
Augmented Reality-Assisted Percutaneous Pedicle Screw Instrumentation: A Cadaveric Feasibility and Accuracy Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
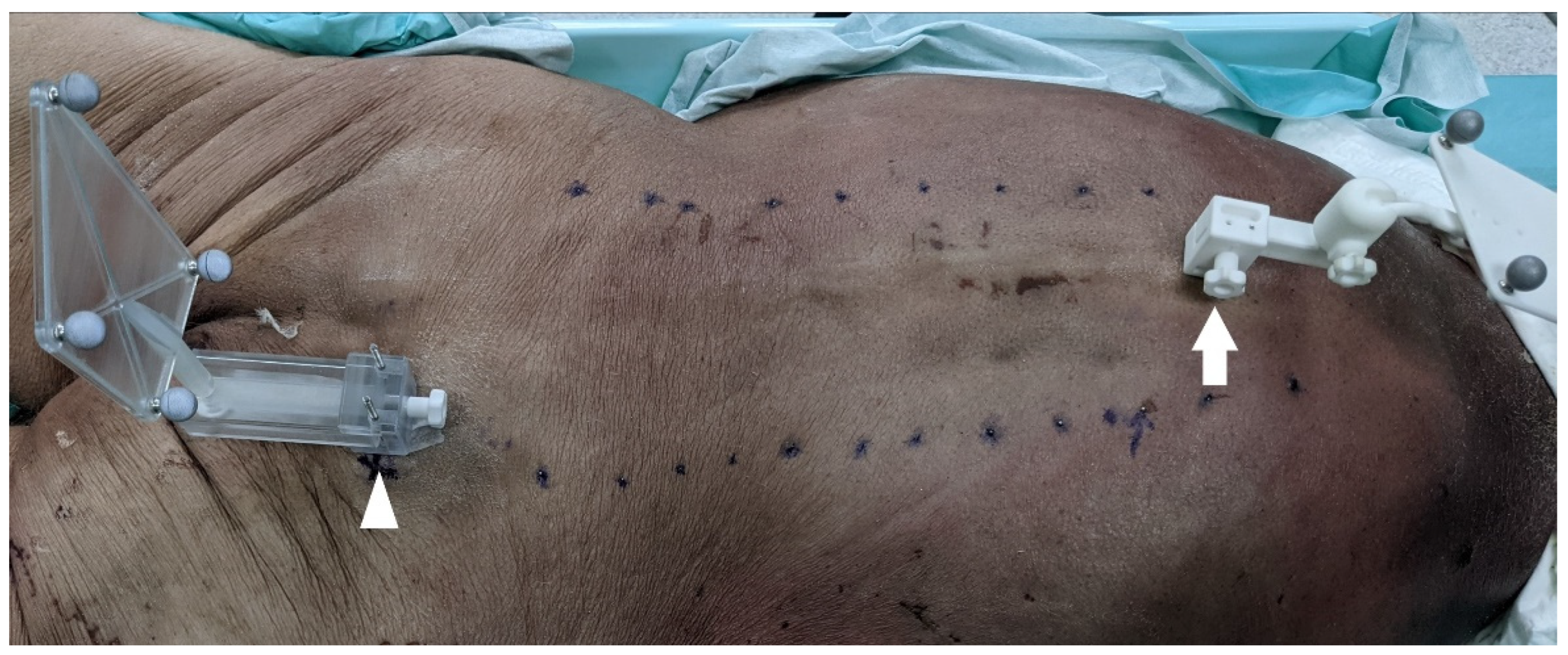
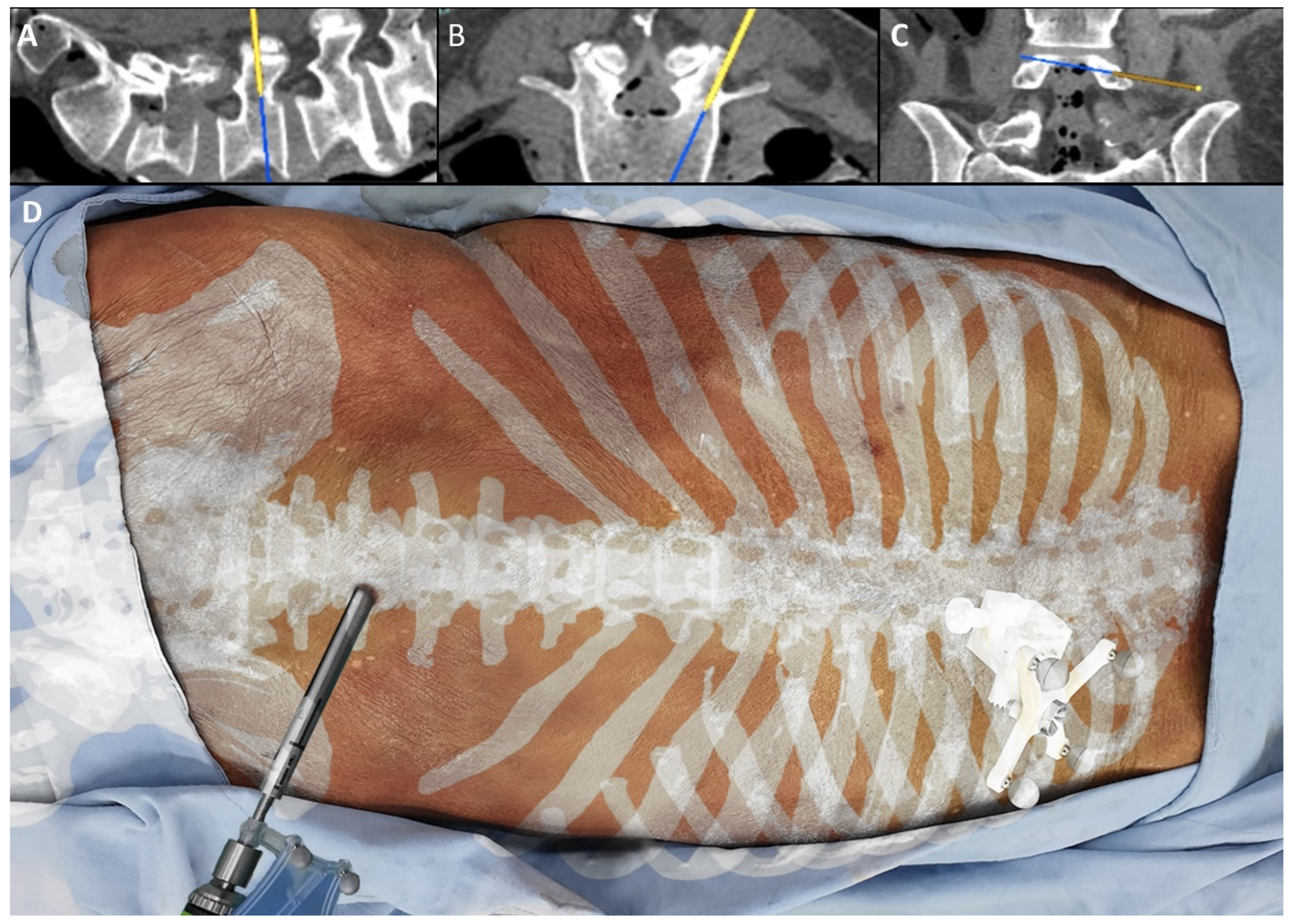
2.2. Instrumentation Method
2.3. Radiographic Accuracy Analysis
3. Results
4. Discussion
5. Conclusions
6. Disclosures
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Edström, E.; Burström, G.; Omar, A.; Nachabe, R.; Söderman, M.; Persson, O.; Gerdhem, P.; Elmi-Terander, A. Augmented Reality Surgical Navigation in Spine Surgery to Minimize Staff Radiation Exposure. Spine 2020, 45, E45–E53. [Google Scholar] [CrossRef] [PubMed]
- Mishra, R.; Narayanan, M.D.K.; Umana, G.E.; Montemurro, N.; Chaurasia, B.; Deora, H. Virtual Reality in Neurosurgery: Beyond Neurosurgical Planning. Int. J. Environ. Res. Public Health 2022, 19, 1719. [Google Scholar] [CrossRef] [PubMed]
- Fiani, B.; De Stefano, F.; Kondilis, A.; Covarrubias, C.; Reier, L.; Sarhadi, K. Virtual Reality in Neurosurgery: “Can You See It?”—A Review of the Current Applications and Future Potential. World Neurosurg. 2020, 141, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Condino, S.; Montemurro, N.; Cattari, N.; D’Amato, R.; Thomale, U.; Ferrari, V.; Cutolo, F. Evaluation of a Wearable AR Platform for Guiding Complex Craniotomies in Neurosurgery. Ann. Biomed. Eng. 2021, 49, 2590–2605. [Google Scholar] [CrossRef] [PubMed]
- Urakov, T.M.; Wang, M.Y.; Levi, A.D. Workflow Caveats in Augmented Reality-Assisted Pedicle Instrumentation: Cadaver Lab. World Neurosurg. 2019, 126, e1449–e1455. [Google Scholar] [CrossRef] [PubMed]
- Elmi-Terander, A.; Nachabe, R.; Skulason, H.; Pedersen, K.; Söderman, M.; Racadio, J.; Babic, D.; Gerdhem, P.; Edström, E. Feasibility and Accuracy of Thoracolumbar Minimally Invasive Pedicle Screw Placement With Augmented Reality Navigation Technology. Spine 2018, 43, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Wu, J.; Tang, Y.; Li, H.; Wang, W.; Li, C.; Zhou, Y. Percutaneous placement of lumbar pedicle screws via intraoperative CT image-based augmented reality-guided technology. J. Neurosurg. Spine 2019, 32, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Molina, C.A.; Phillips, F.M.; Colman, M.W.; Ray, W.Z.; Khan, M.; Orru, E.; Poelstra, K.; Khoo, L. A cadaveric precision and accuracy analysis of augmented reality-mediated percutaneous pedicle implant insertion. J. Neurosurg. Spine 2020, 34, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Molina, C.A.; Theodore, N.; Ahmed, A.K.; Westbroek, E.M.; Mirovsky, Y.; Harel, R.; Orru, E.; Khan, M.; Witham, T.; Sciubba, D.M. Augmented reality-assisted pedicle screw insertion: A cadaveric proof-of-concept study. J. Neurosurg. Spine 2019, 31, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Gertzbein, S.D.; Robbins, S.E. Accuracy of pedicular screw placement in vivo. Spine 1990, 15, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Choy, W.; Miller, C.A.; Chan, A.K.; Fu, K.M.; Park, P.; Mummaneni, P.V. Evolution of the Minimally Invasive Spinal Deformity Surgery Algorithm: An Evidence-Based Approach to Surgical Strategies for Deformity Correction. Neurosurg. Clin. N. Am. 2018, 29, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Mummaneni, P.V.; Park, P.; Shaffrey, C.I.; Wang, M.Y.; Uribe, J.S.; Fessler, R.G.; Chou, D.; Kanter, A.S.; Okonkwo, D.O.; Mundis, G.M.; et al. The MISDEF2 algorithm: An updated algorithm for patient selection in minimally invasive deformity surgery. J. Neurosurg. Spine 2019, 32, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Chou, D.; Mundis, G.; Wang, M.; Fu, K.M.; Shaffrey, C.; Okonkwo, D.; Kanter, A.; Eastlack, R.; Nguyen, S.; Deviren, V.; et al. Minimally Invasive Surgery for Mild-to-Moderate Adult Spinal Deformities: Impact on Intensive Care Unit and Hospital Stay. World Neurosurg. 2019, 127, e649–e655. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Fu, K.M.; Uribe, J.S.; Chou, D.; Mummaneni, P.V. State of the art advances in minimally invasive surgery for adult spinal deformity. Spine Deform. 2020, 8, 1143–1158. [Google Scholar] [CrossRef] [PubMed]
- Park, P.; Than, K.D.; Mummaneni, P.V.; Nunley, P.D.; Eastlack, R.K.; Uribe, J.S.; Wang, M.Y.; Le, V.; Fessler, R.G.; Okonkwo, D.O.; et al. Factors affecting approach selection for minimally invasive versus open surgery in the treatment of adult spinal deformity: Analysis of a prospective, nonrandomized multicenter study. J. Neurosurg. Spine 2020, 33, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.Y.; Uribe, J.; Mummaneni, P.V.; Tran, S.; Brusko, G.D.; Park, P.; Nunley, P.; Kanter, A.; Okonkwo, D.; Anand, N.; et al. Minimally Invasive Spinal Deformity Surgery: Analysis of Patients Who Fail to Reach Minimal Clinically Important Difference. World Neurosurg. 2020, 137, e499–e505. [Google Scholar] [CrossRef] [PubMed]
- Elmi-Terander, A.; Skulason, H.; Söderman, M.; Racadio, J.; Homan, R.; Babic, D.; van der Vaart, N.; Nachabe, R. Surgical Navigation Technology Based on Augmented Reality and Integrated 3D Intraoperative Imaging: A Spine Cadaveric Feasibility and Accuracy Study. Spine 2016, 41, E1303–E1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urakov, T.M. Augmented Reality-assisted Pedicle Instrumentation: Versatility Across Major Instrumentation Sets. Spine 2020, 45, E1622–E1626. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Screw Side | ||
|---|---|---|
| Lt | Rt | |
| T6 | 3 (M) | 0 |
| T7 | 3 (M) | 0 |
| T8 | 3 (M) | 0 |
| T9 | 0 | 0 |
| T10 | 0 | 0 |
| T11 | 0 | 0 |
| T12 | 0 | 0 |
| L1 | 3 (I/O) | 3 (I/O) |
| L2 | 3 (I/O) | 3 (I/O) |
| L3 | 3 (I/O) | 0 |
| L4 | 0 | 0 |
| L5 | 0 | 0 |
| Overall accuracy | 87.5% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-C.; Kuo, C.-H.; Chang, H.-K.; Tu, T.-H.; Fay, L.-Y.; Wu, J.-C.; Cheng, H.; Huang, W.-C. Augmented Reality-Assisted Percutaneous Pedicle Screw Instrumentation: A Cadaveric Feasibility and Accuracy Study. Appl. Sci. 2022, 12, 5261. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105261
Chang C-C, Kuo C-H, Chang H-K, Tu T-H, Fay L-Y, Wu J-C, Cheng H, Huang W-C. Augmented Reality-Assisted Percutaneous Pedicle Screw Instrumentation: A Cadaveric Feasibility and Accuracy Study. Applied Sciences. 2022; 12(10):5261. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105261
Chicago/Turabian StyleChang, Chih-Chang, Chao-Hung Kuo, Hsuan-Kan Chang, Tsung-Hsi Tu, Li-Yu Fay, Jau-Ching Wu, Henrich Cheng, and Wen-Cheng Huang. 2022. "Augmented Reality-Assisted Percutaneous Pedicle Screw Instrumentation: A Cadaveric Feasibility and Accuracy Study" Applied Sciences 12, no. 10: 5261. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105261