1. Introduction
Similar to other cutaneous lesions with malignant transformation potential, keratoacanthoma represents one of the pathologies with a negative impact on public health systems; a significant increase in the number of cases diagnosed is being reported worldwide. It is described and classified by Schartz et al. as a premalignant precursor lesion of squamous cell carcinoma of the skin, one of the most aggressive oncological pathologies developed in epithelial tissues. At the same time, the latest studies also support the idea that keratoacanthoma is a type of carcinoma in situ. Although some meta-analyses of the last decade indicate an average of about 12%, data on the risk rate of malignant transformation are contradictory and incompletely elucidated [
1,
2,
3,
4].
The non-specific symptomatology of these lesion types negatively influences referral to specialist clinics making it impossible to accurately and completely quantify the risk of malignancy in the early stages of progression. In addition, clinical studies reveal the phenotypic and morphological variability of these lesions, a variability conditioned and determined by the action of highly heterogeneous etiopathogenic mechanisms [
5,
6,
7].
The identification and description of the cellular and molecular characteristics of keratoacanthomatous lesions facilitates the understanding of pathogenic mechanisms specific to the early stages of epidermal carcinogenesis [
2,
7,
8].
Over the years, in the case of keratoacanthoma (molluscum sebaceum) the histopathological examination, considered the “gold-standard” in establishing the diagnosis, describes several aspects, depending on its evolution. Thus, at onset, a marked proliferation of the epidermis, acanthosis, dyskeratotic cells, with a reduced degree of keratinisation and inflammatory infiltrate in the dermis underlying the lesion are revealed. During the stability period, a differential diagnosis between keratoacanthoma and well-differentiated squamous cell carcinoma remains difficult [
3,
6,
9].
Photon microscopy, the resolution power of which is limited, does not always reveal features suggestive of epithelial lesions with mild-to-moderate dysplasia. Thus, there may be cases in which carcinomas develop on dysplastic lesions undiagnosed or unidentified in previous biopsies [
4,
6,
10].
Epithelial-mesenchymal transition (EMT) is a key time process in malignant transformation. At this stage, epithelial cells acquire morphological characteristics of fibroblasts through a process regulated by dermal-epidermal interactions. These interactions condition cell growth and differentiation in the epidermis. As early as 1981, Komitowshy et al. observed that during premalignant hyperplasia, defined as epidermal hyperplasia progressing to carcinoma, basal layer keratinocytes maintain their normal architecture, with disorganization of intercellular coupling structures and enlargement of intercellular spaces [
9,
10,
11,
12].
Starting from all the aspects mentioned above, the present study aims to evaluate the evolutionary potential of keratoacanthoma lesions by describing the tissue microenvironment at the ultrastructural level, revealing the cellular interactions involved in the staging and efficiency of diagnostic and therapeutic protocols.
2. Materials and Methods
To achieve the objectives of the present research, 25 female patients, aged 45–60 years, non-smokers and without chronic ethanol consumption, clinically and histopathologically diagnosed with keratoacanthoma, were enrolled. Lesions were excisionally biopsied in healthy tissue.
All surgical therapeutic interventions were preceded by an individual informed consent, as required by law.
The pathological diagnosis was performed in the Pathological Anatomy and Forensic Department of the C.F. Clinical Hospital Iași and in the Pathological Anatomy Laboratory of “Dr. I. Chizac” Military Emergency Hospital, Iași.
After rapid harvesting on ice and the use of a few drops of 2% glutaraldehyde, the tissue preparations were processed following the standard transmission electron microscopy (TEM) technique protocol: prefixation with 2% glutaraldehyde in PBS at 4 °C for 2 h, overnight wash in PBS at 4 °C, postfixation with 1% osmium tetroxide in PBS at 4 °C for 1 h, wash in PBS for 2 h, dehydration with 30% alcohol at 4 °C for 15 min, block staining with 2% uranyl acetate in 30% alcohol at 4 °C for 45 min, dehydration with 30% alcohol at 4 °C for 15 min, 50% alcohol at 4 °C for 15 min, 70% alcohol at 4 °C overnight, 90% alcohol at room temperature for 15 min, 100% alcohol at room temperature for 20 min, absolute acetone at room temperature for 20 min.
After impregnation and embedding in EPON 812, in gelatin capsules, the samples were phased and sectioned with Leica ultramicrotome in the Electron Microscopy Laboratory of the Cell and Molecular Biology Department, “Grigore T. Popa” University of Medicine and Pharmacy, Iași. Examination of the sections was performed in the Electron Microscopy Laboratory of the Institute of Life Sciences, “Vasile Goldiș” Western University, Arad, and the Electron Microscopy Laboratory, UAIC, Iași.
3. Results
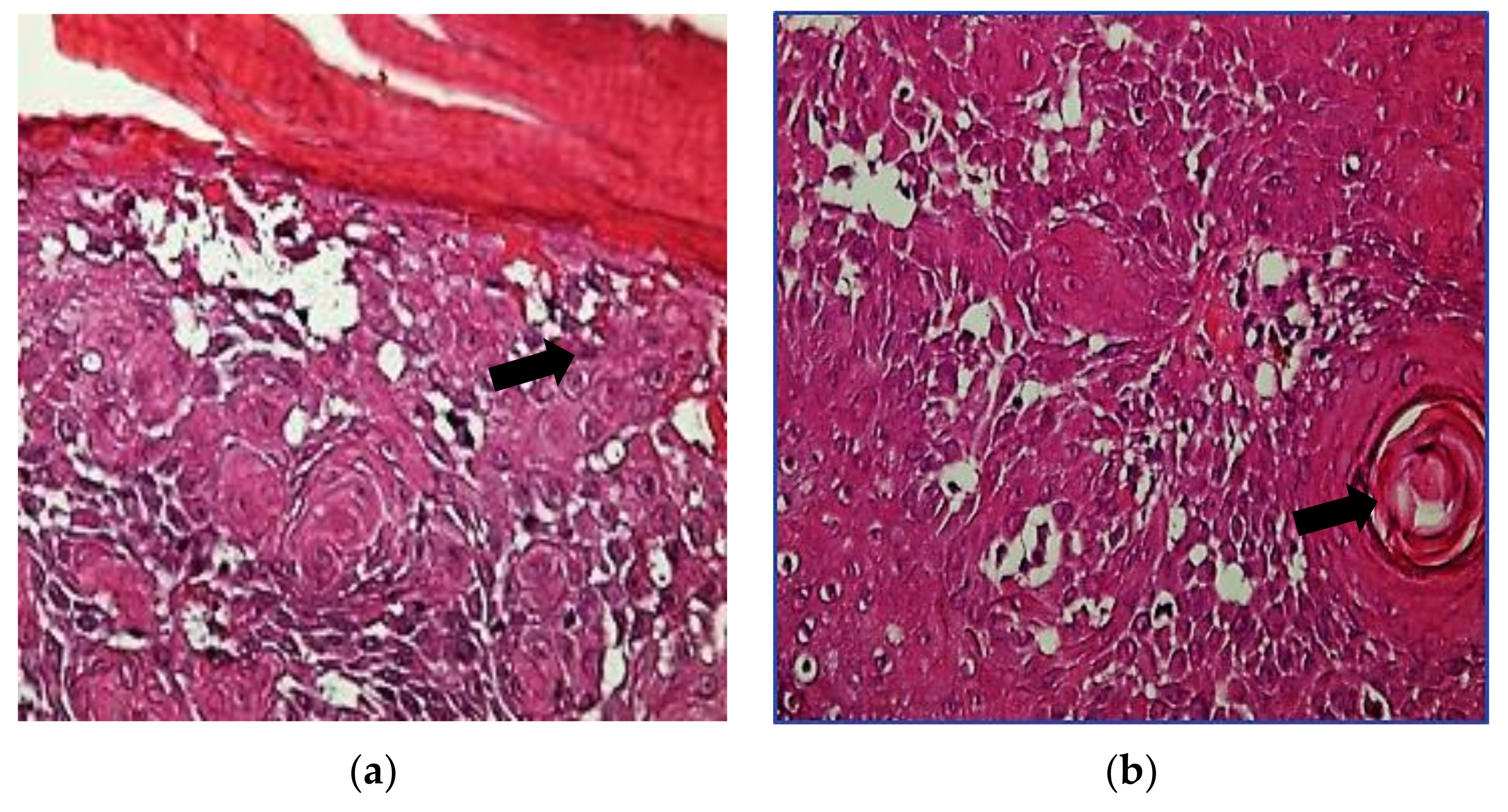
Photon microscopy examination of hmatoxylin-eosin (HE) stained sections using the Olympus BX40 optical microscope with attached Olympus E330 camera identified a number of aspects suggestive of the diagnosis of keratoacanthoma—epidermis with the presence of horny plugs formed by keratin lamellae between which polymorphonuclear cells were detected. The epidermis showed significant acanthosis, papillomatosis, rare horny cysts, and pseudoepitheliomatous aspects and, in the superficial dermis, an abundant polymorphous inflammatory infiltrate was identified (
Figure 1).
Complementary to the histopathological examination,
electron microscopic examination of keratoacanthoma lesions with a mild-to-moderate degree of dysplasia revealed the following ultrastructural details (
Figure 2):
- -
at the cytoplasmic level—there are numerous types of vacuoles with heterogeneous appearance among which vesicles specific to classical endocytosis but also to fluid phase micropinocytosis can be found. In all keratinocyte layers, nuclei are enlarged in volume and irregularly shaped by undulation and edentulousness of the nuclear envelope. In contrast to basal layers, in suprabasal layers the number of mitochondria, responsible for cellular energetics, progressively increases and the matrix shows a smooth, vacuolated appearance through reduction and disorganization of mitochondrial ridges, with negative influence on cellular metabolic processes. Organelles specialised in cell synthesis and secretion such as ribosomes, the rough endoplasmic reticulum (RER) and the Golgi apparatus are hypertrophied, especially in perivascular macrophages;
- -
at the cytoskeletal level—tonofilaments are reduced in number and grouped into short clusters located at a distance from the plasmalemma;
- -
at the membrane level—cell–cell adhesion junctional complexes are disorganized inducing acantholysis and widening of intercellular spaces. At the basal pole level, both basement membrane discontinuity and hemidesmosome disruption are identified, with damage to the extracellular matrix.
Compared to the lesions described above, in keratoacanthomas associated with a moderate-severe degree of dysplasia there is both an increase in the frequency and intensity of the ultrastructural changes mentioned above and additional details such as (
Figure 3 and
Table 1):
- -
at the cytoplasmic level—the keratinocyte nuclei of all epidermal layers were strongly edentated by the cytoplasmic invaginations associated with nuclear pore expansion. Enlargement of the perinuclear cisterna imprints the vacuolar appearance of the nuclear envelope. Characteristic of tumour cells, these nuclei have multiple, bulky, peripherally arranged nucleoli. Ribosomes and mitochondria have a degenerative appearance;
- -
at the cytoskeletal level—much thickened tonofilaments are arranged perinuclearly, in a large electron-dense clusters, leading to cytoplasmic membrane invagination and destructuring of desmosomes and hemidesmosomes;
- -
at the membrane level—discontinuities are more frequent and more extensive.
4. Discussion
At the epidermal level the concept that the development of cutaneous squamous cell carcinoma requires two stages indicates the initial presence of a precursor, a premalignant lesion. Thus, a key factor in the prognosis of this pathology is, for both doctors and patients, correct, complete, specific, and early diagnosis and treatment [
1,
5,
6,
7,
12].
Among the most common cutaneous epithelial lesions with increased potential for malignancy, keratoacanthomas have also been identified. Some studies show that more than 50% of dysplastic skin lesions show changes characteristic of squamous cell carcinoma at diagnosis [
2,
3,
4,
10,
13].
The many clinical features described in the literature are matched by a variety of histopathological types, confirming the importance of pathological examination both in the diagnosis of these lesions and in the identification of malignant potential [
10,
11,
12,
13,
14]. In the present work, examination under photon microscopy using the usual Hematoxylin–Eosin staining objectified a number of morphological features important for the establishment of the diagnosis of keratoacanthoma (
Figure 1).
As for epithelial dysplasia, the histopathological diagnosis is subjective depending very much on the experience of the pathologist. In addition, not all dysplastic lesions progress to malignancy [
8,
10,
11,
12,
13,
14].
The severity of dysplastic lesions analysed from a histopathological perspective were confirmed and the detailed electron-microscope studies revealed at the same time the information necessary to elucidate the etiopatogenic factors involved in epithelial carcinogenesis. Thus, in all the lesions studied, the action of ultraviolet radiation as a predisposing and promoting factor of carcinomatous transformation is supported by the polymorphic aspects of the keratinocyte nuclei, nuclei that occupy more than 60% of the cell surface (
Figure 2 and
Figure 3) [
11,
12,
13,
14,
15].
The study group consisted only of female patients who did not have living and working conditions conducive to the development of premalignant and malignant lesions. From this fact, we can conclude that it is necessary to investigate morphological correlations with molecular ones in order to characterize, at ultrastructural level, the tissue microenvironment that conditions the evolution and prognosis of these lesions [
11,
12,
13,
14,
15].
In order to maintain and restore tissue homeostasis, the epidermal epithelium is in constant communication with the underlying structures, from which it is separated by a dynamic structure represented mainly by the basement membrane, a component of the extracellular matrix. This entity can be characterised in detail using more sensitive and specific techniques such as transmission electron microscopy. Thus, in our study we identify thickness varieties, with the presence of residual material in the lamina propria, discontinuities of the basement membrane, aspects directly correlated proportionally with the degree of dysplasia and with the initiation and evolution of the epithelial-mesenchymal transition (
Figure 2 and
Figure 3). All these changes are the result of inflammation–cancer interdependence, supporting thus the hypothesis of Rudolf Virchow et al. that tumour lesions develop in inflammatory areas generically referred to as “lymphoreticular infiltration”. In addition, these aspects draw attention to the initiation of carcinogenesis imprecisely identified and characterized by light microscopy [
7,
14,
15,
16,
17].
Similar to the inflammatory lesions studied and presented in the literature, the substrate of the regulatory action of various biomarkers indicated and used by various experimental studies can be demonstrated by electron microscopy in these keratoacanthomas. Therefore, enlargement and vacuolization of the perinuclear cisternae, with disorganization of the protein complexes underlying the nuclear pore structure, certifies deregulation of transcriptional and posttranslational mechanisms involved in cell proliferation and growth [
17,
18,
19,
20,
21]. Also, degenerating aspects of mitochondrial ridges draw attention to perturbations of the oxidative systems responsible for the efficient control of all cellular metabolisms and represent the morphological profile of the imbalance of pro- and anti-apoptotic coregulatory mechanisms (
Figure 3).
The increase in the number of ribosomes, independent of the degree of lesional dysplasia, correlates with the intensity of the inflammatory process of these lesions under study (
Figure 2 and
Figure 3).
Similar to other epithelial lesions associated with a moderate-severe degree of dysplasia, the present study lesions also showed the presence of a large number of macrophages that pre-suppressed the rough endoplasmic reticulum and the Golgi complex, thus supporting the intensity of the action of proinflammatory molecules. At the same time, the reduction in the number and the altered distribution of microtubules indicate possible perturbations of constitutive synthesis and secretion pathways (
Figure 2 and
Figure 3) [
20,
21,
22].
An important role in defining tissue architecture is attributed to cell-cell and cell-extracellular matrix junctional complexes. According to experimental studies in epithelial thymic sutures, increased migratory capacity of tumour cells correlates directly with the degree of disorganization or absence of desmosomes and hemidesmosomes [
21,
22,
23,
24,
25]. It is also obvious that the separation of tonofilaments from desmosomal plaques correlates with focal or total dyskeratosis, which is also confirmed by the results of this study (
Figure 3).
5. Conclusions
Transmission electron microscopy provided a number of additional details that could not be observed in photon microscopy, which are ultrastructural aspects important for the evolution of keratoacanthomas. This indicates the importance of complementing the classical anatomopathological diagnosis with electron microscopic examination in order to obtain a certain diagnosis and to establish a correct prognosis of these lesions.
The practical applicability of the electron-microscopic aspects captured in the present study can be quantified both in determining the clinical and therapeutic evolution and in calculating the recurrent risk by characterizing the perilesional cancerization field. Moreover, this ultrastructural diagnosis can more accurately assess the severity of adverse effects associated with current therapeutic regimens.
The skin lesions studied have an unpredictable clinical course and are considered by some authors to be at low risk of malignant transformation. The results presented in this research reveal the increased prevalence of important ultrastructural changes, some even specific to tumour cells, supporting the terminology of premalignant lesions and revealing the value of electronomicroscopic examination. Thus, the importance of reassessing the severity of keratoacanthoma lesions and the need to implement a system for early detection of their malignant transformation is emphasized.
The data obtained by examining the samples in photon and electron microscopy provide a complete and relevant picture of the specific morphological context of these changes, while experimental studies of molecular biomarkers indicated by multiple cellular and molecular biology studies will complete this picture, providing important information for the clinical and therapeutic management of these lesions.
Author Contributions
Conceptualization, D.T.-O. and E.-C.C.; methodology, P.B.; software, P.O. and I.F.; validation, L.S., C.D.D. and A.-E.B.; formal analysis, V.-B.G.; investigation, P.B.; resources, D.T.-O.; data curation, D.T.-O.; writing—original draft preparation, D.T.-O.; writing—review and editing, P.B. and I.F.; visualization, V.-B.G.; supervision, E.-C.C.; project administration, D.T.-O.; funding acquisition, E.-C.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Laikova, K.V.; Oberemok, V.V.; Krasnodubets, A.M.; Gal’chinsky, N.V.; Useinov, R.Z.; Novikov, I.A.; Temirova, Z.Z.; Gorlov, M.V.; Shved, N.A.; Kumeiko, V.V.; et al. Advances in the Understanding of Skin Cancer: Ultraviolet Radiation, Mutations, and Antisense Oligonucleotides as Anticancer Drugs. Molecules 2019, 24, 1516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayhan, E.; Ucmak, D.; Akkurt, Z. Vascular structures in dermoscopy. An. Bras. Dermatol. 2015, 90, 545–553. [Google Scholar] [CrossRef] [PubMed]
- Claeson, M.; Pandeya, N.; Dusingize, J.C.; Thompson, B.S.; Green, A.C.; Neale, R.E.; Olsen, C.M.; Whiteman, D.C. Assessment of Incidence Rate and Risk Factors for Keratoacanthoma Among Residents of Queensland, Australia. JAMA Dermatol. 2020, 156, 1324–1332. [Google Scholar] [CrossRef] [PubMed]
- Pancevski, G.; Pepic, S.; Idoska, S.; Tofoski, G.; Nikolovska, S. Topical Imiquimod 5% as a Treatment Option in Solitary Facial Keratoacanthoma. Open Access Maced. J. Med. Sci. 2018, 6, 531–535. [Google Scholar] [CrossRef] [Green Version]
- Panagiotopoulos, A.; Kyriazis, N.; Polychronaki, E.; Leotsakos, G.D.; Vassis, P.; Rigopoulos, D. The Effectiveness of Cryosurgery Combined with Curettage and Electrodessication in the Treatment of Keratoacanthoma: A Retrospective Analysis of 90 Cases. Indian J. Dermatol. 2020, 65, 406–408. [Google Scholar]
- Cotrutz, C.E.; Temelie-Olinici, D. Molecular and cell biology translational researches in the management of oral premalignant lesions. Med. Surg. J. 2019, 123, 7–10. [Google Scholar]
- Amagai, R.; Fujimura, T.; Kambayashi, Y.; Furudate, S.; Sato, Y.; Tanita, K.; Hashimoto, A.; Aiba, S. Keratoacanthoma Centrifugum Marginatum with Spontaneous Regression and Its Possible Differential Diagnosis. Case Rep. Oncol. 2018, 11, 671–675. [Google Scholar] [CrossRef]
- Wolner, Z.J.; Yélamos, O.; Liopyris, K.; Rogers, T.; Marchetti, M.A.; Marghoob, A.A. Enhancing Skin Cancer Diagnosis with Dermoscopy. Dermatol. Clin. 2017, 35, 417–437. [Google Scholar] [CrossRef]
- Michalak-Stoma, A.; Małkińska, K.; Krasowska, D. Usefulness of Dermoscopy to Provide Accurate Assessment of Skin Cancers. Clin. Cosmet. Investig. Dermatol. 2021, 14, 733–746. [Google Scholar] [CrossRef]
- Condurache Hritcu, O.M.; Botez, A.E.; Olinici, D.T.; Onofrei, P.; Stoica, L.; Grecu, V.B.; Toader, P.M.; Gheucă-Solovăstru, L.; Cotrutz, E.C. Molecular markers associated with potentially malignant oral lesions (Review). Exp. Ther. Med. 2021, 22, 1–5. [Google Scholar] [CrossRef]
- Porumb-Andrese, E.; Scutariu, M.M.; Luchian, I.; Schreiner, T.G.; Mârţu, I.; Porumb, V.; Popa, C.G.; Sandu, D.; Ursu, R.G. Molecular Profile of Skin Cancer. Appl. Sci. 2021, 11, 9142. [Google Scholar] [CrossRef]
- Queen, D.; Shen, Y.; Trager, M.H.; Lopez, A.T.; Samie, F.H.; Lewin, J.M.; Niedt, G.W.; Geskin, L.J.; Liu, L. UV biomarker genes for classification and risk stratification of cutaneous actinic keratoses and squamous cell carcinoma subtypes. FASEB J. 2020, 34, 13022–13032. [Google Scholar] [CrossRef]
- Fania, L.; Didona, D.; Di Pietro, F.R.; Verkhovskaia, S.; Morese, R.; Paolino, G.; Donati, M.; Ricci, F.; Coco, V.; Ricci, F.; et al. Cutaneous Squamous Cell Carcinoma: From Pathophysiology to Novel Therapeutic Approaches. Biomedicines 2021, 9, 171. [Google Scholar] [CrossRef]
- Kwiek, B.; Schwartz, R.A. Keratoacanthoma (KA): An update and review. J. Am. Acad. Dermatol. 2016, 74, 1220–1233. [Google Scholar] [CrossRef]
- Yesantharao, P.; Wang, W.; Ioannidis, N.M.; Demehri, S.; Whittemore, A.S.; Asgari, M.M. Cutaneous squamous cell cancer (cSCC) risk and the human leukocyte antigen (HLA) system. Hum. Immunol. 2017, 78, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Corchado-Cobos, R.; García-Sancha, N.; González-Sarmiento, R.; Pérez-Losada, J.; Cañueto, J. Cutaneous Squamous Cell Carcinoma: From Biology to Therapy. Int. J. Mol. Sci 2020, 21, 2956. [Google Scholar] [CrossRef]
- Ishitsuka, Y.; Hanaoka, Y.; Tanemura, A.; Fujimoto, M. Cutaneous Squamous Cell Carcinoma in the Age of Immunotherapy. Cancers 2021, 13, 1148. [Google Scholar] [CrossRef]
- Voiculescu, V.M.; Lisievici, C.V.; Lupu, M.; Vajaitu, C.; Draghici, C.C.; Popa, A.V.; Solomon, I.; Sebe, T.I.; Constantin, M.M.; Caruntu, C. Mediators of Inflammation in Topical Therapy of Skin Cancers. Mediat. Inflamm. 2019, 2019, 8369690. [Google Scholar] [CrossRef] [Green Version]
- Ursu, R.G.; Luchian, I.; Ghetu, N.; Costan, V.V.; Stamatin, O.; Palade, O.D.; Damian, C.; Iancu, L.S.; Porumb-Andrese, E. Emerging Oncogenic Viruses in Head and Neck Cancers from Romanian Patients. Appl. Sci. 2021, 11, 9356. [Google Scholar] [CrossRef]
- Vîlcea, A.M.; Stoica, L.E.; Georgescu, C.V.; Popescu, F.C.; Ciurea, R.N.; Vîlcea, I.D.; Mirea, C.S. Clinical, histopathological and immunohistochemical study of keratoacanthoma. Rom. J. Morphol. Embryol. 2021, 62, 445–456. [Google Scholar] [CrossRef]
- Ogita, A.; Ansai, S.I.; Misago, N.; Anan, T.; Fukumoto, T.; Saeki, H. Histopathological diagnosis of epithelial crateriform tumors: Keratoacanthoma and other epithelial crateriform tumors. J. Dermatol. 2016, 43, 1321–1331. [Google Scholar] [CrossRef] [PubMed]
- Dunn, A.; Kleinfelder, R.E.; Glick, B.P. Intravascular Basal Cell Carcinoma Hiding under a Keratoacanthoma. Case Rep. Dermatol. 2021, 13, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Wagner, V.P.; Martins, M.D.; Dillenburg, C.S.; Meurer, L.; Castilho, R.M.; Squarize, C.H. Histogenesis of keratoacanthoma: His-tochemical and immunohistochemical study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 310–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gleich, T.; Chiticariu, E.; Huber, M.; Hohl, D. Keratoacanthoma: A distinct entity? Exp. Derm. 2016, 25, 85–91. [Google Scholar] [CrossRef] [Green Version]
- Ra, S.H.; Su, A.; Li, X.; Zhou, J.; Cochran, A.J.; Kulkarni, R.P.; Binder, S.W. Keratoacanthoma and squamous cell carcinoma are distinct from a molecular perspective. Mod. Pathol. 2015, 28, 799–806. [Google Scholar] [CrossRef] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 



{kind=link}
{kind=link}
{kind=link}