
Haptic-Enabled Hand Rehabilitation in Stroke Patients: A Scoping Review




1
College of Rehabilitation Sciences, University of Manitoba, Winnipeg, MB R3E 0T6, Canada
2
Riverview Health Centre, Winnipeg, MB R3L 2P4, Canada
3
Centre on Aging, University of Manitoba, Winnipeg, MB R3T 2N2, Canada
4
Neil John Maclean Health Sciences Library, University of Manitoba, Winnipeg, MB R3T 2N2, Canada
*
Author to whom correspondence should be addressed.
Appl. Sci. 2021, 11(8), 3712; https://0-doi-org.brum.beds.ac.uk/10.3390/app11083712
Submission received: 1 March 2021
/
Revised: 14 April 2021
/
Accepted: 15 April 2021
/
Published: 20 April 2021
(This article belongs to the Special Issue Advances in Technological Rehabilitation)
Abstract
:There is a plethora of technology-assisted interventions for hand therapy, however, less is known about the effectiveness of these interventions. This scoping review aims to explore studies about technology-assisted interventions targeting hand rehabilitation to identify the most effective interventions. It is expected that multifaceted interventions targeting hand rehabilitation are more efficient therapeutic approaches than mono-interventions. The scoping review will aim to map the existing haptic-enabled interventions for upper limb rehabilitation and investigates their effects on motor and functional recovery in patients with stroke. The methodology used in this review is based on the Arksey and O’Malley framework, which includes the following stages: identifying the research question, identifying relevant studies, study selection, charting the data, and collating, summarizing, and reporting the results. Results show that using three or four different technologies was more positive than using two technologies (one technology + haptics). In particular, when standardized as a percentage of outcomes, the combination of three technologies showed better results than the combination of haptics with one technology or with three other technologies. To conclude, this study portrayed haptic-enabled rehabilitation approaches that could help therapists decide which technology-enabled hand therapy approach is best suited to their needs. Those seeking to undertake research and development anticipate further opportunities to develop haptic-enabled hand telerehabilitation platforms.
Keywords:
hand; neurologic; rehabilitation; sensory integration; haptic; tactile; robotic; virtual reality; augmented reality1. Introduction
Strokes are the second leading cause of death and the third leading cause of disability globally [1]. In 2010, there were 16.9 million new strokes, 33 million stroke survivors, 5.9 million stroke-related deaths, and 102 million disability-adjusted life years lost due to strokes [2]. In Canada, the prevalence of stroke is 1.2% with approximately 405,000 Canadians experiencing a stroke in 2013. This number is expected to increase from 405, 000 to between 654,000 and 726,000 in 2038 [3]. The most common post-stroke deficiency is hemiparesis of the upper contralateral limb. This condition affects the functional independence and satisfaction among 50 to 70% of patients with stroke. Approximately 80% of patients experience acute hemiparesis while 40% experience this condition chronically [4]. Recovery of functional outcomes post-stroke is heterogeneous. About 71% of patients with mild to moderate upper extremity paresis achieved some dexterity after 6 months post-stroke, while the same was true for only 60% of severely affected patients. Only 5% of people who have undergone total paralysis have achieved functional use of their arm [4].
Patients who have had a stroke are often faced with permanent movement impairments that limit their ability to engage in meaningful occupations such as self-care, leisure activities, or work. Impaired hand function is among the most common effects of stroke [5]. Hand or upper limb weakness happens severely in up to 87% of patients with stroke [6,7]. The hand rehabilitation process aims to reduce spasticity, increase neuroplasticity enhance functional outcomes. Spasticity was defined by Lance et al. as “a motor disorder characterized by a velocity-dependent increase in tonic stretch reflexes with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex” [8] (p. 485). Neuroplasticity, also known as neural plasticity, or brain plasticity, is the “capacity of neurons and neural networks in the brain to change their connections and behaviour in response to new information, sensory stimulation, development, damage, or dysfunction” [9]. While clinicians tend to profit from a substantial amount of time spent in treating spasticity and neuroplasticity after the stroke [10,11], studies show that they may not be having enough care. Compared with other patient populations, patients who have had a stroke spend more time inactive and alone or less active on rehabilitation units, more likely because of reduced sensorimotor capacity [12,13]. Hence, there seems to be a difference in practice between how much training stroke patients need and how much they receive. Therefore, it is beneficial to investigate ways to increase both the efficacy of training upper limb and hand movement. Robotic-assisted therapies are increasingly becoming available for stroke rehabilitation. The basic components of robotic-assisted therapy are (1) motorized mechanical component; (2) performance-related visual feedback; and (3) an interactive computer program that monitors progress. The ability to provide high-dosage and high-intensity interventions is a significant advantage of robotic-assisted devices [4]. A lack of devices targeting hand rehabilitation exists as most current devices target elbow and shoulder movements. Evidence shows that robotic-assisted therapy combined with virtual reality appears to be a valuable intervention for stroke rehabilitation [4].
Therapists dealing with this population use strategies to improve motor behaviour to regain occupational performance. Treatment interventions such as materials-based training [14], task-related [15,16] or task-specific training [17,18] are common training methods for restoring function in the upper limb. Such training methods emphasize the patient’s active participation, the use of goal-oriented tasks or environmental features to drive motor activity, and the execution of the entire task or components of the task under different conditions. Several studies have failed to demonstrate the superiority of one type of conventional stroke training over another [19,20,21,22]. Our understanding of brain function and brain trainability is becoming more evident with identifying mirror neurons and the recent development of neuroimaging techniques. This training modality has traditionally been used in athletics in an intuitive manner [23,24] to review or reinforce the sequence of movements that make up the action to be taken. Mental practice has been shown to be effective in reducing impairment and improving functional recovery [25]. Literature shows that mental practice is an effective intervention when it is added to physical practice [25]. Although functional imaging has shown that mental practice induces similar cortical activation patterns, such interventions’ clinical efficacy in the treatment and functional recovery has yet to be demonstrated [25].
Retraining a motor task can be controlled more precisely than conventional treatment approaches by using a variety of technologies such as robots (e.g., [26,27,28,29,30,31,32]), virtual reality (e.g., [33,34,35,36]) and sensor-based devices (e.g., [37,38,39]). The complex nature of the human hands and arms and the various daily activities will contribute to an approach in which specific approaches were integrated to address the diverse needs of upper limb/hand rehabilitation. Further research is needed to determine the most effective technology-assisted intervention or combination of interventions. This paper aims (i) to draw a portrait of existing haptic-enabled hand rehabilitation in stroke patients, (ii) to map the use of haptic technology to support technology-assisted therapeutic interventions, and (iii) to investigate the effects of haptic-enabled interventions on the motor and functional recovery in patients with stroke. One of the common locations to apply haptic technology to provide biofeedback is the hand (e.g., [37,38,39,40,41]). Integration of haptic technology in hand therapy plays a significant role in the interaction between the body and the objects. A better sense of touch determines the efficacy of daily life movements. Haptics can be defined as “the perception of combined tactile and kinesthetic inputs during object manipulation and exploration” [42]. It is expected that the haptic feedback increases motor and functional recovery. It is hypothesized that the more different technologies are combined with haptic technology, the better the therapeutic outcomes.
2. Methods
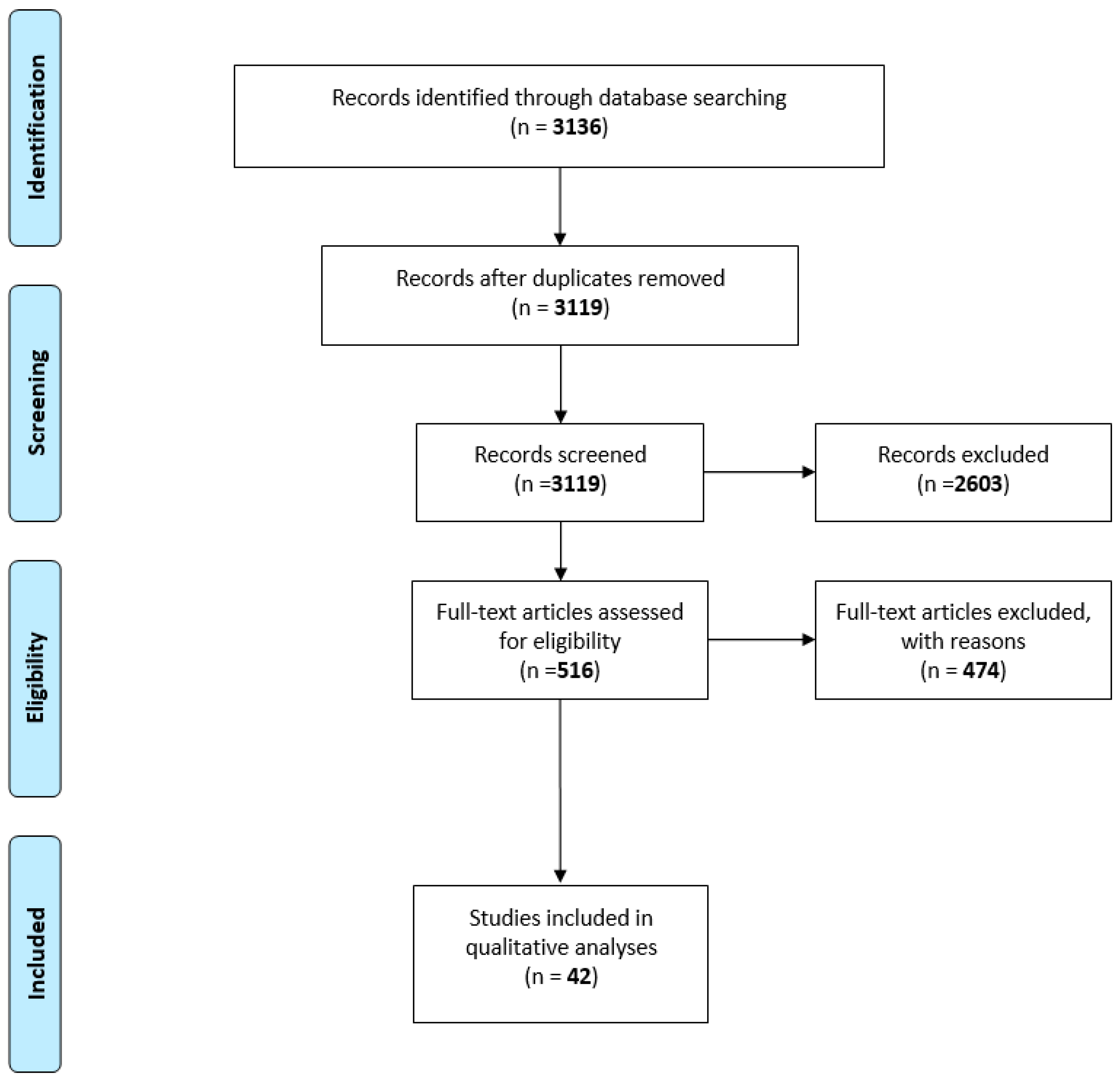
The scoping review followed a four-phase flow diagram (Figure 1) put forth by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [43]. The methodology used in this review is based on the Arksey and O’Malley framework [44], which includes the following stages: identifying the research question, identifying relevant studies, study selection, charting the data, and collating, summarizing, and reporting the results.
2.1. Context
This scoping review included all studies conducted in various healthcare settings, such as acute care, long-term care, or sport medicine clinics, as well as studies conducted in laboratory settings for clinical research purposes (typically randomized controlled trial). Studies written in English and published in any country will be eligible for inclusion.
2.2. Type of Studies
The study types included in this scoping review are randomized controlled trials, quasi-experimental, case study, systematic review, meta-analysis, prospective cohort study. Alternative study designs were considered based on study quality.
2.3. Concept
The technology-assisted interventions examined in this scoping review are various (e.g., robotic device, brain-computer interface, virtual reality, haptic technology) applied to treating patients of any age undergoing hand rehabilitation after stroke. Interventions should target training, specifically the transport of the arm and/or manipulation of an object. Studies that explore the effects of technology-assisted therapy for the upper limb, involving hand and fingers, were included. The primary outcome of interest to be included was the motor and/or functional recovery of the paretic upper limb focusing on hand/fingers motion. Manuscripts reporting on interventions that did not involve haptic technology were excluded. Additionally, articles that focused on validating haptic technology from a technical standpoint or in laboratory conditions with healthy participants were excluded.
2.4. Search Strategy
The search was completed by a professional librarian (C.C.) using a blend of standardized vocabulary and keywords derived from relevant systematic reviews covering the different concepts included in the search [45,46,47,48] (Appendix A). The search strategy was peer reviewed by another librarian, using the PRESS standard [49].
2.5. Databases
The preliminary search was completed in Medline (OVID) and then translated for Embase (OVID), CINAHL (EbscoHost), Cochrane Library, Scopus and Web of Science.
3. Results
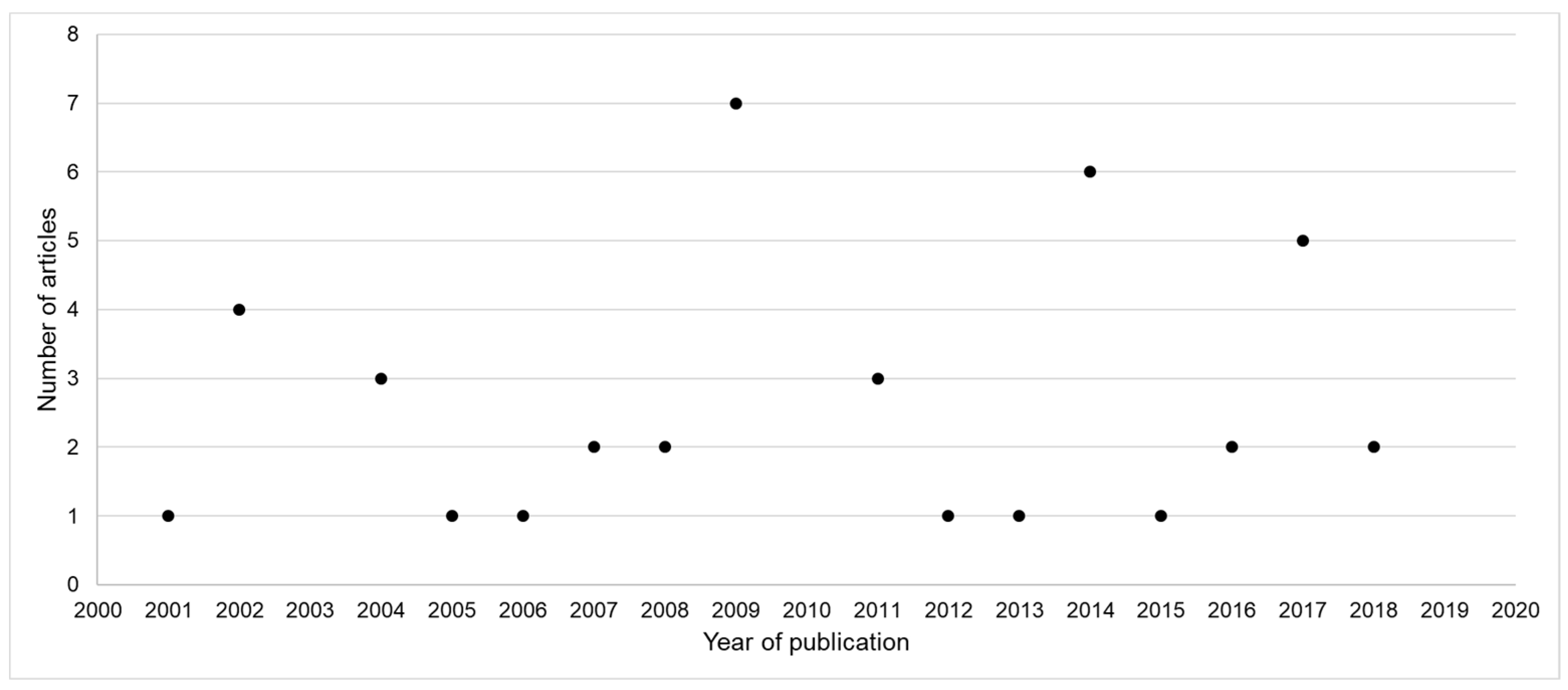
A total of 3136 results were generated from the literature search. After removing duplicates and screening titles and abstracts, full-text articles for 516 articles were retrieved. Those reported on the use of technology to support hand therapy intervention targeting the motor and functional recovery, without necessarily mentioning technology types in the title and/or abstract. Of those, 42 peer-reviewed articles involved the use of haptic technology in particular to support the hand therapy intervention and were included in the study. Articles were published between 2001 and 2018 with an average of 2.6 (±1.8) articles per year (Figure 2). Of the articles, 61% were published in the USA (26 articles). Three articles were published in Sweden, two in Taiwan, China and Italy, and one article in Australia, Canada, Netherlands, Russia and the United Kingdom.
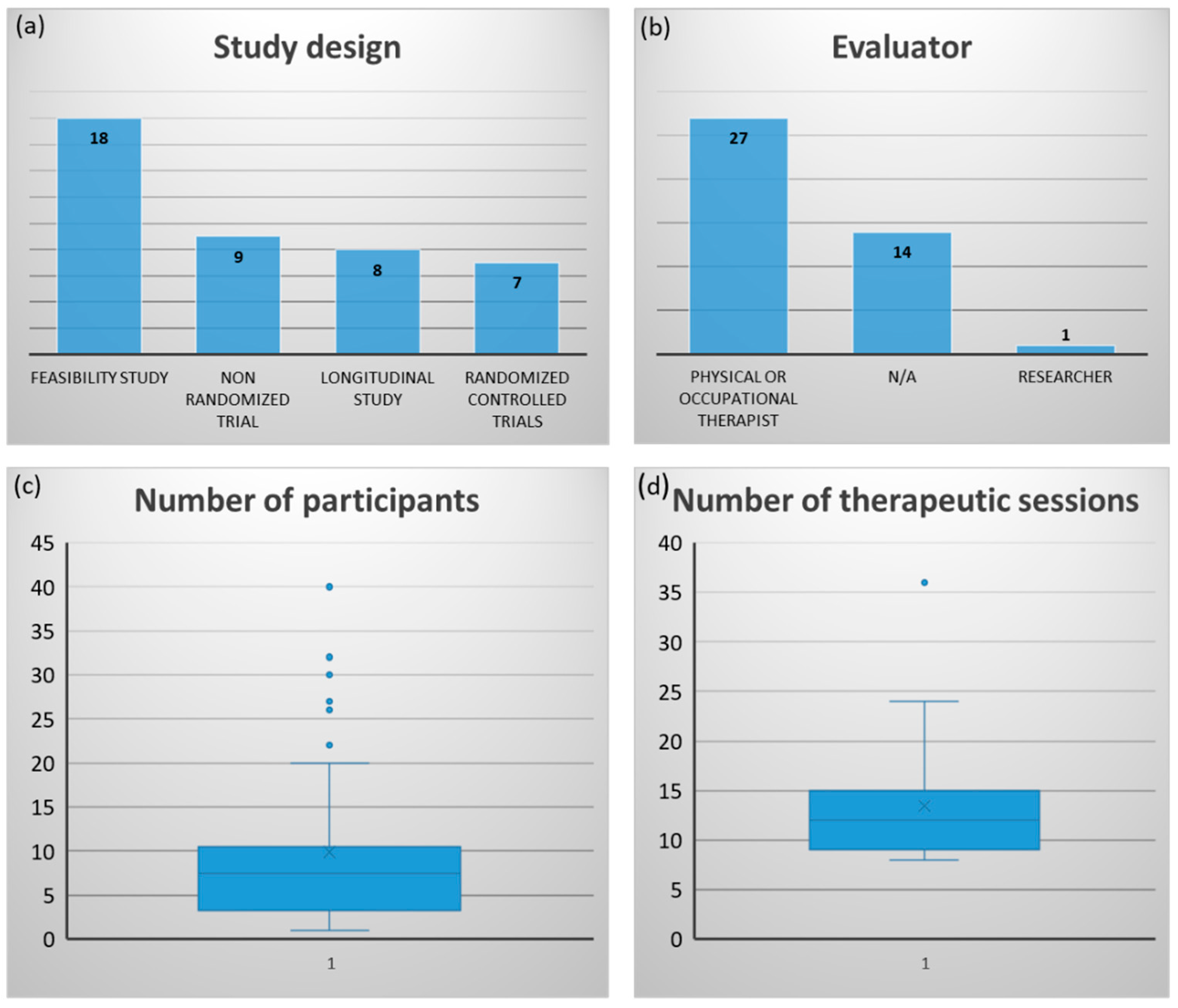
Figure 3 represents the characteristics of the studies reported in the 42 included articles. Of the articles, 43% (n = 18) were feasibility studies followed by non-randomized trials (21.4%), longitudinal studies (19%) and randomized controlled trials (17%) (Figure 3a). Most of the studies (64%) were carried out by occupational therapists or physiotherapists (Figure 3b). Many studies have not reported explicitly the profession of the person who is responsible for the therapy and the evaluations. The studies involved an average of 9.9 participants (±9.51), ranging from 1 to 40 participants. Figure 3c shows that the number of participants tends to be low in most studies with some outliers studies, including higher numbers such as 30 or 40 participants. The interventions included about 14.8 sessions (±8.8) ranging between 8 and 35 sessions. Figure 3d shows that the number of therapeutic sessions tends to be low in most studies.
3.1. Technology to Support Hand Rehabilitation
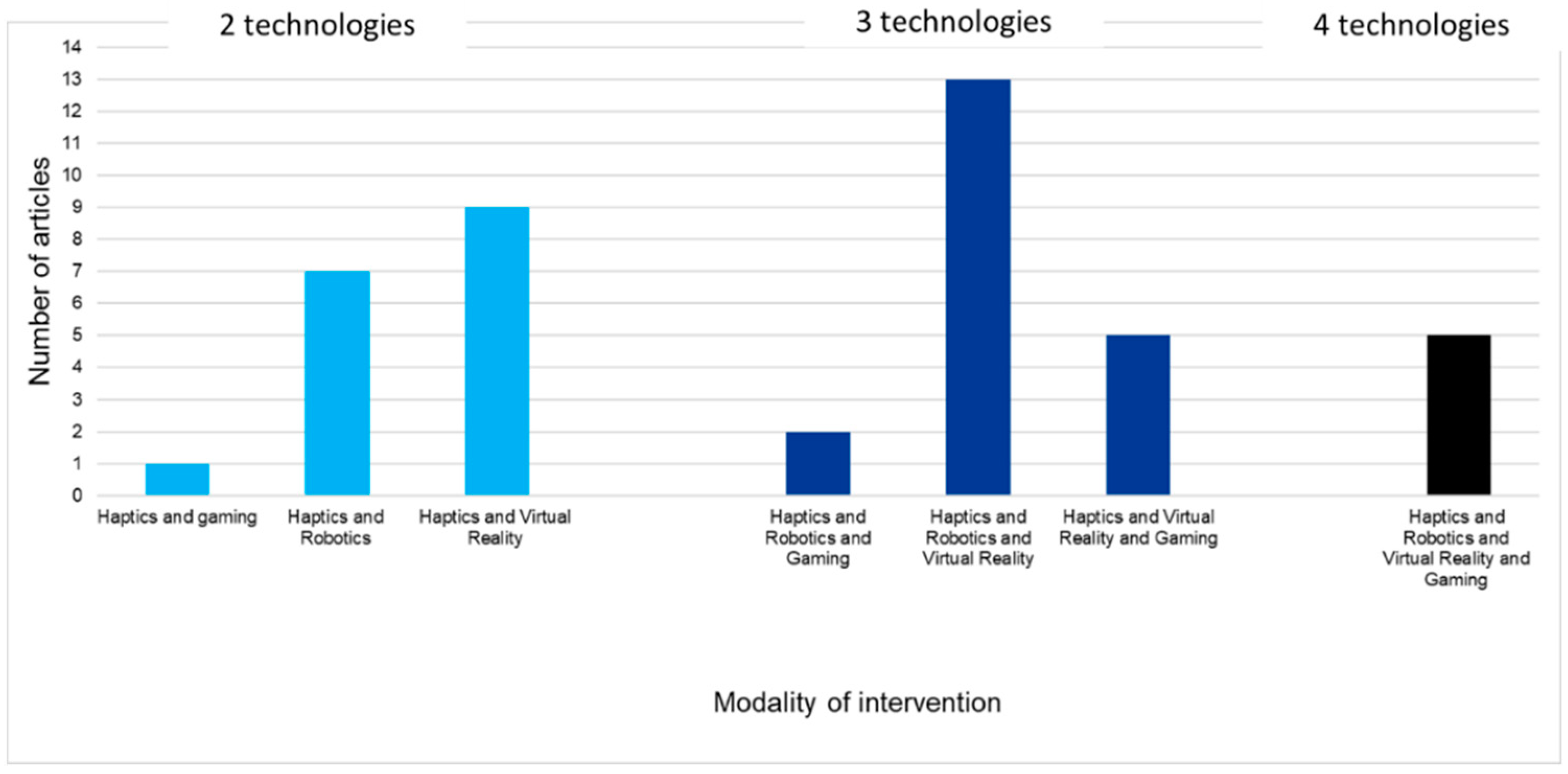
The articles related to haptics as targeted intervention modalities involved a combination of haptics associated with one to three other intervention modalities: robotics and/or virtual reality and/or gaming). Figure 4 shows the modalities of interventions classified by the number of technologies involved, namely two technologies or three or four. The combination of haptics with robotics and virtual reality was the most represented combination of intervention modalities to support hand rehabilitation (13 articles), followed by haptics and virtual reality (9 articles) and haptics and robotics (7 articles) (Figure 4). The interventions included in the 42 articles are described in Table 1.
3.2. Outcomes
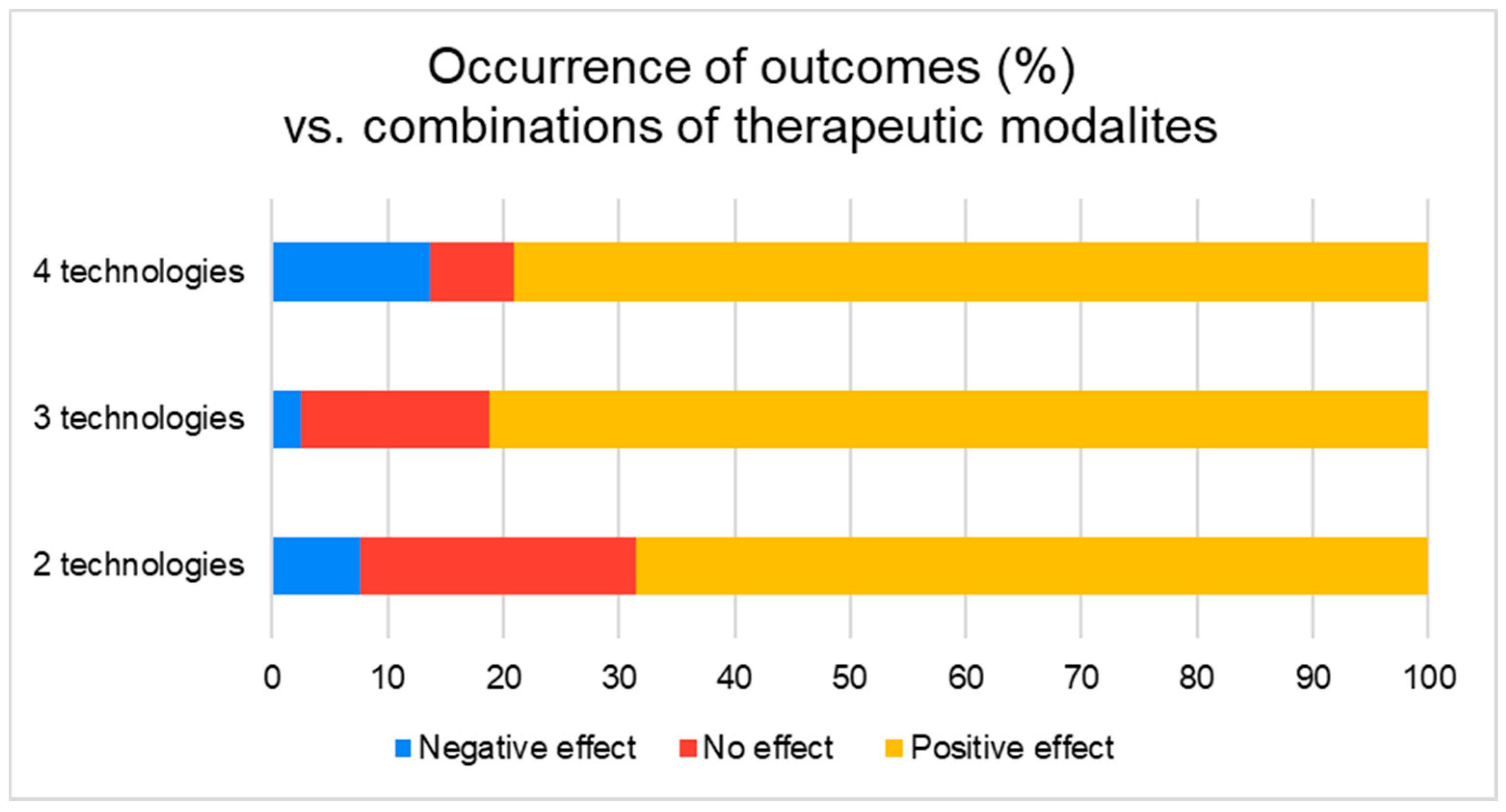
We evaluated the clinical outcomes from the included articles. Two reviewers evaluated the outcomes and classified them into three categories of effect: “negative effect”, “no effect” and “positive effect”. Positive and negative effects as defined in this section refer to a trend in the outcomes or significant results, meaning that, for example, tendencies to positive results and presence of significant results were both considered “positive effect” and vice-versa. Figure 5 shows the repartition of effects according to each modality of interventions calculated as a number of occurrences of every outcome throughout the articles. Interventions involving three technologies (47%, 20 articles) tend to show more positive effects and less negative effects than the other combinations.
3.3. Outcome Classification
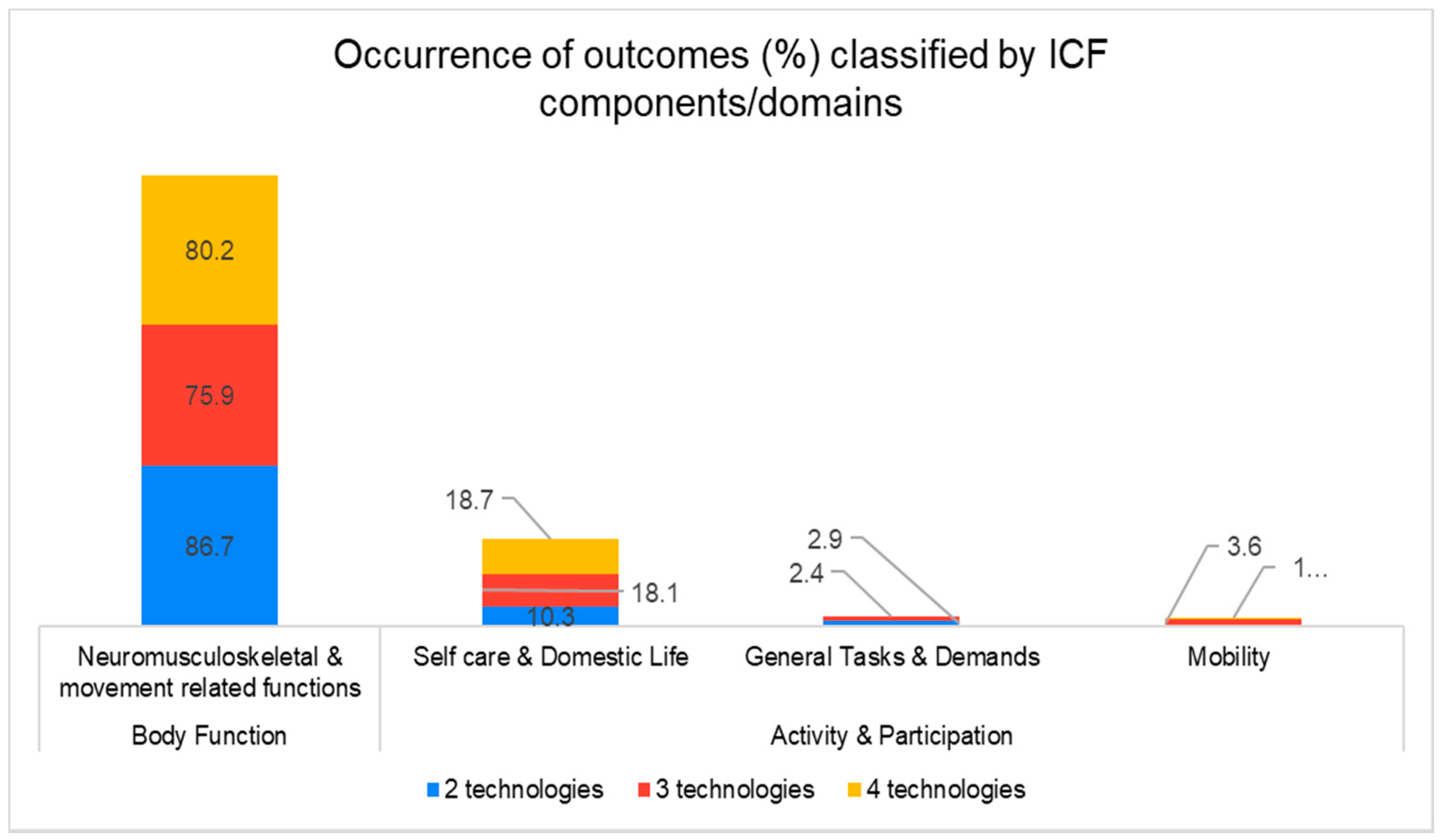
We classified the outcomes according to the International Classification of Functioning, Disability and Health (ICF) to portray health aspects evaluated in the retrieved articles. Outcomes mainly matched two ICF components, “body function” and “Activity and Participation”. Figure 6 illustrates the representations of ICF components and domains according to each combination of intervention modalities. “Body function” is the most represented ICF component with almost the same repartition over the three combinations of intervention modalities (in percentage).
3.4. User’s Perspective
Eight articles had investigated user perspective using a total of eight questionnaires and two evaluation scales. Six articles mentioned perception of motor function based on questionnaires. Ease of use, comfort, satisfaction, interest, motivation, and perception of results was mentioned once through questionnaires. None of the papers included users’ feedback on safety when using haptics.
4. Discussion
This paper aimed to (i) portray existing haptic-enabled hand rehabilitation in stroke patients, (ii) to map the use of haptic technology to support technology-assisted therapeutic interventions, and (iii) to investigate the effects of haptic-enabled interventions on motor and functional recovery in patients with stroke. The results revealed that literature on the topics is recent, small and sparse, as shown in Figure 2 and Figure 3. The literature on the use of haptics as a technology to support hand therapy spanned over the two last decades, and articles are published first in North America than in Europe and Asia. Most of the studies involved a low number of participants and may include methodological biases as only 17% of the studies were randomized controlled trials. Lack of randomized clinical trials involved the last trend in health technologies is expected as, historically, most of the innovations are evaluated as part proof-of-concept and feasibility studies involving a tiny group of participants. The successful technologies get marketed speedily, and the conduction of randomized controlled trials may be expensive and complicated to run in some legislations. Developers may lean toward trusting real-world evidence elaborated throughout the post-commercialization phase rather than waiting for randomized controlled trial outcomes. Haptics is a technology that is increasingly integrated into hand rehabilitation, and it is used in combinations with up to three technologies: robotics and/or virtual reality and/or gaming. Robots are a technology that helps stroke patients move their limbs during practice so that clinicians save time and effort when treating patients and increasing the amount of therapy for each patient [77,78]. Virtual reality is a technology used successfully with stroke patients and other conditions such as Parkinson’s disease [79] to create an interactive virtual world to fully immerse the patient in sensory and virtual feedback environments [80]. Virtual reality has been recommended to improve upper limb rehabilitation as an alternative that is more motivational and cost-effective than traditional care, mainly used for stroke patients. However, this field of investigation requires more research in terms of feasibility and usefulness in the telerehabilitation model with other neurological conditions [80,81]. Video games or console-based therapy are also used in rehabilitation, and its introduction offers results comparable to conventional therapy [82]. Haptic technology is a technology used to emulate the sense of touch by applying forces to the user and provide kinesthetic and tactile stimulation. Haptics can be used in virtual reality, augmented reality, rehabilitation robots and exoskeletons [83] to enhance the patient experience. Studies have shown that haptic technologies’ sense of touch is essential for dexterity and manipulating objects involving fine motor skills, which could not be stimulated without haptic devices [40,41]. This review explored the effect of using haptics in combination with different technologies on hand rehabilitation outcomes hypothesizing that the more different technologies are combined with the haptics, the better the therapeutic outcomes. This review revealed that using three or four different technologies showed more positive outcomes than using two technologies (only one technology + haptic device/component). In particular, when normalized in the percentage of outcomes, combining three technologies presented more positive rehabilitation outcomes and less negative outcomes than combining haptics with one other technology or with three other technologies. The most cited combinations of three technologies identified in this study were “robotics and virtual reality and haptics” represented by 13 studies representing 32% of the studies. This combination appears to best fulfill the rehabilitation needs as the robotic part enables strengthening the hand and upper limb. Virtual reality helps reproduce and practice the mental image of the task to be performed and the haptic biofeedback improves dexterity and fine motor skills retraining [55,56,57,58,59,60,61,62,63,64,65,66].
Most of the studies reported on body functions (80% of the outcomes) compared to the other health domains, such as activity and participation as defined by the ICF framework, meaning that most interventions focused on hand functions without necessarily involving and evaluating the patient in meaningful daily tasks and occupations. This clinical direction would have to do with potential technical challenges. While it is expected that there will be endless possibilities for virtual environments, it is also likely that the provision of biofeedback in simulated daily tasks is a complex development. This complexity could be explained by the emergence of the use of haptics in hand therapy. The use of haptics to provide a patient with biofeedback is more developed in the rehabilitation of the arms [84,85,86,87,88]. Surprisingly, none of the articles included involved telerehabilitation as a model of rehabilitation. Although home-based telerehabilitation is an emerging trend [89] that has been shown to be needed in pandemic times, home-based telerehabilitation targeting hand therapy appears to be uncovered by research and development. Barriers to technology-enabled telerehabilitation services for hand therapy include the weakness of the patient’s impaired upper limb and the complexity of applying a targeted passive range of motion tasks to patients who are not trained in the medical field (e.g., stretching impaired fingers with the unimpaired hand). Further research in this direction is needed to provide the general public with user-friendly and clinically approved digital platforms. Haptic devices have the potential to be implemented in the future as a diagnostic telerehabilitation tool used during clinical examination especially in palpation and special tests since in today’s age this action is not possible [90]. This futuristic feature could help conduct a thorough patient assessment without the need for face-to-face visits and decrease by the same fact the cost and effort for both the clinician and patient. The inclusion of haptic-supported virtual examination could be an interesting solution for providing telerehabilitation in complex contexts, such as for patients living in rural, remote or underserved communities, or during pandemics (e.g., the COVID-19).
User’s perspectives on the use of haptic technology in hand rehabilitation need to be addressed in future research. This scoping review revealed that there was no information on how haptics specifically affected the patient–robot interaction as well as engagement in the practice and adherence to the therapy. Clinicians’ perspectives on using haptic technology in hand rehabilitation and how it impacted their practice were not addressed either. Haptic technology can emit high force outputs, and users may suffer from decreased motor and functional levels allowing them to counteract this external mechanical stress. This risk of mechanical stress is worthy of exploration through continuous verbal questions throughout the therapy or the use of self-perceived scales (e.g., comfort, pain). Therefore, including user perspective in technology-enabled hand rehabilitation research is critical in promoting user-centred approaches to technology development and exploring novel therapeutic approaches. In the absence of validated questionnaires and consistent methodologies, it is recommended to integrate qualitative or mixed methods into the clinical trials to gather patients’ and clinical views on their experience with the technology deployed as part of the therapy.
5. Limitations
This study explored the literature that included clinical outcomes related to haptic-enabled hand rehabilitation, which is limited in terms of finding technologies per se. Technologies that are published in technical journals or any other academic report or grey literature have not been included in the current study. This means that the included studies did not cover potential haptic-enabling technologies targeting hand rehabilitation that did not undergo clinical studies or tested on humans to validate clinical relevance. This paper aimed to present the technologies that are already available on the market or are more likely to be available, and that underwent clinical studies.
6. Conclusions
This study identified and presented haptic-enabled rehabilitation approaches that could help therapists decide which technology-enabled hand therapy approach is best suited to their needs. Results have shown that combining three technologies, such as robotics and virtual reality and haptics, has produced better results than when only two technologies are combined. The use of four technologies did not necessarily show better results. Further research is encouraged to explore the provision of haptic biofeedback for complex daily tasks, such as simulated cooking tasks or actual keyboard typing.
Author Contributions
M.-A.C. has initiated the ideas of this study. M.-A.C. and C.C. have made substantial contributions to the conception and design of the study. S.M., J.B.H. and M.-A.C. have handled the screening and data extraction processes. M.-A.C. drafted the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This project and the APC are supported by M.-A.C.’s start-up funds, provided by the College of Rehabilitation Science, University of Manitoba.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors thank Janet Rothney, MLIS (Neil John Maclean Health Sciences Library, University of Manitoba) for peer review of the MEDLINE search strategy.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
CINAHL: Cumulated Index to Nursing and Allied Health Literature; PRISMA: Preferred reporting items for systematic reviews and meta-analyses.
Appendix A
Search strategy
- Robotics/
- Exoskeleton device/
- Man-Machine Systems/
- Orthotic Devices/
- Self-Help Devices/
- Automation/
- Therapy, Computer-Assisted/
- (electromechanical or “electro mechanical” or mechanical or mechanised or mechanized or driven or “assistive device*”).tw,kw.
- (robot* or automat* or “computer aided” or “computer assisted” or “power assist*”).tw,kw.
- (orthos* or orthotic*).tw,kw.
- or/1–10 [Robotic Concept]
- Computer Simulation/
- software/
- Mobile Applications/
- Video Games/
- Computers/
- exp Microcomputers/
- exp Cell Phones/
- Games, Experimental/
- (“virtual realit*” or VR).tw,kw.
- simulat*.tw,kw.
- ((interactiv* or virtual) adj2 technolog*).tw,kw.
- “augmented realit*”.tw,kw.
- (smartphone* or “smart-phone*”).tw,kw.
- ((mobile or cell or smart) adj2 phone*).tw,kw.
- (iphone* or android* or ipad*).tw,kw.
- (“personal digital assistant*” or “handheld computer*” or “handheld device*”).tw,kw.
- (“mobile app” or “mobile application”).tw,kw.
- (“serious game*” or “serious gaming”).tw,kw.
- or/12–29 [Virtual Reality Concept]
- Wearable Electronic Devices/
- Touch/
- exp Touch Perception/
- haptic*.tw,kw.
- biofeedback.tw,kw.
- (tactile or tactual).tw,kw.
- ((force or tactile or touch) adj2 (feedback or perception)).tw,kw.
- “sensory substitution”.tw,kw.
- (“electro-tactile” or “electro tactile” or electrotactile).tw,kw.
- (“electro-vibration” or “electro vibration” or electrovibration).tw,kw.
- ((vibrat* or servo or stepper) adj2 (motor or motors)).tw,kw.
- “wire actuator*”.tw,kw.
- piezoelectric*.tw,kw.
- pneumatic*.tw,kw.
- “shape memory alloy*”.tw,kw.
- solenoid*.tw,kw.
- “electro-active polymer*”.tw,kw.
- electrode*.tw,kw.
- (vibrotactile or vibration).tw,kw.
- wearable*.tw,kw.
- or/31–50 [Haptic Concept]
- (technolog* adj2 assist*).tw,kw.
- or/11,30,51–52 [Technological assistance concept]
- Hand/
- wrist/
- (hand* or wrist* or finger* or thumb*).tw,kw.
- or/54–56 [Hand Concept]
- exp cerebrovascular disorders/ or brain injury, chronic/
- (stroke* or cva or poststroke or “post stroke”).tw,kw.
- (cerebrovasc* or cerebral vascular).tw,kw.
- (cerebral or cerebellar or brain* or vertebrobasilar).tw,kw.
- (infarct* or isch?emi* or thrombo$ or emboli* or apoplexy).tw,kw.
- and/61–62
- (cerebral or brain or subarachnoid).tw,kw.
- (haemorrhage or hemorrhage or haematoma or hematoma or bleed*).tw,kw.
- and/64–65
- hemiplegia/ or exp paresis/
- (hempar* or hemipleg* or brain injur*).tw,kw.
- or/58–60,63,66–68 [Stroke Concept]
- and/53,57,69
- (rehabilitat* or rehab or “occupational therap*” or physiotherap* or “physical therap*”).tw,kw.
- exp Physical Therapy Modalities/
- exp Occupational Therapy/
- or/71–73 [Rehabilitation Concept]
- 70 and 74
References
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2014, 383, 245–255. [Google Scholar] [CrossRef]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global Burden of Stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef]
- Krueger, H.; Koot, J.; Hall, R.E.; O’Callaghan, C.; Bayley, M.; Corbett, D. Prevalence of Individuals Experiencing the Effects of Stroke in Canada: Trends and Projections. Stroke 2015, 46, 2226–2231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatem, S.M.; Saussez, G.; Della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of Motor Function after Stroke: A Multiple Systematic Review Focused on Techniques to Stimulate Upper Extremity Recovery. Front. Hum. Neurosci. 2016, 10, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, S.-M.; Studenski, S.; Duncan, P.W.; Perera, S. Persisting Consequences of Stroke Measured by the Stroke Impact Scale. Stroke 2002, 33, 1840–1844. [Google Scholar] [CrossRef] [Green Version]
- Parker, V.M.; Wade, D.T.; Hewer, R.L. Loss of arm function after stroke: Measurement, frequency, and recovery. Int. Rehabil. Med. 1986, 8, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Wade, D.T.; Langton-Hewer, R.; Wood, V.A.; Skilbeck, C.E.; Ismail, H.M. The hemiplegic arm after stroke: Measurement and recovery. J. Neurol. Neurosurg. Psychiatry 1983, 46, 521–524. [Google Scholar] [CrossRef] [Green Version]
- LeWinn, E.B. Physiological Factors in Childhood Epilepsy. Epilepsia 1980, 21, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Rugnetta, M. “Neuroplasticity”. Encyclopedia Britannica. 3 September 2020. Available online: https://www.britannica.com/science/neuroplasticity (accessed on 16 April 2021).
- Kwakkel, G. Impact of intensity of practice after stroke: Issues for consideration. Disabil. Rehabil. 2006, 28, 823–830. [Google Scholar] [CrossRef]
- Wolf, S.L.; Winstein, C.J.; Miller, J.P.; Taub, E.; Uswatte, G.; Morris, D.; Giuliani, C.; Light, K.E.; Nichols-Larsen, D. EXCITE Investigators. Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke: The EXCITE randomized clinical trial. JAMA 2006, 296, 2095–2104. [Google Scholar] [CrossRef]
- Bear-Lehman, J.; Bassile, C.C.; Gillen, G. A Comparison of Time Use on an Acute Rehabilitation Unit: Subjects with and without a Stroke. Phys. Occup. Ther. Geriatr. 2001, 20, 17–27. [Google Scholar] [CrossRef]
- Bernhardt, J.; Dewey, H.; Thrift, A.; Donnan, G. Inactive and alone: Physical activity within the first 14 days of acute stroke unit care. Stroke 2004, 35, 1005–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, E.M.; Nelson, D.L.; Bush, M.A. Comparison of Performance in Materials-Based Occupation, Imagery-Based Occupation, and Rote Exercise in Nursing Home Residents. Am. J. Occup. Ther. 1992, 46, 607–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thielman, G.; Kaminski, T.; Gentile, A.M. Rehabilitation of Reaching After Stroke: Comparing 2 Training Protocols Utilizing Trunk Restraint. Neurorehabilit. Neural Repair 2008, 22, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Thielman, G.T.; Dean, C.M.; Gentile, A. Rehabilitation of reaching after stroke: Task-related training versus progressive resistive exercise. Arch. Phys. Med. Rehabil. 2004, 85, 1613–1618. [Google Scholar] [CrossRef] [PubMed]
- Ada, L.; Canning, C.G.; Carr, J.H.; Kilbreath, S.L.; Shepherd, R.B. Task-Specific Training of Reaching and Manipulation. In Advances in Psychology; Bennett, K.M.B., Castiello, U., Eds.; Elsevier: North-Holland, The Netherlands, 1994; Volume 105, pp. 239–265. [Google Scholar]
- Michaelsen, S.M.; Dannenbaum, R.; Levin, M.F. Task-specific training with trunk restraint on arm recovery in stroke: Randomized control trial. Stroke 2006, 37, 186–192. [Google Scholar] [CrossRef] [Green Version]
- Bütefisch, C.; Hummelsheim, H.; Denzler, P.; Mauritz, K.-H. Repetitive training of isolated movements improves the outcome of motor rehabilitation of the centrally paretic hand. J. Neurol. Sci. 1995, 130, 59–68. [Google Scholar] [CrossRef]
- Logigian, M.K.; Samuels, M.A.; Falconer, J.; Zagar, R. Clinical exercise trial for stroke patients. Arch. Phys. Med. Rehabil. 1983, 64, 364–367. [Google Scholar]
- Wagenaar, R.C.; Meijer, O.G.; Van Wieringen, P.C.; Kuik, D.J.; Hazenberg, G.J.; Lindeboom, J.; Wichers, F.; Rijswijk, H. The functional recovery of stroke: A comparison between neuro-developmental treatment and the Brunnstrom method. Scand. J. Rehabil. Med. 1990, 22, 1–8. [Google Scholar] [PubMed]
- Wolf, S.L.; Lecraw, D.E.; Barton, L.A. Comparison of Motor Copy and Targeted Biofeedback Training Techniques for Restitution of Upper Extremity Function among Patients with Neurologic Disorders. Phys. Ther. 1989, 69, 719–735. [Google Scholar] [CrossRef]
- Guillot, A.; Collet, C. Construction of the Motor Imagery Integrative Model in Sport: A review and theoretical investigation of motor imagery use. Int. Rev. Sport. Exerc. Psychol. 2008, 1, 31–44. [Google Scholar] [CrossRef]
- Watt, A.P.; Morris, T.; Andersen, M.B. Development and validation of the sport imagery ability measure. Vic. Univ. Technol. 2003, 28, 149–180. [Google Scholar]
- Nilsen, D.M.; Gillen, G.; Gordon, A.M. Use of mental practice to improve upper-limb recovery after stroke: A systematic review. Am. J. Occup. Ther. 2010, 64, 695–708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brokaw, E.B.; Murray, T.M.; Nef, T.; Lum, P.S.; Nichols, D.; Holley, R.J. Time Independent Functional Task Training: A case study on the effect of inter-joint coordination driven haptic guidance in stroke therapy. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011. [Google Scholar] [CrossRef]
- Squeri, V.; Masia, L.; Giannoni, P.; Sandini, G.; Morasso, P. Wrist rehabilitation in chronic stroke patients by means of adaptive, progressive robot-aided therapy. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 312–325. [Google Scholar] [CrossRef] [PubMed]
- Timmermans, A.A.; Lemmens, R.J.; Monfrance, M.; Geers, R.P.; Bakx, W.; Smeets, R.J.; Seelen, H.A. Effects of task-oriented robot training on arm function, activity, and quality of life in chronic stroke patients: A randomized controlled trial. J. Neuroeng. Rehabil. 2014, 11, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdullah, H.A.; Tarry, C.; Lambert, C.; Barreca, S.; Allen, B.O. Results of Clinicians Using a Therapeutic Robotic System in an Inpatient Stroke Rehabilitation Unit. J. Neuroeng. Rehabil. 2011, 8, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.-C.; Liao, Y.-C.; Cheng, Y.-H.; Shih, P.-C.; Tsai, C.-M.; Lin, C.-Y. The potential effect of a vibrotactile glove rehabilitation system on motor recovery in chronic post-stroke hemiparesis. Technol. Health Care 2017, 25, 1183–1187. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Mukherjee, M.; Tsaur, Y.; Kim, S.; Liu, H.; Natarajan, P.; Agah, A. Development and feasibility study of a sensory-enhanced robot-aided motor training in stroke rehabilitation. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 5965–5968. [Google Scholar] [CrossRef]
- Mokienko, O.A.; Lyukmanov, R.K.; Chernikova, L.A.; Suponeva, N.A.; Piradov, M.A.; Frolov, A.A. Brain–computer interface: The first experience of clinical use in Russia. Hum. Physiol. 2016, 42, 24–31. [Google Scholar] [CrossRef]
- Connelly, L.; Stoykov, M.E.; Jia, Y.; Toro, M.L.; Kenyon, R.V.; Kamper, D.G. Use of a pneumatic glove for hand rehabilitation following stroke. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 2434–2437. [Google Scholar] [CrossRef]
- Deutsch, J.E.; Merians, A.S.; Burdea, G.C.; Boian, R.; Adamovich, S.V.; Poizner, H. Haptics and Virtual Reality Used to Increase Strength and Improve Function in Chronic Individuals Post-stroke: Two Case Reports. J. Neurol. Phys. Ther. 2002, 26, 79–86. [Google Scholar] [CrossRef]
- Tsoupikova, D.; Stoykov, N.S.; Corrigan, M.; Thielbar, K.; Vick, R.; Li, Y.; Triandafilou, K.; Preuss, F.; Kamper, D. Virtual immersion for post-stroke hand rehabilitation therapy. Ann. Biomed. Eng. 2015, 43, 467–477. [Google Scholar] [CrossRef]
- Deutsch, J.E.; Merians, A.S.; Adamovich, S.; Poizner, H.; Burdea, G.C. Development and application of virtual reality technology to improve hand use and gait of individuals post-stroke. Restor. Neurol. Neurosci. 2004, 22, 371–386. [Google Scholar]
- Reinkensmeyer, D.; Pang, C.; Nessler, J.; Painter, C. Web-based telerehabilitation for the upper extremity after stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2002, 10, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Acosta, A.M.; Dewald, H.A.; Dewald, J.P.A. Pilot study to test effectiveness of video game on reaching performance in stroke. J. Rehabil. Res. Dev. 2011, 48, 431–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merians, A.S.; Poizner, H.; Boian, R.; Burdea, G.; Adamovich, S. Sensorimotor training in a virtual reality environment: Does it improve functional recovery poststroke? Neurorehabil. Neural. Repair. 2006, 20, 252–267. [Google Scholar] [CrossRef]
- Jiang, L.; Cutkosky, M.; Ruutiainen, J.; Raisamo, R. Using Haptic Feedback to Improve Grasp Force Control in Multiple Sclerosis Patients. IEEE Trans. Robot. 2009, 25, 593–601. [Google Scholar] [CrossRef]
- Wan, A.H.; Wong, D.W.; Ma, C.Z.; Zhang, M.; Lee, W.C. Wearable Vibrotactile Biofeedback Device Allowing Identification of Different Floor Conditions for Lower-Limb Amputees. Arch. Phys. Med. Rehabil. 2016, 97, 1210–1213. [Google Scholar] [CrossRef] [Green Version]
- Stone, K.D.; Gonzalez, C.L.R. The contributions of vision and haptics to reaching and grasping. Front. Psychol. 2015, 6, 1403. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ Res. Method Rep. 2009, 339, 2700. [Google Scholar] [CrossRef] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Amirabdollahian, F.; Livatino, S.; Vahedi, B.; Gudipati, R.; Sheen, P.; Gawrie-Mohan, S.; Vasdev, N. Prevalence of haptic feedback in robot-mediated surgery: A systematic review of literature. J. Robot. Surg. 2017, 12, 11–25. [Google Scholar] [CrossRef] [Green Version]
- Mehrholz, J.; Thomas, S.; Werner, C.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, CD006185. [Google Scholar] [CrossRef]
- Saxena, N.; Kyaw, B.M.; Vseteckova, J.; Dev, P.; Paul, P.; Lim, K.T.K.; Kononowicz, A.A.; Masiello, I.; Car, L.T.; Nikolaou, C.K.; et al. Virtual reality environments for health professional education. Cochrane Database Syst. Rev. 2018, 2018, CD012090. [Google Scholar] [CrossRef]
- Williams, M.A.; Srikesavan, C.; Heine, P.J.; Bruce, J.; Brosseau, L.; Hoxey-Thomas, N.; Lamb, S.E. Exercise for rheumatoid arthritis of the hand. Cochrane Database Syst. Rev. 2018, CD003832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sampson, M.; McGowan, J.; Cogo, E.; Grimshaw, J.; Moher, D.; Lefebvre, C. An evidence-based practice guideline for the peer review of electronic search strategies. J. Clin. Epidemiol. 2009, 62, 944–952. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Boian, R.; Sharma, A.; Han, C.; Merians, A.; Burdea, G.; Adamovich, S.; Recce, M.; Tremaine, M.; Poizner, H. Virtual reality-based post-stroke hand rehabilitation. Stud. Health Technol. Inform. 2002, 85, 64–70. [Google Scholar]
- Broeren, J.; Claesson, L.; Goude, D.; Rydmark, M.; Sunnerhagen, K.S. Virtual Rehabilitation in an Activity Centre for Community-Dwelling Persons with Stroke. Cerebrovasc. Dis. 2008, 26, 289–296. [Google Scholar] [CrossRef]
- Yeh, S.-C.; Lee, S.-H.; Chan, R.-C.; Chen, S.; Rizzo, A. A virtual reality system integrated with robot-assisted haptics to simulate pinch-grip task: Motor ingredients for the assessment in chronic stroke. Neurorehabilitation 2014, 35, 435–449. [Google Scholar] [CrossRef]
- Turolla, A.; Albasini, O.A.D.; Oboe, R.; Agostini, M.; Tonin, P.; Paolucci, S.; Sandrini, G.; Venneri, A.; Piron, L. Haptic-Based Neurorehabilitation in Poststroke Patients: A Feasibility Prospective Multicentre Trial for Robotics Hand Rehabilitation. Comput. Math. Methods Med. 2013, 2013, 895492. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.-C.; Lee, S.-H.; Chan, R.-C.; Wu, Y.; Zheng, L.-R.; Flynn, S. The Efficacy of a Haptic-Enhanced Virtual Reality System for Precision Grasp Acquisition in Stroke Rehabilitation. J. Health Eng. 2017, 2017, 9840273. [Google Scholar] [CrossRef] [Green Version]
- Adamovich, S.; Fluet, G.G.; Merians, A.S.; Mathai, A.; Qiu, Q. Recovery of hand function in virtual reality: Training hemiparetic hand and arm together or separately. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 3475–3478. [Google Scholar] [CrossRef]
- Abdollahi, F.; Case Lazarro, E.D.; Listenberger, M.; Kenyon, R.V.; Kovic, M.; Bogey, R.A.; Hedeker, D.; Jovanovic, B.D.; Patton, J.L. Error augmentation enhancing arm recovery in individuals with chronic stroke: A randomized crossover design. Neurorehabil. Neural. Repair. 2014, 28, 120–128. [Google Scholar] [CrossRef]
- Adamovich, S.V.; Fluet, G.G.; Mathai, A.; Qiu, Q.; Lewis, J.; Merians, A.S. Design of a complex virtual reality simulation to train finger motion for persons with hemiparesis: A proof of concept study. J. Neuroeng. Rehabil. 2009, 6, 28. [Google Scholar] [CrossRef] [Green Version]
- Adamovich, S.V.; Fluet, G.G.; Merians, A.S.; Mathai, A.; Qiu, Q. Incorporating Haptic Effects Into Three-Dimensional Virtual Environments to Train the Hemiparetic Upper Extremity. IEEE Trans. Neural Syst. Rehabil. Eng. 2009, 17, 512–520. [Google Scholar] [CrossRef] [Green Version]
- Fluet, G.G.; Merians, A.S.; Qiu, Q.; Davidow, A.; Adamovich, S.V. Comparing integrated training of the hand and arm with isolated training of the same effectors in persons with stroke using haptically rendered virtual environments, a randomized clinical trial. J. Neuroeng. Rehabil. 2014, 11, 126. [Google Scholar] [CrossRef] [Green Version]
- Fluet, G.G.; Merians, A.S.; Qiu, Q.; Lafond, I.; Saleh, S.; Ruano, V.; Delmonico, A.R.; Adamovich, S.V. Robots integrated with virtual reality simulations for customized motor training in a person with upper extremity hemiparesis: A case study. J. Neurol. Phys. Ther. 2012, 36, 79–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fluet, G.; Merians, A.; Patel, J.; Wingerden, A.V.; Qiu, Q.; Yarossi, M.; Tunik, E.; Adamovich, S.; Massood, S. Virtual reality-augmented rehabilitation for patients in subacute phase post stroke: A feasibility study. J. Pain. Manag. 2016, 9, 227–234. [Google Scholar]
- Jack, D.; Boian, R.; Merians, A.; Tremaine, M.; Burdea, G.; Adamovich, S.; Recce, M.; Poizner, H. Virtual reality-enhanced stroke rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, R.C.V.; Harwin, W.S.; Lamperd, R.; Collin, C. Evaluation of Reach and Grasp Robot-Assisted Therapy Suggests Similar Functional Recovery Patterns on Proximal and Distal Arm Segments in Sub-Acute Hemiplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 22, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Maris, A.; Coninx, K.; Seelen, H.; Truyens, V.; De Weyer, T.; Geers, R.; Lemmens, M.; Coolen, J.; Stupar, S.; Lamers, I.; et al. The impact of robot-mediated adaptive I-TRAVLE training on impaired upper limb function in chronic stroke and multiple sclerosis. Disabil. Rehabil. Assist. Technol. 2018, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Q.; Fluet, G.G.; Lafond, I.; Merians, A.S.; Adamovich, S.V. Coordination changes demonstrated by subjects with hemiparesis performing hand-arm training using the NJIT-RAVR robotically assisted virtual rehabilitation system. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 1143–1146. [Google Scholar] [CrossRef] [Green Version]
- Rozario, S.V.; Housman, S.; Kovic, M.; Kenyon, R.V.; Patton, J.L. Therapist-mediated post-stroke rehabilitation using haptic/graphic error augmentation. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 1151–1156. [Google Scholar] [CrossRef]
- Rowe, J.B.; Chan, V.; Ingemanson, M.L.; Cramer, S.C.; Wolbrecht, E.T.; Reinkensmeyer, D.J. Robotic Assistance for Training Finger Movement Using a Hebbian Model: A Randomized Controlled Trial. Neurorehabilit. Neural Repair 2017, 31, 769–780. [Google Scholar] [CrossRef]
- Adamovich, S.; Merians, A.; Boian, R.; Tremaine, M.; Burdea, G.; Recce, M.; Poizner, H. A virtual reality based exercise system for hand rehabilitation post-stroke: Transfer to function. In Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004; pp. 4936–4939. [Google Scholar] [CrossRef]
- Broeren, J.; Rydmark, M.; Sunnerhagen, K.S. Virtual reality and haptics as a training device for movement rehabilitation after stroke: A single-case study. Arch. Phys. Med. Rehabil. 2004, 85, 1247–1250. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.C.; Yeh, S.-C.; Jung, Y.; Yoon, H.; Whitford, M.; Chen, S.-Y.; Li, L.; McLaughlin, M.; Rizzo, A.; Winstein, C.J. Intervention to enhance skilled arm and hand movements after stroke: A feasibility study using a new virtual reality system. J. Neuroeng. Rehabil. 2007, 4, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broeren, J.; Rydmark, M.; Björkdahl, A.; Sunnerhagen, K.S. Assessment and Training in a 3-Dimensional Virtual Environment with Haptics: A Report on 5 Cases of Motor Rehabilitation in the Chronic Stage after Stroke. Neurorehabilit. Neural Repair 2007, 21, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Naghdy, F.; Naghdy, G.; Du, H. Clinical effectiveness of combined virtual reality and robot assisted fine hand motion rehabilitation in subacute stroke patients. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 511–515. [Google Scholar] [CrossRef]
- Huang, X.; Naghdy, F.; Du, H.; Naghdy, G.; Murray, G. Design of adaptive control and virtual reality-based fine hand motion rehabilitation system and its effects in subacute stroke patients. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2017, 6, 678–686. [Google Scholar] [CrossRef]
- Merians, A.S.; Jack, D.; Boian, R.; Tremaine, M.; Burdea, G.C.; Adamovich, S.V.; Recce, M.; Poizner, H. Virtual Reality–Augmented Rehabilitation for Patients Following Stroke. Phys. Ther. 2002, 82, 898–915. [Google Scholar] [CrossRef] [Green Version]
- Merians, A.S.; Tunik, E.; Fluet, G.G.; Qiu, Q.; Adamovich, S.V. Innovative approaches to the rehabilitation of upper extremity hemiparesis using virtual environments. Eur. J. Phys. Rehabil. Med. 2009, 45, 123–133. [Google Scholar] [PubMed]
- Brewer, B.R.; McDowell, S.K.; Worthen-Chaudhari, L.C. Poststroke Upper Extremity Rehabilitation: A Review of Robotic Systems and Clinical Results. Top. Stroke Rehabil. 2007, 14, 22–44. [Google Scholar] [CrossRef]
- Zariffa, J.; Kapadia, N.; Kramer, J.L.K.; Taylor, P.; Alizadeh-Meghrazi, M.; Zivanovic, V.; Willms, R.; Townson, A.; Curt, A.; Popovic, M.R.; et al. Effect of a robotic rehabilitation device on upper limb function in a sub-acute cervical spinal cord injury population. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–5. [Google Scholar] [CrossRef]
- Eftekharsadat, B.; Babaei-Ghazani, A.; Mohammadzadeh, M.; Talebi, M.; Eslamian, F.; Azari, E. Effect of virtual reality-based balance training in multiple sclerosis. Neurol. Res. 2014, 37, 539–544. [Google Scholar] [CrossRef]
- Massetti, T.; Trevizan, I.L.; Arab, C.; Favero, F.M.; Ribeiro-Papa, D.C.; Monteiro, C.B.D.M. Virtual reality in multiple sclerosis—A systematic review. Mult. Scler. Relat. Disord. 2016, 8, 107–112. [Google Scholar] [CrossRef]
- Lozano-Quilis, J.-A.; Gil-Gómez, H.; Gil-Gómez, J.-A.; Albiol-Pérez, S.; Palacios-Navarro, G.; Fardoun, H.M.; Mashat, A.S. Virtual Rehabilitation for Multiple Sclerosis Using a Kinect-Based System: Randomized Controlled Trial. JMIR Serious Games 2014, 2, e12. [Google Scholar] [CrossRef]
- Bonnechère, B.; Jansen, B.; Omelina, L.L.; Jan, S.V.S. The use of commercial video games in rehabilitation: A systematic review. Int. J. Rehabil. Res. 2016, 39, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Piggott, L.; Wagner, S.; Ziat, M. Haptic Neurorehabilitation and Virtual Reality for Upper Limb Paralysis: A Review. Crit. Rev. Biomed. Eng. 2016, 44, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.A.; Risi, N.; Ballardini, G.; Mrotek, L.A.; Casadio, M.; Scheidt, R.A. Effect of Dual Tasking on Vibrotactile Feedback Guided Reaching—A Pilot Study. In International Conference on Human Haptic Sensing and Touch Enabled Computer Applications; Springer: Cham, Switzerland, 2018; pp. 3–14. [Google Scholar]
- Bark, K.; Wheeler, J.; Shull, P.; Savall, J.; Cutkosky, M. Rotational Skin Stretch Feedback: A Wearable Haptic Display for Motion. IEEE Trans. Haptics 2010, 3, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Huisman, G.; Frederiks, A.D.; van Erp, J.B.; Heylen, D.K. Simulating affective touch: Using a vibrotactile array to generate pleasant stroking sensations. In International Conference on Human Haptic Sensing and Touch Enabled Computer Applications; Springer: Cham, Switzerland, 2016; pp. 240–250. [Google Scholar]
- Risi, N.; Shah, V.; Mrotek, L.A.A.; Casadio, M.; Scheidt, R.A. Supplemental vibrotactile feedback of real-time limb position enhances precision of goal-directed reaching. J. Neurophysiol. 2019, 122, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Krueger, A.R.; Giannoni, P.; Shah, V.; Casadio, M.; Scheidt, R.A. Erratum to: Supplemental vibrotactile feedback control of stabilization and reaching actions of the arm using limb state and position error encodings. J. Neuroeng. Rehabil. 2017, 14, 69. [Google Scholar] [CrossRef] [Green Version]
- Handelzalts, S.; Ballardini, G.; Avraham, C.; Pagano, M.; Casadio, M.; Nisky, I. Integrating Tactile Feedback Technologies into Home-Based Telerehabilitation: Opportunities and Challenges in Light of COVID-19 Pandemic. Front. Neurorobot. 2021, 15, 617636. [Google Scholar] [CrossRef]
- Howard, I.M.; Kaufman, M.S. Telehealth applications for outpatients with neuromuscular or musculoskeletal disorders. Muscle Nerve 2018, 58, 475–485. [Google Scholar] [CrossRef]
Figure 1.
Study selection process [50].
Figure 1.
Study selection process [50].

Figure 2.
Frequency of publication per year.

Figure 3.
(a–d) Characteristics of the interventions reported in the included articles.

Figure 4.
Combinations of hand rehabilitation technologies.

Figure 5.
Outcomes according to number of technologies involved.

Figure 6.
Outcomes classified according to intervention modality and the ICF framework components and domain according to intervention modality.
Figure 6.
Outcomes classified according to intervention modality and the ICF framework components and domain according to intervention modality.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Portrait of the haptic enabled interventions retrieved in this scoping review. This table shows the technologies used in hand rehabilitation in combination with haptic technologies. Each row presents a study, and studies are classified by the number of technology involved in the intervention ranging from two to four technologies.
Table 1.
Portrait of the haptic enabled interventions retrieved in this scoping review. This table shows the technologies used in hand rehabilitation in combination with haptic technologies. Each row presents a study, and studies are classified by the number of technology involved in the intervention ranging from two to four technologies.
| Number of Technology | Combinations | Description | Ref ID |
|---|---|---|---|
| Two Technologies | Haptic and gaming | A system that can physically assist or resist the user in playing the therapy games. For example, in Breakout Therapy, the force feedback joystick physically assists in hand movement by predicting the trajectory of the ball after each rebound | [37] |
| Haptics and robotics | Special robot handle generating cutaneous sensory inputs for the middle and index fingers, the thumb, or the palm of the subject + InMotion2 robot | [31] | |
| Haptic system enabling classification of the signals for the real-time identification of a command; exoskeleton of a hand (robotic orthosis) + BCI system consisted of an EEG, encephalograph, and a personal computer | [32] | ||
| Haptic 3 DoF robot: a singly actuated 3 DoF device for assisting in reaching movements in three dimensions across the user’s workspace | [27] | ||
| Haptic Master to correct trajectory performance guided by extra proprioceptive feedback | [28] | ||
| A magnetic plate that is equipped with a force sensor that gauges how hard the fingers press + Vibrotactile glove system designed with light fabric for greater wearability, which is a finger training system in which users interact with the computer | [30] | ||
| An industrial robot (5 DoF desktop robot with position-based control) converted into a novel sensory system incorporating force feedback combined with a graphical interface | [29] | ||
| The ARMin III exoskeleton, which can apply torques directly to each of the 6 DOF of the arm (3 shoulder torques, elbow, flexion–extension, supination–pronation, wrist flexion–extension). The robot applies haptic walls that are exponentially related to each individual joint’s error from its ideal position | [26] | ||
| Haptics and VR | A CyberGlove and a Rutgers Master II (RMII) haptic glove. The two sensing gloves are integrated with VR exercises running on the PC host. RMII glove applies forces to help the patient open the hand before switching to the target of the exercise | [51] | |
| A semi-immersive workbench that uses stereographic shuttered glasses, a 3D image displayed above the tabletop was observed by the user. The system has also a haptic game selection menu | [52] | ||
| 2 PHANToM devices placed perpendicular to each other for the pinch movement and reconfigured to provide hepatic feedback for the pinch task. Haptic feedback was provided for the thumb and index finger, so that the participants felt they were lifting a real cube with mass | [53] | ||
| The PneuGlove used in conjunction with a VR environment (the virtual hand is controlled by the user, who attempts to open the hand sufficiently to grasp the objects displayed), to provide haptic feedback in addition to the assistance of finger extension | [33] | ||
| Four VR hand exercises developed using the WorldToolKit graphics library. Rutgers Master II glove, a compact haptic interface, was used to apply force to the user’s fingertips. It uses non-contact position sensors to measure the fingertip position in relation to the palm | [34] | ||
| VR environments designed for impairment and task-specific training using discrete tasks. Augmented feedback was provided in the form of sensory feedback using haptic cues | [36] | ||
| An immersive VR environment based on the classic story of Alice in Wonderland + The PneuGlove system provides pneumatic assistance to digit extension to help with hand opening or resistance to finger flexion to provide haptic feedback | [35] | ||
| Visual and haptic feedbacks were implemented using the Handshake proSENSE Toolbox. The haptic device is focused on a single finger haptic display, in which the force is exerted at the fingertip. | [54] | ||
| VR tasks were formulated to ensure that pinch movements were required to complete each task and that the patients experienced finger strengthening. Here, 2 Novint Falcon devices operated in coordination to simulate the haptic perceptions of 2 fingertips (perceived the reaction force of the surface and/or the weight of the box). | [55] | ||
| Three Technologies | Haptics, Robotics and VR | CyberGlove Haptic MASTER, a 3 DoF, admittance controlled (force-controlled) robot + Simulations for the hand alone, the arm alone, and the hand and arm together using Virtools software package with the VRPack plug-in + haptic guidance of arm movement in 3D space that is adaptive in real-time as well as on a trial-by-trial basis | [56] |
| PHANTOM robot and the WREX swiveling wrist support + Virtual Reality Robotic and Optical Operations Machine (VRROOM) + Forces only applied by the robot during the Error Augmentation treatment phase | [57] | ||
| CyberGrasp, an exoskeleton device placed on the dorsum of the hand which allows for multiplane arm motion while exerting an extensor force on each individual finger + the virtual piano trainer + CyberGrasp, a force-reflecting exoskeleton that fits over a CyberGlove data glove | [58] | ||
| Haptic Master, a 3 DoF admittance controlled (force-controlled) robot + A haptic system with force feedback available only for pronation/supination + VR environments enabling multiplane movements against gravity in a 3D workspace | [59] | ||
| Haptic MASTER + using Virtools software package with the VRPack plug-in + CyberGrasp to facilitate individual finger movement by resisting flexion of the adjacent fingers in patients with more pronounced deficits allowing for individual movement of each finger. | [56] | ||
| NJIT RAVR system consists of CyberGlove combined with the Haptic Master + Virtual piano trainer + the robotic arm provides tracking of multiplane movements against gravity in a 3D workspace | [60] | ||
| NJIT-RAVR system using a CyberGlove and a Haptic Master + NJIT Track0Glove system + VR simulations for customized motor training | [61] | ||
| NJIT RAVR System including Haptic Master to produce haptic effects, such as spring, damper and constant force and to create haptic objects like blocks, cylinders and spheres as well as walls, floors, ramps and complex surfaces + A suite of simulations for training shoulder, elbow, wrist and finger movements using the Virtools software package | [62] | ||
| RMII glove is an exoskeleton device that applies force to the user’s fingertips and uses noncontact position sensors to measure the fingertip position in relation to the palm + the CyberGlove, a sensorized structure worn on the hand + VR simulations consist of four exercises: range, speed, fractionation, and strength | [63] | ||
| Haptic Master robot coupled to the Grasp Assistance robot—via a 3 passive DoF gimbal + interactive virtual worlds (e.g., cleaning the table) + haptic feedback when touching the object | [64] | ||
| Haptic Master that can move in the virtual learning environment by means of an avatar that is shown on the screen + haptic feedback can be provided to either support or challenge the participants | [65] | ||
| Haptic Master’s to program the robot to produce haptic objects + VR gaming simulations that translates movement of both the upper arm and the hand | [66] | ||
| A 6 DoF PHANTOM Premium 3.0 robot + a haptics/graphics display combining a projected stereo, head-tracked rendering on a semi-silvered mirror overlay display with a robotic system that can record wrist position, track movements and generate force feedback + A cinema-quality digital projector combined with LCD shutter glasses | [67] | ||
| Haptics, Robotics and Gaming | Arm Coordination Training 3D system providing a haptic interface to simulate various loading conditions while subjects performed arm reaching movements with avatar and game feedback + haptic feedback consisting of a simulated viscous environment that prevented subjects from moving on the haptic table + Air Hockey 3D game | [38] | |
| FINGER robotic exoskeleton providing 2 levels of assistance + Musical computer game in the style of Guitar Hero | [68] | ||
| Haptics, VR and Gaming | Four hand exercises simulations developed with WorldToolKit (Sense 8) + Rutgers Master II-ND (RMII) force feedback glove prototype + Simple games that provided frequent feedback about the success of the action as well as the quality of the performance to encourage participation and concentration | [69] | |
| Four hand exercises simulations developed with WorldToolKit (Sense 8) + RMII glove has a dedicated electropneumatic control interface to provide force feedback to the patient’s fingers + simple video games developed with WorldToolKit (Sense8) graphics library | [69] | ||
| PHANToM haptic device + Reachin 3.0. Reachin API, a 3D model programming (haptic interface) + grasping and reaching game. | [70] | ||
| 4 hand exercise simulations developed with the WorldTool Kit graphics library + Rutgers Master II-ND (RMII), a force feedback prototype glove + games designed to exercise one parameter of finger movement at a time | [39] | ||
| PHANToM devices + tasks displayed using a desktop personal computer and shutter glasses (StereoGraphics) to provide a three-dimensional view of stimuli + Reaching, Ball Shooting, Rotation and Pinch games | [71] | ||
| Four Technologies | Haptics, Robotics, VR and Gaming | A desk-mounted robot + a haptic stylus. + a semi-immersive workbench + 3D Bricks game | [72] |
| Amadeo, A 5 DoF hand rehabilitation robotic device named + incorporated Real-time force and position signals + highly repetitive functional VR tasks + Flying bird and Spaceship games | [73] | ||
| Amadeo, A 5 DoF hand rehabilitation robotic device named + 2D, one 3D VR-based RGS and a 2D transferring virtual environment + Flying bird | [74] | ||
| CyberGlove + haptic (force), visual and auditory feedback + 3D graphics were displayed on a flat personal computer screen using only shadows and perspective cues to give the illusion of depth. + computer games using graphics feedback to encourage participation and concentration | [75] | ||
| Haptic Master + 3 more DoF can be added to the arm by using a gimbal, with force feedback available only pronation/supination + Stimulated unimanual “virtual mirror” + Piano Trainer, Space Pong, Plasma pong, bird hunt and Hammer games | [76] |
VR: virtual reality; DoF: Degree of Freedom.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Choukou, M.-A.; Mbabaali, S.; Bani Hani, J.; Cooke, C. Haptic-Enabled Hand Rehabilitation in Stroke Patients: A Scoping Review. Appl. Sci. 2021, 11, 3712. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083712
AMA Style
Choukou M-A, Mbabaali S, Bani Hani J, Cooke C. Haptic-Enabled Hand Rehabilitation in Stroke Patients: A Scoping Review. Applied Sciences. 2021; 11(8):3712. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083712
Chicago/Turabian StyleChoukou, Mohamed-Amine, Sophia Mbabaali, Jasem Bani Hani, and Carol Cooke. 2021. "Haptic-Enabled Hand Rehabilitation in Stroke Patients: A Scoping Review" Applied Sciences 11, no. 8: 3712. https://0-doi-org.brum.beds.ac.uk/10.3390/app11083712
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.