
Analysis of Functional Layout in Emergency Departments (ED). Shedding Light on the Free Standing Emergency Department (FSED) Model

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
1.1. Background of the Study: EDs and Introduction of the FSED Model
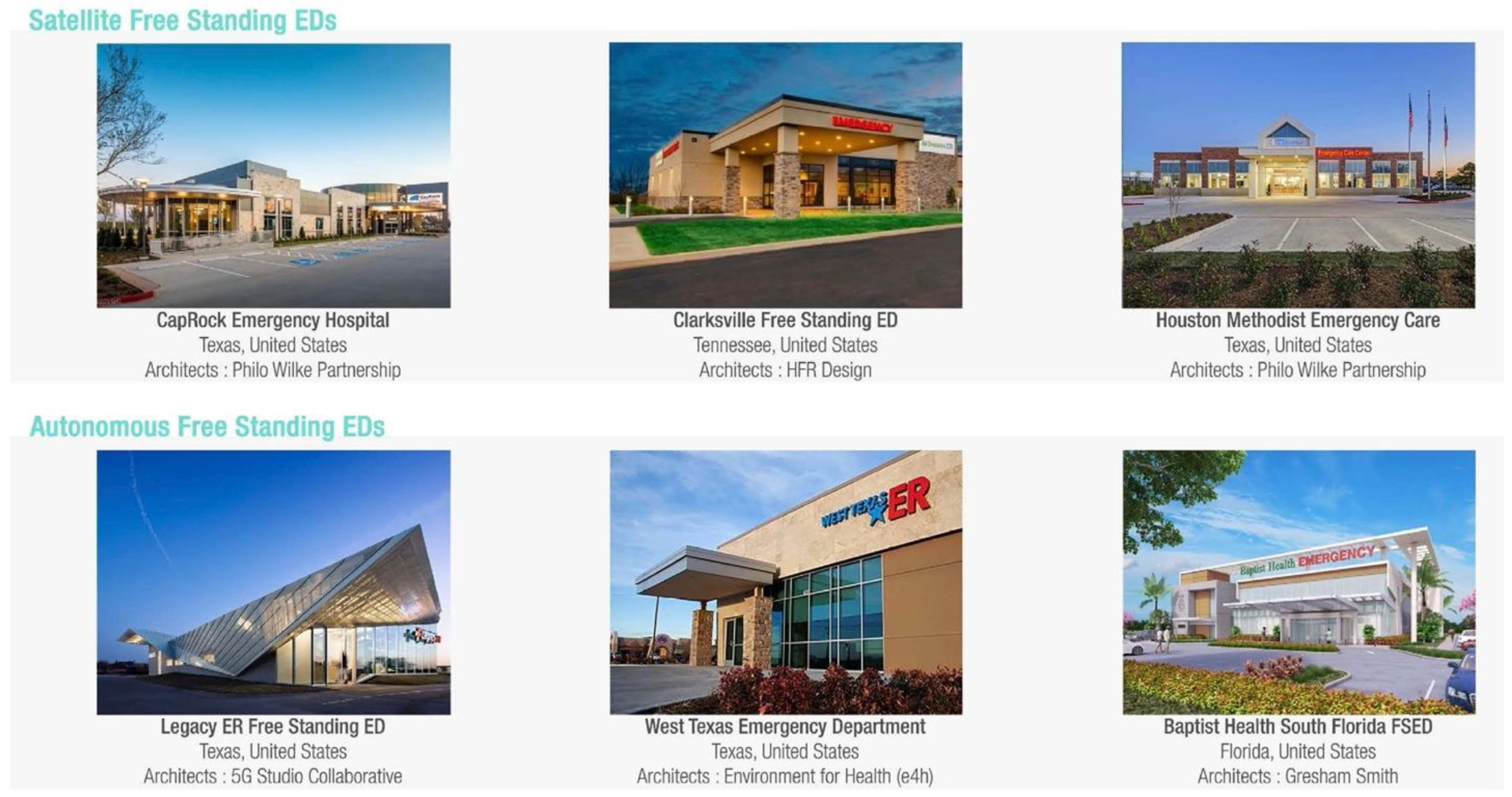
- Satellite Free Standing Emergency Departments (SFSED);
- Autonomous Free Standing Emergency Departments (AFSED);
1.2. Contemporary Challenges of Emergency Departments
1.3. Research Gap and Aim of the Study
2. Materials and Methods
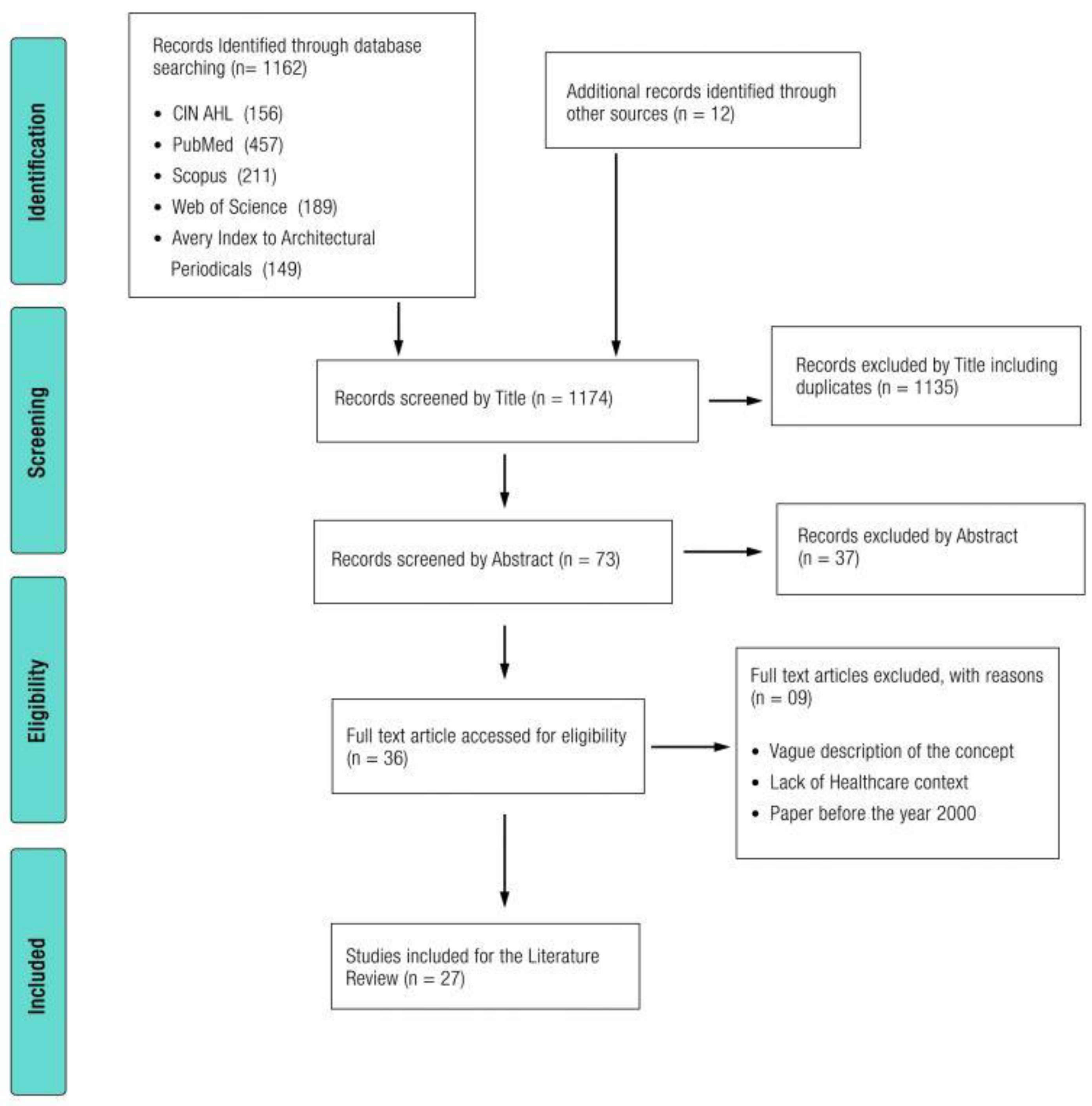
2.1. Literature Review
- date of publication: Only contributions from January 2000 to December 2021 have been included, in order to acquire information about the most recent trends;
- content focusing on hospital design: papers or documents pertaining to alternative architectural typologies were excluded from consideration;
- exclusion of papers or documents pertaining solely to working spaces in order to concentrate on diagnosis and treatment areas;
- emphasis on physical characteristics; publications that are solely concerned with managerial or clinical issues were excluded;
- regulations as the primary focus: publications that are entirely concerned with the laws or mandatory technical regulations of a given location are excluded;
- concentration on a certain model: publications not connected to HBED or FSED models were excluded;
- no specificity on temporary COVID-19 Emergency Department.
2.2. Case Studies Functional Layout Analysis
3. Results
3.1. Literature Review
3.1.1. Organizational Models
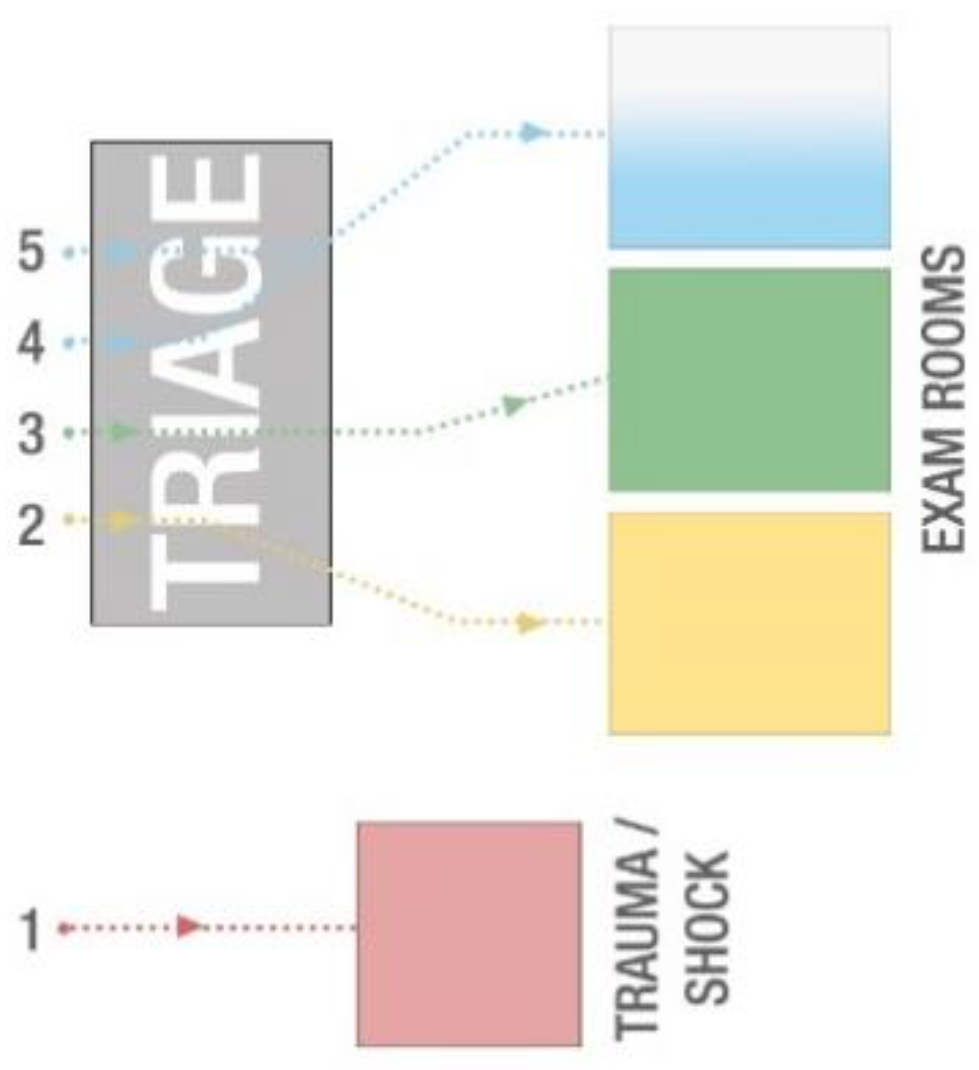
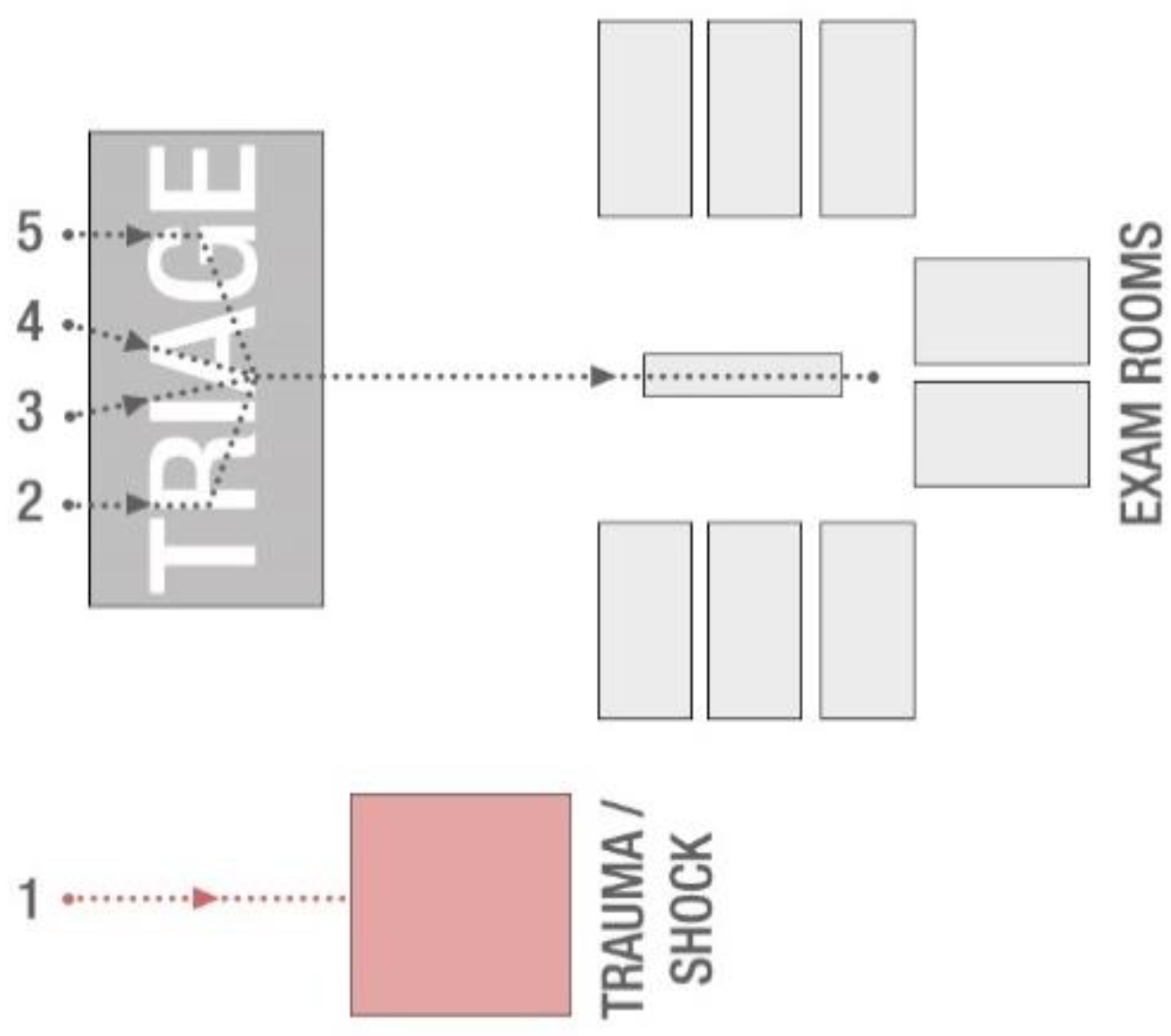
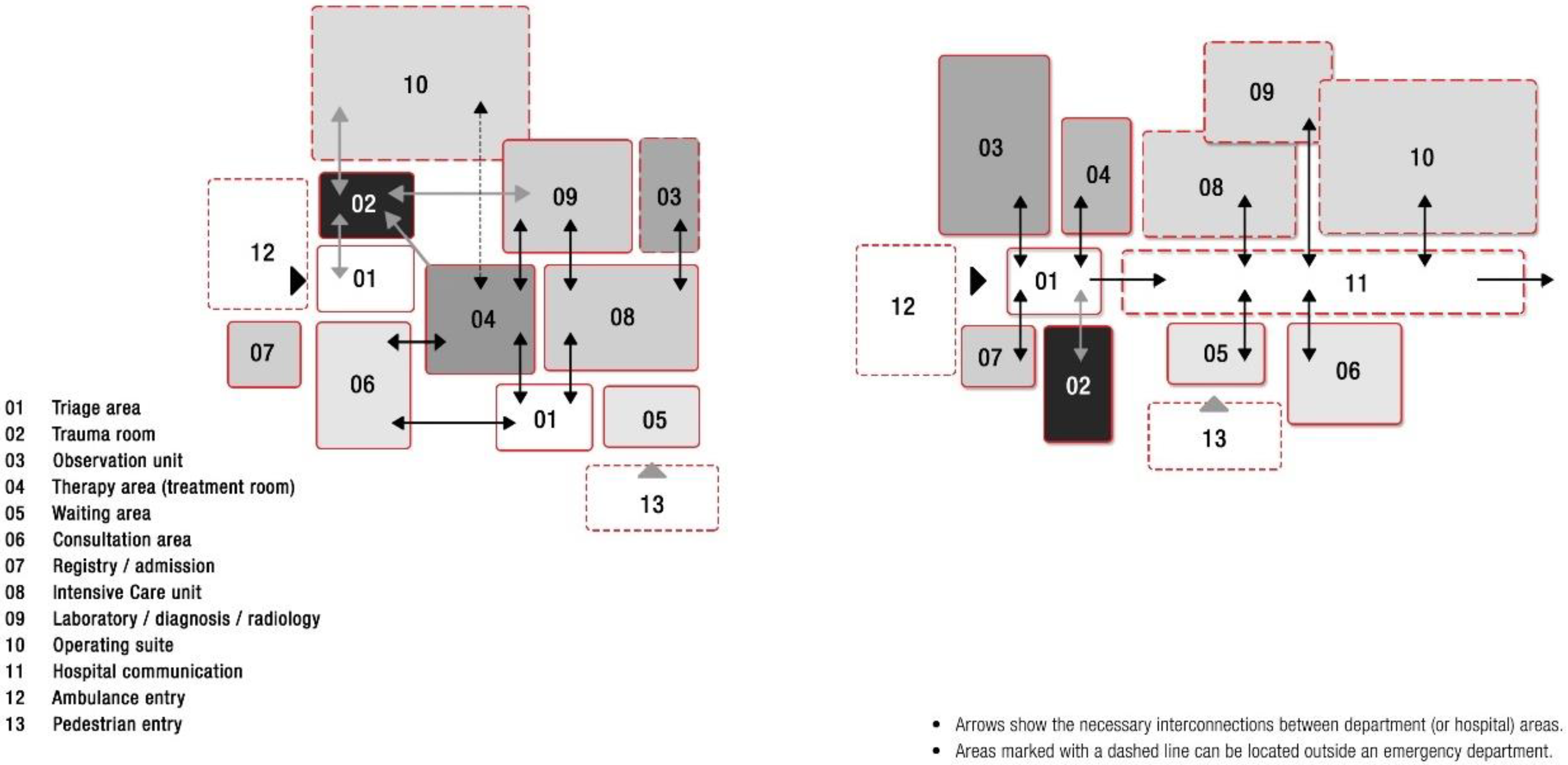
3.1.2. The Functional Layout
- −
- Lack trauma level verification by the American College of Surgeons;
- −
- Do not receive patients via ambulance diversion or transfer;
- −
- Do not have overnight beds or intensive care capabilities (mostly);
- −
- Lack inpatient referral or admissions capabilities; and
- −
- Do not have the resources to deal with large influxes of patients from natural and/or man-made disasters.
3.1.3. Structural and Technical Features
3.1.4. Design Features and Amenities
3.2. Case Studies Analysis
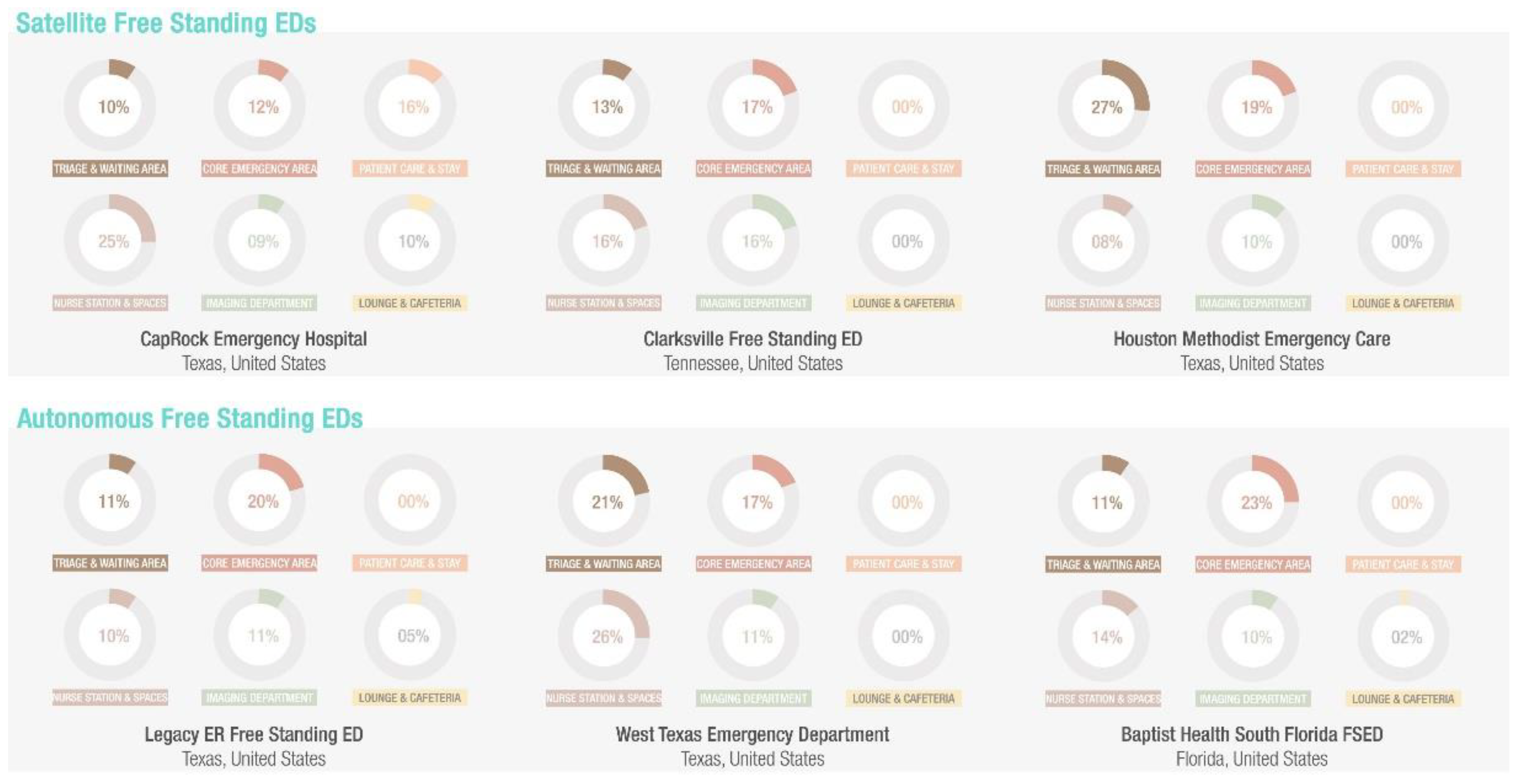
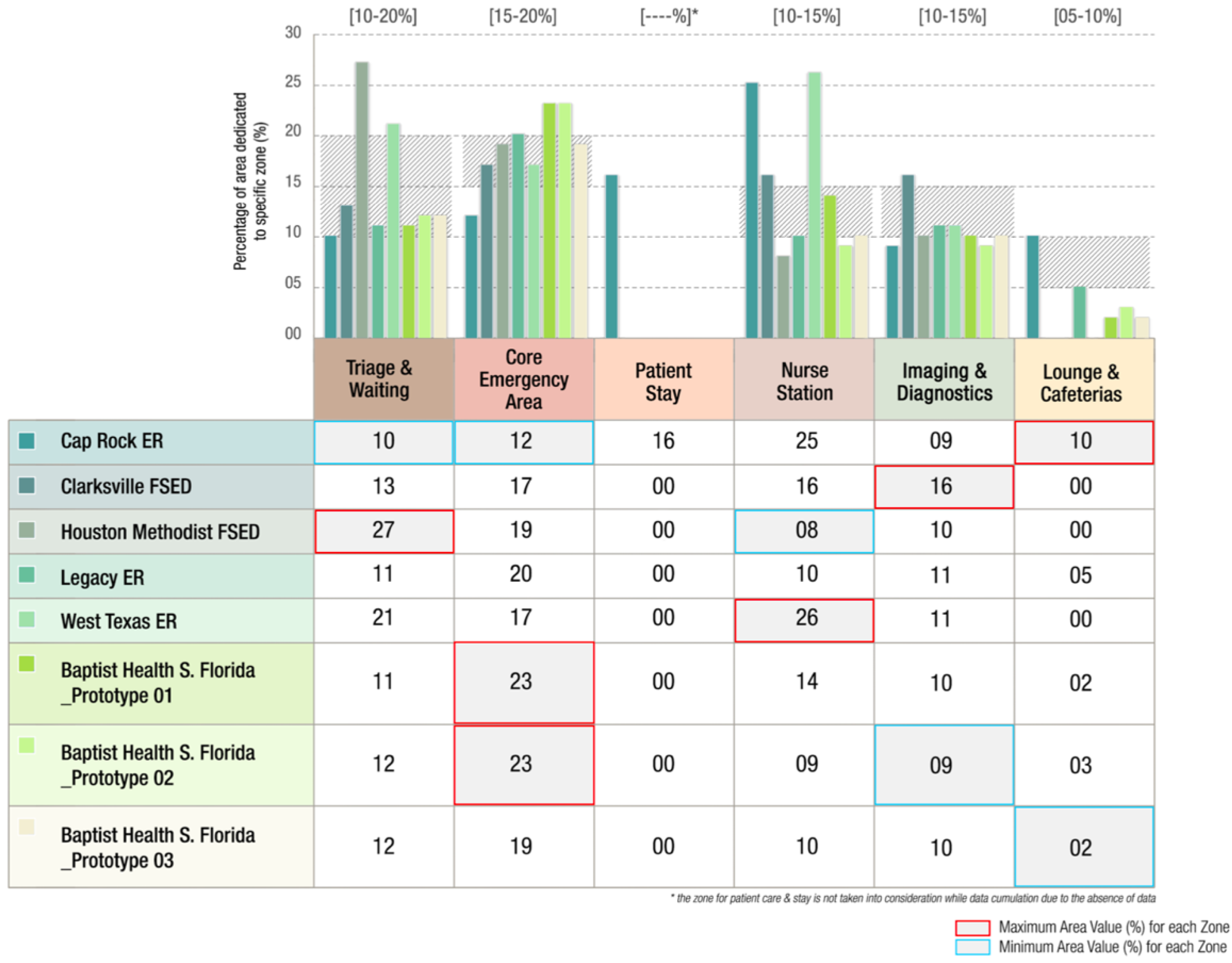
3.2.1. Area Analysis for Dedicated FSED Zones


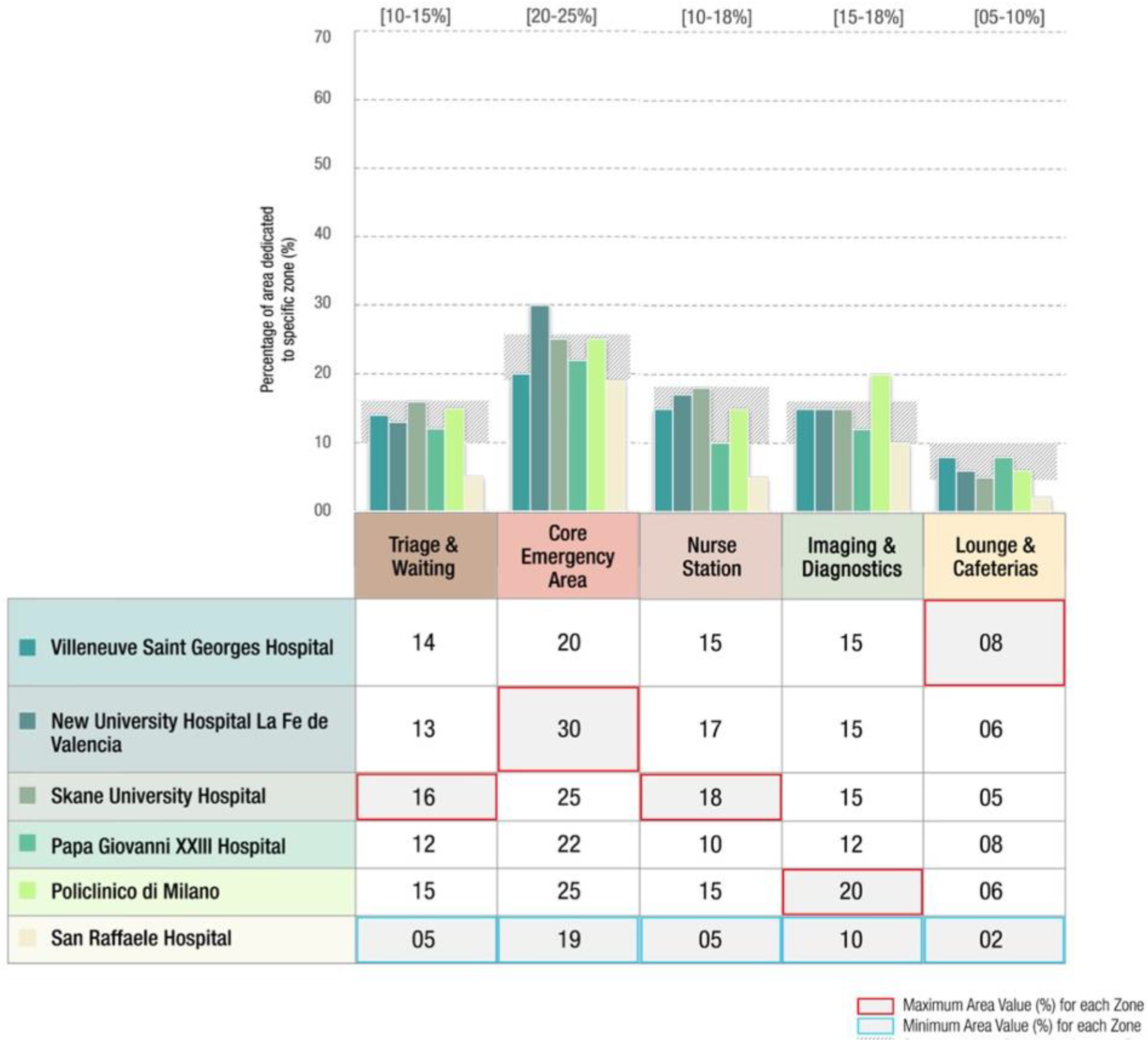
3.2.2. Area Analysis for Dedicated HBED Zones


4. Discussion and Conclusions
4.1. Research Outlooks
4.2. Conclusions
4.3. Research Limitations and Future Developments
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brambilla, A.; Lindahl, G.; Dell’Ovo, M.; Capolongo, S. Validation of a Multiple Criteria Tool for Healthcare Facilities Quality Evaluation. Facilities 2021, 39, 434–447. [Google Scholar] [CrossRef]
- Reiling, J.; Hughes, R.G.; Murphy, M.R. The Impact of Facility Design on Patient Safety. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Hughes, R.G., Ed.; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Alowad, A.; Samaranayake, P.; Ahsan, K.; Alidrisi, H.; Karim, A. Enhancing Patient Flow in Emergency Department (ED) Using Lean Strategies—An Integrated Voice of Customer and Voice of Process Perspective. BPMJ 2021, 27, 75–105. [Google Scholar] [CrossRef]
- Steptoe, A.P.; Corel, B.; Sullivan, A.F.; Camargo, C.A. Characterizing Emergency Departments to Improve Understanding of Emergency Care Systems. Int. J. Emerg. Med. 2011, 4, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayaprakash, N.; O’Sullivan, R.; Bey, T.; Ahmed, S.S. Crowding and Delivery of Healthcare in Emergency Departments: The European Perspective. West. J. Emerg. Med. 2009, 8, 233–239. [Google Scholar]
- Pines, J.M.; Hilton, J.A.; Weber, E.J.; Alkemade, A.J.; Al Shabanah, H.; Anderson, P.D.; Bernhard, M.; Bertini, A.; Gries, A.; Ferrandiz, S.; et al. International Perspectives on Emergency Department Crowding: International Perspectives On Ed Crowding. Acad. Emerg. Med. 2011, 18, 1358–1370. [Google Scholar] [CrossRef]
- Barish, R.A.; McGauly, P.L.; Arnold, T.C. Emergency Room Crowding: A Marker of Hospital Health. Trans. Am. Clin. Climatol. Assoc. 2012, 123, 304–310; discussion 310–311. [Google Scholar]
- Brambilla, A.; Morganti, A.; Lindahl, G.; Riva, A.; Capolongo, S. Complex Projects Assessment. The Impact of Built Environment on Healthcare Staff Wellbeing. In Computational Science and Its Applications—ICCSA 2020; Gervasi, O., Murgante, B., Misra, S., Garau, C., Blečić, I., Taniar, D., Apduhan, B.O., Rocha, A.M.A.C., Tarantino, E., Torre, C.M., Karaca, Y., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2020; Volume 12253, pp. 345–354. ISBN 978-3-030-58813-7. [Google Scholar]
- Sasanfar, S.; Bagherpour, M.; Moatari-Kazerouni, A. Improving Emergency Departments: Simulation-Based Optimization of Patients Waiting Time and Staff Allocation in an Iranian Hospital. Int. J. Healthc. Manag. 2021, 14, 1449–1456. [Google Scholar] [CrossRef]
- de Alwis, W. Should Freestanding Emergency Departments Be Considered in Australia?: Freestanding Emergency Departments in Australia. Emerg. Med Australas. 2019, 31, 129–134. [Google Scholar] [CrossRef] [Green Version]
- Herscovici, D.; Boggs, K.; Sullivan, A.; Camargo, C., Jr. What Is a Freestanding Emergency Department? Definitions Differ Across Major United States Data Sources. WestJEM 2020, 21, 660–664. [Google Scholar] [CrossRef]
- Schuur, J.D.; Baker, O.; Freshman, J.; Wilson, M.; Cutler, D.M. Where Do Freestanding Emergency Departments Choose to Locate? A National Inventory and Geographic Analysis in Three States. Ann. Emerg. Med. 2017, 69, 383–392.e5. [Google Scholar] [CrossRef]
- Ho, V.; Metcalfe, L.; Dark, C.; Vu, L.; Weber, E.; Shelton, G.; Underwood, H.R. Comparing Utilization and Costs of Care in Freestanding Emergency Departments, Hospital Emergency Departments, and Urgent Care Centers. Ann. Emerg. Med. 2017, 70, 846–857.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, A.F.; Bachireddy, C.; Steptoe, A.P.; Oldfield, J.; Wilson, T.; Camargo, C.A. A Profile of Freestanding Emergency Departments in the United States, 2007. J. Emerg. Med. 2012, 43, 1175–1180. [Google Scholar] [CrossRef] [PubMed]
- Morley, C.; Unwin, M.; Peterson, G.M.; Stankovich, J.; Kinsman, L. Emergency Department Crowding: A Systematic Review of Causes, Consequences and Solutions. PLoS ONE 2018, 13, e0203316. [Google Scholar] [CrossRef]
- McCarthy, M.L.; Aronsky, D.; Jones, I.D.; Miner, J.R.; Band, R.A.; Baren, J.M.; Desmond, J.S.; Baumlin, K.M.; Ding, R.; Shesser, R. The Emergency Department Occupancy Rate: A Simple Measure of Emergency Department Crowding? Ann. Emerg. Med. 2008, 51, 15–24.e2. [Google Scholar] [CrossRef] [PubMed]
- Capolongo, S.; Brambilla, A.; Girardi, A.; Signorelli, C. Validation Checklist for Massive Vaccination Centers. Ann. Di Ig. Med. Prev. E Di Comunita. 2021, 33, 513–517. [Google Scholar] [CrossRef]
- Capolongo, S.; Mauri, M.; Peretti, G.; Pollo, R.; Tognolo, C. Facilities for Territorial Medicine: The Experiences of Piedmont and Lombardy Regions. TECHNE-J. Technol. Archit. Environ. 2015, 9, 230–236. [Google Scholar] [CrossRef]
- Dell’Ovo, M.; Oppio, A.; Capolongo, S. The Location Problem. Addressing Decisions About Healthcare Facilities. In Decision Support System for the Location of Healthcare Facilities; Springer Briefs in Applied Sciences and Technology; Springer International Publishing: Cham, Switzerland, 2020; pp. 1–28. ISBN 978-3-030-50172-3. [Google Scholar]
- Gutierrez, C.; Lindor, R.A.; Baker, O.; Cutler, D.; Schuur, J.D. State Regulation Of Freestanding Emergency Departments Varies Widely, Affecting Location, Growth, And Services Provided. Health Aff. 2016, 35, 1857–1866. [Google Scholar] [CrossRef]
- Gola, M.; Brambilla, A.; Barach, P.; Signorelli, C.; Capolongo, S. Educational Challenges in Healthcare Design: Training Multidisciplinary Professionals for Future Hospitals and Healthcare. Ann. Di Ig. Med. Prev. E Di Comunita 2020, 32, 549–566. [Google Scholar] [CrossRef]
- Pati, D.; Lorusso, L.N. How to Write a Systematic Review of the Literature. HERD 2018, 11, 15–30. [Google Scholar] [CrossRef]
- Bakowski, J. A Mobile Hospital–Its Advantages and Functional Limitations. Int. J. SAFE 2016, 6, 746–754. [Google Scholar] [CrossRef]
- Kelly, D.; Pingel, M.J. Space Use and the Physical Attributes of Acute Care Units: A Quantitative Study. HERD 2022, 15, 222–238. [Google Scholar] [CrossRef] [PubMed]
- Lavy, S.; Hamilton, D.K.; Jiang, Y.; Kircher, A.; Dixit, M.K.; Lee, J.-T. Hospital Building and Departmental Area Calculation: Comparison of 36 Recent North American Projects. HERD 2019, 12, 174–185. [Google Scholar] [CrossRef] [PubMed]
- Bąkowski, J. Several Notes on Differences between American and European Model of an Emergency Department. In An Architect’s Point of View; Athens Institute for Education and Research: Athens, Greece, 2013. [Google Scholar]
- Buffoli, M.; Bellini, E.; Dell’Ovo, M.; Gola, M.; Nachiero, D.; Rebecchi, A.; Capolongo, S. Humanisation and Soft Qualities in Emergency Rooms. Ann. Dell’Istituto Super. Di Sanit. 2016, 52, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Lukens, J. Freestanding Emergency Departments: An Alternative Model for Rural Communities. 2016. The Rural Monitor. Available online: https://www.ruralhealthinfo.org/rural-monitor/freestanding-emergency-departments/ (accessed on 27 February 2022).
- Ayers, A.A. Understanding The Free Standing Emergency Department Phenomenon. J. Urg. Care Med 2017. Available online: https://www.jucm.com/understanding-the-freestanding-emergency-department-phenomenon/ (accessed on 27 February 2022).
- Rismanchian, F.; Lee, Y.H. Process Mining–Based Method of Designing and Optimizing the Layouts of Emergency Departments in Hospitals. HERD 2017, 10, 105–120. [Google Scholar] [CrossRef]
- Frascio, M.; Mandolfino, F.; Zomparelli, F.; Petrillo, A. A Cognitive Model for Emergency Management in Hospitals: Proposal of a Triage Severity Index. In Theory and Application on Cognitive Factors and Risk Management-New Trends and Procedures; Felice, F.D., Petrillo, A., Eds.; InTech: Kanagawa, Japan, 2017; ISBN 978-953-51-3295-0. [Google Scholar]
- Brunelle, A.; Henes, M.; Hu, A.; Kosovrasti, K.; Lambert, B.; Tavera, A. Freestanding Emergency Departments (FSEDs)—A Stakeholder Study. 2017. Available online: https://web.wpi.edu/Pubs/E-project/Available/E-project-050117-123753/unrestricted/Freestanding_Emergency_Department_A_Stakeholder_Study.pdf (accessed on 27 February 2022).
- Langlands, B.; Coleman, D.; Savage, T. Reimagining the ED: Ideas for Shaping the Emergency Department of the Future 2018. Facility Guidelines Institute. Available online: https://www.fgiguidelines.org/wp-content/uploads/2019/02/FGI-ReImagining-the-ED_rev.pdf (accessed on 27 February 2022).
- Burgess, L.; Kynoch, K.; Hines, S. Implementing Best Practice into the Emergency Department Triage Process. Int. J. Evidence-Based Healthc. 2019, 17, 27–35. [Google Scholar] [CrossRef]
- Zamani, Z. Effects of Emergency Department Physical Design Elements on Security, Wayfinding, Visibility, Privacy, and Efficiency and Its Implications on Staff Satisfaction and Performance. HERD 2019, 12, 72–88. [Google Scholar] [CrossRef]
- Gharaveis, A.; Kirk Hamilton, D.; Shepley, M.; Pati, D.; Rodiek, S. Design Suggestions for Greater Teamwork, Communication and Security in Hospital Emergency Departments. Indoor Built Environ. 2019, 28, 1126–1139. [Google Scholar] [CrossRef]
- Ehmann, M.R.; Kane, E.M.; Arciaga, Z.; Duval-Arnould, J.; Saheed, M. Emergency Department Ergonomic Redesign Improves Team Satisfaction in Cardiopulmonary Resuscitation Delivery: A Simulation-Based Quality Improvement Approach. J. Healthc. Qual. 2020, 42, 326–332. [Google Scholar] [CrossRef]
- Gharaveis, A.; Pati, D.; Hamilton, D.K.; Shepley, M.; Rodiek, S.; Najarian, M. The Correlation Between Visibility and Medical Staff Collaborative Communication in Emergency Departments. HERD 2020, 13, 81–97. [Google Scholar] [CrossRef]
- Tindle, K.; David, A.; Carlisle, S.; Faircloth, B.; Fields, J.M.; Hayden, G.; Ku, B. Relationship of the Built Environment on Nursing Communication Patterns in the Emergency Department: A Task Performance and Analysis Time Study. J. Emerg. Nurs. 2020, 46, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Nourazari, S.; Harding, J.; Davis, S.; Litvak, O.; Traub, S.; Sanchez, L. Are Smaller Emergency Departments More Prone to Volume Variability? WestJEM 2021, 22, 878–881. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.-W.; Yang, J.; Li, J. Generation of Hospital Emergency Department Layouts Based on Generative Adversarial Networks. J. Build. Eng. 2021, 43, 102539. [Google Scholar] [CrossRef]
- Douillet, D.; Saloux, T.; Ravon, P.; Morin, F.; Moumneh, T.; Carneiro, B.; Roy, P.M.; Savary, D. Adaptation of ED Design Layout during the COVID-19 Pandemic: A National Cross-Sectional Survey. Emerg. Med. J. 2021, 38, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Jeong, C.-H.; Jakobsen, H.C.W. Influence of Architectural Layouts on Noise Levels in Danish Emergency Departments. J. Build. Eng. 2021, 42, 102449. [Google Scholar] [CrossRef]
- MohammadiGorji, S.; Bosch, S.J.; Valipoor, S.; De Portu, G. Investigating the Impact of Healthcare Environmental Design on Staff Security: A Systematic Review. HERD 2021, 14, 251–272. [Google Scholar] [CrossRef] [PubMed]
- Brambilla, A.; Sun, T.; Elshazly, W.; Ghazy, A.; Barach, P.; Lindahl, G. Flexibility during the COVID-19 Pandemic Response: Healthcare Facility Assessment Tools for Resilient Evaluation. Int. J. Environ. Res. Public Health 2021, 18, 1478. [Google Scholar] [CrossRef]
- Hartigan, L.; Cussen, L.; Meaney, S.; O’Donoghue, K. Patients’ Perception of Privacy and Confidentiality in the Emergency Department of a Busy Obstetric Unit. BMC Health Serv. Res. 2018, 18, 978. [Google Scholar] [CrossRef]
- Capolongo, S.; Bellini, E.; Nachiero, D. Soft Qualities in Healthcare Method and Tools for Soft Qualities Design in Hospitals’ Built Environments. Ann. Di Ig. Med. Prev. E Di Comunità 2014, 26, 391–399. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Type | Location | Year | Area Sqm |
|---|---|---|---|---|
| Cap-Rock Emergency Hospital | FSED-Satellite | USA | 2018 | 1928 |
| Clarksville Freestanding Emergency Department | FSED-Satellite | USA | 2017 | 1022 |
| Huston Methodist Emergency care Centre | FSED-Satellite | USA | 2014 | 892 |
| Legacy ER Freestanding Emergency Department | FSED-Autonomus | USA | 2013 | 785 |
| West Texas Emergency Department | FSED-Autonomus | USA | 2014 | 600 |
| Baptist Health South Florida FSED | FSED-Autonomus | USA | 2019 | 1730 |
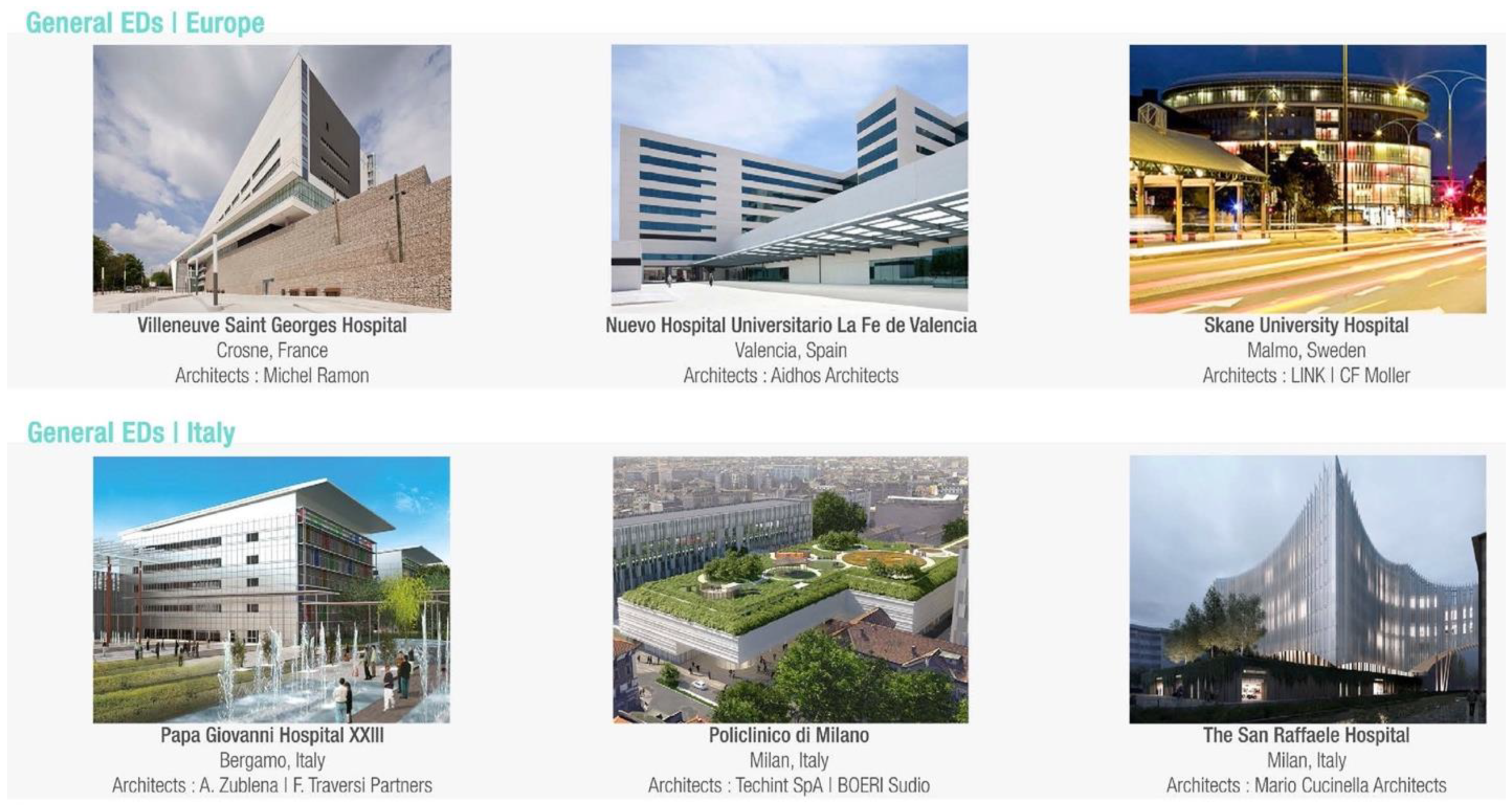
| Villeneuve-Saint-Georges Hospital | HED-Europe | FRANCE | 2012 | 17,800 (hospital) |
| New University Hospital La Fe de Valencia | HED-Europe | SPAIN | 2010 | 260,400 (hospital) |
| Skane University Hospital Malmo | HED-Europe | SWEDEN | 2010 | 25,800 (hospital) |
| Papa Giovanni XXIII Bergamo | HED-Italy | ITALY | 2012 | 5580 |
| Policlinico di Milano | HED-Italy | ITALY | On Going | 70,000 (hospital) |
| San Raffaele Hospital Milano | HED-Italy | ITALY | 2021 | 6752 |
| N° | Authors | Title | Year |
|---|---|---|---|
| 1 | Bąkowski J | Several notes on differences between American and European model of an emergency department. An architect’s point of view [26] | 2014 |
| 2 | Buffoli M, Bellini E, Dell’Ovo M, Gola M, Nachiero D, Rebecchi A, Capolongo S | Humanization and soft qualities in emergency rooms [27] | 2016 |
| 3 | Lukens J | Freestanding Emergency Departments: An Alternative Model for Rural Communities [28] | 2016 |
| 4 | Ayers AA | Understanding the Free Standing Emergency Department Phenomenon [29] | 2016 |
| 5 | Schuur JD, Baker O, Freshman J, Wilson M, Cutler DM | Where Do Freestanding Emergency Departments Choose to Locate? A National Inventory and Geographic Analysis in Three States [12] | 2016 |
| 6 | Rismanchian F, Lee HY | Process Mining–Based Method of Designing and Optimizing the Layouts of Emergency Departments in Hospitals [30] | 2016 |
| 7 | Frascio M, Mandolfino F, Zomparelli F, Petrillo A | A Cognitive Model for Emergency Management in Hospitals: Proposal of a Triage Severity Index [31] | 2017 |
| 8 | Brunelle A, Henes M, Hu A, Kosovrasti K, Lambert B, Tavera, A | Freestanding Emergency Departments (FSEDs)—A Stakeholder Study [32] | 2017 |
| 9 | Langlands B, Coleman D, Savage T | Reimagining the ED:Ideas for Shaping the Emergency Department of the Future [33] | 2018 |
| 10 | Hartigan L, Cussen L, Meaney S, O’Donoghue K | Patients’ perception of privacy and confidentiality in the emergency department of a busy obstetric unit | 2018 |
| 11 | Burgess L, Kynoch K, Hines S | Implementing best practice into the emergency department triage process [34] | 2019 |
| 12 | Zamani, Z | Effects of Emergency Department Physical Design Elements on Security, Way-finding, Visibility, Privacy, and Efficiency and Its Implications on Staff Satisfaction and Performance [35] | 2019 |
| 13 | Gharaveis A, Hamilton DK, Shepley M, Pati D, Rodiek S | Design suggestions for greater teamwork, communication and security in hospital emergency departments [36] | 2019 |
| 14 | Sasanfar S, Bagherpour M, Moatari-Kazerouni A | Improving emergency departments: Simulation-based optimization of patients waiting time and staff allocation in an Iranian hospital [9] | 2020 |
| 15 | Ehmann MR, Erin KM., Zakk A, Jordan D, Mustapha S | Emergency Department Ergonomic Redesign Improves Team Satisfaction in Cardiopulmonary Resuscitation Delivery: A Simulation-Based Quality Improvement Approach [37] | 2020 |
| 16 | Gharaveis A, Pati D, Hamilton DK, Shepley M, Rodiek S, Najarian M | The Correlation Between Visibility and Medical Staff Collaborative Communication in Emergency Departments [38] | 2020 |
| 17 | Tindle K, David A, Carlisle S, Faircloth B, Fields JM, Hayden G, Ku B. | Relationship of the Built Environment on Nursing Communication Patterns in the Emergency Department: A Task Performance and Analysis Time Study [39] | 2020 |
| 18 | Nourazari S, Harding JW, Davis SR, Litvak O, Traub SJ, Sanchez LD | Are Smaller Emergency Departments More Prone to Volume Variability? [40] | 2021 |
| 19 | Zhao-Wang Z, Jian Y, Jiatong L, | Generation of hospital emergency department layouts based on generative adversarial networks [41] | 2021 |
| 20 | Douillet D, Saloux T, Ravon P | Adaptation of ED design layout during the COVID-19 pandemic: a national cross-sectional survey [42] | 2021 |
| 21 | Jeong C, Jakobsen HCW | Influence of architectural layouts on noise levels in Danish emergency departments [43] | 2021 |
| 22 | Alowad A, Samaranayake P, Ahsan K, Alidrisi, Karim A | Enhancing patient flow in emergency department (ED) using lean strategies–an integrated voice of customer and voice of process perspective [3] | 2021 |
| 23 | MohammadiGorji S, Bosch SJ, Valipoor S, De Portu G | Investigating the Impact of Healthcare Environmental Design on Staff Security: A Systematic Review [44] | 2021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brambilla, A.; Mangili, S.; Das, M.; Lal, S.; Capolongo, S. Analysis of Functional Layout in Emergency Departments (ED). Shedding Light on the Free Standing Emergency Department (FSED) Model. Appl. Sci. 2022, 12, 5099. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105099
Brambilla A, Mangili S, Das M, Lal S, Capolongo S. Analysis of Functional Layout in Emergency Departments (ED). Shedding Light on the Free Standing Emergency Department (FSED) Model. Applied Sciences. 2022; 12(10):5099. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105099
Chicago/Turabian StyleBrambilla, Andrea, Silvia Mangili, Mohana Das, Sanchit Lal, and Stefano Capolongo. 2022. "Analysis of Functional Layout in Emergency Departments (ED). Shedding Light on the Free Standing Emergency Department (FSED) Model" Applied Sciences 12, no. 10: 5099. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105099