
Influencing Factors in Autotransplantation of Teeth with Open Apex: A Review of the Literature

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- Full access to the text;
- Text published in English;
- Studies conducted in humans;
- Published in the last 5 years, from 2015 to 2020;
- Young patients with open apex autotransplanted teeth.
2.2. Search Strategy
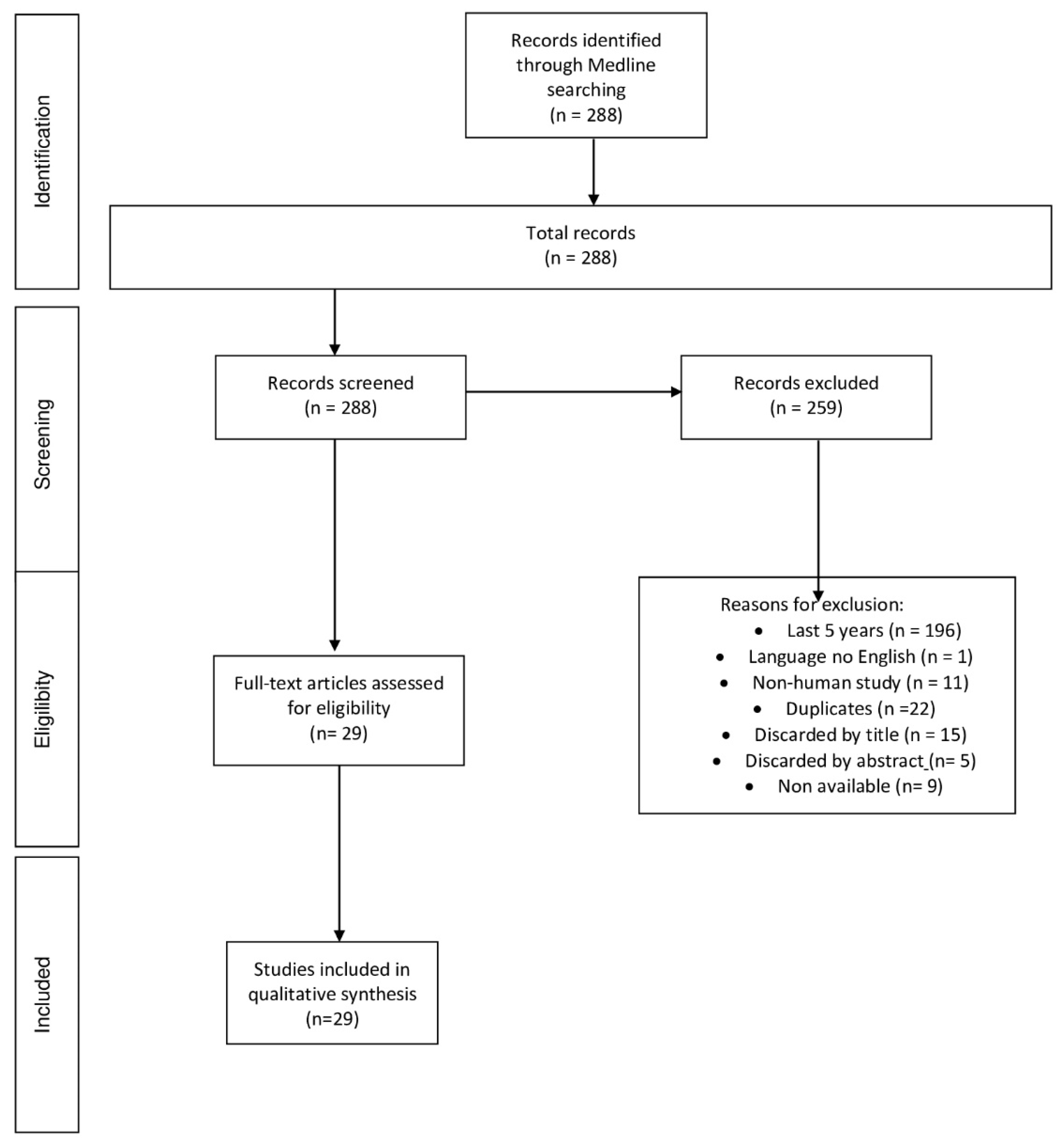
2.3. Study Selection
2.4. Data Extraction
3. Results
4. Review
- Stage of tooth root formation: It is most optimal when between two-thirds and three-quarters of the root have formed [22]. Some authors did not find significant differences if the tooth presented a minor root formation [23]. Some authors indicated that the diameter of the root canal in a tooth with a wide open apex (1–2 mm) decreases the risk of pulp necrosis, since the revascularization of the pulp is greater and implies a new supply of blood and nervous fibers that achieve the vitality of the tooth [17,24]. If the formation of the tooth root is not completed, it will do so in its new location [25]. In addition, the preservation of the alveolar bone and revascularization of the pulp may be achieved [25], avoiding root canal treatment and its possible complications due to its difficulty in this kind of tooth [26].
- Type of tooth [17]: According to the literature, the premolar is the tooth most used as a donor in cases of open apex [27,28]. It has been described that this may be because premolars are the teeth most commonly extracted in orthodontic treatments [22,27,29,30]. Others report that transplants of third molars, impacted canines and supernumerary teeth are also common, and that there is no significant difference if the donor’s tooth comes from the maxilla or the mandible [29,31,32,33]. In his study, Tang considered an optimal root as one that is morphologically conical, smooth and simple, considering teeth with multiple roots and a rough surface to be more complicated [29].
- The state of the periodontal ligament [17]: Kafourou et al. [17] described how the state of the periodontal ligament is key to the success of dental transplantation and that excessive trauma has a negative influence on the treatment’s prognosis [17]. It of vital importance that the soft tissue surrounding the periodontal ligament—that is, the cells that make up Hertwig’s root sheath—is not injured during the extraction of the donor’s tooth [26], as well as the apical papilla stem cells (SCAPs), which are fundamental for the root development of immature teeth [34]. The extraction must be atraumatic and prevent damage to the tissues surrounding the tooth [25,27,29], in order to increase the success and survival rate of the autotransplant [23]. Additionally, Gilijamse et al. [35] assured us that an intact periodontal ligament around the tooth facilitates its growth and adaptation to the alveolar bone, and also explained that to avoid damage to this tissue, the size of the new alveolus must be greater than that of the donor tooth. This guarantees the preservation of the tissue and thus reduces the risk of ankylosis and external root resorption [35]. However, he also described how teeth transplanted into the socket without any modification have a higher survival rate [35]. Tsukiboshi qualified this factor as the most important for successful transplantation [36]. Altogether, it is essential that the periodontal ligament covering the tooth is not damaged to avoid ankylosis and root resorption, and induce the formation of bone for the healing of the area [36], as well as the Hertwig sheath, in order to continue the development of the root of the transplanted tooth [36].
- Location: Regarding the maxillary or mandibular location of the receptor alveolus, better results are described in the maxilla [28], although little significant differences are mentioned [25]. Nevertheless, authors describe how autotransplants in the anterior maxilla require greater aesthetic results [28].
- Volume of alveolar bone and quality: It is stated that if the bone is deficient both in quantity or quality, it has a negative influence on the success of the transplant, since the surgery is hindered and the aesthetic result may be compromised. For this reason, an adequate thickness of the buccal and lingual cortical bone of the area where the tooth will be transplanted is required [17]. In fact, Gilijamse et al. [35] reported that one of the primary factors for the transplant’s success is that the walls of the recipient socket must have acceptable dimensions to guarantee the stability of the donor tooth. Additionally, if the extracted tooth presents ankylosis or infection in the recipient socket, it could influence the new tooth’s adaptation to the socket. [17]. Early tooth loss during the patient’s growth period and the absence of replacement by dental autotransplantation has a negative influence on the quality of the residual bone, which will be needed for the placement of an implant after the growth period has ended [17]. This results in the need for previous bone graft procedures [17,26].
- Tissue damage during the procedure: Some authors stated that the affected tooth must be extracted carefully, trying to contact the ligament as little as possible to avoid ankylosis and other complications [5,27,35]. Verweij et al. [27] also highlighted the importance of minimizing the iatrogenic damage caused by the excessive attempts to fit the replica in the alveolus.
- Use of a 3D replica [30]: that has been manufactured from a previous CBCT [27] and that facilitates the dental autotransplantation process [16,27,28,37,38], reducing the manipulation and extra-alveolar time of the transplanted tooth [26,39]. By using the replica of the donor’s tooth, the extra-alveolar time is minimized to less than 1 minute [27], even seconds [40]. At the same time, as an alternative to this individualized replica of the patient’s tooth, a pre-designed surgical template or guide of the type of donor tooth in question could be used, which can be sterilized and reused, but this entails a size discrepancy between the template and the donor tooth [27,38]. EzEldden et al. [30] made use of this surgical guide to favor the position of the donor tooth and confirmed that as a result of the use of the replica, the time of the surgery itself was reduced, going from 40 to 90 min in surgeries without replication and up to 30 to 45 min in surgeries where this replica was used. Furthermore, EzEldden pointed out that everything manipulated using this replica is not performed on the donor’s tooth, so it helps to keep its periodontal ligament intact, avoiding future root resorption, pulp necrosis or other possible complications [30].
- Stabilization of the donor tooth and its duration [17]: It is important to stabilize the donor tooth to prevent mobility, since a lack of retention increases trauma and instability while healing occurs [41]. There is controversy about the material to be used and the time to splint the donor tooth. Sutures cause less risk of ankylosis compared with wire, while the probability of failure will be higher [27,29]. Verweij et al., Gilijamse et al. and Strbac et al. [23,25,27,35] used sutures to stabilize the tooth in an interocclusal position, as did Jakobsen et al. [22], who also used sutures and kept them for a week. Gonzalez-Ocasio et al. used orthodontic wires with a composite to splint the transplanted teeth to the adjacent teeth for a month [42], and other authors such as Mejía Cardona et al. [26] used a combination of sutures and splints and kept the tooth in infraocclusion for 6 weeks or 3 weeks [33]. Meanwhile, Tang et al. [27] indicated that in a series of treated cases, no significant differences were found in terms of the stabilization method.
- Extra-alveolar time of the donor tooth and its storage [23]: Some authors state that it is vital to minimize the extra-alveolar time of the donor tooth as much as possible to preserve the periodontal ligament and maintain Hertwig’s epithelial sheath [43], and to reduce complications [5,23,27]. Strbac et al. [25] suggested that during this time, the tooth must be preserved in a saline solution in order to not to interfere with the possibility of pulp revascularization [23]. EzEldeen et al. [30] highlighted that with the use of a replica, the donor tooth’s extra-alveolar time is reduced to less than 1 minute, whereas the extra-alveolar time of the donor tooth can be around 10 min in other circumstances.
- Operator/surgeon’s experience: Jakobsen et al. [22], in their study, concluded that there are no significant differences in terms of the operator’s experience, nor in the occurrence of adverse effects. Similarly, Stange et al. [28], in their study, could not validate this factor, since the same operator performed all operations, but they noted that, as in all dental procedures, experience is a must. Meanwhile, Juslin et al. [39] confirmed that surgeon experience increased the survival rate of the dental autotransplantation in 17% of cases.
- Need for endodontic treatment [23]: In the case of an open apex, an immediate root canal treatment should not be performed, so that a follow-up can be carried out and the root may finish forming without showing signs or symptoms of infection [2,31]. Root canal treatment is needed only when there are radiological signs of resorption or periapical pathology [31]. If there is positive pulp sensitivity, it will be classified as success, while if there is negative pulp sensitivity, it will be classified as survival [10]. Moreover, 96% pulp healing success without the need for endodontics has been observed in autotransplants with open apex, compared with 15% in mature teeth [44]. Verweij et al. reflected that if root canal treatment is necessary, it should be performed prior to transplantation or 15 days after it [23]. Kafourou et al. and Tsukiboshi et al. [17,36] considered performing a root canal treatment when necessary, 15 days after transplantation. Furthermore, Kafourou et al. [17] added that teeth treated endodontically after dental autotransplantation have a favorable prognosis.
- Treatment follow-up: Tsukiboshi et al. [36] suggested a follow-up consisting of a monthly X-ray for the first 3 months to verify that there is no root resorption or pulp necrosis. If there is no evidence of this, further follow-up visits are scheduled after 6 months, 2 years and 3 years [36]. The follow-up schedule that Tang et al. [29] described is as follows: 1 week, 2 weeks, 4 weeks, 2 months, 4 months, 6 months, 1 year, and 2 years. In addition, in open apex autotransplantation, it is important to have a radiological sequence taken in the follow-up sessions, where the continuous development of the root of a transplanted tooth with open apex can be ensured [30].
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chung, W.-C.; Tu, Y.-K.; Lin, Y.-H.; Lu, H.-K. Outcomes of autotransplanted teeth with complete root formation: A systematic review and meta-analysis. J. Clin. Periodontol. 2014, 41, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Murtadha, L.; Kwok, J. Do Autotransplanted Teeth Require Elective Root Canal Therapy? A Long-Term Follow-Up Case Series. J. Oral Maxillofac. Surg. 2017, 75, 1817–1826. [Google Scholar] [CrossRef] [PubMed]
- Schwartz-Arad, D.; Bichacho, N. Effect of age on single implant submersion rate in the central maxillary incisor region: A long-term retrospective study. Clin. Implant Dent. Relat. Res. 2015, 17, 509–514. [Google Scholar] [CrossRef]
- Daftary, F.; Mahallati, R.; Bahat, O.; Sullivan, R.M. Lifelong craniofacial growth and the implications for osseointegrated implants. Int. J. Oral Maxillofac. Implant. 2013, 28, 163–169. [Google Scholar] [CrossRef] [Green Version]
- Ong, D.; Itskovich, Y.; Dance, G. Autotransplantation: A viable treatment option for adolescent patients with significantly compromised teeth. Aust. Dent. J. 2016, 61, 396–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaaf, H.; Kerkmann, H.; Pitka, F.; Bock, N.C.; Attia, S. Replantation of a displaced incisor in a boy with a cleft lip and alveolus: A case report. J. Med. Case Rep. 2016, 10, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parvini, P.; Obreja, K.; Trimpou, G.; Mahmud, S.; Sader, R. Autotransplantation of teeth. Int. J. Esthet. Dent. 2018, 13, 274–282. [Google Scholar]
- Candeiro, G.T.; Alencar-Júnior, E.A.; Scarparo, H.C.; Furtado-Júnior, J.H.; Gavini, G.; Caldeira, C.L. Eight-year follow-up of autogenous tooth transplantation involving multidisciplinary treatment. J. Oral Sci. 2015, 57, 273–276. [Google Scholar] [CrossRef] [Green Version]
- Tsukiboshi, M. Autotransplantation of teeth: Requirements for predictable success. Dent. Traumatol. 2002, 18, 157–180. [Google Scholar] [CrossRef]
- Atala-Acevedo, C.; Abarca, J.; Martínez-Zapata, M.J.; Díaz, J.; Olate, S.; Zaror, C. Success rate of autotransplantation of teeth with an open Apex: Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2017, 75, 35–50. [Google Scholar] [CrossRef]
- Boschini, L.; Melillo, M.; Berton, F. Long term survival of mature autotransplanted teeth: A retrospective single center analysis. J. Dent. 2020, 98, 103371. [Google Scholar] [CrossRef] [PubMed]
- Jaiswara, C.; Srivastava, V.K.; Dhiman, N. Autotransplantation of a strange positioned impacted central incisor in a surgically prepared socket: A miracle esthetic concept. Int. J. Clin. Pediatr. Dent. 2016, 9, 269–272. [Google Scholar] [CrossRef] [PubMed]
- Lucas-Taulé, E.; Llaquet, M.; Muñoz-Peñalver, J.; Somoza, J.; Satorres-Nieto, M.; Hernández-Alfaro, F. Fully Guided Tooth Autotransplantation Using a Multidrilling Axis Surgical Stent: Proof of Concept. J. Endod. 2020, 46, 1515–1521. [Google Scholar] [CrossRef] [PubMed]
- Szemraj-Folmer, A.; Kuc-Michalska, M.; Plakwicz, P. Patient with asymmetric multiple hypodontia treated with autotransplantation of 2 premolars. Am. J. Orthod. Dentofac. Orthop. 2019, 155, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, M.M.; Ferreira, H.M.; Botelho, F.; Carrilho, E. Autotransplantation combined with orthodontic treatment: A case involving the maxillary central incisors with root resorption after traumatic injury. Restor. Dent. Endod. 2015, 40, 236–240. [Google Scholar] [CrossRef]
- Cousley, R.R.J.; Gibbons, A.; Nayler, J. A 3D printed surgical analogue to reduce donor tooth trauma during autotransplantation. J. Orthod. 2017, 44, 287–293. [Google Scholar] [CrossRef]
- Kafourou, V.; Tong, H.J.; Day, P.; Houghton, N.; Spencer, R.J.; Duggal, M. Outcomes and prognostic factors that influence the success of tooth autotransplantation in children and adolescents. Dent. Traumatol. 2017, 33, 393–399. [Google Scholar] [CrossRef]
- Kokai, S.; Kanno, Z.; Koike, S.; Uesugi, S.; Takahashi, Y.; Ono, T.; Soma, K. Retrospective study of 100 autotransplanted teeth with complete root formation and subsequent orthodontic treatment. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 982–989. [Google Scholar] [CrossRef]
- Bae, J.-H.; Choi, Y.-H.; Cho, B.-H.; Kim, Y.-K.; Kim, S.-G. Autotransplantation of teeth with complete root formation: A case series. J. Endod. 2010, 36, 1422–1426. [Google Scholar] [CrossRef]
- Almpani, K.; Papageorgiou, S.N.; Papadopoulos, M.A. Autotransplantation of teeth in humans: A systematic review and meta-analysis. Clin. Oral Investig. 2015, 19, 1157–1179. [Google Scholar] [CrossRef]
- Rohof, E.C.M.; Kerdijk, W.; Jansma, J.; Livas, C.; Ren, Y. Autotransplantation of teeth with incomplete root formation: A systematic review and meta-analysis. Clin. Oral Investig. 2018, 22, 1613–1624. [Google Scholar] [CrossRef] [Green Version]
- Jakobsen, C.; Stokbro, K.; Kier-Swiatecka, E.; Ingerslev, J.; Thorn, J.J. Autotransplantation of premolars: Does surgeon experience matter? Int. J. Oral Maxillofac. Surg. 2018, 47, 1604–1608. [Google Scholar] [CrossRef] [PubMed]
- Verweij, J.P.; Toxopeus, E.E.; Fiocco, M.; Mensink, G.; van Merkesteyn, J.P. Success and survival of autotransplanted premolars and molars during short-term clinical follow-up. J. Clin. Periodontol. 2016, 43, 167–172. [Google Scholar] [CrossRef] [PubMed]
- van Westerveld, K.J.H.; Verweij, J.P.; Fiocco, M.; Mensink, G.; van Merkesteyn, J.P.R. Root elongation after autotransplantation in 58 transplanted remolars: The dadiographic width of the apex as a predictor. J. Oral Maxillofac. Surg. 2019, 77, 1351–1357. [Google Scholar] [CrossRef] [PubMed]
- Strbac, G.D.; Giannis, K.; Mittlböck, M.; Fuerst, G.; Zechner, W.; Stavropoulos, A.; Ulm, C. Survival rate of autotransplanted teeth after 5 years-A retrospective cohort study. J. Cranio-Maxillofac. Surg. 2017, 45, 1143–1149. [Google Scholar] [CrossRef]
- Mejía-Cardona, J.L.; Marcano-Caldera, M.; Vera, J.; Sigurdsson, A. Autotransplantation of a premolar with incipient root development, an 18-Year Follow-Up. Eur. Endod. J. 2017, 2, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Verweij, J.P.; Moin, D.A.; Mensink, G.; Nijkamp, P.; Wismeijer, D.; van Merkesteyn, J.P. Autotransplantation of premolars with a 3-dimensional printed titanium replica of the donor tooth functioning as a surgical guide: Proof of concept. J. Oral Maxillofac. Surg. 2016, 74, 1114–1119. [Google Scholar] [CrossRef]
- Stange, K.M.; Lindsten, R.; Bjerklin, K. Autotransplantation of premolars to the maxillary incisor region: A long-term follow-up of 12-22 years. Eur. J. Orthod. 2016, 38, 508–515. [Google Scholar] [CrossRef] [Green Version]
- Tang, H.; Shen, Z.; Hou, M.; Wu, L. Autotransplantation of mature and immature third molars in 23 Chinese patients: A clinical and radiological follow-up study. BMC Oral Health 2017, 17, 163. [Google Scholar] [CrossRef] [Green Version]
- EzEldeen, M.; Wyatt, J.; Al-Rimawi, A.; Coucke, W.; Shaheen, E.; Lambrichts, I.; Willems, G.; Politis, C.; Jacobs, R. Use of CBCT guidance for tooth autotransplantation in children. J. Dent. Res. 2019, 98, 406–413. [Google Scholar] [CrossRef]
- Abela, S.; Murtadha, L.; Bister, D.; Andiappan, M.; Kwok, J. Survival probability of dental autotransplantation of 366 teeth over 34 years within a hospital setting in the United Kingdom. Eur. J. Orthod. 2019, 41, 551–556. [Google Scholar] [CrossRef] [PubMed]
- Grisar, K.; Nys, M.; The, V.; Vrielinck, L.; Schepers, S.; Jacobs, R.; Politis, C. Long-term outcome of autogenously transplanted maxillary canines. Clin. Exp. Dent. Res. 2019, 5, 67–75. [Google Scholar] [CrossRef]
- Tschammler, C.; Angermair, J.; Heiligensetzer, M.; Linsenmann, R.; Huth, K.C.; Nolte, D. Primary canine auto-transplantation: A new surgical technique. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Palma, P.J.; Martins, J.; Diogo, P.; Sequeira, D.; Ramos, J.C.; Diogenes, A.; Santos, J.M. Does apical papilla survive and develop in apical periodontitis presence after regenerative endodontic procedures? Appl. Sci. 2019, 9, 3942. [Google Scholar] [CrossRef] [Green Version]
- Gilijamse, M.; Baart, J.A.; Wolff, J.; Sándor, G.K.; Forouzanfar, T. Tooth autotransplantation in the anterior maxilla and mandible: Retrospective results in young patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, e187–e192. [Google Scholar] [CrossRef]
- Tsukiboshi, M.; Yamauchi, N.; Tsukiboshi, Y. Long-term outcomes of autotransplantation of teeth: A case series. Dent. Traumatol. 2019, 35, 358–367. [Google Scholar] [CrossRef] [Green Version]
- Erdem, N.F.; Gümüşer, Z. Retrospective evaluation of immediate impacted third molars autotransplantation after extractions of mandibular first and/or second molars with chronic periapical lesions. J. Oral Maxillofac. Surg. 2021, 79, 37–48. [Google Scholar] [CrossRef]
- Strbac, G.D.; Schnappauf, A.; Giannis, K.; Bertl, M.H.; Moritz, A.; Ulm, C. Guided autotransplantation of teeth: A novel method using virtually planned 3-dimensional templates. J. Endod. 2016, 42, 1844–1850. [Google Scholar] [CrossRef]
- Juslin, J.; Jääsaari, P.; Teerijoki-Oksa, T.; Suominen, A.; Thorén, H. Survival of Autotransplanted teeth with open apices: A retrospective cohort study. J. Oral Maxillofac. Surg. 2020, 78, 902.e1–902.e9. [Google Scholar] [CrossRef]
- Ashkenazi, M.; Shashua, D.; Kegen, S.; Nuni, E.; Duggal, M.; Shuster, A. Computerized three-dimensional design for accurate orienting and dimensioning artificial dental socket for tooth autotransplantation. Quintessence Int. 2018, 49, 663–671. [Google Scholar] [CrossRef]
- Anitua, E.; Mendinueva-Urkia, M.; Galan-Bringas, S.; Murias-Freijo, A.; Alkhraisat, M.H. Tooth autotransplantation as a pillar for 3D regeneration of the alveolar process after severe traumatic injury: A case report. Dent. Traumatol. 2017, 33, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Ocasio, J.; Stevens, M. Autotransplantation of third molars with platelet-rich plasma for immediate replacement of extracted non-restorable teeth: A case series. J. Oral Maxillofac. Surg. 2017, 75, 1833.e1–1833.e6. [Google Scholar] [CrossRef] [PubMed]
- Mohd Mokhtar, S.; Abd Jalil, L.; Muhd Noor, N. Autotransplantation of ectopic permanent maxillary incisors. Case Rep. Dent. 2017, 2017, 7361924. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.; O'Reilly, C.; Ahmed, B. Autotransplantation of third molars: A literature review and preliminary protocols. Br. Dent. J. 2020, 228, 247–251. [Google Scholar] [CrossRef]


{kind=link}
| Database | Search Strategy | Findings |
|---|---|---|
| Medline | (Tooth autotransplantation) AND (incomplete root) | 28 |
| (Tooth autotransplantation) AND (open apex) | 12 | |
| (Tooth autotransplantation) and (children patients) | 148 | |
| (Tooth autotransplantation) AND (young patients) | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pecci Lloret, M.P.; Martínez, E.P.; Rodríguez Lozano, F.J.; Pecci Lloret, M.R.; Guerrero Gironés, J.; Riccitiello, F.; Spagnuolo, G. Influencing Factors in Autotransplantation of Teeth with Open Apex: A Review of the Literature. Appl. Sci. 2021, 11, 4037. https://0-doi-org.brum.beds.ac.uk/10.3390/app11094037
Pecci Lloret MP, Martínez EP, Rodríguez Lozano FJ, Pecci Lloret MR, Guerrero Gironés J, Riccitiello F, Spagnuolo G. Influencing Factors in Autotransplantation of Teeth with Open Apex: A Review of the Literature. Applied Sciences. 2021; 11(9):4037. https://0-doi-org.brum.beds.ac.uk/10.3390/app11094037
Chicago/Turabian StylePecci Lloret, María P., Elena Pina Martínez, Francisco J. Rodríguez Lozano, Miguel R. Pecci Lloret, Julia Guerrero Gironés, Francesco Riccitiello, and Gianrico Spagnuolo. 2021. "Influencing Factors in Autotransplantation of Teeth with Open Apex: A Review of the Literature" Applied Sciences 11, no. 9: 4037. https://0-doi-org.brum.beds.ac.uk/10.3390/app11094037