
Augmented Reality in Orthopedic Surgery and Its Application in Total Joint Arthroplasty: A Systematic Review

 , and
, and
Abstract
:1. Introduction
2. General Principles of Augmented Reality
3. Materials and Methods
3.1. Search Strategy
3.2. Inclusion and Exclusion Criteria
3.3. Data Extraction and Collection
4. Results
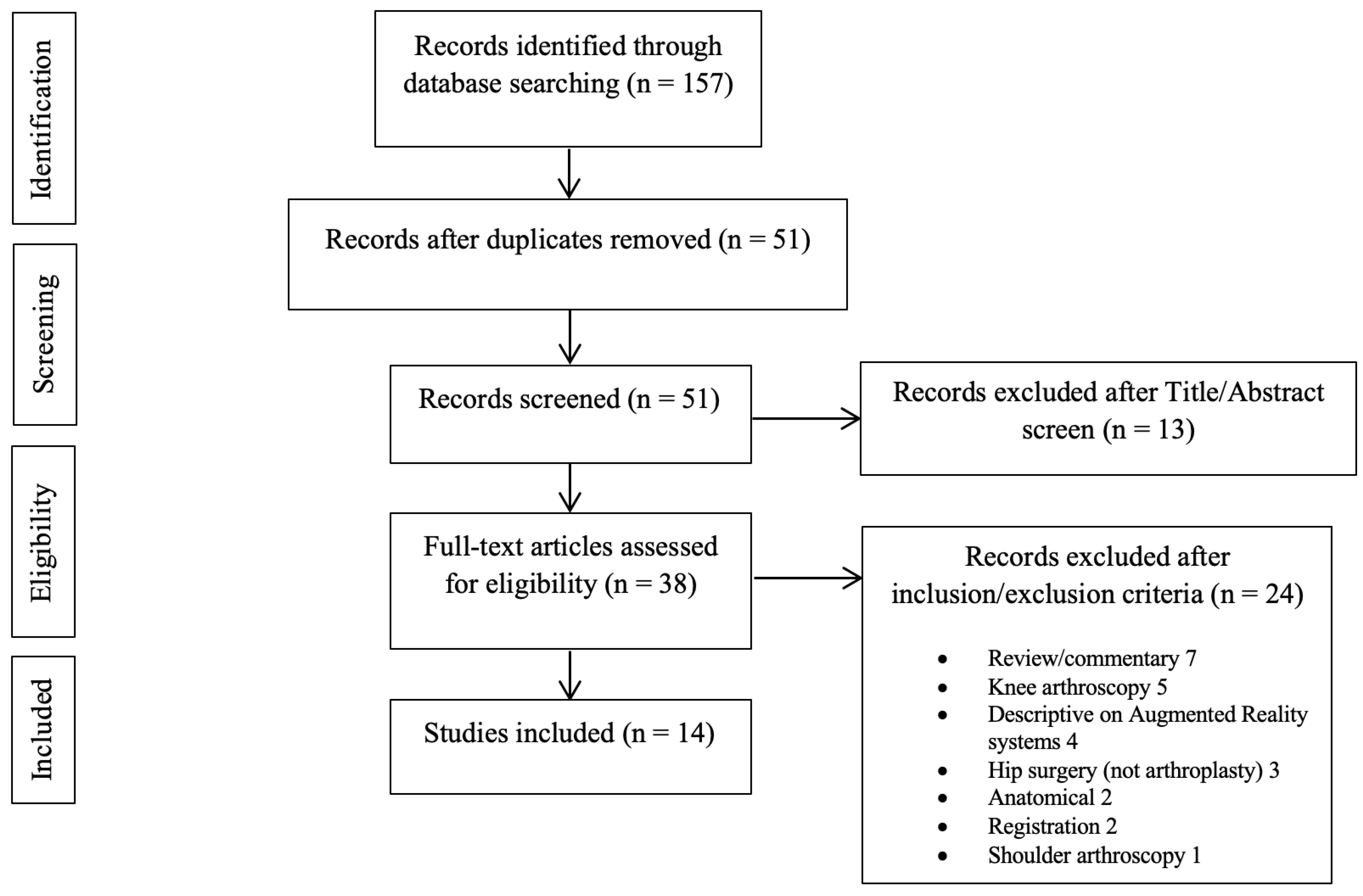
4.1. Study Selection
4.2. Total Knee Arthroplasty
4.3. Total Hip Arthroplasty
4.4. Reverse Shoulder Arthroplasty
4.5. Total Elbow Arthroplasty
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Cheng, T.; Feng, J.G.; Liu, T.; Zhang, X.L. Minimally invasive total hip arthroplasty: A systematic review. Int. Orthop. 2009, 33, 1473–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancino, F.; Cacciola, G.; Malahias, M.-A.; De Filippis, R.; De Marco, D.; Di Matteo, V.; Gu, A.; Sculco, P.K.; Maccauro, G.; De Martino, I. What are the benefits of robotic-assisted total knee arthroplasty over conventional manual total knee arthroplasty? A systematic review of comparative studies. Orthop. Rev. 2020, 12, 8657. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.W.; Jerabek, S.A. Current Role of Computer Navigation in Total Knee Arthroplasty. J. Arthroplast. 2018, 33, 1989–1993. [Google Scholar] [CrossRef] [PubMed]
- Nikou, C.; Digioia, A.M.; Blackwell, M.; Jaramaz, B.; Kanade, T. Augmented reality imaging technology for orthopaedic surgery. Oper. Tech. Orthop. 2000, 10, 82–86. [Google Scholar] [CrossRef]
- Chen, T.K.; Abolmaesumi, P.; Pichora, D.R.; Ellis, R.E. A system for ultrasound-guided computer-assisted orthopaedic surgery. Comput. Aided Surg. 2005, 10, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, J.; Boudissa, M.; Kerschbaumer, G.; Seurat, O. Role of 3D intraoperative imaging in orthopedic and trauma surgery. Orthop. Traumatol. Surg. Res. 2019, 106, S19–S25. [Google Scholar] [CrossRef]
- Azuma, R.T. A Survey of Augmented Reality. Presence Teleoperators Virtual Environ. 1997, 6, 355–385. [Google Scholar] [CrossRef]
- Tabrizi, L.B.; Mahvash, M. Augmented reality–guided neurosurgery: Accuracy and intraoperative application of an image projection technique. J. Neurosurg. 2015, 123, 206–211. [Google Scholar] [CrossRef]
- Blackwell, M.; Morgan, F.; DiGioia, A.M., III. Augmented Reality and Its Future in Orthopaedics. Clin. Orthop. Relat. Res. 1998, 354, 111–122. [Google Scholar] [CrossRef]
- Liebmann, F.; Roner, S.; von Atzigen, M.; Scaramuzza, D.; Sutter, R.; Snedeker, J.; Farshad, M.; Fürnstahl, P. Pedicle screw navigation using surface digitization on the Microsoft HoloLens. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1157–1165. [Google Scholar] [CrossRef]
- Vavra, P.; Roman, J.; Zonča, P.; Ihnát, P.; Němec, M.; Kumar, J.; Habib, N.; El-Gendi, A. Recent Development of Augmented Reality in Surgery: A Review. J. Heal. Eng. 2017, 2017, 4574172. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, M.; Yasuda, H.; Koda, K.; Suzuki, M.; Yamazaki, M.; Tezuka, T.; Kosugi, C.; Higuchi, R.; Watayo, Y.; Yagawa, Y.; et al. Image overlay navigation by markerless surface registration in gastrointestinal, hepatobiliary and pancreatic surgery. J. Hepato-Biliary-Pancreat. Sci. 2009, 17, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Gavaghan, K.A.; Peterhans, M.; Oliveira-Santos, T.; Weber, S. A Portable Image Overlay Projection Device for Computer-Aided Open Liver Surgery. IEEE Trans. Biomed. Eng. 2011, 58, 1855–1864. [Google Scholar] [CrossRef] [PubMed]
- Gavaghan, K.; Oliveira-Santos, T.; Peterhans, M.; Reyes, M.; Kim, H.; Anderegg, S.; Weber, S. Evaluation of a portable image overlay projector for the visualisation of surgical navigation data: Phantom studies. Int. J. Comput. Assist. Radiol. Surg. 2011, 7, 547–556. [Google Scholar] [CrossRef]
- Wen, R.; Chui, C.-K.; Ong, S.-H.; Lim, K.-B.; Chang, S.K.-Y. Projection-based visual guidance for robot-aided RF needle insertion. Int. J. Comput. Assist. Radiol. Surg. 2013, 8, 1015–1025. [Google Scholar] [CrossRef]
- Kocev, B.; Ritter, F.; Linsen, L. Projector-based surgeon–computer interaction on deformable surfaces. Int. J. Comput. Assist. Radiol. Surg. 2013, 9, 301–312. [Google Scholar] [CrossRef]
- Pessaux, P.; Diana, M.; Soler, L.; Piardi, T.; Mutter, D.; Marescaux, J. Towards cybernetic surgery: Robotic and augmented reality-assisted liver segmentectomy. Langenbeck’s Arch. Surg. 2014, 400, 381–385. [Google Scholar] [CrossRef]
- Badiali, G.; Ferrari, V.; Cutolo, F.; Freschi, C.; Caramella, D.; Bianchi, A.; Marchetti, C. Augmented reality as an aid in maxillofacial surgery: Validation of a wearable system allowing maxillary repositioning. J. Cranio-Maxillofac. Surg. 2014, 42, 1970–1976. [Google Scholar] [CrossRef]
- Ogawa, H.; Hasegawa, S.; Tsukada, S.; Matsubara, M. A Pilot Study of Augmented Reality Technology Applied to the Acetabular Cup Placement During Total Hip Arthroplasty. J. Arthroplast. 2018, 33, 1833–1837. [Google Scholar] [CrossRef]
- Navab, N.; Heining, S.-M.; Traub, J. Camera Augmented Mobile C-Arm (CAMC): Calibration, Accuracy Study, and Clinical Applications. IEEE Trans. Med. Imaging 2009, 29, 1412–1423. [Google Scholar] [CrossRef] [Green Version]
- Shuhaiber, J.H. Augmented Reality in Surgery. Arch. Surg. 2004, 139, 170–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Auvinet, E.; Giles, J.; Baena, F.R.Y. Augmented Reality Based Navigation for Computer Assisted Hip Resurfacing: A Proof of Concept Study. Ann. Biomed. Eng. 2018, 46, 1595–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Krevelen, D.; Poelman, R. A survey of augmented reality technologies, applications and limitations. Int. J. Virtual Real. 2010, 9, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Fallavollita, P.; Brand, A.; Wang, L.; Euler, E.; Thaller, P.; Navab, N.; Weidert, S. An augmented reality C-arm for intraoperative assessment of the mechanical axis: A preclinical study. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 2111–2117. [Google Scholar] [CrossRef]
- Tsukada, S.; Ogawa, H.; Nishino, M.; Kurosaka, K.; Hirasawa, N. Augmented reality-based navigation system applied to tibial bone resection in total knee arthroplasty. J. Exp. Orthop. 2019, 6, 1–7. [Google Scholar] [CrossRef]
- Iacono, V.; Farinelli, L.; Natali, S.; Piovan, G.; Screpis, D.; Gigante, A.; Zorzi, C. The use of augmented reality for limb and component alignment in total knee arthroplasty: Systematic review of the literature and clinical pilot study. J. Exp. Orthop. 2021, 8, 52. [Google Scholar] [CrossRef]
- Tsukada, S.; Ogawa, H.; Nishino, M.; Kurosaka, K.; Hirasawa, N. Augmented Reality-Assisted Femoral Bone Resection in Total Knee Arthroplasty. JBJS Open Access 2021, 6, e21.00001. [Google Scholar] [CrossRef]
- Fotouhi, J.; Alexander, C.P.; Unberath, M.; Taylor, G.; Lee, S.C.; Fuerst, B.; Johnson, A.; Osgood, G.; Taylor, R.H.; Khanuja, H.; et al. Plan in 2-D, execute in 3-D: An augmented reality solution for cup placement in total hip arthroplasty. J. Med. Imaging 2018, 5, 021205. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, H.; Kurosaka, K.; Sato, A.; Hirasawa, N.; Matsubara, M.; Tsukada, S. Does An Augmented Reality-based Portable Navigation System Improve the Accuracy of Acetabular Component Orientation During THA? A Randomized Controlled Trial. Clin. Orthop. Relat. Res. 2020, 478, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Alexander, C.; Loeb, A.E.; Fotouhi, J.; Navab, N.; Armand, M.; Khanuja, H.S. Augmented Reality for Acetabular Component Placement in Direct Anterior Total Hip Arthroplasty. J. Arthroplast. 2020, 35, 1636–1641.e3. [Google Scholar] [CrossRef] [PubMed]
- Logishetty, K.; Western, L.; Morgan, R.; Iranpour, F.; Cobb, J.; Auvinet, E. Can an Augmented Reality Headset Improve Accuracy of Acetabular Cup Orientation in Simulated THA? A Randomized Trial. Clin. Orthop. Relat. Res. 2018, 477, 1190–1199. [Google Scholar] [CrossRef] [PubMed]
- Tanji, A.; Nagura, T.; Iwamoto, T.; Matsumura, N.; Nakamura, M.; Matsumoto, M.; Sato, K. Total elbow arthroplasty using an augmented reality–assisted surgical technique. J. Shoulder Elb. Surg. 2021, 31, 175–184. [Google Scholar] [CrossRef]
- Schlueter-Brust, K.; Henckel, J.; Katinakis, F.; Buken, C.; Opt-Eynde, J.; Pofahl, T.; Baena, F.R.Y.; Tatti, F. Augmented-Reality-Assisted K-Wire Placement for Glenoid Component Positioning in Reversed Shoulder Arthroplasty: A Proof-of-Concept Study. J. Pers. Med. 2021, 11, 777. [Google Scholar] [CrossRef]
- Kriechling, P.; Roner, S.; Liebmann, F.; Casari, F.; Fürnstahl, P.; Wieser, K. Augmented reality for base plate component placement in reverse total shoulder arthroplasty: A feasibility study. Arch. Orthop. Trauma. Surg. 2020, 141, 1447–1453. [Google Scholar] [CrossRef]
- Kriechling, P.; Loucas, R.; Loucas, M.; Casari, F.; Fürnstahl, P.; Wieser, K. Augmented reality through head-mounted display for navigation of baseplate component placement in reverse total shoulder arthroplasty: A cadaveric study. Arch. Orthop. Trauma. Surg. 2021; published online ahead of print. [Google Scholar] [CrossRef]
- Molina, C.A.; Theodore, N.; Ahmed, A.K.; Westbroek, E.M.; Mirovsky, Y.; Harel, R.; Orru’, E.; Khan, M.; Witham, T.; Sciubba, D.M. Augmented reality–assisted pedicle screw insertion: A cadaveric proof-of-concept study. J. Neurosurg. Spine 2019, 31, 139–146. [Google Scholar] [CrossRef]
- Gibby, J.T.; Swenson, S.A.; Cvetko, S.; Rao, R.; Javan, R. Head-mounted display augmented reality to guide pedicle screw placement utilizing computed tomography. Int. J. Comput. Assist. Radiol. Surg. 2018, 14, 525–535. [Google Scholar] [CrossRef]
- Elmi-Terander, A.; Burström, G.; Nachabe, R.; Skulason, H.; Pedersen, K.; Fagerlund, M.; Ståhl, F.; Charalampidis, A.; Söderman, M.; Holmin, S.; et al. Pedicle Screw Placement Using Augmented Reality Surgical Navigation with Intraoperative 3D Imaging. Spine 2019, 44, 517–525. [Google Scholar] [CrossRef]
- Müller, F.; Roner, S.; Liebmann, F.; Spirig, J.M.; Fürnstahl, P.; Farshad, M. Augmented reality navigation for spinal pedicle screw instrumentation using intraoperative 3D imaging. Spine J. 2020, 20, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.W.; Chen, R.E.; Han, P.K.; Si, P.; Freeman, M.W.D.; Pirris, S.M. Technical feasibility and safety of an intraoperative head-up display device during spine instrumentation. Int. J. Med. Robot. Comput. Assist. Surg. 2016, 13, e1770. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.-R.; Wang, M.-L.; Liu, K.-C.; Hu, M.-H.; Lee, P.-Y. Real-time advanced spinal surgery via visible patient model and augmented reality system. Comput. Methods Programs Biomed. 2014, 113, 869–881. [Google Scholar] [CrossRef] [PubMed]
- Kosterhon, M.; Gutenberg, A.; Kantelhardt, S.R.; Archavlis, E.; Giese, A. Navigation and Image Injection for Control of Bone Removal and Osteotomy Planes in Spine Surgery. Oper. Neurosurg. 2017, 13, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Ortega, G.; Wolff, A.; Baumgaertner, M.; Kendoff, D. Usefulness of a head mounted monitor device for viewing intraoperative fluoroscopy during orthopaedic procedures. Arch. Orthop. Trauma. Surg. 2007, 128, 1123–1126. [Google Scholar] [CrossRef] [PubMed]
- Shen, F.; Chen, B.; Guo, Q.; Qi, Y.; Shen, Y. Augmented reality patient-specific reconstruction plate design for pelvic and acetabular fracture surgery. Int. J. Comput. Assist. Radiol. Surg. 2012, 8, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Mancino, F.; Cacciola, G.; Di Matteo, V.; Perna, A.; Proietti, L.; Greenberg, A.; Malahias, M.; Sculco, P.K.; Maccauro, G.; De Martino, I. Surgical implications of the hip-spine relationship in total hip arthroplasty. Orthop. Rev. 2020, 12, 8656. [Google Scholar] [CrossRef]
- Kayani, B.; Konan, S.; Tahmassebi, J.; Pietrzak, J.R.T.; Haddad, F.S. Robotic-arm assisted total knee arthroplasty is associated with improved early functional recovery and reduced time to hospital discharge compared with conventional jig-based total knee arthroplasty. Bone Jt. J. 2018, 100-B, 930–937. [Google Scholar] [CrossRef]
- Hafez, M.A.; Moholkar, K. Patient-specific instruments: Advantages and pitfalls. SICOT-J. 2017, 3, 66. [Google Scholar] [CrossRef]
- Makhni, E.C.; Makhni, S.; Ramkumar, P.N. Artificial Intelligence for the Orthopaedic Surgeon: An Overview of Potential Benefits, Limitations, and Clinical Applications. J. Am. Acad. Orthop. Surg. 2020, 29, 235–243. [Google Scholar] [CrossRef]
- Audenaert, E.; De Smedt, K.; Gelaude, F.; Clijmans, T.; Pattyn, C.; Geebelen, B. A custom-made guide for femoral component positioning in hip resurfacing arthroplasty: Development and validation study. Comput. Aided Surg. 2011, 16, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Scott, J.W. Scott’s parabola. BMJ 2001, 323, 1477. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors (Year) | Joint | AR System | Type of Study | Supporting Device | Images | Clinical Application | Potential Benefits |
|---|---|---|---|---|---|---|---|
| Fallavolita et al. (2016) [26] | TKA | Cam-C | Preclinical Cadaveric | N/A | 3 intraoperative images | Intraoperative MA | N/A |
| Tsukada et al. (2019) [27] | TKA | AR-KNEE system | Preclinical Pilot study | Smartphone | No preop images | Tibial bone resection (varus/valgus, posterior slope) | Cost-effective Reduced X-ray exposure |
| Iacono et al. (2021) [28] | TKA | Knee+ (Pixee Medical Company, Besancon, France) | Clinical Pilot | N/A | N/A | N/A | N/A |
| Tsukada et al. (2021) [29] | TKA | AR-KNEE system | Clinical | Smartphone | Standard preoperative protocol | N/A | N/A |
| Liu et al. (2018) [22] | HR | Depth Camera (Xtion Pro Live, Asustek Computer, Inc., Taipei, Taiwan, China) + HoloLense | Preclinical | HoloLens | N/A | Femoral preparation | N/A |
| Ogawa et al. (2018) [19] | THA | AR-Hip System | Clinical Pilot | Smartphone | Preoperative CT | Acetabular angles | More accurate than goniometer in measuring placement angles |
| Fotouhi et al. (2018) [30] | THA | RGBD camera + CBCT-C-arm | Preclinical | N/A | Standard preoperative protocol | Acetabular translational and orientational errors | Quick planning and visualization. Reduction in radiation and time. Increased accuracy and efficiency |
| Alexander et al. (2019) [32] | THA | RGBD camera | Preclinical | N/A | 3D images C-arm CBCT capability | N/A | N/A |
| Logishetty et al. (2019) [33] | THA | MicronTraker (ClaroNav, Toronto, Canada) + HoloLense | Preclinical Simulation Trial | HoloLense | N/A | Acetabular angles | AR training more accurate. Need to compare effectiveness with conventional training approaches |
| Ogawa et al. (2020) [31] | THA | AR-Hip System | RCT | Smartphone | Preoperative CT | Acetabular angles | Comparable with conventional |
| Tanji et al. (2021) [34] | TEA | 3DPI | Preclinical (Basic Science Study) | N/A | Preoperative CT | Implant positioning | Translational and rotational improvements in humeral and ulnar components |
| Schlueter-Brust et al. (2021) [35] | RTSA | HoloLense 2 | Proof of concept | HoloLense | Preoperative CT | k-wire placement guidance | Compares favorably with standard instrumentation techniques |
| Kriechling et al. (2021) [36] | RTSA | 3D-printed | Preclinical | HoloLense | Preoperative Ct | Glenoid guidewire positioning | highly precise surgical execution of 3D preoperative planning in RSA |
| Kriechling et al. (2021) [37] | RTSA | 3D-Planning software (CASPA, Balgrist CARD, Zurich, Switzerland) | Preclinical | HoloLense 1 | Preoperative CT | Baseplate positioning | Good accuracy in cadaveric setting |
| Authors (Year) | Patients/Sawbones | 1st End-Point | Additional Information | Results 1 | Results 2 | Other Results |
|---|---|---|---|---|---|---|
| Fallavolita et al. (2016) [26] | 25 cadaveric knees | Cam-C VS CT | MA intraoperative evaluation | N/A | N/A | n.s. difference |
| Tsukada et al. (2019) [27] | 10 tibia sawbones | N/A | N/A | Coronal error <1° | Sagittal error <1° | Rotation error <2° |
| Iacono et al. (2021) [28] | 5 pts | Evolution Medial Pivot Knee System (MicroPort Orthopedics) | VRSQ | Coronal error <1° | Sagittal error <2° | Controlled vs. radiographic error ≤1° |
| Tsukada et al. (2021) [29] | 74 pts | 31AR vs. 43IM | N/A | Coronal error sawbones <1° (tibia) <1° femur | Sagittal error sawbones <1° (tibia) <1° femur | Clinical\LDFA1.1° vs. 2.2° IM error (p < 0.001) |
| Liu et al. (2018) [22] | sawbones | Compared to 3D plan | Femoral drilling guide hole | N/A | N/A | 3D position error (mm) 1.90 3D direction error (°) 2.06 Inclination error (°) −1.53 Version error (°) 0 |
| Ogawa et al. (2018) [19] | 54 pts | Vs conventional mechanical guide (goniometer) | Acetabular placement angles | Inclination: Δ 0.5° n.s. | Anteversion: Δ 4.1° (p < 0.0001) | / |
| Fotouhi et al. (2018) [30] | sawbones | Comparison with planned | Translational and orientational errors | Translational error 1.98 mm | Orientational error 1.22° | / |
| Alexander et al. (2019) [32] | sawbones | Vs fluoroscopic technique | Acetabular placement angles in DAA | Inclination: AR more accurate (p = 0.01) Similar precision | Anteversion: AR more accurate (p = 0.02) AR more precise (p < 0.01) | Similar radiation dose. Shorter AR time (p < 0.01) |
| Logishetty et al. (2019) [33] | Sawbones 24 students × 4 trials | AR training vs. experienced-surgeon training | Acetabular placement angles | Error 6° ± 4° (expert surgeon) vs. 1° ± 1° (AR) (p < 0.001) | / | / |
| Ogawa et al. (2020) [31] | 41 pts | Vs conventional and goniometer | Acetabular placement angles | No clinically important differences in ac. inclination | No differences in ac. anteversion accuracy | N/A |
| Tanji et al. (2021) [34] | 12 cadaveric upper extremities | AR vs. conventional | Humeral and ulnar placement | Humeral Δ AR vs. conventional: v/v rot. 0.6° ± 0.4° vs. 1.9° ± 1.4° (p = 0.015) f/e rot. 0.9° ± 0.6° vs. 3.3° ± 0.6° (p = 0.002) a/p trans. 0.6° ± 0.6° vs. 3.6° ± 1.5° (p = 0.002) p/d trans. 0.5° ± 0.4° vs. 2.8° ± 2.6° (p = 0.002) | Ulnar Δ AR vs. conventional: f/e rot. 2.1° ± 1.1° vs. 7.7° ± 3.6° (p = 0.009) i/e rot. 4.9° ± 3.1° vs. 17° ± 10.9° (p = 0.015) a/p trans. 0.7° ± 0.4° vs. 4.8° ± 1.6° (p = 0.002) | N/A |
| Schlueter-Brust et al. (2021) [35] | 9 sawbones on 1 patient’s CT | Achieved vs. planned | Glenoid entry point | Δ 2.5 mm Δ 4° | / | k-wire insertion time increased by about 3′ |
| Kriechling et al. (2021) [36] | 10 3D printed scapulae from 1 patient’s CT | Achieved vs. planned | Guidewire positioning | Mean deviation entry point 2.3 mm ± 1.1 mm | Mean deviation of the planned trajectory 2.7° ± 1.3° | / |
| Kriechling et al. (2021) [37] | 12 cadaveric scapulae | Achieved vs. planned | Baseplate RSA positioning | Mean deviation entry point 3.5 mm ± 1.7 mm | Mean deviation of the planned trajectory 3.8°± 1.7° | / |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rossi, S.M.P.; Mancino, F.; Sangaletti, R.; Perticarini, L.; Lucenti, L.; Benazzo, F. Augmented Reality in Orthopedic Surgery and Its Application in Total Joint Arthroplasty: A Systematic Review. Appl. Sci. 2022, 12, 5278. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105278
Rossi SMP, Mancino F, Sangaletti R, Perticarini L, Lucenti L, Benazzo F. Augmented Reality in Orthopedic Surgery and Its Application in Total Joint Arthroplasty: A Systematic Review. Applied Sciences. 2022; 12(10):5278. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105278
Chicago/Turabian StyleRossi, Stefano Marco Paolo, Fabio Mancino, Rudy Sangaletti, Loris Perticarini, Ludovico Lucenti, and Francesco Benazzo. 2022. "Augmented Reality in Orthopedic Surgery and Its Application in Total Joint Arthroplasty: A Systematic Review" Applied Sciences 12, no. 10: 5278. https://0-doi-org.brum.beds.ac.uk/10.3390/app12105278