
Effect of Ligament Mapping from Different Magnetic Resonance Image Quality on Joint Stability in a Personalized Dynamic Model of the Human Ankle Complex


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
2.1. The Model
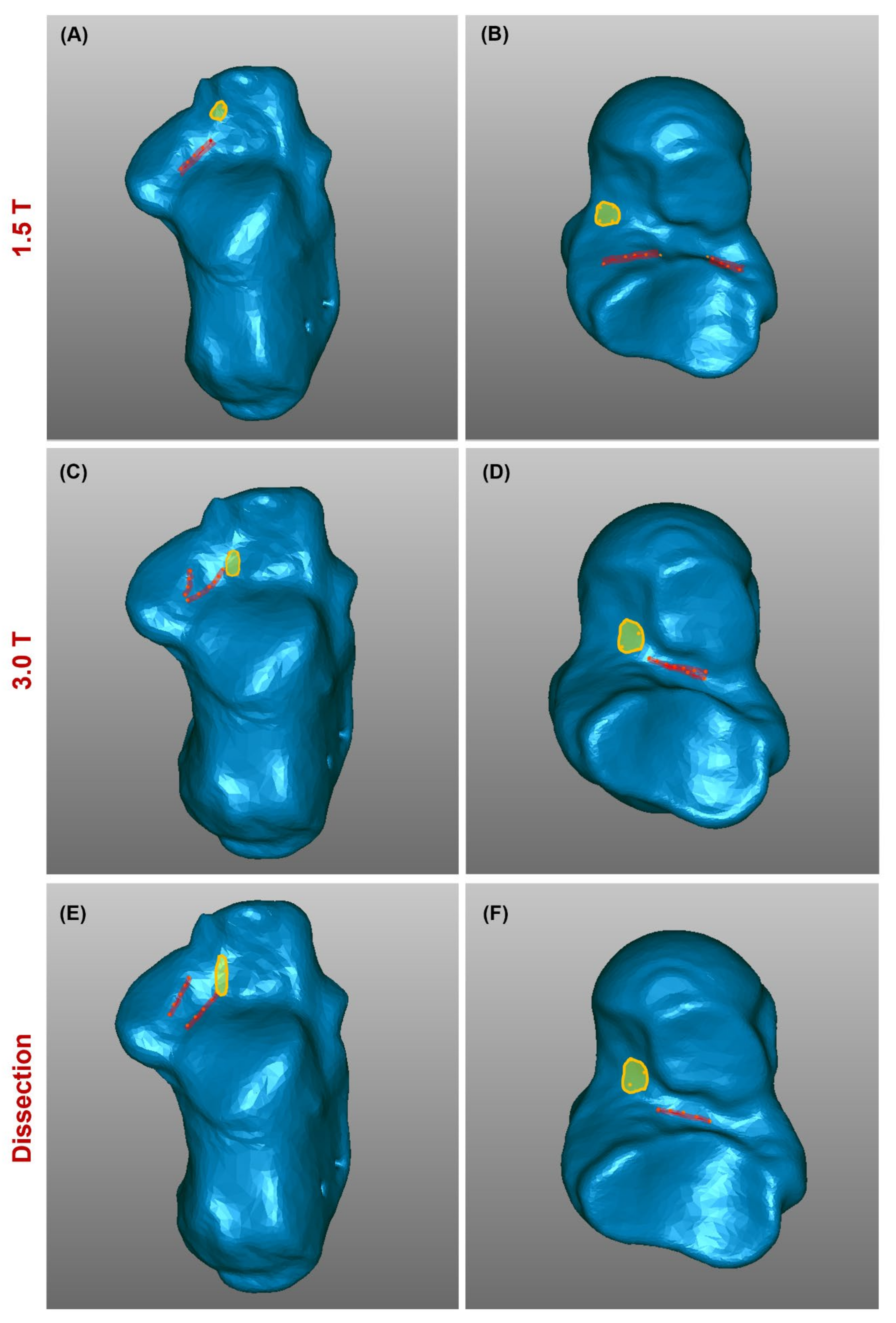
2.2. Identification of 1.5 T MRI-Based Ligament Attachments
2.3. Identification of 3.0 T MRI-Based Ligament Attachments
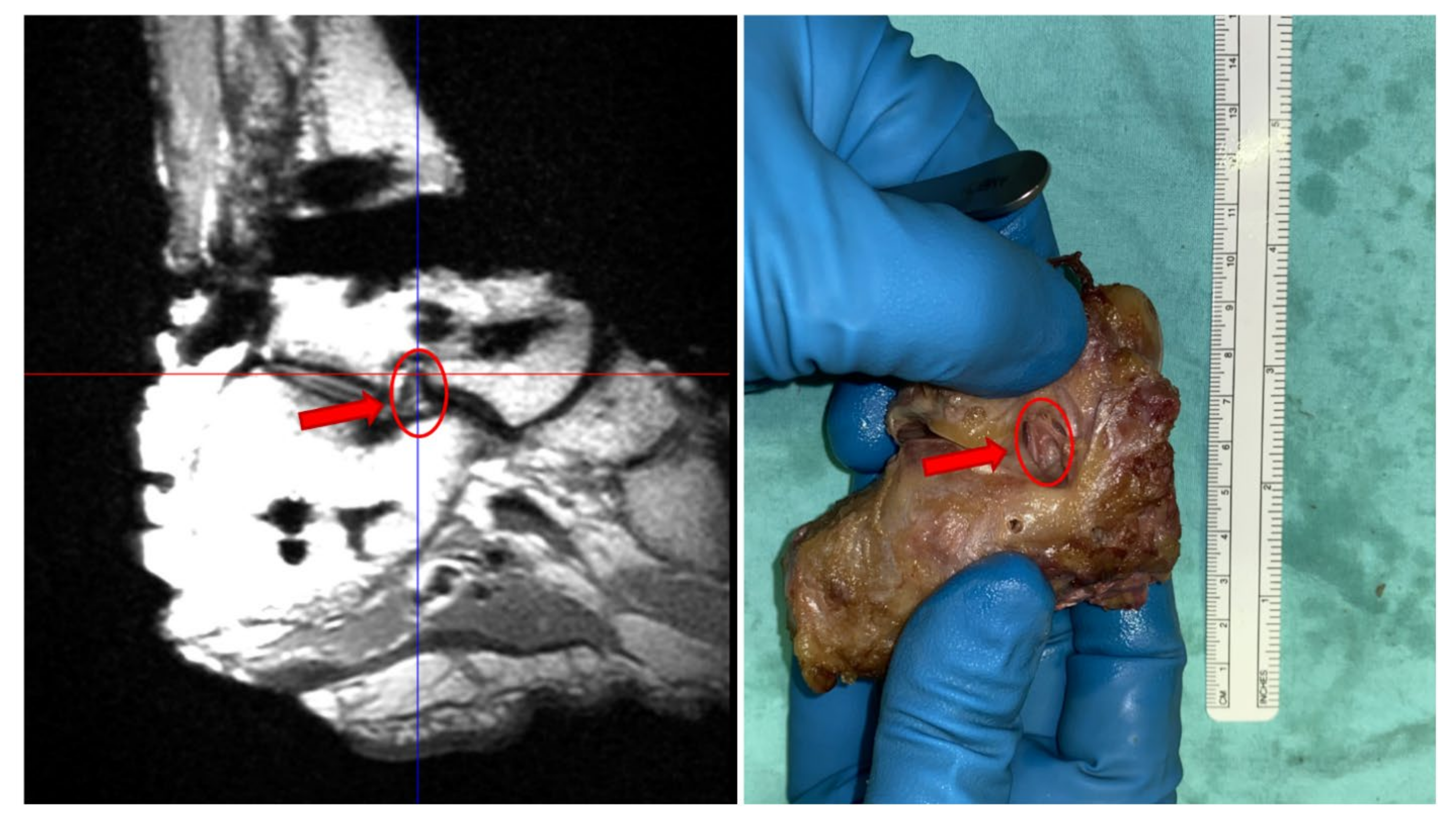
3. Dissection
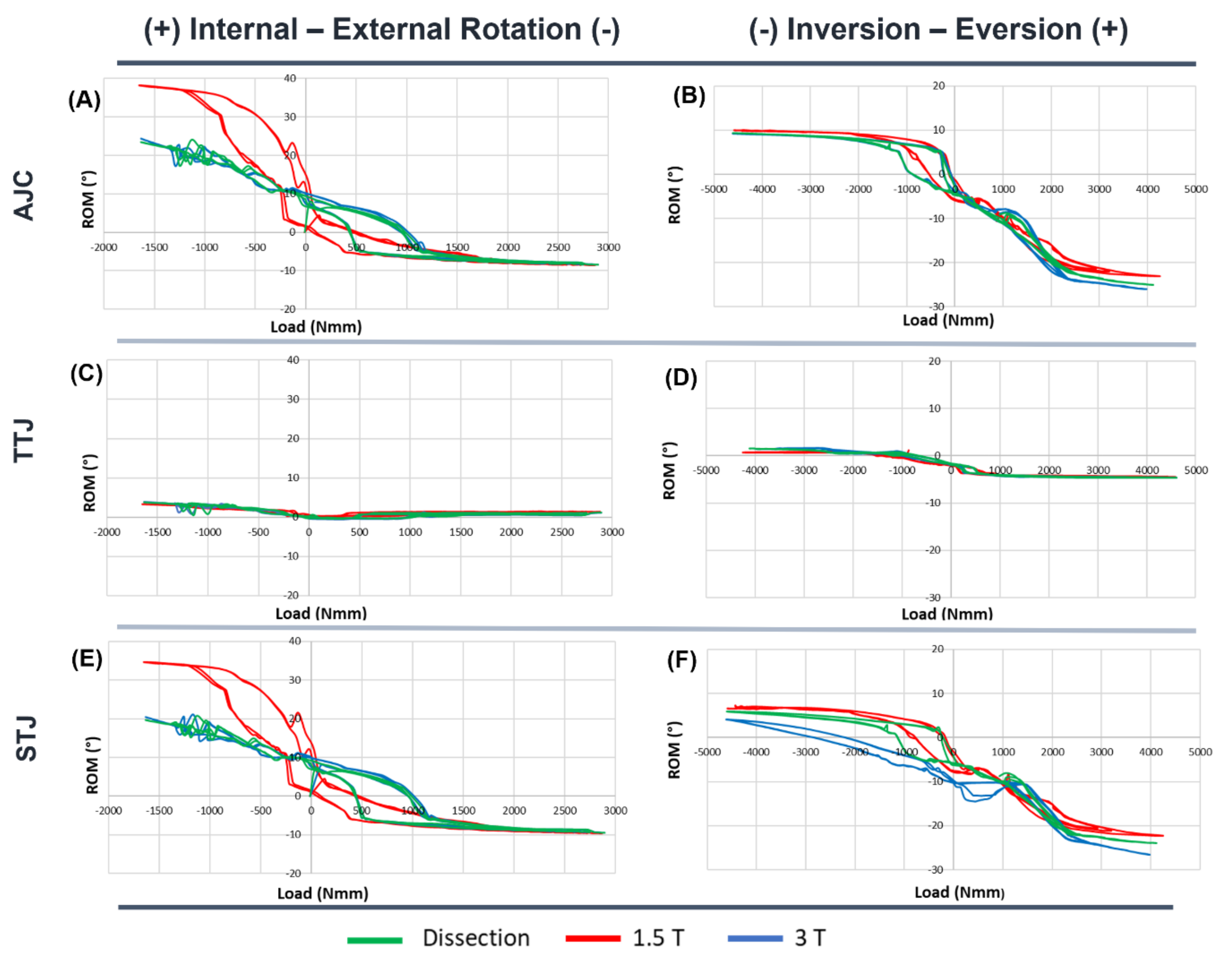
Model Simulations with Updated Mapping
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Leardini, A.; O’Connor, J.J.; Catani, F.; Giannini, S. The role of the passive structures in the mobility and stability of the human ankle joint: A literature review. Foot Ankle Int. 2000, 21, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Stagni, R.; Leardini, A.; O’Connor, J.J.; Giannini, S. Role of passive structures in the mobility and stability of the human subtalar joint: A literature review. Foot Ankle Int. 2003, 24, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Petersen, W.; Rembitzki, I.V.; Koppenburg, A.G.; Ellermann, A.; Liebau, C.; Bruggemann, G.P.; Best, R. Treatment of acute ankle ligament injuries: A systematic review. Arch. Orthop. Trauma. Surg. 2013, 133, 1129–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Bekerom, M.P.; Kerkhoffs, G.M.; McCollum, G.A.; Calder, J.D.; van Dijk, C.N. Management of acute lateral ankle ligament injury in the athlete. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2013, 21, 1390–1395. [Google Scholar] [CrossRef]
- Guillo, S.; Bauer, T.; Lee, J.W.; Takao, M.; Kong, S.W.; Stone, J.W.; Mangone, P.G.; Molloy, A.; Perera, A.; Pearce, C.J.; et al. Consensus in chronic ankle instability: Aetiology, assessment, surgical indications and place for arthroscopy. Orthop. Traumatol. Surg. Res. 2013, 99, S411–S419. [Google Scholar] [CrossRef] [Green Version]
- Michels, F.; Pereira, H.; Calder, J.; Matricali, G.; Glazebrook, M.; Guillo, S.; Karlsson, J.; Group, E.-A.A.I.; Acevedo, J.; Batista, J.; et al. Searching for consensus in the approach to patients with chronic lateral ankle instability: Ask the expert. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2018, 26, 2095–2102. [Google Scholar] [CrossRef]
- Yamaguchi, R.; Nimura, A.; Amaha, K.; Yamaguchi, K.; Segawa, Y.; Okawa, A.; Akita, K. Anatomy of the Tarsal Canal and Sinus in Relation to the Subtalar Joint Capsule. Foot Ankle Int. 2018, 39, 1360–1369. [Google Scholar] [CrossRef]
- Kim, T.H.; Moon, S.G.; Jung, H.G.; Kim, N.R. Subtalar instability: Imaging features of subtalar ligaments on 3D isotropic ankle MRI. BMC Musculoskelet. Disord. 2017, 18, 475. [Google Scholar] [CrossRef] [Green Version]
- Leardini, A.; O’Connor, J.J.; Giannini, S. Biomechanics of the natural, arthritic, and replaced human ankle joint. J. Foot Ankle Res. 2014, 7, 8. [Google Scholar] [CrossRef] [Green Version]
- Nie, B.; Panzer, M.B.; Mane, A.; Mait, A.R.; Donlon, J.P.; Forman, J.L.; Kent, R.W. Determination of the in situ mechanical behavior of ankle ligaments. J. Mech. Behav. Biomed. Mater. 2017, 65, 502–512. [Google Scholar] [CrossRef]
- Iaquinto, J.M.; Wayne, J.S. Computational model of the lower leg and foot/ankle complex: Application to arch stability. J. Biomech. Eng. 2010, 132, 021009. [Google Scholar] [CrossRef] [PubMed]
- Imhauser, C.W.; Siegler, S.; Udupa, J.K.; Toy, J.R. Subject-specific models of the hindfoot reveal a relationship between morphology and passive mechanical properties. J. Biomech. 2008, 41, 1341–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leardini, A.; O’Connor, J.J.; Catani, F.; Giannini, S. A geometric model of the human ankle joint. J. Biomech. 1999, 32, 585–591. [Google Scholar] [CrossRef]
- Forlani, M.; Sancisi, N.; Parenti-Castelli, V. A three-dimensional ankle kinetostatic model to simulate loaded and unloaded joint motion. J. Biomech. Eng. 2015, 137, 061005. [Google Scholar] [CrossRef] [PubMed]
- Liacouras, P.C.; Wayne, J.S. Computational modeling to predict mechanical function of joints: Application to the lower leg with simulation of two cadaver studies. J. Biomech. Eng. 2007, 129, 811–817. [Google Scholar] [CrossRef]
- Purevsuren, T.; Kim, K.; Batbaatar, M.; Lee, S.; Kim, Y.H. Influence of ankle joint plantarflexion and dorsiflexion on lateral ankle sprain: A computational study. Proc. Inst. Mech. Eng. Part H 2018, 232, 458–467. [Google Scholar] [CrossRef]
- Palazzi, E.; Siegler, S.; Balakrishnan, V.; Leardini, A.; Caravaggi, P.; Belvedere, C. Estimating the stabilizing function of ankle and subtalar ligaments via a morphology-specific three-dimensional dynamic model. J. Biomech. 2020, 98, 109421. [Google Scholar] [CrossRef]
- Li, J.; Wei, Y.; Wei, M. Finite Element Analysis of the Effect of Talar Osteochondral Defects of Different Depths on Ankle Joint Stability. Med. Sci. Monit. 2020, 26, e921823. [Google Scholar] [CrossRef]
- Haraguchi, N.; Armiger, R.S.; Myerson, M.S.; Campbell, J.T.; Chao, E.Y. Prediction of three-dimensional contact stress and ligament tension in the ankle during stance determined from computational modeling. Foot Ankle Int. 2009, 30, 177–185. [Google Scholar] [CrossRef]
- Belvedere, C.; Siegler, S.; Ensini, A.; Toy, J.; Caravaggi, P.; Namani, R.; Giannini, G.; Durante, S.; Leardini, A. Experimental evaluation of a new morphological approximation of the articular surfaces of the ankle joint. J. Biomech. 2017, 53, 97–104. [Google Scholar] [CrossRef]
- Golano, P.; Vega, J.; de Leeuw, P.A.; Malagelada, F.; Manzanares, M.C.; Gotzens, V.; van Dijk, C.N. Anatomy of the ankle ligaments: A pictorial essay. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2010, 18, 557–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anand Prakash, A. Anatomy of Ankle Syndesmotic Ligaments: A Systematic Review of Cadaveric Studies. Foot Ankle Spec. 2020, 13, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Michels, F.; Matricali, G.; Vereecke, E.; Dewilde, M.; Vanrietvelde, F.; Stockmans, F. The intrinsic subtalar ligaments have a consistent presence, location and morphology. Foot Ankle Surg. 2021, 27, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Poonja, A.J.; Hirano, M.; Khakimov, D.; Ojumah, N.; Tubbs, R.S.; Loukas, M.; Kozlowski, P.B.; Khan, K.H.; DiLandro, A.C.; D’Antoni, A.V. Anatomical Study of the Cervical and Interosseous Talocalcaneal Ligaments of the Foot with Surgical Relevance. Cureus 2017, 9, e1382. [Google Scholar] [CrossRef] [Green Version]
- Sconfienza, L.M.; Orlandi, D.; Lacelli, F.; Serafini, G.; Silvestri, E. Dynamic high-resolution US of ankle and midfoot ligaments: Normal anatomic structure and imaging technique. Radiographics 2015, 35, 164–178. [Google Scholar] [CrossRef]
- Ngai, S.S.; Tafur, M.; Chang, E.Y.; Chung, C.B. Magnetic Resonance Imaging of Ankle Ligaments. Can. Assoc. Radiol. J. 2016, 67, 60–68. [Google Scholar] [CrossRef] [Green Version]
- Chen, E.T.; Borg-Stein, J.; McInnis, K.C. Ankle Sprains: Evaluation, Rehabilitation, and Prevention. Curr. Sports Med. Rep. 2019, 18, 217–223. [Google Scholar] [CrossRef]
- Van Dyck, P.; Kenis, C.; Vanhoenacker, F.M.; Lambrecht, V.; Wouters, K.; Gielen, J.L.; Dossche, L.; Parizel, P.M. Comparison of 1.5-and 3-T MR imaging for evaluating the articular cartilage of the knee. Knee Surg. Sports Traumatol. Arthrosc. Off. J. ESSKA 2014, 22, 1376–1384. [Google Scholar] [CrossRef]
- Van Dyck, P.; Vanhoenacker, F.M.; Lambrecht, V.; Wouters, K.; Gielen, J.L.; Dossche, L.; Parizel, P.M. Prospective comparison of 1.5 and 3.0-T MRI for evaluating the knee menisci and ACL. J. Bone Jt. Surg. 2013, 95, 916–924. [Google Scholar] [CrossRef]
- Nouri, N.; Bouaziz, M.C.; Riahi, H.; Mechri, M.; Kherfani, A.; Ouertatani, M.; Ladeb, M.F. Traumatic Meniscus and Cruciate Ligament Tears in Young Patients: A Comparison of 3T Versus 1.5T MRI. J. Belg. Soc. Radiol. 2017, 101, 14. [Google Scholar] [CrossRef] [Green Version]
- Grossman, J.W.; De Smet, A.A.; Shinki, K. Comparison of the accuracy rates of 3-T and 1.5-T MRI of the knee in the diagnosis of meniscal tear. AJR Am. J. Roentgenol. 2009, 193, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Barr, C.; Bauer, J.S.; Malfair, D.; Ma, B.; Henning, T.D.; Steinbach, L.; Link, T.M. MR imaging of the ankle at 3 Tesla and 1.5 Tesla: Protocol optimization and application to cartilage, ligament and tendon pathology in cadaver specimens. Eur. Radiol. 2007, 17, 1518–1528. [Google Scholar] [CrossRef] [PubMed]
- Oehler, N.; Ruby, J.K.; Strahl, A.; Maas, R.; Ruether, W.; Niemeier, A. Hip abductor tendon pathology visualized by 1.5 versus 3. 0 Tesla MRIs. Arch. Orthop. Trauma. Surg. 2020, 140, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.S.; Barr, C.; Henning, T.D.; Malfair, D.; Ma, C.B.; Steinbach, L.; Link, T.M. Magnetic resonance imaging of the ankle at 3.0 Tesla and 1.5 Tesla in human cadaver specimens with artificially created lesions of cartilage and ligaments. Investig. Radiol. 2008, 43, 604–611. [Google Scholar] [CrossRef]
- Bauer, J.S.; Monetti, R.; Krug, R.; Matsuura, M.; Mueller, D.; Eckstein, F.; Rummeny, E.J.; Lochmueller, E.M.; Raeth, C.W.; Link, T.M. Advances of 3T MR imaging in visualizing trabecular bone structure of the calcaneus are partially SNR-independent: Analysis using simulated noise in relation to micro-CT, 1.5T MRI, and biomechanical strength. J. Magn. Reson. Imaging 2009, 29, 132–140. [Google Scholar] [CrossRef]
- Neri, E.; Caramella, D.; Bartolozzi, C. Image Processing in Radiology: Current Applications; Springer: Berlin, Germany; New York, NY, USA, 2008; p. x, 434p. [Google Scholar]
- Stevens, K.J.; Busse, R.F.; Han, E.; Brau, A.C.; Beatty, P.J.; Beaulieu, C.F.; Gold, G.E. Ankle: Isotropic MR imaging with 3D-FSE-cube--initial experience in healthy volunteers. Radiology 2008, 249, 1026–1033. [Google Scholar] [CrossRef] [Green Version]
- Siegler, S.; Block, J.; Schneck, C.D. The mechanical characteristics of the collateral ligaments of the human ankle joint. Foot Ankle 1988, 8, 234–242. [Google Scholar] [CrossRef]
- Funk, J.R.; Hall, G.W.; Crandall, J.R.; Pilkey, W.D. Linear and quasi-linear viscoelastic characterization of ankle ligaments. J. Biomech. Eng. 2000, 122, 15–22. [Google Scholar] [CrossRef]
- Lopez-Ben, R. Imaging of the subtalar joint. Foot Ankle Clin. 2015, 20, 223–241. [Google Scholar] [CrossRef]
- Sormaala, M.J.; Ruohola, J.P.; Mattila, V.M.; Koskinen, S.K.; Pihlajamaki, H.K. Comparison of 1.5T and 3T MRI scanners in evaluation of acute bone stress in the foot. BMC Musculoskelet. Disord. 2011, 12, 128. [Google Scholar] [CrossRef] [Green Version]
- Cledera, T.H.C.; Flores, D.V. Magnetic Resonance Imaging of Ankle Ligaments. Contemp. Diagn. Radiol. 2021, 44, 1–7. [Google Scholar] [CrossRef]
- Fritz, B.; Fritz, J.; Sutter, R. 3D MRI of the Ankle: A Concise State-of-the-Art Review. Semin. Musculoskelet. Radiol. 2021, 25, 514–526. [Google Scholar] [CrossRef] [PubMed]
- Durastanti, G.; Leardini, A.; Siegler, S.; Durante, S.; Bazzocchi, A.; Belvedere, C. Comparison of cartilage and bone morphological models of the ankle joint derived from different medical imaging technologies. Quant. Imaging Med. Surg. 2019, 9, 1368–1382. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campagnoli, E.; Siegler, S.; Ruiz, M.; Leardini, A.; Belvedere, C. Effect of Ligament Mapping from Different Magnetic Resonance Image Quality on Joint Stability in a Personalized Dynamic Model of the Human Ankle Complex. Appl. Sci. 2022, 12, 5087. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105087
Campagnoli E, Siegler S, Ruiz M, Leardini A, Belvedere C. Effect of Ligament Mapping from Different Magnetic Resonance Image Quality on Joint Stability in a Personalized Dynamic Model of the Human Ankle Complex. Applied Sciences. 2022; 12(10):5087. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105087
Chicago/Turabian StyleCampagnoli, Elena, Sorin Siegler, Maria Ruiz, Alberto Leardini, and Claudio Belvedere. 2022. "Effect of Ligament Mapping from Different Magnetic Resonance Image Quality on Joint Stability in a Personalized Dynamic Model of the Human Ankle Complex" Applied Sciences 12, no. 10: 5087. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105087