
The Role of Acetyl-Carnitine and Rehabilitation in the Management of Patients with Post-COVID Syndrome: Case-Control Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
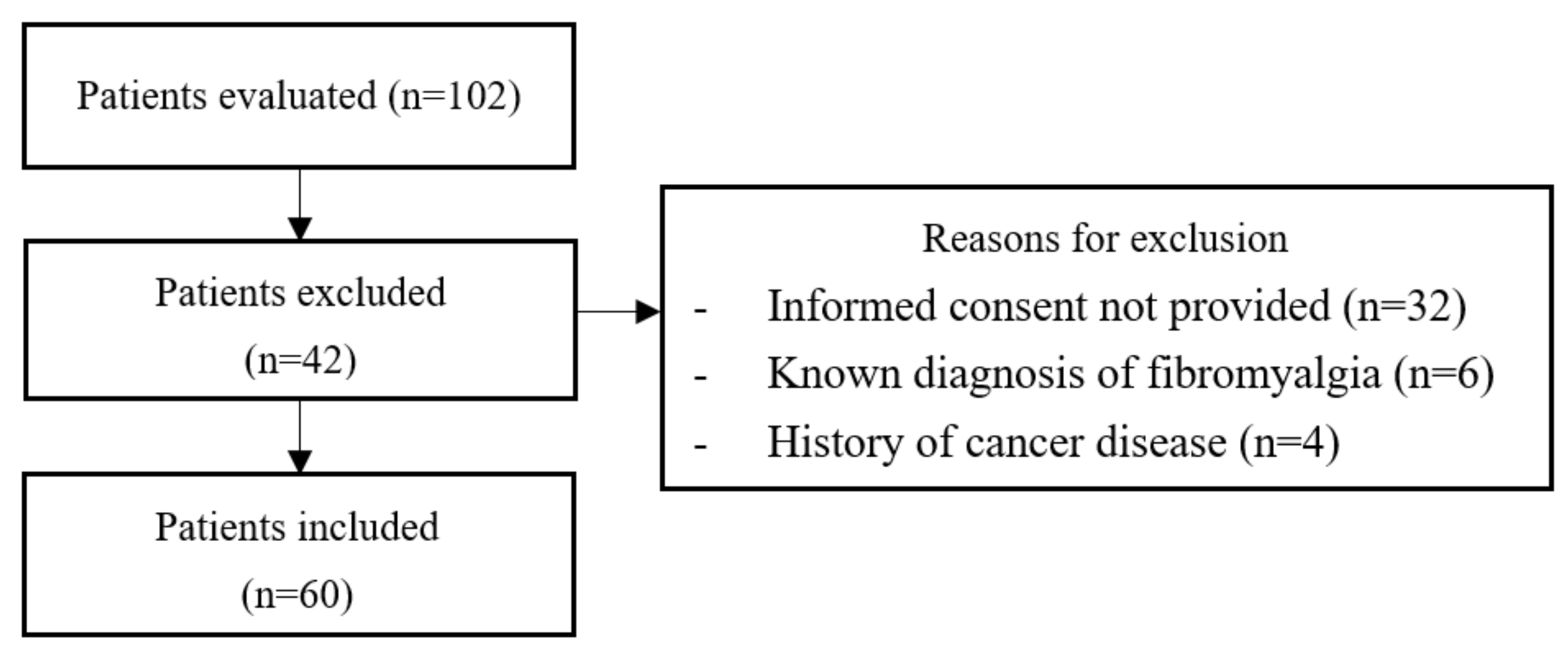
2.2. Participants
2.3. Intervention
2.4. Clinical Evaluation
2.5. Statistic Analysis
3. Result
3.1. General and Clinical Characteristics of Patients
3.2. Effects of Combining Functional Rehabilitation with ALC Supplementation in Treatment Group
3.3. Effects of Functional Rehabilitation Alone in Control Group
3.4. Comparison between the Results of the Two Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E.; et al. Mental health and well-being during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br. J. Psychiatry 2021, 218, 326–333. [Google Scholar] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V.; WHO Clinical Case Definition Working Group on Post- COVID-19 Condition. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2021, 22, e102–e107. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, R.; Rahman, M.M.; Rassel, M.A.; Monayem, F.B.; Sayeed, S.K.J.B.; Islam, M.S.; Islam, M.M. Post-COVID-19 syn- drome among symptomatic COVID-19 patients: A prospective cohort study in a tertiary care center of Bangladesh. PLoS ONE 2021, 16, e0249644. [Google Scholar] [CrossRef]
- Ursini, F.; Ciaffi, J.; Mancarella, L.; Lisi, L.; Brusi, V.; Cavallari, C.; D’Onghia, M.; Mari, A.; Borlandelli, E.; Faranda Cordella, J.; et al. Fibromyalgia: A new facet of the post-COVID-19 syndrome spectrum? Results from a web-based survey. RMD Open 2021, 7, e001735. [Google Scholar] [CrossRef]
- Mendelson, M.; Nel, J.; Blumberg, L.; Madhi, S.A.; Dryden, M.; Stevens, W.; Venter, F.W.D. Long-COVID: An evolving problem with an extensive impact. S. Afr. Med. J. 2020, 111, 10–12. [Google Scholar] [CrossRef]
- Pavli, A.; Theodoridou, M.; Maltezou, H.C. Post-COVID Syndrome: Incidence, Clinical Spectrum, and Challenges for Primary Healthcare Professionals. Arch. Med. Res. 2021, 52, 575–581. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Parums, D.V. Editorial: Long COVID, or Post-COVID Syndrome, and the Global Impact on Health Care. Med. Sci. Monit. 2021, 27, e933446. [Google Scholar] [CrossRef]
- Yunus, M.B. The prevalence of fibromyalgia in other chronic pain conditions. Pain Res. Treat. 2012, 2012, 584573. [Google Scholar] [CrossRef] [PubMed]
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in adults at 6 months after COVID-19 infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef] [PubMed]
- Dotan, A.; Shoenfeld, Y. Post-COVID syndrome: The aftershock of SARS-CoV-2. Int. J. Infect. Dis. 2022, 114, 233–235. [Google Scholar] [CrossRef]
- Arnold, L.M.; Bennett, R.M.; Crofford, L.J.; Dean, L.E.; Clauw, D.J.; Goldenberg, D.L.; Fitzcharles, M.A.; Paiva, E.S.; Staud, R.; Sarzi-Puttini, P.; et al. AAPT Diagnostic Criteria for Fibromyalgia. J. Pain 2019, 20, 611–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buskila, D.; Atzeni, F.; Sarzi-Puttini, P. Etiology of fibromyalgia: The possible role of infection and vaccination. Autoimmun. Rev. 2008, 8, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Lowry, E.; Marley, J.; McVeigh, J.G.; McSorley, E.; Allsopp, P.; Kerr, D. Dietary Interventions in the Management of Fibromyalgia: A Systematic Review and Best-Evidence Synthesis. Nutrients 2020, 12, 2664. [Google Scholar] [CrossRef] [PubMed]
- Scaturro, D.; Guggino, G.; Tumminelli, L.G.; Ciccia, F.; Letizia Mauro, G. An intense physical rehabilitation programme determines pain relief and improves the global quality of life in patients with fibromyalgia. Clin. Exp. Rheumatol. 2019, 37, 670–675. [Google Scholar] [PubMed]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Karcioglu, O.; Topacoglu, H.; Dikme, O.; Dikme, O. A systematicreview of the painscales in adults: Which to use? Am. J. Emerg. Med. 2018, 36, 707–714. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Yamamoto, A.; Oki, Y.; Sakai, H.; Misu, S.; Iwata, Y.; Kaneko, M.; Sawada, K.; Oki, Y.; Mitani, Y.; et al. Reliability and Validity of the Japanese Version of the Barthel Index Dyspnea Among Patients with Res- piratory Diseases. Int. J. Chron. Obstruct. Pulmon. Dis. 2021, 16, 1863–1871. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A. Comparison of the short form-12 (SF-12) health status questionnaire with the SF-36 in patients with knee osteoarthritis who have replacement surgery. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2620–2626. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.A.; Arnold, L.M. Measures of fibromyalgia: Fibromyalgia Impact Questionnaire (FIQ), Brief Pain Inven-tory (BPI), Multidimensional Fatigue Inventory (MFI-20), Medical Outcomes Study (MOS) Sleep Scale, and Multiple Ability Self-Report Questionnaire (MASQ). Arthritis Care Res. 2011, 63 (Suppl. 11), S86–S97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levis, B.; Benedetti, A.; Thombs, B.D.; DEPRESsion Screening Data (DEPRESSD) Collaboration. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: Individual participant data meta-analysis. BMJ 2019, 365, l1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bierle, D.M.; Aakre, C.A.; Grach, S.L.; Salonen, B.R.; Croghan, I.T.; Hurt, R.T.; Ganesh, R. Central Sensitization Phenotypes in Post Acute Sequelae of SARS-CoV-2 Infection (PASC): Defining the Post COVID Syndrome. J. Prim. Care Community Health 2021, 12, 21501327211030826. [Google Scholar] [CrossRef]
- Bornstein, S.R.; Voit-Bak, K.; Donate, T.; Rodionov, R.N.; Gainetdinov, R.R.; Tselmin, S.; Kanczkowski, W.; Müller, G.M.; Achleitner, M.; Wang, J.; et al. Chronic post-COVID-19 syndrome and chronic fatigue syndrome: Is there a role for extracorporeal apheresis? Mol. Psychiatry 2021, 27, 34–37. [Google Scholar] [CrossRef]
- Puchner, B.; Sahanic, S.; Kirchmair, R.; Pizzini, A.; Sonnweber, B.; Wöll, E.; Mühlbacher, A.; Garimorth, K.; Dareb, B.; Ehling, R.; et al. Beneficial effects of multi-disciplinary rehabilitation in post-acute COVID-19—An observational cohort study. Eur. J. Phys. Rehabil. Med. 2021, 57, 189–198. [Google Scholar] [CrossRef]
- Ferraro, F.; Calafiore, D.; Dambruoso, F.; Guidarini, S.; de Sire, A. COVID-19 related fatigue: Which role for rehabilitation in post-COVID-19 patients? A case series. J. Med. Virol. 2021, 93, 1896–1899. [Google Scholar] [CrossRef]
- Liu, K.; Zhang, W.; Yang, Y.; Zhang, J.; Li, Y.; Chen, Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement. Ther. Clin. Pract. 2020, 39, 101166. [Google Scholar] [CrossRef]
- Bruls, Y.M.; de Ligt, M.; Lindeboom, L.; Phielix, E.; Havekes, B.; Schaart, G.; Kornips, E.; Wildberger, J.E.; Hesselink, M.K.; Muoio, D.; et al. Carnitine supplementation improves metabolic flexibility and skeletal muscle acetylcarnitine formation in volunteers with impaired glucose tolerance: A randomised controlled trial. EBioMedicine 2019, 49, 318–330. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Ou, R.; Wei, Q.; Shang, H. Carnitine and COVID-19 Susceptibility and Severity: A Mendelian Randomization Study. Front. Nutr. 2021, 8, 780205. [Google Scholar] [CrossRef]
- Zheng, M.; Schultz, M.B.; Sinclair, D.A. NAD+ in COVID-19 and viral infections. Trends Immunol. 2022, 43, 283–295. [Google Scholar] [CrossRef] [PubMed]
- Rossini, M.; Di Munno, O.; Valentini, G.; Bianchi, G.; Biasi, G.; Cacace, E.; Malesci, D.; La Montagna, G.; Viapiana, O.; Adami, S. Double-blind, multicenter trial comparing acetyl l-carnitine with placebo in the treatment of fibromyalgia patients. Clin. Exp. Rheumatol. 2007, 25, 182–188. [Google Scholar] [PubMed]
- Leombruni, P.; Miniotti, M.; Colonna, F.; Sica, C.; Castelli, L.; Bruzzone, M.; Parisi, S.; Fusaro, E.; Sarzi-Puttini, P.; Atzeni, F.; et al. A randomised controlled trial comparing duloxetine and acetyl L-carnitine in fibromyalgic patients: Pre-liminary data. Clin. Exp. Rheumatol. 2015, 33 (Suppl. 88), S82–S85. [Google Scholar] [PubMed]
- Wang, S.M.; Han, C.; Lee, S.J.; Patkar, A.A.; Masand, P.S.; Pae, C.U. A review of current evidence for acetyl-l-carnitine in the treatment of depression. J. Psychiatr. Res. 2014, 53, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Smeland, O.B.; Meisingset, T.W.; Borges, K.; Sonnewald, U. Chronic acetyl-L-carnitine alters brain energy metabolism and increases noradrenaline and serotonin content in healthy mice. Neurochem. Int. 2012, 61, 100–107. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total (n = 60) | Treatment Group (n = 33) | Control Group (n = 27) | p-Value |
|---|---|---|---|---|
| Age, mean ± SD | 58.7 ± 5.4 | 61.3 ± 4.8 | 59.8 ± 4.5 | 0.22 |
| Gender, n (%) | ||||
| Male | 26 (43.3) | 15 (45.4) | 11 (40.7) | 0.67 |
| Female | 34 (56.7) | 18 (54.6) | 16 (59.3) | |
| BMI, mean ± SD (Kg/m2) | 28.8 ± 3.2 | 28.4 ± 2.9 | 27.9 ± 3.3 | 0.62 |
| Occupation, n (%) | ||||
| Working | 42 (70) | 24 (72.7) | 18 (66.6) | 0.34 |
| Unemployed | 18 (30) | 9 (27.3) | 9 (33.4) | |
| Oxygen therapy n (%) | ||||
| Yes | 39 (65) | 22 (66.7) | 17 (59.3) | 0.48 |
| No | 21 (35) | 11 (33.3) | 10 (40.7) |
| Characteristics | T0 | T1 | p-Value |
|---|---|---|---|
| NRS | 7.18 ± 0.9 | 4.9 ± 0.75 | <0.05 |
| NPI | 83.33 ± 6.47 | 85.30 ± 6.02 | 0.21 |
| FIQ | 50.66 ± 10.63 | 41.96 ± 8.68 | <0.05 |
| SF-12 | 26.18 ± 2.88 | 30.45 ± 2.49 | <0.05 |
| PHQ-9 | 13.03 ± 3.51 | 9.84 ± 3.02 | <0.05 |
| Characteristics | T0 | T1 | p-Value |
|---|---|---|---|
| NRS | 7.22 ± 0.87 | 6.8 ± 0.92 | 0.08 |
| NPI | 83.88 ± 5.15 | 86.11 ± 4.96 | 0.10 |
| FIQ | 49.55 ± 6.44 | 43.03 ± 5.86 | <0.05 |
| SF-12 | 25.07 ± 3.19 | 27.29 ± 3.16 | <0.05 |
| PHQ-9 | 13.74 ± 3.08 | 12.34 ± 2.89 | 0.09 |
| Characteristics | ΔT1-T0 | ΔT2-T0 | p-Value |
|---|---|---|---|
| NRS | 2.28 ± 0.63 | 0.42 ± 0.63 | <0.05 |
| NPI | 1.97 ± 3.88 | 2.23 ± 3.92 | 0.79 |
| FIQ | 8.7 ± 5.72 | 6.52 ± 2.68 | 0.07 |
| SF-12 | 4.27 ± 1.91 | 2.22 ± 2.53 | <0.05 |
| PHQ-9 | 3.19 ± 2.04 | 1.4 ± 1.33 | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scaturro, D.; Vitagliani, F.; Di Bella, V.E.; Falco, V.; Tomasello, S.; Lauricella, L.; Letizia Mauro, G. The Role of Acetyl-Carnitine and Rehabilitation in the Management of Patients with Post-COVID Syndrome: Case-Control Study. Appl. Sci. 2022, 12, 4084. https://0-doi-org.brum.beds.ac.uk/10.3390/app12084084
Scaturro D, Vitagliani F, Di Bella VE, Falco V, Tomasello S, Lauricella L, Letizia Mauro G. The Role of Acetyl-Carnitine and Rehabilitation in the Management of Patients with Post-COVID Syndrome: Case-Control Study. Applied Sciences. 2022; 12(8):4084. https://0-doi-org.brum.beds.ac.uk/10.3390/app12084084
Chicago/Turabian StyleScaturro, Dalila, Fabio Vitagliani, Vito Emanuele Di Bella, Vincenzo Falco, Sofia Tomasello, Lorenza Lauricella, and Giulia Letizia Mauro. 2022. "The Role of Acetyl-Carnitine and Rehabilitation in the Management of Patients with Post-COVID Syndrome: Case-Control Study" Applied Sciences 12, no. 8: 4084. https://0-doi-org.brum.beds.ac.uk/10.3390/app12084084