
Photodynamic Therapy—An Up-to-Date Review



1
Faculty of Engineering in Foreign Languages, University Politehnica of Bucharest, 011061 Bucharest, Romania
2
Faculty of Applied Chemistry and Materials Science, University Politehnica of Bucharest, 011061 Bucharest, Romania
3
Research Institute of the University of Bucharest—ICUB, University of Bucharest, 050657 Bucharest, Romania
*
Author to whom correspondence should be addressed.
Appl. Sci. 2021, 11(8), 3626; https://0-doi-org.brum.beds.ac.uk/10.3390/app11083626
Submission received: 20 March 2021
/
Revised: 8 April 2021
/
Accepted: 14 April 2021
/
Published: 17 April 2021
(This article belongs to the Special Issue Innovative and Emerging Light-Based Technologies for Biomedicine, Food Safety and Agriculture)
Abstract
:The healing power of light has attracted interest for thousands of years. Scientific discoveries and technological advancements in the field have eventually led to the emergence of photodynamic therapy, which soon became a promising approach in treating a broad range of diseases. Based on the interaction between light, molecular oxygen, and various photosensitizers, photodynamic therapy represents a non-invasive, non-toxic, repeatable procedure for tumor treatment, wound healing, and pathogens inactivation. However, classic photosensitizing compounds impose limitations on their clinical applications. Aiming to overcome these drawbacks, nanotechnology came as a solution for improving targeting efficiency, release control, and solubility of traditional photosensitizers. This paper proposes a comprehensive path, starting with the photodynamic therapy mechanism, evolution over the years, integration of nanotechnology, and ending with a detailed review of the most important applications of this therapeutic approach.
1. Introduction
Light has been noticed to have healing potential since antiquity [1], phototherapy being traced back to ~3000 B.C. [2]. Back then, exposure to sunlight was employed to treat various ailments, ranging from mood and mental health issues to locomotor disorders and skin diseases [3,4]. The discoveries of the infrared spectrum, ultraviolet radiation, and electromagnetic induction, coupled with the invention of artificial light sources, significantly contributed to the emergence of modern phototherapy [1,3].
Photodynamic therapy (PDT) was discovered more than a century ago by Oscar Raab, a medical student working with Prof. Hermann von Tappeiner. He observed that paramecia incubated with a fluorescent dye and exposed to light died, whereas those kept in the dark were unaffected [5]. Von Tappeiner was the first to coin the term “photodynamic reaction” [6].
Despite being known since early 1900, PDT’s clinical application is relatively recent, as it started to be widely used only after the 1970 s [6]. Therefore, PDT is a modern, non-invasive, and rapidly developing method for diagnosing and treating various diseases. Due to its spatiotemporal selectivity, PDT is a promising therapeutic approach for a wide range of cancers and non-oncological diseases, while the antibacterial effect renders it suitable for non-clinical applications as well [2,7,8].
Based on the beneficial interaction between light, photosensitive compounds (called photosensitizers), and oxygen, PDT has gained popularity among various types of therapies. The better cosmetic outcomes, minimal functional disturbances, good patient tolerance, fertility preservation, and minimization of systemic toxicity are the main PDT advantages that render this method more promising than classic treatment strategies like chemotherapy, radiotherapy, and surgery [2,9,10,11,12].
However, some drawbacks remain, being mainly imposed by traditional organic photosensitizers. To overcome the issues of limited solubility, optical absorption, and tumor targeting ability, PDT can be enhanced through nanotechnology [2,13,14,15]. In this respect, nanoplatforms have been designed to modify existing photosensitizers towards increased treatment efficiency [16].
This paper aims to explain the biophysical mechanisms of PDT, the generation-by-generation improvement of photosensitizers, and nanomaterials’ role in obtaining unprecedented PDT treatment performances. Moreover, an extensive review of current and emerging PDT applications was elaborated.
2. Photodynamic Therapy Working Principle
PDT is a special kind of light therapy based on the combined action of three main elements: A photosensitizer (PS), a light source, and molecular oxygen (Figure 1) [12,17,18,19]. The main types of light sources employed in PDT are lasers, light-emitting diodes, and lamps, the choice depending on the target location, absorption spectrum of the used photosensitizer, and required light dose [20]. Under appropriate light irradiation, the non-toxic photosensitizing compound placed at the target site is activated, being able to absorb and transfer electrons, while the in situ found oxygen molecules act as electron acceptors [19,21,22]. Hence, cytotoxic reactive oxygen species (ROS) are generated, producing irreversible damage to microorganisms and target tissues by rupturing the cell membrane and causing cell death by necrosis or apoptosis [17,19,23,24,25].
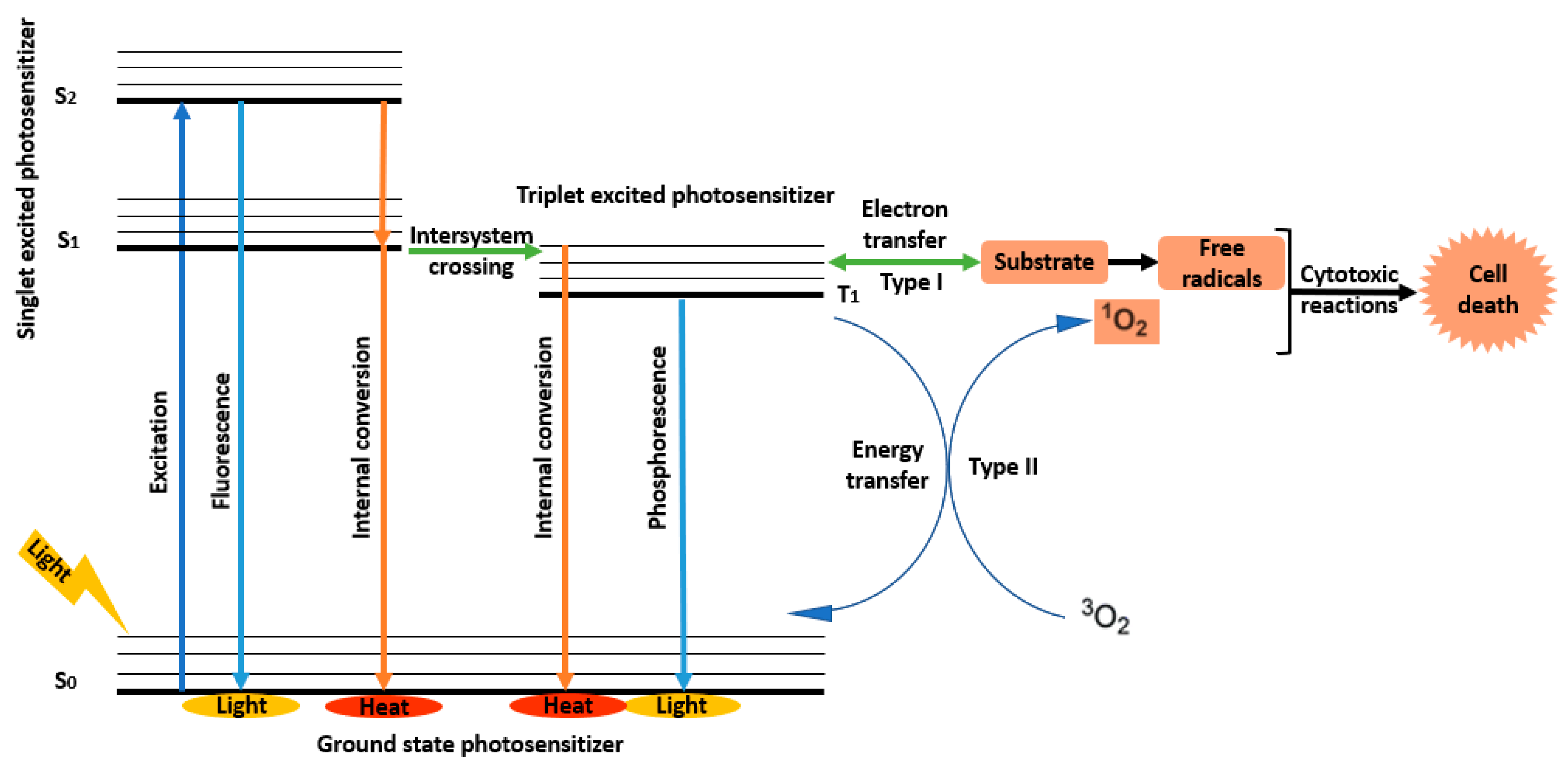
There are two main types of ROS, each corresponding to a distinctive PDT mechanism (Figure 2). By electron transfer are produced oxygen radicals (e.g., superoxide anion O2•−, hydroxyl radical HO•, hydroperoxyl radical HOO•), while by energy transfer is obtained singlet oxygen (1O2) [21]. Type I mechanism supposes the transition of PS molecules from the ground state to the singlet excited state and to the triplet excited state [8]. Then, through electron transfer, these excited PS molecules interact with the substrate to form free radicals [29,30,31]. In contrast, in the photodynamic reaction of type II, excited PS molecules transfer energy to molecular oxygen to produce highly active singlet oxygen that further interacts with lipids, proteins, and nucleic acids, causing cell death by necrosis or apoptosis [8,22,29].
3. Photosensitizers
One of the essential components of PDT, apart from light and oxygen, is the presence of photosensitizers. These substances’ intrinsic properties determine their therapeutic efficiency as PSs can absorb light of a specific wavelength and trigger photochemical or photophysical reactions [7,32,36]. An ideal PS should be chemically pure and uniform in composition, be an effective ROS generator, selectively accumulate in the target tissue, be innocuous in the absence of radiation, absorb light in the long-wave part of the spectrum (600–850 nm, a range called “phototherapeutic window”), be stable in solution, serum or plasma, be easily eliminated from the organism, and have an economical production route [8,29,37,38,39].
Photosensitizers were first introduced to the treatment on a commercial scale in the 1970s when Dr. Thomas Dougherty and his colleagues tested the “hematoporphyrin derivative” (HpD), a water-soluble mixture of hematoporphyrin, protoporphyrin, deuteroporphyrin, their derivatives, monomers, dimers and oligomers and their esters [7,8,26]. Nowadays, more than 1000 natural and synthetic PSs are known [8] (Table 1), their development facing generations of iterative evolution towards ideal photonic and biological properties [25].
The first generation of PSs relies on various forms of HpDs that have been used upon thousands of patients in clinical trials for over 30 years [26]. The first clinically approved PS is commercially known as Photofrin® (Axcan Pharma, Mont-Saint-Hilaire, QC, Canada) and has been involved in treating several types of cancer, such as non-small lung, bladder, esophageal, and brain cancer [31,40]. However, despite their wide application, first-generation PSs have a series of disadvantages. These PSs have a low chemical purity and can be efficiently activated only using wavelengths below 640 nm, limiting tissue penetration. Moreover, the long half-life of PSs renders the skin hypersensitive to light for several weeks, requiring patients treated with them to stay in a dark room for up to 6 weeks. To overcome these limitations, developing a new generation of PSs became imperative [7,26].
Therefore, in the late 1980s, the next generation of photosensitizers started being studied [7,26]. Second-generation PSs consist of pure synthetic compounds with an aromatic macrocycle (e.g., porphyrins, benzoporphyrins, chlorins, bacteriochlorins, and phthalocyanines) [28]. PSs that are either clinically approved or were/are currently undertaking clinical trials include temoporfin (Foscan®, Biolitec, Gina, Germany), motexafin lutetium (Lutex ®, Pharmacyclics, Sunnyvale, CA, USA), palladium bacteriopheophorbide (Tookad® soluble, Negma-Lerads, Elancourt, France), tin ethyl etiopurpurin (Purlytin®, Miravant, Santa Barbara, CA, USA), verteporfin (Visudyne®, Novartis, Basel, Switzerland), talaporfin (Laserphyrin®, Meiji Seika, Tokyo, Japan) [31]. In contrast with first-generation PSs, these porphyrinoid compounds allow a better tumor specificity and penetration to deeply located tissues, as their absorption spectrum is in the range of 650–800 nm. Moreover, they have a faster elimination from the body, resulting in fewer side effects and reduced time (under 2 weeks) spent by the patient in a dark room. However, their major drawback comes from their poor water solubility. This property causes second-generation PSs to aggregate under physiological conditions, reducing the yield of ROS production. The hydrophobic nature is also a limiting factor for intravenous administration, forcing the search for new drug delivery methods [7,26]. Hence, developing another generation of photosensitizers was needed to facilitate delivery and cell uptake and improve the therapeutic outcomes [41].
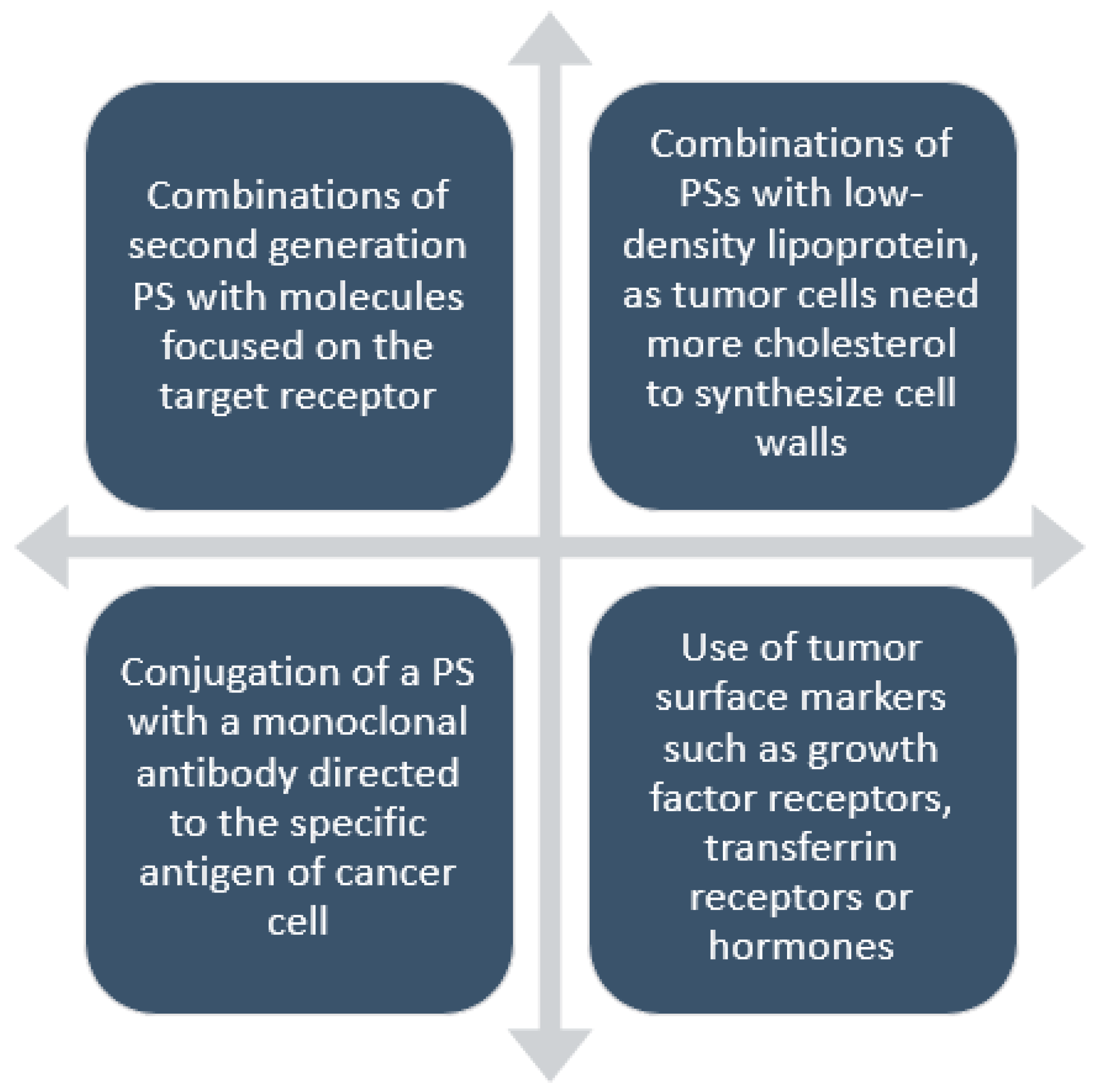
The development of the third-generation PSs primarily focuses on synthesizing structures with higher affinity for the target cells [7] (Figure 3). These PSs are usually composed of a second-generation PS or a photoactivatable drug conjugated to or encapsulated in biodegradable/biocompatible nanoparticles (NPs). Therefore, the stability and hydrophilicity of PSs are increased, pharmacokinetics, pharmacodynamics and biodistribution in vivo are improved, unwanted side-effects are reduced, and dark toxicity is limited [42,43]. Even though important advances have been made in the past decade, third-generation PSs are still under development [41]. Difficulties in parental administration of PSs limit widespread clinical application of PDT, new drug delivery systems being an urgent requirement for increasing the bioavailability of the photodynamic method [7].
4. Nanomaterials for Photodynamic Therapy
By exploring new strategies to improve PDT, integrating PSs with nanotechnology came as a highly promising solution to increase therapy effectiveness [15]. Nanomaterials have recently become an important component of PDT for achieving enhanced results in terms of specific targeting, high drug loading, multifunctional integration, improved solubility of hydrophobic PSs, maintenance of a constant PS delivery rate, and reduced toxic effects over healthy cells [15,36].
One of the attractive features of nanoparticles is their large surface-to-volume ratio. This property promotes loading capacity, improving concentration delivery and uptake in the target cells. The small size of nanoparticles also helps them mimic biological molecules, allowing these nanocarriers to easily pass through the immune system barriers [29]. Moreover, their surface can be functionalized with specific ligands that can be recognized only by certain receptors, this unique match being the drug-release trigger [7,26].
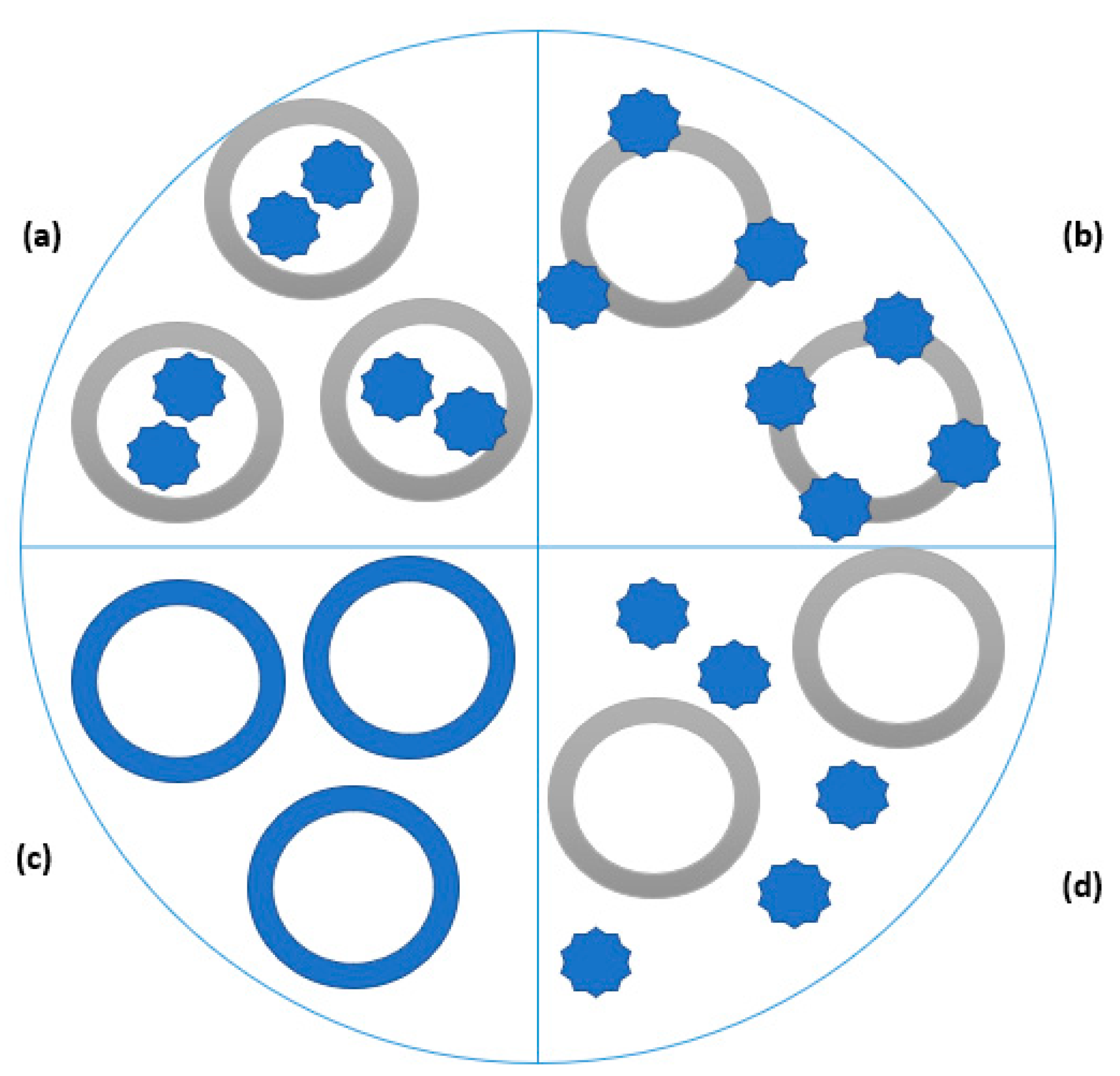
In this respect, PSs may be encapsulated in or immobilized to nanoplatforms to be selectively delivered into the tumor [7,16] (Figure 4). A variety of nanostructures can be employed for this purpose, including diverse metallic, organic, inorganic, and polymeric materials in the form of dendrimers, micelles, liposomes, quantum dots, nanoparticles, antibody–drug conjugates, and more [15,16,43].
A promising approach is represented by metal-based nanoparticles that can carry and deliver hydrophobic PSs to tumoral tissues through the enhanced permeability and retention (EPR) effect [8,29,65,66]. Compared to conventional photosensitizers, metal-based nanoparticles have a long cycle time, slow degradation, targeted and controllable release, being advantageous for PDT [8].
Due to its low toxicity, inertness, and good biocompatibility, gold is one of the preferred materials among metallic nanoparticles. Moreover, its affinity towards thiol and amine groups allows facile surface functionalization with ligands like antibodies, proteins, nucleic acids, and carbohydrates [14,29,67,68]. Gold nanocages, nanorods, and nanoshells are considered brilliant photo-response structures, capable of sensitizing singlet oxygen formation and generating ROS that can destroy cancer cells [69]. Gold nanoclusters were reported as effective delivery vehicles for clinically approved PSs, providing spatiotemporal control and diminishing undesirable side effects [70].
Silver is another material of interest in PDT because, besides its ability to generate singlet oxygen, it also has antimicrobial properties [14,64,71,72,73]. Ag nanoparticles’ large specific area increases the contact area between this material and bacteria or viruses, thus enhancing its bactericidal effect. Moreover, when being used as nanocontainers of PSs, these particles perform a bimodal action, increasing the efficiency of fault detection and isolation of microorganisms [8,74].
Copper sulfide nanoparticles are widely used in PDT as they are cheap, simple, easy to prepare, and can be surface functionalized [8]. CuS nanoparticles also present photothermal and photodynamic properties that, coupled with their insignificant cytotoxicity, make them suitable for bacteria eradication from infected wounds [75]. CuS nanodots can also serve as the base material for nanotheranostics with excellent biocompatibility [76].
Titanium dioxide can also act as a photosensitive agent, being able to generate singlet oxygen [8,24,77,78]. These nanoparticles gained interest due to their adjustable bandgap, band position, excellent photostability, low toxicity, high catalytic activity, abundance, and affordability [36]. Used either alone or as composites and combinations with other compounds, TiO2 nanoparticles can be successfully involved in PDT for treating malignant tumors or inactivate antibiotic-resistant bacteria [79].
Manganese oxide-based drug nanoplatforms have also been proven effective in PDT. MnO2 nanosheets can regenerate oxygen through the reaction with H2O2 present in the tumor microenvironment while simultaneously consuming glutathione to enhance antitumor efficacy. Moreover, these materials present strong PS absorption ability and good biocompatibility, which are attractive properties for PSs carriers [14,36,80].
Other metal-based nanomaterials reportedly used in PDT are molybdenum oxide, zinc oxide, and tungsten oxide nanoparticles [8], yttrium oxide nanoparticles [81], ruthenium nanomaterial complexes [82], transition metal dichalcogenide nanosheets [14], transition metal carbides nanosheets, and nanoparticles [14].
Another attractive alternative to classic PDT is using silica nanoparticles for encapsulating PSs. Despite not being active itself, silica has other features recommending it for this light-based therapy, namely nontoxicity, chemical inertness, and optical transparency [14]. In this regard, mesoporous silica nanoparticles have been extensively used as nanocarriers for hydrophobic PSs, particularly zinc phthalocyanine [83,84].
Carbon-based nanomaterials have also gained considerable research interest in the field of PDT. Their physicochemical and biological properties, such as unique optical and mechanical features, good biocompatibility, low toxicity, versatile chemical functionalization, enhanced permeability effect, and ability to produce ROS, make them suitable for cancer PDT and antimicrobial photodynamic inactivation [14,85]. Among the allotropic forms of carbon, the most applied are carbon nanotubes [14,86], fullerenes [5,87], and graphene-based nanomaterials [88,89,90].
Carbon nanotubes, with their unique structures and features, have attracted interest for PDT application. In particular, single-walled carbon nanotubes have been used as potential sensitizers in cancer therapy, as they are also considered efficient delivery vehicles for hydrophobic PSs [91,92].
Fullerenes can also be used as PSs, presenting advantageous properties, such as versatile functionalization, ability to undergo photochemistry, the possibility of self-assembly into supramolecular fullerosomes, and high resistance to photobleaching [5]. Moreover, reference [60] fullerene derivatives can be employed in the targeted delivery of drugs to the nuclear pore complex and tumor vasculature [87].
Graphene-based nanomaterials, such as graphene quantum dots, graphene oxide, and reduced graphene oxide, have also been employed in cancer therapy, either for anticancer drug delivery or in PDT [14]. Particularly, graphene quantum dots’ ability to generate singlet oxygen can be exploited to destroy pathogenic bacteria and cancer cells [88].
The versatility and diversity of polymeric nanoparticles gained attention in PDT [93]. Their ability to protect drugs against initial deterioration, increase drug permeability into targeted tissue, and diminish systemic toxicity increased polymer-based nanosystems’ popularity over free drugs [94]. Biodegradable polymers are the preferred class of such materials, as they release the PS cargo when degraded by the biological environment [95]. Different architectures, ranging from linear and branched to crosslinked polymers, have been designed as delivery systems for the photo-based treatment of cancers [24].
An example of a convenient polymer for PDT use is polyacrylamide (PAA). PAA nanoparticles can be functionalized with amine or carboxyl groups, with a targeting moiety and/or with polyethylene glycol, and filled with actuating molecules, making them suitable for tumor-selective PDT [52]. PAA nanoparticles are highly soluble in water, being excellent delivery vehicles for PSs, such as methylene blue [96,97,98], Photofrin [98], 5,10,15,20-tetrakis(1-methyl 4-pyridinio) porphyrin tetra(p-toluenesulfonate) (TMPyP) [52], and Temoporfin (m-THPC) [52,99].
Poly (D,L-lactide-co-glycolide) (PLGA) has also attracted attention for PSs encapsulation due to its biodegradability and ease of formulation. PLGA nanoparticles loaded with PSs have shown a higher photoactivity than free PDT drugs against cells from mammary tumors and ovarian cancer cells [52].
Due to their highly branched structure and monodispersity, dendrimers have been adopted in PDT for PS-delivery [52,100]. Dendrimers-based delivery vehicles also benefit from enhanced permeability, sustained drug-release, high solubilization potential, high loading capacity, and improved colloidal, biological, and shelf-stability [101]. Particularly, dendrimers were used as carrier platforms for 5-aminolevulinic acid (ALA), an FDA-approved precursor of a PS employed in topical PDT [52].
Natural polymers, such as proteins and polysaccharides, can be turned into PDT-useful nanoparticles [52]. Human serum albumin, bovine serum albumin, xanthan gum, alginate, chitosan, and gelatin are several examples of such materials investigated for PDT [52,100].
Lipid-based nanostructures can also serve well in PDT [102]. Liposomes may be a promising targeted delivery nanosystem, as they can encapsulate unstable PSs and facilitate their permeation to and through the cell membrane [7,23,46]. Liposome-based PS delivery was shown efficient against metastatic melanoma cells, breast cancer cells, skin cancer cells, and tumor-derived angiogenic vascular endothelial cells [100].
Another option is to combine PSs with low-density lipoproteins (LDL), especially due to many LDL receptors present on tumor cells’ surface. Studies have proved that a PS-bonded non-covalently to LDL before administration results in improved PDT efficiency compared to free PS delivery [7].
Organic–inorganic hybrid materials, such as nanoscale metal–organic frameworks (MOFs), have also emerged as favorable delivery platforms in PDT. What recommends them for such application are their versatile functionalities owed to their chemical composition, the well-defined crystalline structures, large surface-to-volume ratio, high porosity, low-density, regular channel, adjustable aperture, and diverse topology and tailoring [8,14]. MOFs can be successfully applied in the treatment of various malignancies [103,104,105].
5. Photodynamic Therapy Applications
Due to its non-invasive nature, PDT gained increasing interest in treating both malignant and non-malignant diseases. Over the last 40 years, PDT has been employed in various medical fields, ranging from oncology to dermatology, urology, ophthalmology, and dentistry, being efficient in healing a wide range of ailments [10,11,19,29,46].
5.1. Malignant Diseases
Aiming to address the invasive nature of previous anticancer therapeutic strategies (e.g., radiotherapy, chemotherapy, surgery), PDT was developed as a promising alternative [8,15,16,106,107,108]. The main advantage of PDT is its selectivity to tumoral tissues, whereas non-malignant cell damage is minimized [29,109]. PDT can induce cancer cells’ death through three inter-combined mechanisms: direct cellular damage by inducing ROS production, indirect damage by shutting down tumor blood vessels, and stimulation of the patient’s immune system by increasing cancer cell-derived antigen presentation to T cells [109,110,111].
PDT was first used in human trials in 1976 for patients with bladder cancer. Afterward, promising responses were obtained from early-stage patients suffering from lung, esophageal and gastric carcinomas. The next studies included PDT in treating other tumors and cancer types, such as brain tumors, intraocular cancer, breast cancer, head and neck tumors, pancreatic cancer, gynecological tumors [12].
PDT can be employed in the treatment of skin cancers, both melanoma and non-melanoma, the latter being categorized into two subgroups, namely basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) [11,46,85,112]. Melanoma originates from the cells responsible for pigment production (melanocytes) and is the most aggressive of all forms, being likely to grow and spread if left untreated. Therefore, it is vital to diagnose this disease early and start treatment right away [113]. PDT is considered an alternative treatment for melanoma. However, some challenges still hinder its therapeutic efficacy, better tumor targeting, and near-infrared absorbing PSs being required [46].
On the other hand, non-melanoma skin cancers are most commonly found in the areas exposed to the sun [113]. BCC starts from the lower layer of the epidermis (made of basal cells) and tends to grow slowly, with only low metastatic potential [112]. In contrast, SCCs are more likely to extend towards deeper layers of the skin and invade other parts of the body, even though this is rather uncommon. Nonetheless, to avoid spreading to surrounding areas and create multicentric, synchronic, and metachronic lesions, these cancers should not be left untreated [112,113,114,115]. In this respect, PDT has been proved to produce the most appropriate cosmetic and functional results [112]. However, patients treated in this manner should be further monitored as there remains a risk of incomplete response and recurrence [114].
Breast cancer is the most common type of carcinoma in females, being the most prominent cause of cancer-related mortality in women worldwide [94,106,116,117]. The first treatment option for breast cancer is the combination between chemotherapeutic agents, radiation therapy, and surgical intervention. Nonetheless, drugs do not yet penetrate tumor tissue at adequate levels, and systemic side effects are observed [94]. Overcoming these drawbacks, PDT is seen as a promising, safe, and minimally invasive procedure. Moreover, if part of a tumor of known and limited extent appears on an MRI scan, PDT treatment is much simpler to repeat than conventional therapies [118].
In terms of diagnosed cases and associated deaths, one of the top three cancers in the US is lung cancer [13]. Chemotherapy is the dominant treatment modality, yet cancer cells develop drug resistance and no longer respond to therapy after a while. Consequently, a new treatment strategy must be applied, either after chemotherapy becomes inefficient or as the main treatment modality [119]. In this respect, PDT has a long history of clinical success, being FDA-approved for the ablation of microinvasive endobronchial non-small cell lung cancer (NSCLC) not suitable for other treatments and of completely or partially obstructive endobronchial NSCLC [11,13,120].
In terms of incidence and mortality rate, the fourth most common malignancy among women globally is cervical cancer [121]. Classical treatment strategies against this disease cause side effects, including pain and bleeding, and can even compromise the patients’ reproductive capacity, effects that no longer appear when using PDT [9,122].
Similarly, prostate cancer is one of the most common cancers in men worldwide. Unfortunately, most prostate cancers are discovered in advanced stages when there is a poor prognosis due to both pathophysiological changes and inadequate response to treatment [69]. To overcome these drawbacks, PDT emerged as an alternative, and various PSs have been tested in the clinic for the focal ablation of prostate tumors [11,37,123,124].
PDT was reported effective in the treatment of gastrointestinal tract malignancies [125], being used for the remedy of esophageal [11,126,127], gastric [59,128,129,130], liver [131,132], pancreatic [133,134,135], and colorectal [136,137,138] cancers. The main advantages of using PDT for these types of cancer are the less-invasive nature compared to surgery and wider indication than endoscopic resection. Moreover, it can be used as a complementary treatment after local failure of chemoradiotherapy [127].
There has also been renewed interest in using PDT to treat various brain tumors [11,108]. Brain cancers may be highly aggressive and infiltrative, the overall prognosis of patients being poor. Tumor resection is a delicate and not curative process, requiring subsequential chemotherapy and fractionated radiotherapy. A solution to these issues would be the simultaneous action of fluorescence-guided surgery and PDT that allows synergic tumor cell visualization and selective destruction [139].
5.2. Non-Malignant Diseases
Despite being best-known for cancer treatment, PDT is not limited to destroying tumoral cells. At the beginning of the last century, the photodynamic effect was demonstrated against bacteria. Considering the present challenges of antibiotic resistance and the rise of new infections, it is no surprise that PDT gained attention for fighting against bacteria, fungi, viruses, and protozoa [17,35].
Antimicrobial photodynamic therapy (found in the literature also as “photodynamic inactivation”) is a safe and cost-effective method to treat various infectious diseases [33]. This is of great importance since the skin and soft tissue lesions can easily become infected by multi-drug resistant pathogens that delay proper healing. Moreover, classic local therapies for infected wounds from burns, trauma, surgery, or diseases are expensive and frequently ineffective [140,141]. As a solution, PDT has been proposed for the treatment of localized bacterial infections. [140]. PDT has shown excellent wound healing results, accelerating tissue repair by killing bacterial cells and simultaneously stimulating fibroblasts’ proliferation [142].
Dental infections represent one of the greatest expanding fields of clinical antibacterial PDT. Studies have reported that pathogens prevalent in the subgingival periodontal plaques (e.g., Porphyromonas gingivalis, Fusobacterium nucleatum, Staphylococcus spp.) have been successfully destroyed through photodynamic treatment, both in aqueous suspension and as a biofilm [33,143].
Another application of PDT is for treating fungal infections. These infections are increasing in prevalence worldwide, especially because only three major classes of antifungal drugs are available for invasive infections, and the efficiency of the treatment depends on the patient’s immune response [19]. A particular case is represented by onychomycosis, one of the most frequent and severe nail fungal infections [144]. PDT is considered promising towards treating this disease through an appropriate formulation, including a PS and keratolytic agents that would increase nail plates’ permeability towards active agents uptake [17].
PDT has been reported to be effective in the inactivation of mammalian viruses, such as human immunodeficiency virus (HIV), human papillomavirus (HPV), hepatitis A, B, and C viruses, herpes viruses, human parvovirus B19, human cytomegalovirus, enteroviruses, and adenoviruses [145,146,147]. PDT started to be intensively researched in the pandemic context as an alternative or complementary treatment strategy to target SARS-CoV-2 [34,148,149,150,151,152]. The photodynamic effect can disrupt the membrane structures of the viral envelope, proteins, and RNA. Hence, PDT is proving to be a powerful tool to inactivate infectious agents [34,152].
Besides pathogen-related diseases, PDT can be employed in the treatment of central serous chorioretinopathy (CSC). This condition is caused by the serous retinal detachment and retinal pigment epithelial detachment at the macula, leading to visual difficulties under low light levels [153]. Several treatments have been proposed to treat CSC (e.g., laser photocoagulation, carbonic anhydrase inhibitors), yet they are not specific enough in dealing with this fundamental choroidal vascular issue [154]. Fortunately, PDT seems effective for treating CSC, as it impacts choroidal vasculature structure, altering its permeability [154,155,156].
5.3. Other Applications
The versatility of PDT is not limited to clinical applications. This technique is valuable for other applications. One example is the removal of biofilms from medical devices. This is highly important, especially because contaminated devices pose a serious threat to human health through the nosocomial infections they can generate. In this respect, PDT can be used to repel biofilm infections from implants, such as prosthetic joint infections and infections caused by ventilator-associated pneumonia biofilms [157].
PDT can also be involved in developing photoactive fabrics by incorporating PSs triggered by sunlight. Masks, suits, and gloves can be designed in this manner to ensure a sterile, safe, decontaminated outfit for healthcare workers [150]. Similarly, antimicrobial surfaces can be obtained to avoid infectious disease outbreaks within healthcare facilities [158].
The selective inactivation of pathogens achievable through PDT is useful for environmental water treatments [33]. Microorganisms like Gram-positive and Gram-negative bacteria, viruses, fungi, and parasites can be eliminated from the surface, ground, drinking, and wastewaters, without developing resistance [159].
Biotechnology is another attractive field for applying the principles of PDT. For instance, inactivating the microbes from fruits’ surfaces prolongs their shelf life, PDT being considered a high-efficiency and nonthermal sterilization technology [160,161]. Another beneficial use is replacing antibiotics treatment of milk by PDT, to reduce bacteria content from dairy products [162].
The food industry can be improved through PDT, not only by killing microbes in food itself but also by creating better packaging. Packaging materials that inhibit bacterial growth were reportedly fabricated using this sterilization technique [163].
6. Advantages and Disadvantages of Photodynamic Therapy
Being so widely used, it is clear that PDT presents a series of advantages when compared to traditional therapy alternatives. One of the most important is spatiotemporal selectivity, which is owed to irradiation control in terms of position and time. This feature allows minimal invasiveness, minimization of systemic toxicity, and minimal functional disturbances [2,10].
PDT is well-tolerated by the patients, can be repeatedly applied at the same site, and either no or only a slight trauma occurs when it is employed to treat target tissues inside the body [2,10]. Unlike other therapies, PDT also preserves fertility and does not affect pregnancy and delivery [9]. Moreover, ROS’s ability to damage a broad range of cells makes PDT suitable for an extensive number of clinical and non-clinical applications [2].
Even though PDT is a promising and beneficial treatment strategy for many diseases, its application is hindered by classic PSs. Their poor water solubility, limited light-penetration depth, and lack of good tumor targeting efficiency are the most commonly associated drawbacks to traditional PDT [8,14]. Other disadvantages include complex scheduling, the necessity of multiple procedures, patient observation after treatment, and photosensitivity issues during few weeks after therapy [13,33]. Therefore, developing a newer generation of PSs is a must in the advancement of PDT and its standardization in clinical practice.
Another possibility of overcoming PDT limitations is represented by combinatorial approaches with other therapeutic modalities (Figure 5) [2]. In this way, the advantages of each treatment can be exploited, while their disadvantages can be offset. For instance, PDT might enhance antitumor immune response, and, in combination with immunotherapy, “abscopal” responses can be obtained from lesions too deep to be efficiently treated by PDT [11].
7. Conclusions
To summarize, photodynamic therapy has been increasingly used in the last decades, covering a wide range of practical applications. Due to its mechanism of generating ROS through the combined interaction of light, oxygen, and photosensitizing compounds, PDT has become attractive for destroying tumoral tissues, bacteria, fungi, and viruses. This therapy’s non-invasive and non-toxic nature rendered it popular for treating various types of cancers and infections.
However, PDT has not yet reached its maximum potential since classic photosensitizers impose limitations on light absorbance, penetration depth, and cellular uptake. In this respect, nanotechnology-integrated PDT started being researched. Various materials with dimensions in the nano range were tested as either as PSs or PSs carriers, showing promising results. Nonetheless, most of the studies are at the in vitro testing stage, while few have moved to clinical trials.
Despite being such a convenient therapeutic approach, PDT has not come to the large-scale application of traditional chemotherapy and radiotherapy methods. The recent intensive research is expected to change this aspect soon, with the advancements in material testing and integrated multimodal platforms.
Author Contributions
A.-G.N. and A.M.G. participated in the review writing and revision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
This manuscript has no acknowledgments.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Foresto, E.; Gilardi, P.; Ibarra, L.E.; Cogno, I.S. Light-activated green-drugs: How we can use them in Photodynamic therapy and mass-produce them with biotechnological tools. Phytomed. Plus 2021, 1, 100044. [Google Scholar] [CrossRef]
- Li, X.; Lee, S.; Yoon, J. Supramolecular photosensitizers rejuvenate photodynamic therapy. Chem. Soc. Rev. 2018, 47, 1174–1188. [Google Scholar] [CrossRef]
- Grzybowski, A.; Sak, J.; Pawlikowski, J. A brief report on the history of phototherapy. Clin. Dermatol. 2016, 34, 532–537. [Google Scholar] [CrossRef] [PubMed]
- Choukroun, J.; Geoffroy, P.A. Light Therapy in Mood Disorders: A Brief History with Physiological Insights. Chronobiol. Med. 2019, 1, 3–8. [Google Scholar] [CrossRef]
- Hamblin, M.R. Fullerenes as photosensitizers in photodynamic therapy: Pros and cons. Photochem. Photobiol. Sci. 2018, 17, 1515–1533. [Google Scholar] [CrossRef] [PubMed]
- Raizada, K.; Naik, M. Photodynamic Therapy; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Kwiatkowski, S.; Knap, B.; Przystupski, D.; Saczko, J.; Kędzierska, E.; Knap-Czop, K.; Kotlińska, J.; Michel, O.; Kotowski, K.; Kulbacka, J. Photodynamic therapy—Mechanisms, photosensitizers and combinations. Biomed. Pharmacother. 2018, 106, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Kormakov, S.; Liu, Y.; Huang, Y.; Wu, D.; Yang, Z. Recent Progress in Metal-Based Nanoparticles Mediated Photodynamic Therapy. Molecules 2018, 23, 1704. [Google Scholar] [CrossRef] [Green Version]
- Chizenga, E.P.; Chandran, R.; Abrahamse, H. Photodynamic therapy of cervical cancer by eradication of cervical cancer cells and cervical cancer stem cells. Oncotarget 2019, 10, 4380–4396. [Google Scholar] [CrossRef] [PubMed]
- Kaczorowska, A.; Malinga-Drozd, M.; Kałas, W.; Kopaczyńska, M.; Wołowiec, S.; Borowska, K. Biotin-Containing Third Generation Glucoheptoamidated Polyamidoamine Dendrimer for 5-Aminolevulinic Acid Delivery System. Int. J. Mol. Sci. 2021, 22, 1982. [Google Scholar] [CrossRef]
- Wang, B.-C.; Fu, C.; Qin, L.; Zeng, X.-Y.; Liu, Q. Photodynamic therapy with methyl-5-aminolevulinate for basal cell carcinoma: A systematic review and meta-analysis. Photodiagn. Photodyn. Ther. 2020, 29, 101667. [Google Scholar] [CrossRef]
- Turksoy, A.; Yildiz, D.; Akkaya, E.U. Photosensitization and controlled photosensitization with BODIPY dyes. Coord. Chem. Rev. 2019, 379, 47–64. [Google Scholar] [CrossRef]
- Chhatre, S.; Vachani, A.; Allison, R.R.; Jayadevappa, R. Survival Outcomes with Photodynamic Therapy, Chemotherapy and Radiation in Patients with Stage III or Stage IV Non-Small Cell Lung Cancer. Cancers 2021, 13, 803. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Fan, T.; Xie, Z.; Zeng, Q.; Xue, P.; Zheng, T.; Chen, Y.; Luo, X.; Zhang, H. Advances in nanomaterials for photodynamic therapy applications: Status and challenges. Biomaterials 2020, 237, 119827. [Google Scholar] [CrossRef] [PubMed]
- Abrahamse, H.; Kruger, C.A.; Kadanyo, S.; Mishra, A. Nanoparticles for Advanced Photodynamic Therapy of Cancer. Photomed. Laser Surg. 2017, 35, 581–588. [Google Scholar] [CrossRef]
- Gao, S.; Islam, R.; Fang, J. Tumor Environment-Responsive Hyaluronan Conjugated Zinc Protoporphyrin for Targeted Anticancer Photodynamic Therapy. J. Pers. Med. 2021, 11, 136. [Google Scholar] [CrossRef] [PubMed]
- Valkov, A.; Zinigrad, M.; Nisnevitch, M. Photodynamic Eradication of Trichophyton rubrum and Candida albicans. Pathogens 2021, 10, 263. [Google Scholar] [CrossRef] [PubMed]
- Ghate, V.S.; Zhou, W.; Yuk, H.-G. Perspectives and Trends in the Application of Photodynamic Inactivation for Microbiological Food Safety. Compr. Rev. Food Sci. Food Saf. 2019, 18, 402–424. [Google Scholar] [CrossRef] [Green Version]
- Bapat, P.; Singh, G.; Nobile, C.J. Visible Lights Combined with Photosensitizing Compounds Are Effective against Candida albicans Biofilms. Microorganisms 2021, 9, 500. [Google Scholar] [CrossRef]
- Kim, M.M.; Darafsheh, A. Light Sources and Dosimetry Techniques for Photodynamic Therapy. Photochem. Photobiol. 2020, 96, 280–294. [Google Scholar] [CrossRef] [Green Version]
- Le Guern, F.; Ouk, T.-S.; Yerzhan, I.; Nurlykyz, Y.; Arnoux, P.; Frochot, C.; Leroy-Lhez, S.; Sol, V. Photophysical and Bactericidal Properties of Pyridinium and Imidazolium Porphyrins for Photodynamic Antimicrobial Chemotherapy. Molecules 2021, 26, 1122. [Google Scholar] [CrossRef]
- Abrahamse, H.; Hamblin, M.R. New photosensitizers for photodynamic therapy. Biochem. J. 2016, 473, 347–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, H.; Feng, M.; Chen, S.; Wang, R.; Luo, Y.; Yin, B.; Li, J.; Wang, X. Near-infrared photothermal liposomal nanoantagonists for amplified cancer photodynamic therapy. J. Mater. Chem. B 2020, 8, 7149–7159. [Google Scholar] [CrossRef]
- Husni, P.; Shin, Y.; Kim, J.C.; Kang, K.; Lee, E.S.; Youn, Y.S.; Rusdiana, T.; Oh, K.T. Photo-Based Nanomedicines Using Polymeric Systems in the Field of Cancer Imaging and Therapy. Biomedicines 2020, 8, 618. [Google Scholar] [CrossRef]
- Luby, B.M.; Walsh, C.D.; Zheng, G. Advanced Photosensitizer Activation Strategies for Smarter Photodynamic Therapy Beacons. Angew. Chem. Int. Ed. 2019, 58, 2558–2569. [Google Scholar] [CrossRef]
- Park, W.; Cho, S.; Han, J.; Shin, H.; Na, K.; Lee, B.; Kim, D.-H. Advanced smart-photosensitizers for more effective cancer treatment. Biomater. Sci. 2018, 6, 79–90. [Google Scholar] [CrossRef]
- Reddy, R.; Ramya, K.; Ramesh, T.; Gudapati, S.; Madhavi, N.; Chennoju, S. Photodynamic therapy in oral diseases. Int. J. Biol. Med. Res. 2012, 3, 1875–1883. [Google Scholar]
- Dhanalekshmi, K.I.; Sangeetha, K.; Magesan, P.; Johnson, J.; Zhang, X.; Jayamoorthy, K. Photodynamic cancer therapy: Role of Ag- and Au-based hybrid nano-photosensitizers. J. Biomol. Struct. Dyn. 2020. [Google Scholar] [CrossRef]
- Montaseri, H.; Kruger, C.A.; Abrahamse, H. Inorganic Nanoparticles Applied for Active Targeted Photodynamic Therapy of Breast Cancer. Pharmaceutics 2021, 13, 296. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas, G.; Nogueira, J.J. Stacking Effects on Anthraquinone/DNA Charge-Transfer Electronically Excited States. Molecules 2020, 25, 5927. [Google Scholar] [CrossRef]
- Karges, J.; Basu, U.; Blacque, O.; Chao, H.; Gasser, G. Polymeric Encapsulation of Novel Homoleptic Bis(dipyrrinato) Zinc(II) Complexes with Long Lifetimes for Applications as Photodynamic Therapy Photosensitisers. Angew. Chem. Int. Ed. 2019, 58, 14334–14340. [Google Scholar] [CrossRef] [PubMed]
- Lan, M.; Zhao, S.; Liu, W.; Lee, C.-S.; Zhang, W.; Wang, P. Photosensitizers for Photodynamic Therapy. Adv. Healthc. Mater. 2019, 8, 1900132. [Google Scholar] [CrossRef]
- Amos-Tautua, B.M.; Songca, S.P.; Oluwafemi, O.S. Application of Porphyrins in Antibacterial Photodynamic Therapy. Molecules 2019, 24, 2456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhapkar, S.; Kumbhar, N.; Gacche, R.; Jagtap, S.; Jadhav, U. Photodynamic Therapy (PDT): An Alternative Approach for Combating COVID-19. Biointerface Res. Appl. Chem. 2021, 11, 12808–12830. [Google Scholar] [CrossRef]
- Wiehe, A.; O’Brien, J.M.; Senge, M.O. Trends and targets in antiviral phototherapy. Photochem. Photobiol. Sci. 2019, 18, 2565–2612. [Google Scholar] [CrossRef] [PubMed]
- Yan, K.; Zhang, Y.; Mu, C.; Xu, Q.; Jing, X.; Wang, D.; Dang, D.; Meng, L.; Ma, J. Versatile Nanoplatforms with enhanced Photodynamic Therapy: Designs and Applications. Theranostics 2020, 10, 7287–7318. [Google Scholar] [CrossRef] [PubMed]
- Kazantzis, K.T.; Koutsonikoli, K.; Mavroidi, B.; Zachariadis, M.; Alexiou, P.; Pelecanou, M.; Politopoulos, K.; Alexandratou, E.; Sagnou, M. Curcumin derivatives as photosensitizers in photodynamic therapy: Photophysical properties and in vitro studies with prostate cancer cells. Photochem. Photobiol. Sci. 2020, 19, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Martins, T.D.; Lima, E.; Boto, R.E.; Ferreira, D.; Fernandes, J.R.; Almeida, P.; Ferreira, L.F.V.; Silva, A.M.; Reis, L.V. Red and Near-Infrared Absorbing Dicyanomethylene Squaraine Cyanine Dyes: Photophysicochemical Properties and Anti-Tumor Photosensitizing Effects. Materials 2020, 13, 2083. [Google Scholar] [CrossRef]
- Hamidi, A.; Shamlouei, H.R.; Maleki, A.; Goodajdar, B.M. Improving the Optical Properties of Porphyrin Ring with Different Substitutions: As Candidate Using in Photosensitizer. Int. J. Nanoelectron. Mater. 2020, 13, 411–420. [Google Scholar]
- McFarland, S.A.; Mandel, A.; Dumoulin-White, R.; Gasser, G. Metal-based photosensitizers for photodynamic therapy: The future of multimodal oncology? Curr. Opin. Chem. Biol. 2020, 56, 23–27. [Google Scholar] [CrossRef]
- Mfouo-Tynga, I.S.; Dias, L.D.; Inada, N.M.; Kurachi, C. Features of third generation photosensitizers used in anticancer photodynamic therapy: Review. Photodiagn. Photodyn. Ther. 2021, 34, 102091. [Google Scholar] [CrossRef]
- Setaro, F.; Wennink, J.W.H.; Mäkinen, P.I.; Holappa, L.; Trohopoulos, P.N.; Ylä-Herttuala, S.; van Nostrum, C.F.; de la Escosura, A.; Torres, T. Amphiphilic phthalocyanines in polymeric micelles: A supramolecular approach toward efficient third-generation photosensitizers. J. Mater. Chem. B 2020, 8, 282–289. [Google Scholar] [CrossRef]
- Gualdesi, M.S.; Vara, J.; Aiassa, V.; Alvarez Igarzabal, C.I.; Ortiz, C.S. New poly(acrylamide) nanoparticles in the development of third generation photosensitizers. Dye. Pigment. 2021, 184, 108856. [Google Scholar] [CrossRef]
- Hosokawa, S.; Takahashi, G.; Sugiyama, K.-I.; Takebayashi, S.; Okamura, J.; Takizawa, Y.; Mineta, H. Porfimer sodium-mediated photodynamic therapy in patients with head and neck squamous cell carcinoma. Photodiagn. Photodyn. Ther. 2020, 29, 101627. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.M.; MacRobert, A.J.; Mosse, C.A.; Periera, B.; Bown, S.G.; Keshtgar, M.R.S. Photodynamic therapy: Inception to application in breast cancer. Breast 2017, 31, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.H.; Lim, S.J.; Lee, M.K. Chitosan-coated liposomes to stabilize and enhance transdermal delivery of indocyanine green for photodynamic therapy of melanoma. Carbohydr. Polym. 2019, 224, 115143. [Google Scholar] [CrossRef]
- Urbanska, K.; Romanowska-Dixon, B.; Matuszak, Z.; Oszajca, J.; Nowak-Sliwinska, P.; Stochel, G. Indocyanine green as a prospective sensitizer for photodynamic therapy of melanomas. Acta Biochim. Pol. 2002, 49, 387–391. [Google Scholar] [CrossRef]
- Bashir, N.Z.; Singh, H.A.; Virdee, S.S. Indocyanine green-mediated antimicrobial photodynamic therapy as an adjunct to periodontal therapy: A systematic review and meta-analysis. Clin. Oral Investig. 2021. [Google Scholar] [CrossRef]
- Rodrigues, G.B.; Brancini, G.T.P.; Uyemura, S.A.; Bachmann, L.; Wainwright, M.; Braga, G.U.L. Chemical features of the photosensitizers new methylene blue N and S137 influence their subcellular localization and photoinactivation efficiency in Candida albicans. J. Photochem. Photobiol. B Biol. 2020, 209, 111942. [Google Scholar] [CrossRef]
- Hirose, M.; Yoshida, Y.; Horii, K.; Hasegawa, Y.; Shibuya, Y. Efficacy of antimicrobial photodynamic therapy with Rose Bengal and blue light against cariogenic bacteria. Arch. Oral Biol. 2021, 122, 105024. [Google Scholar] [CrossRef] [PubMed]
- Samy, N.A.; Salah, M.M.; Ali, M.F.; Sadek, A.M. Effect of methylene blue-mediated photodynamic therapy for treatment of basal cell carcinoma. Lasers Med. Sci. 2015, 30, 109–115. [Google Scholar] [CrossRef]
- Lee, Y.-E.K.; Kopelman, R. Polymeric Nanoparticles for Photodynamic Therapy. In Biomedical Nanotechnology: Methods and Protocols; Hurst, S.J., Ed.; Humana Press: Totowa, NJ, USA, 2011; pp. 151–178. [Google Scholar] [CrossRef]
- Li, Z.; Wang, Y.; Wang, J.; Li, S.; Xiao, Z.; Feng, Y.; Gu, J.; Li, J.; Peng, X.; Li, C.; et al. Evaluation of the efficacy of 5-aminolevulinic acid photodynamic therapy for the treatment of vulvar lichen sclerosus. Photodiagn. Photodyn. Ther. 2020, 29, 101596. [Google Scholar] [CrossRef]
- Malik, Z. Fundamentals of 5-aminolevulinic acid photodynamic therapy and diagnosis: An overview. Transl. Biophotonics 2020, 2, e201900022. [Google Scholar] [CrossRef] [Green Version]
- Alcántara-González, J.; Calzado-Villarreal, L.; Sánchez-Largo, M.E.; Andreu-Barasoain, M.; Ruano-Del Salado, M. Recalcitrant viral warts treated with photodynamic therapy methyl aminolevulinate and red light (630 nm): A case series of 51 patients. Lasers Med Sci. 2020, 35, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, H.; Yamamoto, S.; Karashima, T.; Inoue, K. Photodynamic diagnosis and therapy for urothelial carcinoma and prostate cancer: New imaging technology and therapy. Int. J. Clin. Oncol. 2021, 26, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Salgado, C.N.; Habigton, P.; Itasaki, N.; Scholz, D. Photodynamic Application of Hexvix for Cancer Therapy. Cell Mol. Biol. J. 2016, 1, 2. [Google Scholar]
- Kiesslich, T.; Berlanda, J.; Plaetzer, K.; Krammer, B.; Berr, F. Comparative characterization of the efficiency and cellular pharmacokinetics of Foscan®- and Foslip®-based photodynamic treatment in human biliary tract cancer cell lines. Photochem. Photobiol. Sci. 2007, 6, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Mae, Y.; Kanda, T.; Sugihara, T.; Takata, T.; Kinoshita, H.; Sakaguchi, T.; Hasegawa, T.; Tarumoto, R.; Edano, M.; Kurumi, H.; et al. Verteporfin‑photodynamic therapy is effective on gastric cancer cells. Mol. Clin. Oncol. 2020, 13, 10. [Google Scholar] [CrossRef]
- Iacono, P.; Da Pozzo, S.; Varano, M.; Parravano, M. Photodynamic Therapy with Verteporfin for Chronic Central Serous Chorioretinopathy: A Review of Data and Efficacy. Pharmaceuticals 2020, 13, 349. [Google Scholar] [CrossRef]
- Van Dijk, E.H.C.; van Rijssen, T.J.; Subhi, Y.; Boon, C.J.F. Photodynamic Therapy for Chorioretinal Diseases: A Practical Approach. Ophthalmol. Ther. 2020, 9, 329–342. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, T.; Tanaka, M.; Sasaki, M.; Ichikawa, H.; Nishie, H.; Kataoka, H. Vascular Shutdown by Photodynamic Therapy Using Talaporfin Sodium. Cancers 2020, 12, 2369. [Google Scholar] [CrossRef]
- Nanashima, A.; Hiyoshi, M.; Imamura, N.; Hamada, T.; Nishida, T.; Kawakami, H.; Ban, T.; Kubota, Y.; Nakashima, K.; Yano, K.; et al. Two cases of bile duct carcinoma patients who underwent the photodynamic therapy using talaporfin sodium (Laserphyrin®). Clin. J. Gastroenterol. 2020, 13, 102–109. [Google Scholar] [CrossRef]
- Anju, V.T.; Siddhardha, B.; Dyavaiah, M. Nanostructures for Antimicrobial and Antibiofilm Photodynamic Therapy. In Nanostructures for Antimicrobial and Antibiofilm Applications; Springer: Berlin/Heidelberg, Germany, 2020; pp. 305–325. [Google Scholar]
- Fang, J.; Islam, W.; Maeda, H. Exploiting the dynamics of the EPR effect and strategies to improve the therapeutic effects of nanomedicines by using EPR effect enhancers. Adv. Drug Deliv. Rev. 2020, 157, 142–160. [Google Scholar] [CrossRef]
- Shi, Y.; van der Meel, R.; Chen, X.; Lammers, T. The EPR effect and beyond: Strategies to improve tumor targeting and cancer nanomedicine treatment efficacy. Theranostics 2020, 10, 7921–7924. [Google Scholar] [CrossRef]
- Canaparo, R.; Foglietta, F.; Limongi, T.; Serpe, L. Biomedical Applications of Reactive Oxygen Species Generation by Metal Nanoparticles. Materials 2021, 14, 53. [Google Scholar] [CrossRef]
- Fan, M.; Han, Y.; Gao, S.; Yan, H.; Cao, L.; Li, Z.; Liang, X.-J.; Zhang, J. Ultrasmall gold nanoparticles in cancer diagnosis and therapy. Theranostics 2020, 10, 4944–4957. [Google Scholar] [CrossRef]
- Wang, Q.; Zhang, X.; Sun, Y.; Wang, L.; Ding, L.; Zhu, W.H.; Di, W.; Duan, Y.R. Gold-caged copolymer nanoparticles as multimodal synergistic photodynamic/photothermal/chemotherapy platform against lethality androgen-resistant prostate cancer. Biomaterials 2019, 212, 73–86. [Google Scholar] [CrossRef]
- Tabero, A.; Planas, O.; Gallavardin, T.; Nieves, I.; Nonell, S.; Villanueva, A. Smart Dual-Functionalized Gold Nanoclusters for Spatio-Temporally Controlled Delivery of Combined Chemo- and Photodynamic Therapy. Nanomaterials 2020, 10, 2474. [Google Scholar] [CrossRef]
- Zhang, L.; Cheng, Q.; Li, C.; Zeng, X.; Zhang, X.-Z. Near infrared light-triggered metal ion and photodynamic therapy based on AgNPs/porphyrinic MOFs for tumors and pathogens elimination. Biomaterials 2020, 248, 120029. [Google Scholar] [CrossRef]
- Husain, Q. An overview on the green synthesis of nanoparticles and other nano-materials using enzymes and their potential applications. Biointerface Res. Appl. Chem. 2019, 9, 4255–4271. [Google Scholar] [CrossRef]
- Podgoreanu, P.; Negrea, S.M.; Buia, R.; Delcaru, C.; Trusca, S.B.; Lazar, V.; Chifiriuc, M.C. Alternative strategies for fighting multidrug resistant bacterial infections. Biointerface Res. Appl. Chem. 2019, 9, 3834–3841. [Google Scholar] [CrossRef]
- Parasuraman, P.; Thamanna, R.Y.; Shaji, C.; Sharan, A.; Bahkali, A.H.; Al-Harthi, H.F.; Syed, A.; Anju, V.T.; Dyavaiah, M.; Siddhardha, B. Biogenic Silver Nanoparticles Decorated with Methylene Blue Potentiated the Photodynamic Inactivation of Pseudomonas aeruginosa and Staphylococcus aureus. Pharmaceutics 2020, 12, 709. [Google Scholar] [CrossRef] [PubMed]
- Nain, A.; Wei, S.-C.; Lin, Y.-F.; Tseng, Y.-T.; Mandal, R.P.; Huang, Y.-F.; Huang, C.-C.; Tseng, F.-G.; Chang, H.-T. Copper Sulfide Nanoassemblies for Catalytic and Photoresponsive Eradication of Bacteria from Infected Wounds. ACS Appl. Mater. Interfaces 2021, 13, 7865–7878. [Google Scholar] [CrossRef]
- Qi, C.; Jiang, C.; Fu, L.-H.; Sun, T.; Wang, T.; Lin, J.; Nie, Z.; Huang, P. Melanin-instructed biomimetic synthesis of copper sulfide for cancer phototheranostics. Chem. Eng. J. 2020, 388, 124232. [Google Scholar] [CrossRef]
- Liang, X.; Xie, Y.; Wu, J.; Wang, J.; Petković, M.; Stepić, M.; Zhao, J.; Ma, J.; Mi, L. Functional titanium dioxide nanoparticle conjugated with phthalocyanine and folic acid as a promising photosensitizer for targeted photodynamic therapy in vitro and in vivo. J. Photochem. Photobiol. B Biol. 2021, 215, 112122. [Google Scholar] [CrossRef]
- Badry, R.; Ibrahim, A.; Gamal, F.; Shehata, D.; Ezzat, H.; Elhaes, H.; Ibrahim, M. Electronic Properties of Polyvinyl Alcohol/TiO2/SiO2 Nanocomposites. Biointerface Res. Appl. Chem. 2020, 10, 6427–6435. [Google Scholar] [CrossRef]
- Ziental, D.; Czarczynska-Goslinska, B.; Mlynarczyk, D.T.; Glowacka-Sobotta, A.; Stanisz, B.; Goslinski, T.; Sobotta, L. Titanium Dioxide Nanoparticles: Prospects and Applications in Medicine. Nanomaterials 2020, 10, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, L.; Hu, C.; Liu, S.; Zhou, Y.; Pang, M.; Lin, J. A covalent organic framework-based multifunctional therapeutic platform for enhanced photodynamic therapy via catalytic cascade reactions. Sci. China Mater. 2021, 64, 488–497. [Google Scholar] [CrossRef]
- Rajakumar, G.; Mao, L.; Bao, T.; Wen, W.; Wang, S.; Gomathi, T.; Gnanasundaram, N.; Rebezov, M.; Shariati, M.A.; Chung, I.-M.; et al. Yttrium Oxide Nanoparticle Synthesis: An Overview of Methods of Preparation and Biomedical Applications. Appl. Sci. 2021, 11, 2172. [Google Scholar] [CrossRef]
- Zeng, L.; Gupta, P.; Chen, Y.; Wang, E.; Ji, L.; Chao, H.; Chen, Z.-S. The development of anticancer ruthenium(ii) complexes: From single molecule compounds to nanomaterials. Chem. Soc. Rev. 2017, 46, 5771–5804. [Google Scholar] [CrossRef]
- Er, O.; Tuncel, A.; Ocakoglu, K.; Ince, M.; Kolatan, E.H.; Yilmaz, O.; Aktaş, S.; Yurt, F. Radiolabeling, In Vitro Cell Uptake, and In Vivo Photodynamic Therapy Potential of Targeted Mesoporous Silica Nanoparticles Containing Zinc Phthalocyanine. Mol. Pharm. 2020, 17, 2648–2659. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Gai, S.; Wang, C.; Yang, G.; Zhong, C.; Dai, Y.; He, F.; Yang, D.; Yang, P. Self-assembled zinc phthalocyanine nanoparticles as excellent photothermal/photodynamic synergistic agent for antitumor treatment. Chem. Eng. J. 2019, 361, 117–128. [Google Scholar] [CrossRef]
- Serda, M.; Szewczyk, G.; Krzysztyńska-Kuleta, O.; Korzuch, J.; Dulski, M.; Musioł, R.; Sarna, T. Developing [60] Fullerene Nanomaterials for Better Photodynamic Treatment of Non-Melanoma Skin Cancers. ACS Biomater. Sci. Eng. 2020, 6, 5930–5940. [Google Scholar] [CrossRef]
- Sundaram, P.; Abrahamse, H. Effective Photodynamic Therapy for Colon Cancer Cells Using Chlorin e6 Coated Hyaluronic Acid-Based Carbon Nanotubes. Int. J. Mol. Sci. 2020, 21, 4745. [Google Scholar] [CrossRef]
- Barańska, E.; Wiecheć-Cudak, O.; Rak, M.; Bienia, A.; Mrozek-Wilczkiewicz, A.; Krzykawska-Serda, M.; Serda, M. Interactions of a Water-Soluble Glycofullerene with Glucose Transporter 1. Analysis of the Cellular Effects on a Pancreatic Tumor Model. Nanomaterials 2021, 11, 513. [Google Scholar] [CrossRef] [PubMed]
- Monroe, J.D.; Belekov, E.; Er, A.O.; Smith, M.E. Anticancer Photodynamic Therapy Properties of Sulfur-Doped Graphene Quantum Dot and Methylene Blue Preparations in MCF-7 Breast Cancer Cell Culture. Photochem. Photobiol. 2019, 95, 1473–1481. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, R.; Thakur, M.; Kumawat, M.K.; Bahadur, R. Graphene-Based Nanomaterials in Cancer Therapy. In Next Generation Graphene Nanomaterials for Cancer Theranostic Applications; Springer: Berlin/Heidelberg, Germany, 2021; pp. 95–125. [Google Scholar]
- Radhi, A.; Mohamad, D.; Abdul Rahman, F.S.; Abdullah, A.M.; Hasan, H. Mechanism and factors influence of graphene-based nanomaterials antimicrobial activities and application in dentistry. J. Mater. Res. Technol. 2021, 11, 1290–1307. [Google Scholar] [CrossRef]
- Lu, D.; Tao, R.; Wang, Z. Carbon-based materials for photodynamic therapy: A mini-review. Front. Chem. Sci. Eng. 2019, 13, 310–323. [Google Scholar] [CrossRef]
- Ménard-Moyon, C. Applications of Carbon Nanotubes in the Biomedical Field. In Smart Nanoparticles for Biomedicine; Ciofani, G., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 83–101. [Google Scholar] [CrossRef]
- Duan, X.; Jiang, X.-F.; Hu, D.; Liu, P.; Li, S.; Huang, F.; Ma, Y.; Xu, Q.-H.; Cao, Y. Red emitting conjugated polymer based nanophotosensitizers for selectively targeted two-photon excitation imaging guided photodynamic therapy. Nanoscale 2019, 11, 185–192. [Google Scholar] [CrossRef]
- Grewal, I.K.; Singh, S.; Arora, S.; Sharma, N. Polymeric Nanoparticles for Breast Cancer Therapy: A Comprehensive Review. Biointerface Res. Appl. Chem. 2020, 11, 11151–11171. [Google Scholar] [CrossRef]
- Bechet, D.; Couleaud, P.; Frochot, C.; Viriot, M.-L.; Guillemin, F.; Barberi-Heyob, M. Nanoparticles as vehicles for delivery of photodynamic therapy agents. Trends Biotechnol. 2008, 26, 612–621. [Google Scholar] [CrossRef]
- Qin, M.; Hah, H.J.; Kim, G.; Nie, G.; Lee, Y.-E.K.; Kopelman, R. Methylene blue covalently loaded polyacrylamide nanoparticles for enhanced tumor-targeted photodynamic therapy. Photochem. Photobiol. Sci. 2011, 10, 832–841. [Google Scholar] [CrossRef] [Green Version]
- Tang, W.; Xu, H.; Park, E.J.; Philbert, M.A.; Kopelman, R. Encapsulation of methylene blue in polyacrylamide nanoparticle platforms protects its photodynamic effectiveness. Biochem. Biophys. Res. Commun. 2008, 369, 579–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gualdesi, M.S.; Vara, J.; Aiassa, V.; Alvarez Igarzabal, C.I.; Ortiz, C.S. Thionine in the design of new photosensitizers: Bromination and vehiculization in polymeric nanoparticles. J. Mol. Liq. 2020, 310, 113247. [Google Scholar] [CrossRef]
- Yakavets, I.; Millard, M.; Zorin, V.; Lassalle, H.-P.; Bezdetnaya, L. Current state of the nanoscale delivery systems for temoporfin-based photodynamic therapy: Advanced delivery strategies. J. Control. Release 2019, 304, 268–287. [Google Scholar] [CrossRef]
- Calixto, G.M.; Bernegossi, J.; De Freitas, L.M.; Fontana, C.R.; Chorilli, M. Nanotechnology-Based Drug Delivery Systems for Photodynamic Therapy of Cancer: A Review. Molecules 2016, 21, 342. [Google Scholar] [CrossRef]
- Prajapati, S.K.; Maurya, S.D.; Das, M.K.; Tilak, V.K.; Verma, K.K.; Dhakar, R.C. Dendrimers in drug delivery, diagnosis and therapy: Basics and potential applications. J. Drug Deliv. Ther. 2016, 6, 67–92. [Google Scholar] [CrossRef]
- Mizrahy, S.; Hazan-Halevy, I.; Landesman-Milo, D.; Peer, D. Advanced strategies in immune modulation of cancer using lipid-based nanoparticles. Front. Immunol. 2017, 8, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, T.; Ni, K.; Culbert, A.; Lan, G.; Li, Z.; Jiang, X.; Kaufmann, M.; Lin, W. Nanoscale Metal–Organic Frameworks Stabilize Bacteriochlorins for Type I and Type II Photodynamic Therapy. J. Am. Chem. Soc. 2020, 142, 7334–7339. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, F.; Liu, C.; Wang, Z.; Kang, L.; Huang, Y.; Dong, K.; Ren, J.; Qu, X. Nanozyme Decorated Metal–Organic Frameworks for Enhanced Photodynamic Therapy. ACS Nano 2018, 12, 651–661. [Google Scholar] [CrossRef]
- Liu, Y.; Gong, C.S.; Lin, L.; Zhou, Z.; Liu, Y.; Yang, Z.; Shen, Z.; Yu, G.; Wang, Z.; Wang, S.; et al. Core-shell metal-organic frameworks with fluorescence switch to trigger an enhanced photodynamic therapy. Theranostics 2019, 9, 2791–2799. [Google Scholar] [CrossRef]
- Xu, W.; Qian, J.; Hou, G.; Wang, Y.; Wang, J.; Sun, T.; Ji, L.; Suo, A.; Yao, Y. A dual-targeted hyaluronic acid-gold nanorod platform with triple-stimuli responsiveness for photodynamic/photothermal therapy of breast cancer. Acta Biomater. 2019, 83, 400–413. [Google Scholar] [CrossRef]
- Radwan, A.; Khalid, M.; Amer, H.; Alotaibi, M. Anticancer and molecular docking studies of some new pyrazole-1-carbothioamide. Biointerface Res. Appl. Chem. 2019, 9, 4642–4648. [Google Scholar] [CrossRef]
- Asaduzzaman, S.; Chakma, R.; Rehana, H.; Raihan, M. Regulatory Gene Network Pathway among Brain Cancer and Associated Disease: A Computational Analysis. Biointerface Res. Appl. Chem. 2021, 11, 12973–12984. [Google Scholar] [CrossRef]
- Mai, T.T.; Yoo, S.W.; Park, S.; Kim, J.Y.; Choi, K.-H.; Kim, C.; Kwon, S.Y.; Min, J.-J.; Lee, C. In Vivo Quantitative Vasculature Segmentation and Assessment for Photodynamic Therapy Process Monitoring Using Photoacoustic Microscopy. Sensors 2021, 21, 1776. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, H.; Nishie, H.; Tanaka, M.; Sasaki, M.; Nomoto, A.; Osaki, T.; Okamoto, Y.; Yano, S. Potential of Photodynamic Therapy Based on Sugar-Conjugated Photosensitizers. J. Clin. Med. 2021, 10, 841. [Google Scholar] [CrossRef]
- Mroz, P.; Yaroslavsky, A.; Kharkwal, G.B.; Hamblin, M.R. Cell Death Pathways in Photodynamic Therapy of Cancer. Cancers 2011, 3, 2516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Albuquerque, I.O.; Nunes, J.; Figueiró Longo, J.P.; Muehlmann, L.A.; Azevedo, R.B. Photodynamic therapy in superficial basal cell carcinoma treatment. Photodiagn. Photodyn. Ther. 2019, 27, 428–432. [Google Scholar] [CrossRef]
- Rey-Barroso, L.; Peña-Gutiérrez, S.; Yáñez, C.; Burgos-Fernández, F.J.; Vilaseca, M.; Royo, S. Optical Technologies for the Improvement of Skin Cancer Diagnosis: A Review. Sensors 2021, 21, 252. [Google Scholar] [CrossRef] [PubMed]
- Zaar, O.; Fougelberg, J.; Hermansson, A.; Gillstedt, M.; Wennberg-Larkö, A.M.; Paoli, J. Effectiveness of photodynamic therapy in Bowen’s disease: A retrospective observational study in 423 lesions. J. Eur. Acad. Dermatol. Venereol. JEADV 2017, 31, 1289–1294. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M.; Sandhu, S.S.; Sivamani, R.K. Clinical utility of daylight photodynamic therapy in the treatment of actinic keratosis—A review of the literature. Clin. Cosmet. Investig. Dermatol. 2019, 12, 427–435. [Google Scholar] [CrossRef] [Green Version]
- Abe, C.; Imai, T.; Sezaki, A.; Miyamoto, K.; Kawase, F.; Shirai, Y.; Sanada, M.; Inden, A.; Kato, T.; Shimokata, H. A longitudinal association between the traditional Japanese diet score and incidence and mortality of breast cancer—an ecological study. Eur. J. Clin. Nutr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, R.T.D.; Franca, E.L.; Triches, D.; Fujimori, M.; Machi, P.G.F.; Massmman, P.F.; Tozetti, I.A.; Honorio-Franca, A.C. Nanodoses of melatonin induces apoptosis on human breast cancer cells co-cultured with colostrum cells. Biointerface Res. Appl. Chem. 2019, 9, 4416–4423. [Google Scholar] [CrossRef]
- Banerjee, S.M.; El-Sheikh, S.; Malhotra, A.; Mosse, C.A.; Parker, S.; Williams, N.R.; MacRobert, A.J.; Hamoudi, R.; Bown, S.G.; Keshtgar, M.R.S. Photodynamic Therapy in Primary Breast Cancer. J. Clin. Med. 2020, 9, 483. [Google Scholar] [CrossRef] [Green Version]
- El-Hussein, A.; Manoto, S.L.; Ombinda-Lemboumba, S.; Alrowaili, Z.A.; Mthunzi-Kufa, P. A Review of Chemotherapy and Photodynamic Therapy for Lung Cancer Treatment. Anti-Cancer Agents Med. Chem. Anti-Cancer Agents 2021, 21, 149–161. [Google Scholar] [CrossRef]
- Jayadevappa, R.; Chhatre, S.; Soukiasian, H.J.; Murgu, S. Outcomes of patients with advanced non-small cell lung cancer and airway obstruction treated with photodynamic therapy and non-photodynamic therapy ablation modalities. J. Thorac. Dis. 2019, 11, 4389–4399. [Google Scholar] [CrossRef]
- Luo, M.; Fan, D.; Xiao, Y.; Zeng, H.; Zhang, D.; Zhao, Y.; Ma, X. Anticancer Effect of Natural Product Sulforaphane by Targeting MAPK Signal through miRNA-1247-3p in Human Cervical Cancer Cells. Biointerface Res. Appl. Chem. 2020, 11, 7943–7972. [Google Scholar] [CrossRef]
- Vendette, A.C.F.; Piva, H.L.; Muehlmann, L.A.; de Souza, D.A.; Tedesco, A.C.; Azevedo, R.B. Clinical treatment of intra-epithelia cervical neoplasia with photodynamic therapy. Int. J. Hyperth. 2020, 37, 50–58. [Google Scholar] [CrossRef]
- Xu, D.D.; Leong, M.M.L.; Wong, F.-L.; Lam, H.M.; Hoeven, R. Photodynamic therapy on prostate cancer cells involve mitochondria membrane proteins. Photodiagn. Photodyn. Ther. 2020, 31, 101933. [Google Scholar] [CrossRef] [PubMed]
- Osuchowski, M.; Bartusik-Aebisher, D.; Osuchowski, F.; Aebisher, D. Photodynamic therapy for prostate cancer—A narrative review. Photodiagn. Photodyn. Ther. 2021, 33, 102158. [Google Scholar] [CrossRef]
- Yano, T.; Wang, K.K. Photodynamic Therapy for Gastrointestinal Cancer. Photochem. Photobiol. 2020, 96, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Gan, J.; Li, S.; Meng, Y.; Liao, Y.; Jiang, M.; Qi, L.; Li, Y.; Bai, Y. The influence of photodynamic therapy on the Warburg effect in esophageal cancer cells. Lasers Med. Sci. 2020, 35, 1741–1750. [Google Scholar] [CrossRef]
- Inoue, T.; Ishihara, R. Photodynamic Therapy for Esophageal Cancer. Clin. Endosc. 2020. [Google Scholar] [CrossRef]
- Afzal, A.; Qayyum, M.A.; Shah, M.H. Comparative Assessment of Trace Elements in the Blood of Gastric Cancer Patients and Healthy Subjects. Biointerface Res. Appl. Chem. 2020, 11, 10824–10843. [Google Scholar] [CrossRef]
- Tanaka, M.; Sasaki, M.; Suzuki, T.; Nishie, H.; Kataoka, H. Combination of talaporfin photodynamic therapy and Poly (ADP-Ribose) polymerase (PARP) inhibitor in gastric cancer. Biochem. Biophys. Res. Commun. 2021, 539, 1–7. [Google Scholar] [CrossRef]
- Guo, W.; Chen, Z.; Feng, X.; Shen, G.; Huang, H.; Liang, Y.; Zhao, B.; Li, G.; Hu, Y. Graphene Oxide (GO)-based Nanosheets With Combined Chemo/photothermal/Photodynamic Therapy to Overcome Gastric Cancer (GC) Paclitaxel Resistance by Reducing Mitochondria-Derived Adenosine-Triphosphate (ATP). J. Nanobiotechnol. 2021. [Google Scholar] [CrossRef]
- Zou, H.; Wang, F.; Zhou, J.-J.; Liu, X.; He, Q.; Wang, C.; Zheng, Y.-W.; Wen, Y.; Xiong, L. Application of photodynamic therapy for liver malignancies. J. Gastrointest. Oncol. 2020, 11, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Satiya, J.; Schwartz, I.; Tabibian, J.H.; Kumar, V.; Girotra, M. Ablative therapies for hepatic and biliary tumors: Endohepatology coming of age. Transl. Gastroenterol. Hepatol. 2020, 5, 15. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, H.; Zhou, L.; Lu, J.; Jiang, B.; Liu, C.; Guo, J. Photodynamic therapy of pancreatic cancer: Where have we come from and where are we going? Photodiagn. Photodyn. Ther. 2020, 31, 101876. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Liu, R.; Xu, Y.; Qian, L.; Dai, Z. Photosensitizer Nanoparticles Boost Photodynamic Therapy for Pancreatic Cancer Treatment. Nano-Micro Lett. 2021, 13, 35. [Google Scholar] [CrossRef]
- Quilbe, A.; Moralès, O.; Baydoun, M.; Kumar, A.; Mustapha, R.; Murakami, T.; Leroux, B.; de Schutter, C.; Thecua, E.; Ziane, L.; et al. An Efficient Photodynamic Therapy Treatment for Human Pancreatic Adenocarcinoma. J. Clin. Med. 2020, 9, 192. [Google Scholar] [CrossRef] [Green Version]
- Nompumelelo Simelane, N.W.; Kruger, C.A.; Abrahamse, H. Photodynamic diagnosis and photodynamic therapy of colorectal cancer in vitro and in vivo. RSC Adv. 2020, 10, 41560–41576. [Google Scholar] [CrossRef]
- Nkune, N.W.; Kruger, C.A.; Abrahamse, H. Possible Enhancement of Photodynamic Therapy (PDT) Colorectal Cancer Treatment when Combined with Cannabidiol. Anti Cancer Agents Med. Chem. 2021, 21, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Xu, W.; Wu, H.; Wang, X.; Gong, Q.; Liu, C.; Liu, J.; Zhou, L. Photodynamic therapy induces autophagy-mediated cell death in human colorectal cancer cells via activation of the ROS/JNK signaling pathway. Cell Death Dis. 2020, 11, 938. [Google Scholar] [CrossRef]
- Cramer, S.W.; Chen, C.C. Photodynamic therapy for the treatment of glioblastoma. Front. Surg. 2020, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barra, F.; Roscetto, E.; Soriano, A.A.; Vollaro, A.; Postiglione, I.; Pierantoni, G.M.; Palumbo, G.; Catania, M.R. Photodynamic and Antibiotic Therapy in Combination to Fight Biofilms and Resistant Surface Bacterial Infections. Int. J. Mol. Sci. 2015, 16, 417. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ogawa, R.; Xiao, B.-H.; Feng, Y.-X.; Wu, Y.; Chen, L.-H.; Gao, X.-H.; Chen, H.-D. Antimicrobial photodynamic therapy in skin wound healing: A systematic review of animal studies. Int. Wound J. 2020, 17, 285–299. [Google Scholar] [CrossRef]
- Oyama, J.; Fernandes Herculano Ramos-Milaré, Á.C.; Lopes Lera-Nonose, D.S.S.; Nesi-Reis, V.; Galhardo Demarchi, I.; Alessi Aristides, S.M.; Juarez Vieira Teixeira, J.; Gomes Verzignassi Silveira, T.; Campana Lonardoni, M.V. Photodynamic therapy in wound healing in vivo: A systematic review. Photodiagn. Photodyn. Ther. 2020, 30, 101682. [Google Scholar] [CrossRef]
- Silvestre, A.L.P.; Di Filippo, L.D.; Besegato, J.F.; de Annunzio, S.R.; Almeida Furquim de Camargo, B.; de Melo, P.B.G.; Rastelli, A.N.d.S.; Fontana, C.R.; Chorilli, M. Current applications of drug delivery nanosystems associated with antimicrobial photodynamic therapy for oral infections. Int. J. Pharm. 2021, 592, 120078. [Google Scholar] [CrossRef]
- Aggarwal, R.; Targhotra, M.; Kumar, B.; Sahoo, P.K.; Chauhan, M.K. Treatment and management strategies of onychomycosis. J. Mycol. Méd. 2020, 30, 100949. [Google Scholar] [CrossRef]
- Svyatchenko, V.A.; Nikonov, S.D.; Mayorov, A.P.; Gelfond, M.L.; Loktev, V.B. Antiviral photodynamic therapy: Inactivation and inhibition of SARS-CoV-2 in vitro using methylene blue and Radachlorin. Photodiagn. Photodyn. Ther. 2021, 33, 102112. [Google Scholar] [CrossRef]
- Namvar, M.A.; Vahedi, M.; Abdolsamadi, H.R.; Mirzaei, A.; Mohammadi, Y.; Azizi Jalilian, F. Effect of photodynamic therapy by 810 and 940 nm diode laser on Herpes Simplex Virus 1: An in vitro study. Photodiagn. Photodyn. Ther. 2019, 25, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Owczarek, W.; Slowinska, M.; Walecka, I.; Ciazynska, M.; Nowicka, D.; Walczak, L.; Paluchowska, E. Correlation of the ALA-PDT Treatment Efficacy and the HPV Genotype Profile of Genital Warts after Cryotherapy Failure and Podophyllotoxin Therapy in Male Patients. Life 2021, 11, 146. [Google Scholar] [CrossRef] [PubMed]
- Fekrazad, R. Photobiomodulation and Antiviral Photodynamic Therapy as a Possible Novel Approach in COVID-19 Management. Photobiomodul. Photomed. Laser Surg. 2020, 38, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Kipshidze, N.; Yeo, N.; Kipshidze, N. Photodynamic therapy for COVID-19. Nat. Photonics 2020, 14, 651–652. [Google Scholar] [CrossRef]
- Almeida, A.; Faustino, M.A.F.; Neves, M.G.P.M.S. Antimicrobial Photodynamic Therapy in the Control of COVID-19. Antibiotics 2020, 9, 320. [Google Scholar] [CrossRef] [PubMed]
- Dias, L.D.; Blanco, K.C.; Bagnato, V.S. COVID-19: Beyond the virus. The use of photodynamic therapy for the treatment of infections in the respiratory tract. Photodiagn. Photodyn. Ther. 2020, 31, 101804. [Google Scholar] [CrossRef] [PubMed]
- Conrado, P.C.V.; Sakita, K.M.; Arita, G.S.; Galinari, C.B.; Gonçalves, R.S.; Lopes, L.D.G.; Lonardoni, M.V.C.; Teixeira, J.J.V.; Bonfim-Mendonça, P.S.; Kioshima, E.S. A systematic review of photodynamic therapy as an antiviral treatment: Potential guidance for dealing with SARS-CoV-2. Photodiagn. Photodyn. Ther. 2021, 34, 102221. [Google Scholar] [CrossRef]
- Fujita, K.; Shinoda, K.; Imamura, Y.; Matsumoto, C.S.; Oda, K. Improvement of Low Luminance Visual Acuity in Patients with Chronic Central Serous Chorioretinopathy after Half-Dose Verteporfin Photodynamic Therapy. J. Clin. Med. 2020, 9, 3980. [Google Scholar] [CrossRef]
- Chan, W.M.; Lam, D.S.C.; Lai, T.Y.Y.; Tam, B.S.M.; Liu, D.T.L.; Chan, C.K.M. Choroidal vascular remodelling in central serous chorioretinopathy after indocyanine green guided photodynamic therapy with verteporfin: A novel treatment at the primary disease level. Br. J. Ophthalmol. 2003, 87, 1453. [Google Scholar] [CrossRef] [Green Version]
- Piccolino, F.C.; Eandi, C.M.; Ventre, L.; Rigault De La Longrais, R.C.; Grignolo, F.M. Photodynamic Therapy for Chronic Central Serous Chorioretinopathy. RETINA 2003, 23, 752–763. [Google Scholar] [CrossRef]
- Wakatsuki, Y.; Tanaka, K.; Mori, R.; Furuya, K.; Kawamura, A.; Nakashizuka, H. Morphological Changes and Prognostic Factors before and after Photodynamic Therapy for Central Serous Chorioretinopathy. Pharmaceuticals 2021, 14, 53. [Google Scholar] [CrossRef]
- Li, X.; Sun, L.; Zhang, P.; Wang, Y. Novel Approaches to Combat Medical Device-Associated BioFilms. Coatings 2021, 11, 294. [Google Scholar] [CrossRef]
- Wylie, M.P.; Irwin, N.J.; Howard, D.; Heydon, K.; McCoy, C.P. Hot-melt extrusion of photodynamic antimicrobial polymers for prevention of microbial contamination. J. Photochem. Photobiol. B Biol. 2021, 214, 112098. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A. Photodynamic Therapy in the Inactivation of Microorganisms. Antibiotics 2020, 9, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Wu, J.; Xu, C.; Lu, N.; Gao, Y.; Xue, Y.; Li, Z.; Xue, C.; Tang, Q. Inactivation of microbes on fruit surfaces using photodynamic therapy and its influence on the postharvest shelf-life of fruits. Food Sci. Technol. Int. 2020, 26, 696–705. [Google Scholar] [CrossRef]
- Le, T.D.; Phasupan, P.; Nguyen, L.T. Antimicrobial photodynamic efficacy of selected natural photosensitizers against food pathogens: Impacts and interrelationship of process parameters. Photodiagn. Photodyn. Ther. 2020, 32, 102024. [Google Scholar] [CrossRef] [PubMed]
- Couto, G.K.; Seixas, F.K.; Iglesias, B.A.; Collares, T. Perspectives of photodynamic therapy in biotechnology. J. Photochem. Photobiol. B Biol. 2020, 213, 112051. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Huang, J.; Li, H.; Pan, Y.; Zhu, B.; Zhao, Y.; Liu, H. Chitosan-riboflavin composite film based on photodynamic inactivation technology for antibacterial food packaging. Int. J. Biol. Macromol. 2021, 172, 231–240. [Google Scholar] [CrossRef]
Figure 1.
Main components of photodynamic therapy. Created based on literature references [12,18,26,27,28].

Figure 2.
Schematic representation of photodynamic therapy (PDT) mechanism. Created based on literature references [2,7,8,18,26,27,28,32,33,34,35].

Figure 3.
Modifications of PDT for increasing drug selectivity. Created based on information from literature reference [7].
Figure 3.
Modifications of PDT for increasing drug selectivity. Created based on information from literature reference [7].

Figure 4.
Schematic representation of possible combinations between nanoparticles and photosensitizers (PSs): (a) nanoparticles embedded with PSs; (b) nanoparticles with PSs bound to the surface; (c) nanoparticles as PSs; (d) PSs along nanoparticles. Created based on information from literature reference [64].
Figure 4.
Schematic representation of possible combinations between nanoparticles and photosensitizers (PSs): (a) nanoparticles embedded with PSs; (b) nanoparticles with PSs bound to the surface; (c) nanoparticles as PSs; (d) PSs along nanoparticles. Created based on information from literature reference [64].

Figure 5.
Possible combinations between PDT and other therapeutic strategies. Created based on literature reference [11].
Figure 5.
Possible combinations between PDT and other therapeutic strategies. Created based on literature reference [11].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Examples of photosensitizers.
| Photosensitizer | Absorption Range | Approval Status | Potential Applications | Refs. |
|---|---|---|---|---|
| Photofrin (sodium porfimer) | ~630 nm | FDA approved (for treatment of carcinomas) | Radiation therapy for the palliative treatment of respiratory, alimentary tract, head and neck squamous cell carcinomas, treatment of breast cancer skin metastases | [44,45] |
| Indocyanine green (ICG) | Near-infrared (>800 nm) | FDA approved (for diagnostic in cardiology, hepatology, ophthalmology, fluorescence-guided cancer surgery) | Topical melanoma PDT, management of chronic periodontitis | [46,47,48] |
| Methylene blue | 600–665 nm | Approved in Canada (for periodontal diseases and nasal decolonization of Staphylococcus aureus) | Photoantimicrobial activity against yeasts and filamentous fungi, dental caries, basal cell carcinoma | [19,49,50,51,52] |
| Rose Bengal | 500–550 nm | Dental caries | [19,50] | |
| Curcumin | 300–500 nm | Not yet approved | Local superficial infections and cancers | [1,37] |
| Thiophenes | 225–400 nm | Skin and cervix cancer | [1] | |
| 5-Aminolevulinic acid (ALA) | 410–630 nm | FDA approved (for dermatology indications) | Hypertrophic actinic keratoses on the face and scalp, vulvar lichen sclerosus, glioblastoma | [6,53,54] |
| Methyl aminolevulinate (MAL) | ~630 nm | FDA approved (for dermatology indications) | Actinic keratoses, basal cell carcinoma, Bowen disease, viral warts | [6,11,55] |
| Hexvix/Cysview | 380–450 nm | EU and FDA approved (for intravesical administration and diagnosis of bladder cancer) | Bladder cancer, prostate cancer, colon cancer | [56,57] |
| Meta-tetrahydroxy-phenylchlorin (m-THPC) | ~652 nm | Approved in EU (for palliative treatment of patients with advanced head and neck cancer) | Pancreatic cancer, biliary cancer, breast cancer metastases | [45,52,58] |
| Lutetium texaphyrin | ~732 nm | Phase I trial (for locally recurrent prostate cancer) | Skin metastases, breast cancer | [45,52] |
| Verteporfin | ~689 nm | Approved in Japan (for subfoveal choroidal neovascularization in wet age-related macular degeneration) | Central serous chorioretinopathy (CSCR), choroidal hemangioma, gastric cancer | [6,59,60,61] |
| Talaporfin sodium | ~664 nm | Approved in Japan (for early endobronchial carcinoma) | Esophageal cancer, gastric cancer, bile duct carcinoma | [52,59,62,63] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Niculescu, A.-G.; Grumezescu, A.M. Photodynamic Therapy—An Up-to-Date Review. Appl. Sci. 2021, 11, 3626. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083626
AMA Style
Niculescu A-G, Grumezescu AM. Photodynamic Therapy—An Up-to-Date Review. Applied Sciences. 2021; 11(8):3626. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083626
Chicago/Turabian StyleNiculescu, Adelina-Gabriela, and Alexandru Mihai Grumezescu. 2021. "Photodynamic Therapy—An Up-to-Date Review" Applied Sciences 11, no. 8: 3626. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083626
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.