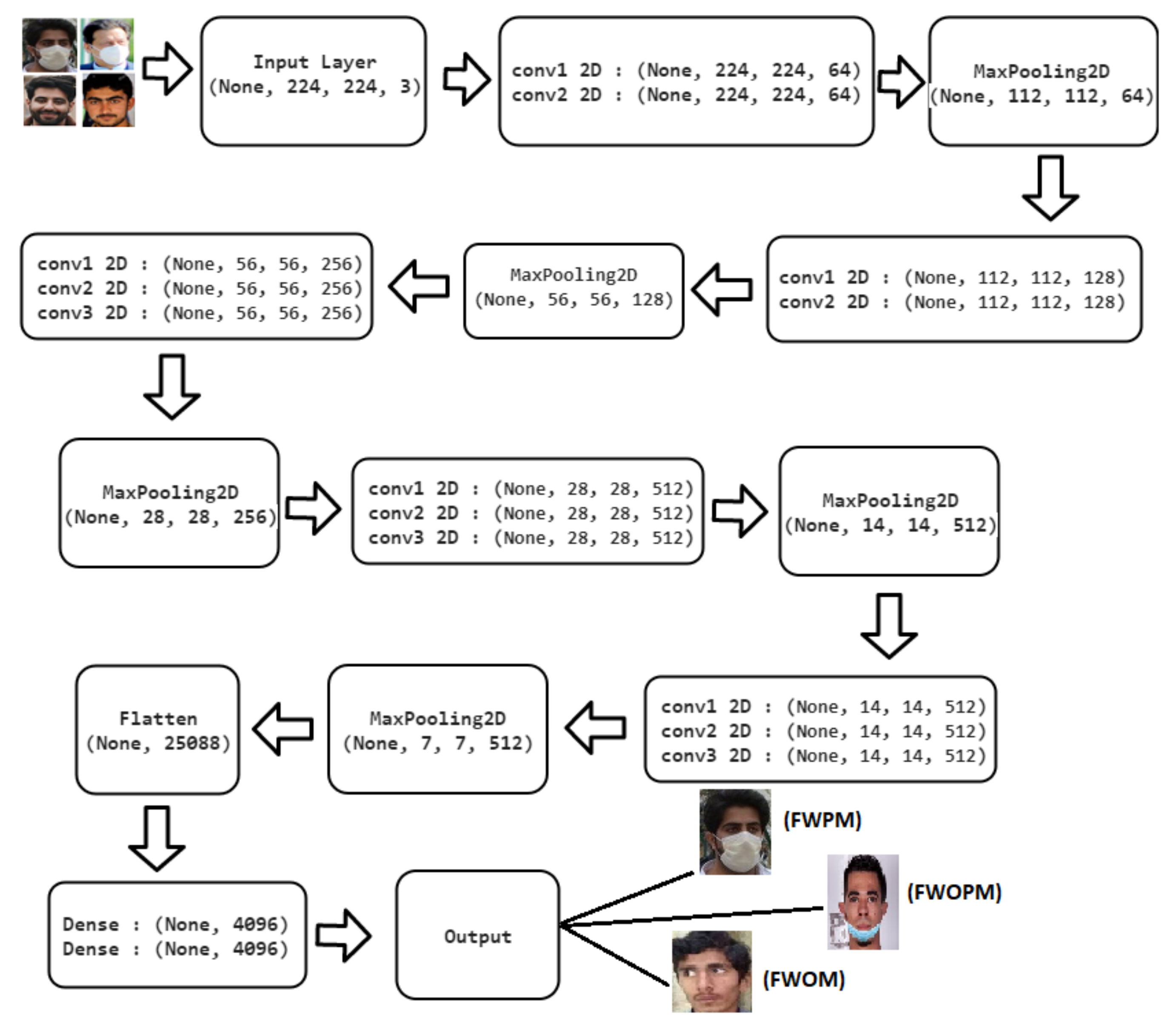
3.3.3. The VGG-16
3.3.4. ResNet-50
3.3.5. Inception V3
3.3.6. MobileNetV2
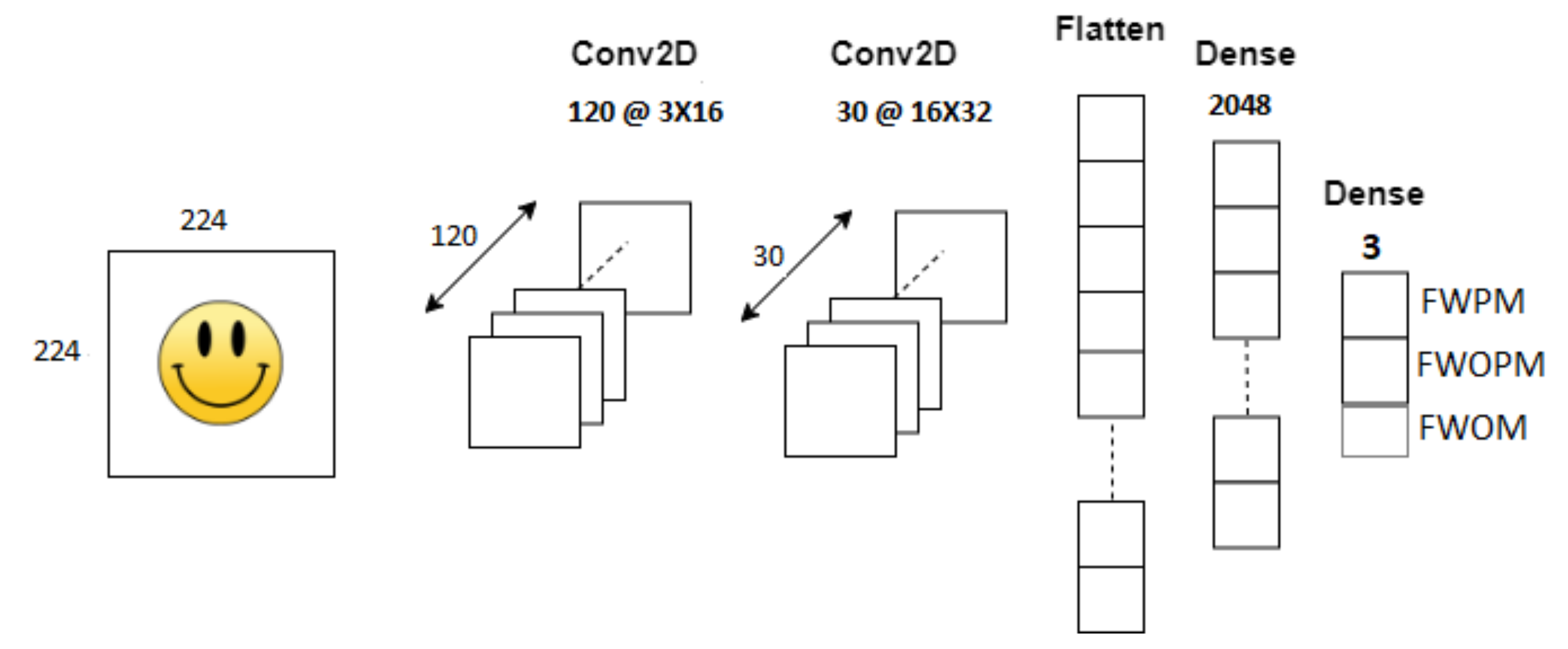
3.3.7. Convolutional Neural Network (CNN)
4. Experimental Results
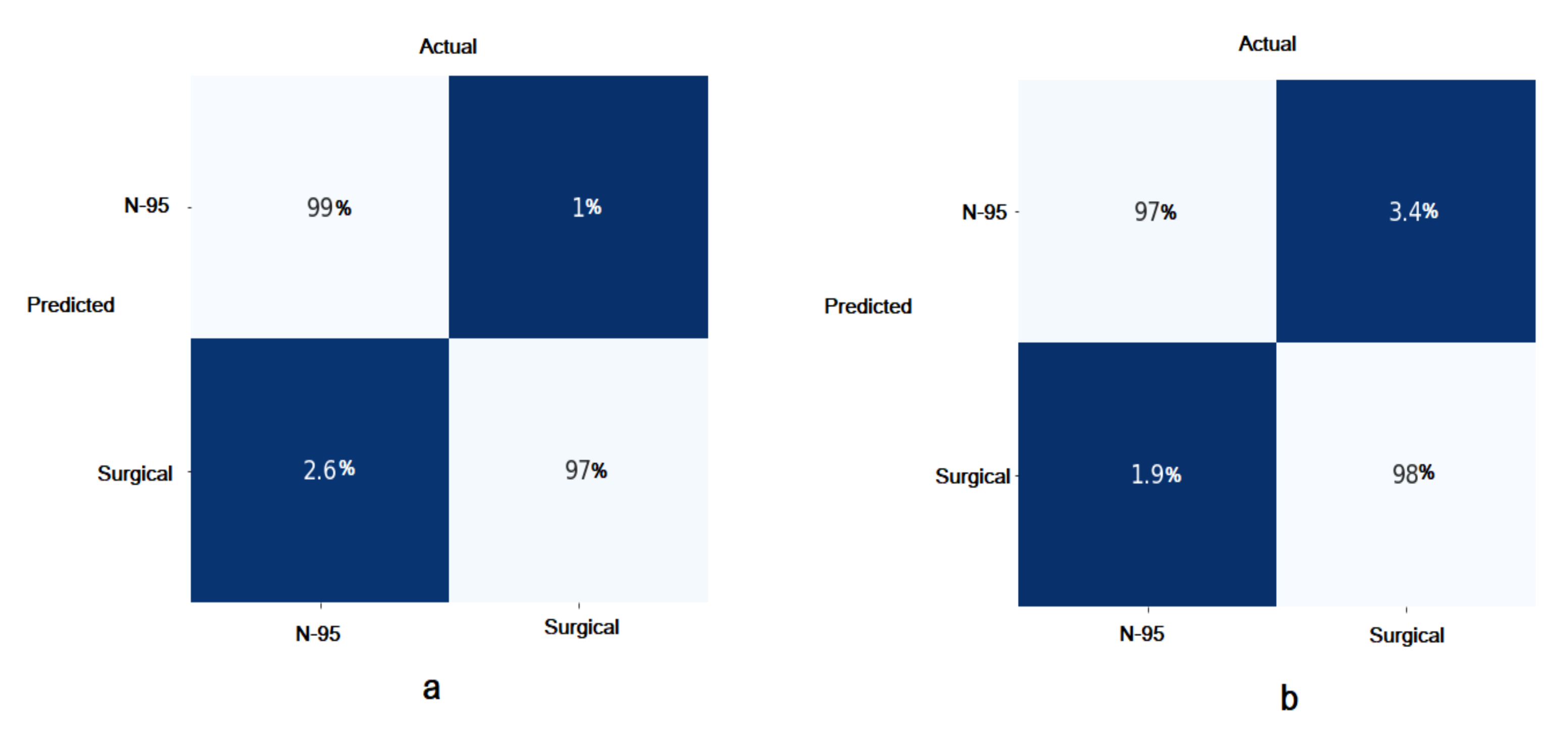
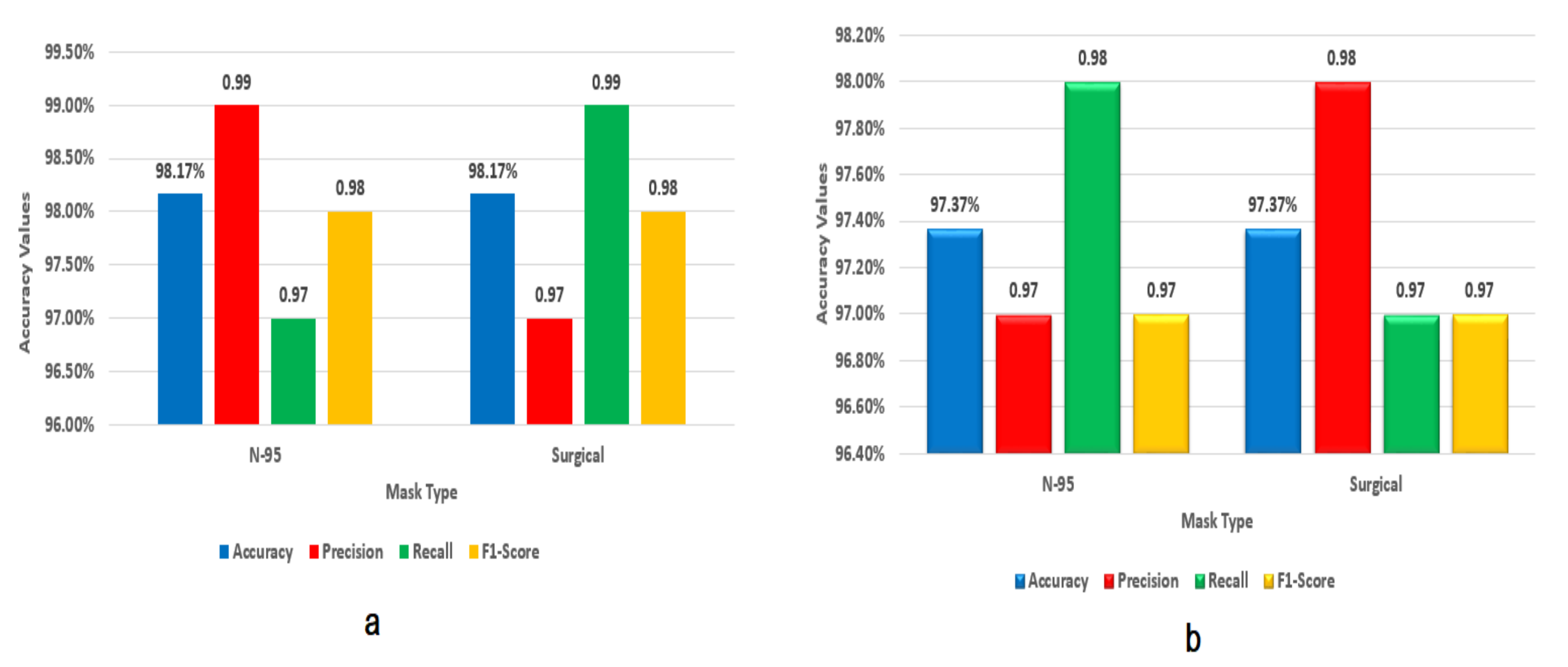
Identification and Classification for the Types of Face Masks
5. Discussion
6. Conclusions
7. Limitations
8. Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC COVID-19 Response Team. Preliminary estimates of the prevalence of selected underlying health conditions among patients with coronavirus disease 2019—United States, February 12–March 28, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 382–386. [Google Scholar] [CrossRef]
- CDC COVID-19 Response Team. Severe Outcomes among Patients with Coronavirus Disease 2019 (COVID-19)-United States, February 12-March 16, 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 343–346. [Google Scholar] [CrossRef]
- Moriyama, M.; Hugentobler, W.J.; Iwasaki, A. Seasonality of respiratory viral infections. Annu. Rev. Virol. 2020, 7, 83–101. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Reuter, T. Three Ways China Is Using Drones to Fight Coronavirus; World Economic Forum: Geneva, Switzerland, 2020; Volume 16. [Google Scholar]
- Gupta, P.; Agrawal, D.; Chhabra, J.; Dhir, P.K. IoT based smart healthcare kit. In Proceedings of the IEEE 2016 International Conference on Computational Techniques in Information and Communication Technologies (ICCTICT), New Delhi, India, 11–13 March 2016; pp. 237–242. [Google Scholar]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Tribune. Govt to End Lockdown from 9th in Phases. The Express Tribune, 7 May 2020. [Google Scholar]
- Greenhalgh, T.; Schmid, M.B.; Czypionka, T.; Bassler, D.; Gruer, L. Face masks for the public during the covid-19 crisis. BMJ 2020, 369, m1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aruna, A.; Mol, Y.B.; Delcy, G.; Muthukumaran, N. Arduino Powered Obstacles Avoidance for Visually Impaired Person. Asian J. Appl. Sci. Technol. 2018, 2, 101–106. [Google Scholar]
- Jayapradha, S.; Vincent, P.D.R. An IOT based Human healthcare system using Arduino Uno board. In Proceedings of the IEEE 2017 International Conference on Intelligent Computing, Instrumentation and Control Technologies (ICICICT), Kerala, India, 6–7 July 2017; pp. 880–885. [Google Scholar]
- Pawar, P.A. Heart rate monitoring system using IR base sensor & Arduino Uno. In Proceedings of the IEEE 2014 Conference on IT in Business, Industry and Government (CSIBIG), Indore, India, 8–9 March 2014; pp. 1–3. [Google Scholar]
- Sugathan, A.; Roy, G.G.; Kirthyvijay, G.; Thomson, J. Application of Arduino based platform for wearable health monitoring system. In Proceedings of the 2013 IEEE 1st International Conference on Condition Assessment Techniques in Electrical Systems (CATCON), Kolkata, India, 6–8 December 2013; pp. 1–5. [Google Scholar]
- Yu, Y.; Waltereit, M.; Matkovic, V.; Hou, W.; Weis, T. Deep Learning-based Vibration Signal Personnel Positioning System. IEEE Access 2020, 8, 226108–226118. [Google Scholar] [CrossRef]
- Elhoseny, M.; Ramírez-González, G.; Abu-Elnasr, O.M.; Shawkat, S.A.; Arunkumar, N.; Farouk, A. Secure medical data transmission model for IoT-based healthcare systems. IEEE Access 2018, 6, 20596–20608. [Google Scholar] [CrossRef]
- Rohokale, V.M.; Prasad, N.R.; Prasad, R. A cooperative Internet of Things (IoT) for rural healthcare monitoring and control. In Proceedings of the IEEE 2011 2nd International Conference on Wireless Communication, Vehicular Technology, Information Theory and Aerospace & Electronic Systems Technology (Wireless VITAE), Chennai, India, 28 February–3 March 2011; pp. 1–6. [Google Scholar]
- Q&A on Coronaviruses (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-coronaviruses (accessed on 7 September 2020).
- World Health Organization. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations: Scientific Brief, 27 March 2020; Technical Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Rao, A.S.S.; Vazquez, J.A. Identification of COVID-19 can be quicker through artificial intelligence framework using a mobile phone–based survey when cities and towns are under quarantine. Infect. Control Hosp. Epidemiol. 2020, 41, 826–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandey, R.; Gautam, V.; Bhagat, K.; Sethi, T. A machine learning application for raising wash awareness in the times of COVID-19 pandemic. arXiv 2020, arXiv:2003.07074. [Google Scholar]
- Narin, A.; Kaya, C.; Pamuk, Z. Automatic detection of coronavirus disease (COVID-19) using X-ray images and deep convolutional neural networks. arXiv 2020, arXiv:2003.10849. [Google Scholar]
- Decencière, E.; Cazuguel, G.; Zhang, X.; Thibault, G.; Klein, J.C.; Meyer, F.; Marcotegui, B.; Quellec, G.; Lamard, M.; Danno, R.; et al. TeleOphta: Machine learning and image processing methods for teleophthalmology. Irbm 2013, 34, 196–203. [Google Scholar] [CrossRef]
- Lu, J.; Gu, J.; Li, K.; Xu, C.; Su, W.; Lai, Z.; Zhou, D.; Yu, C.; Xu, B.; Yang, Z. COVID-19 outbreak associated with air conditioning in restaurant, Guangzhou, China, 2020. Emerg. Infect. Dis. 2020, 26, 1628. [Google Scholar] [CrossRef] [PubMed]
- Sajadi, M.M.; Habibzadeh, P.; Vintzileos, A.; Shokouhi, S.; Miralles-Wilhelm, F.; Amoroso, A. Temperature and Latitude Analysis to Predict Potential Spread and Seasonality for COVID-19. Available at SSRN 3550308. 2020. Available online: https://www.ecplanet.org/sites/ecplanet.com/files/SSRN-id3553027.pdf (accessed on 12 April 2021).
- Guo, Z.D.; Wang, Z.Y.; Zhang, S.F.; Li, X.; Li, L.; Li, C.; Cui, Y.; Fu, R.B.; Dong, Y.Z.; Chi, X.Y.; et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg. Infect. Dis. 2020, 26, 1583–1591. [Google Scholar] [CrossRef]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Loey, M.; Manogaran, G.; Taha, M.H.N.; Khalifa, N.E.M. A hybrid deep transfer learning model with machine learning methods for face mask detection in the era of the COVID-19 pandemic. Measurement 2021, 167, 108288. [Google Scholar] [CrossRef]
- Chowdary, G.J.; Punn, N.S.; Sonbhadra, S.K.; Agarwal, S. Face mask detection using transfer learning of inceptionv3. In International Conference on Big Data Analytics; Springer: Berlin/Heidelberg, Germany, 2020; pp. 81–90. [Google Scholar]
- Nagrath, P.; Jain, R.; Madan, A.; Arora, R.; Kataria, P.; Hemanth, J. SSDMNV2: A real time DNN-based face mask detection system using single shot multibox detector and MobileNetV2. Sustain. Cities Soc. 2021, 66, 102692. [Google Scholar] [CrossRef]
- Venkateswarlu, I.B.; Kakarla, J.; Prakash, S. Face mask detection using MobileNet and Global Pooling Block. In Proceedings of the 2020 IEEE 4th Conference on Information & Communication Technology (CICT), Chennai, India, 3–5 December 2020; pp. 1–5. [Google Scholar]
- Loey, M.; Manogaran, G.; Taha, M.H.N.; Khalifa, N.E.M. Fighting against COVID-19: A novel deep learning model based on YOLO-v2 with ResNet-50 for medical face mask detection. Sustain. Cities Soc. 2020, 65, 102600. [Google Scholar] [CrossRef]
- Hussain, S.A.; Al Balushi, A.S.A. A real time face emotion classification and recognition using deep learning model. J. Phys. Conf. Ser. 2020, 1432, 012087. [Google Scholar] [CrossRef]
- Viola, P.; Jones, M. Rapid object detection using a boosted cascade of simple features. In Proceedings of the 2001 IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR 2001), Kauai, HI, USA, 8–14 December 2001; Volume 1. [Google Scholar]
- Digital Non-Contact Infrared Thermometer (MLX90614) #Melexis. Available online: https://www.melexis.com/en/product/MLX90614/Digital-Plug-Play-Infrared-Thermometer-TO-Can (accessed on 23 January 2021).
- Wang, C.; Xi, Y. Convolutional Neural Network for Image Classification; The Johns Hopkins University Press: Baltimore, MD, USA, 1997. [Google Scholar]
- Lafiosca, P.; Fan, I.S. Review of non-contact methods for automated aircraft inspections. Insight-Non Test. Cond. Monit. 2020, 62, 692–701. [Google Scholar]
- GitHub—Cabani/MaskedFace-Net: MaskedFace-Net Is a Dataset of Human Faces with a Correctly and Incorrectly Worn Mask Based on the Dataset Flickr-Faces-HQ (FFHQ). Available online: https://github.com/cabani/MaskedFace-Net (accessed on 25 February 2021).
- GitHub—Borutb-Fri/FMLD: A Challenging, in the Wild Dataset for Experimentation with Face Masks with 63,072 Face Images. Available online: https://github.com/borutb-fri/FMLD (accessed on 4 April 2021).
- Ge, S.; Li, J.; Ye, Q.; Luo, Z. Detecting Masked Faces in the Wild with LLE-CNNs. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 426–434. [Google Scholar] [CrossRef]
- Bing-Images · PyPI. Available online: https://pypi.org/project/bing-images/ (accessed on 4 April 2021).
- Extracting Covid-19 Insights from Bing Search Data|Bing Search Blog. Available online: https://blogs.bing.com/search/2020_07/Extracting-Covid-19-insights-from-Bing-search-data (accessed on 23 February 2021).
- Kaur, T.; Gandhi, T.K. Automated brain image classification based on VGG-16 and transfer learning. In Proceedings of the IEEE 2019 International Conference on Information Technology (ICIT), Bhubaneswar, India, 19–21 December 2019; pp. 94–98. [Google Scholar]
- Reddy, A.S.B.; Juliet, D.S. Transfer learning with ResNet-50 for malaria cell-image classification. In Proceedings of the IEEE 2019 International Conference on Communication and Signal Processing (ICCSP), Chennai, India, 4–6 April 2019; pp. 0945–0949. [Google Scholar]
- Hussain, M.; Bird, J.J.; Faria, D.R. A study on cnn transfer learning for image classification. In UK Workshop on Computational Intelligence; Springer: Berlin/Heidelberg, Germany, 2018; pp. 191–202. [Google Scholar]
- Hashmi, M.F.; Katiyar, S.; Keskar, A.G.; Bokde, N.D.; Geem, Z.W. Efficient pneumonia detection in chest xray images using deep transfer learning. Diagnostics 2020, 10, 417. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.F.; Hung, K. Design of a non-contact body temperature measurement system for smart campus. In Proceedings of the 2016 IEEE International Conference on Consumer Electronics-China (ICCE-China), Guangzhou, China, 19–21 December 2016; pp. 1–4. [Google Scholar]
- Kaplan, R.B.; Johnson, T.M.; Schneider, R.; Krishnan, S.M. A design for low cost and scalable non-contact fever screening system. In Proceedings of the ASEE Annual Conference and Exposition, Vancouver, BC, Canada, 26–29 June 2011. [Google Scholar]
- Agrawal, A.; Singh, S.G. PREFACE on the Special Issue ‘Technologies for Fighting COVID-19’. Trans. Indian Natl. Acad. Eng. 2020, 5, 91–95. [Google Scholar] [CrossRef]
- Hussain, S.; Cheema, M.J.M.; Motahhir, S.; Iqbal, M.M.; Arshad, A.; Waqas, M.S.; Usman Khalid, M.; Malik, S. Proposed Design of Walk-Through Gate (WTG): Mitigating the Effect of COVID-19. Appl. Syst. Innov. 2020, 3, 41. [Google Scholar] [CrossRef]
- Qin, B.; Li, D. Identifying Facemask-Wearing Condition Using Image Super-Resolution with Classification Network to Prevent COVID-19. Sensors 2020, 20, 5236. [Google Scholar] [CrossRef] [PubMed]
- Militante, S.V.; Dionisio, N.V. Real-Time Facemask Recognition with Alarm System using Deep Learning. In Proceedings of the 2020 11th IEEE Control and System Graduate Research Colloquium (ICSGRC), Shah Alam, Malaysia, 8 August 2020; pp. 106–110. [Google Scholar]

























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types of Object Surfaces | Objects | Positivity Rate of COVID-19 |
|---|---|---|
| ICU and GW items | Computer Mouse | (ICU 6/8, 75%; GW 1/5, 20%) |
| Trash Cans | (ICU 3/5, 60%; GW 0/8) | |
| Sickbed Handrails | (ICU 6/14, 42.9%; GW0/12) | |
| Doorknobs | (GW 1/12, 8.3%) | |
| Shoes | (50% positive) | |
| Miscellaneous Personal item | Exercise Equipment | (81.3% were positive by PCR) |
| Medical Equipment | ||
| PC and iPods | ||
| Reading Glasses | ||
| Other objects | Cellular Phones | (83.3% positive for viral RNA) |
| Remote controls for in-room TVs | (64.7% positive) | |
| Toilets | (81.0% positive) | |
| Room surfaces | (80.4% of all sampled) | |
| Bedside Tables, Bed, rails | (75.0% positive) | |
| Window ledges | (81.8% positive) |
| Dataset | Total Images | Training Images | Testing Images |
|---|---|---|---|
| Github (MAFA) [37] | 12,000 | 9600 | 2400 |
| Bing Dataset [40] | 4039 | 3232 | 807 |
| Github Dataset (Masked Face-Net) [36] | 67,562 | 54,049 | 13,512 |
| Models | Accuracy | Kapa Values |
|---|---|---|
| VGG-16 | 99.8% | 0.996% |
| MobileNetV2 | 99.6% | 0.993% |
| Inception V3 | 99.4% | 0.99% |
| ResNet-50 | 99.2% | 0.986% |
| CNN | 99.0% | 0.983% |
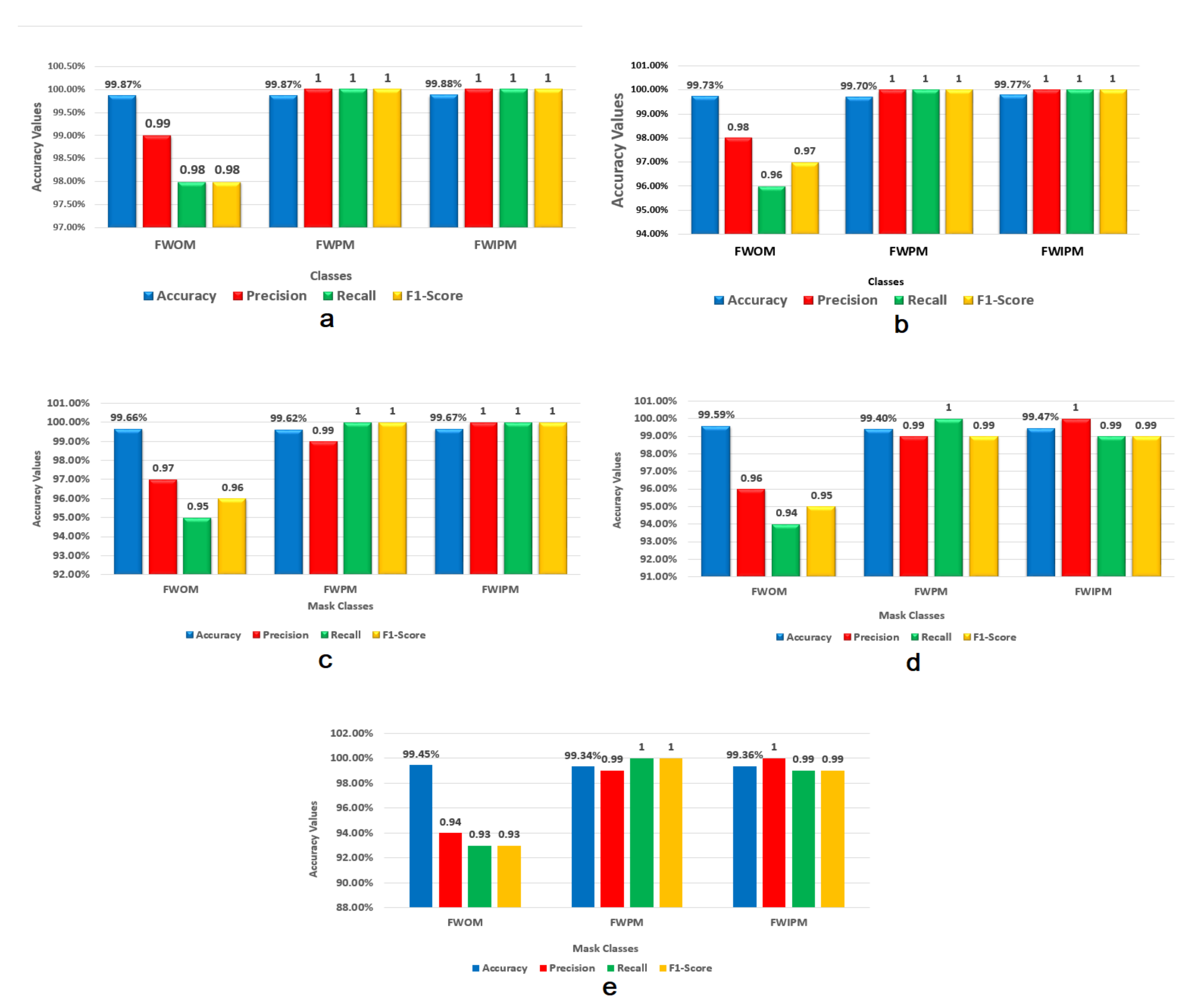
| Classes | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|
| Face Without Mask (FWOM) | 99.87% | 0.99 | 0.98 | 0.98 |
| Face with proper mask (FWPM) | 99.87% | 1.0 | 1.0 | 1.0 |
| Face with improper mask (FWIPM) | 99.88% | 1.0 | 1.0 | 1.0 |
| Classes | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|
| Face Without Mask (FWOM) | 99.73% | 0.98 | 0.96 | 0.97 |
| Face with proper mask (FWPM) | 99.7% | 1.0 | 1.0 | 1.0 |
| Face with improper mask (FWIPM) | 99.77% | 1.0 | 1.0 | 1.0 |
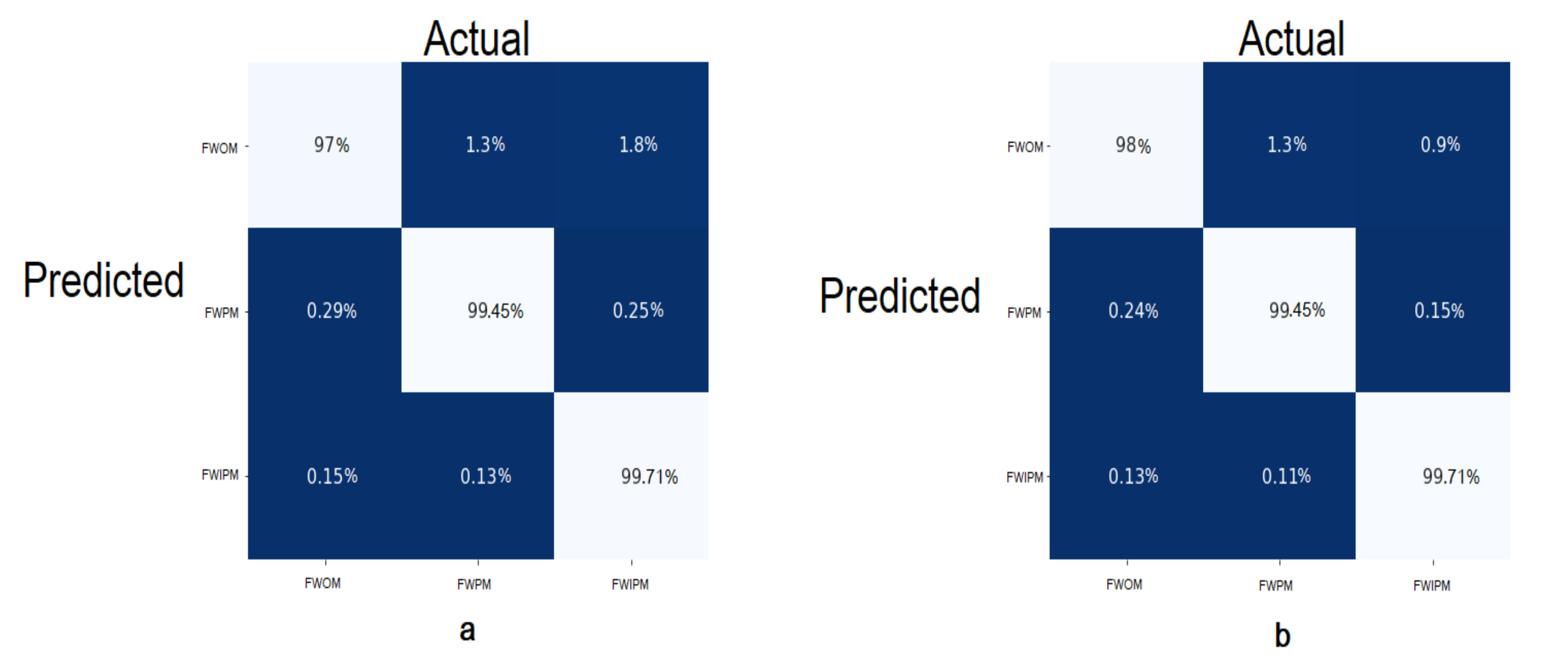
| Classes | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|
| Face Without Mask (FWOM) | 99.66% | 0.97 | 0.95 | 0.96 |
| Face with proper mask (FWPM) | 99.62% | 0.99 | 1.0 | 1.0 |
| Face with improper mask (FWIPM) | 99.67% | 1.0 | 1.0 | 1.0 |
| Classes | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|
| Face Without Mask (FWOM) | 99.59% | 0.96 | 0.94 | 0.95 |
| Face with proper mask (FWPM) | 99.4% | 0.99 | 1.0 | 0.99 |
| Face with improper mask (FWIPM) | 99.47% | 1.0 | 0.99 | 0.99 |
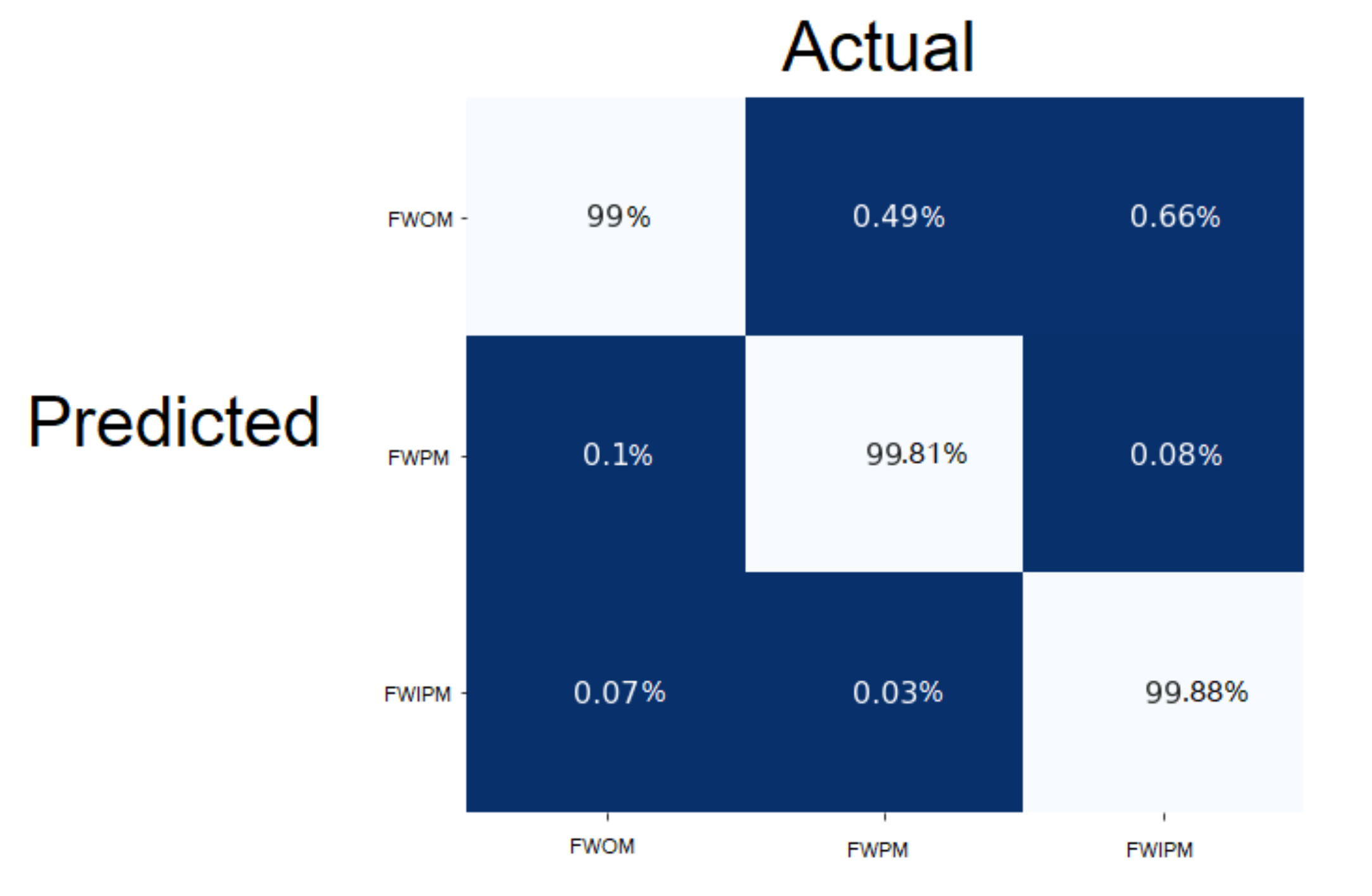
| Classes | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|
| Face Without Mask (FWOM) | 99.45% | 0.94 | 0.93 | 0.93 |
| Face with proper mask (FWPM) | 99.34% | 0.99 | 1.0 | 0.99 |
| Face with improper mask (FWIPM) | 99.36% | 1.0 | 0.99 | 0.99 |
| Models | Accuracy | Kapa Value |
|---|---|---|
| VGG-16 | 98.17% | 0.963 |
| MobileNetV2 | 97.37% | 0.94 |
| Mask Type | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|
| N-95 | 98.17% | 0.99 | 0.97 | 0.98 |
| Surgical | 98.17% | 0.97 | 0.99 | 0.98 |
| Mask Type | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|
| N-95 | 97.37% | 0.97 | 0.98 | 0.97 |
| Surgical | 97.37% | 0.98 | 0.97 | 0.97 |
| References | Disinfect | Temperature Measure | Picture Capture | Mask Detection | Mask Type Identification |
|---|---|---|---|---|---|
| Agrawal et al. [47] | Yes | No | No | No | No |
| Hussain et al. [48] | Yes | Yes | No | No | No |
| Tang et al. [45] | No | Yes | No | No | No |
| Kaplan et al. [46] | No | Yes | No | Yes | No |
| Qin et al. [49] | No | No | No | Yes | Yes |
| Proposed Approach | Yes | Yes | Yes | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussain, S.; Yu, Y.; Ayoub, M.; Khan, A.; Rehman, R.; Wahid, J.A.; Hou, W. IoT and Deep Learning Based Approach for Rapid Screening and Face Mask Detection for Infection Spread Control of COVID-19. Appl. Sci. 2021, 11, 3495. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083495
Hussain S, Yu Y, Ayoub M, Khan A, Rehman R, Wahid JA, Hou W. IoT and Deep Learning Based Approach for Rapid Screening and Face Mask Detection for Infection Spread Control of COVID-19. Applied Sciences. 2021; 11(8):3495. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083495
Chicago/Turabian StyleHussain, Shabir, Yang Yu, Muhammad Ayoub, Akmal Khan, Rukhshanda Rehman, Junaid Abdul Wahid, and Weiyan Hou. 2021. "IoT and Deep Learning Based Approach for Rapid Screening and Face Mask Detection for Infection Spread Control of COVID-19" Applied Sciences 11, no. 8: 3495. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083495