1. Introduction
Ataxia Telangiectasia (
AT; MIM # 208900) is a rare genetic disorder characterized by early onset ataxia (lack of coordination of movements), neurodegeneration and multisystem involvement, including immunological defects, organ failure and predisposition to cancer [
1,
2]. The incidence worldwide is estimated to span from 1:40,000 to 1:100,000 individuals, and 1:300,000 in the West Midlands population. From a clinical point of view, AT is characterized by impaired coordination of the movement of voluntary muscles, with gait unbalance, oculomotor apraxia, altered speech fluency, anterior horn cell degeneration, peripheral neuropathy, and a cerebellar cognitive affective psychological profile. Despite the disease affecting, overall, the central and peripheral nervous system, the involvement of other organs and body systems is variably present. Cutaneous and ocular telangiectasia, growth failure, dysfunction of the immune system with immune deficiency, recurrent respiratory infections, endocrine and gastrointestinal disturbances, proneness to malignancy, premature aging, and hypersensitivity to ionizing radiations, are part of the clinical constellation. The phenotypic spectrum of the disease varies from the severe classical form, presenting with the early onset, relentless progression of neurodegeneration and reduced survival, to the mild variant form, where the clinical picture is consistent with the later onset of the disease, slow progression of ataxia, and longer survival.
Apart from cerebellar ataxia, which is the most common neurological manifestation of AT that gives the syndrome its name, AT encompasses a wide spectrum of movement disorders that complicates patients’ daily activities while impacting the course of the disease [
1,
3]. At the onset, initial manifestations of AT include cerebellar features with gait unbalance, hypotonia, and slow voluntary movements followed by dystonia, choreoathetosis, and tremor, while the occurrence of movement disorders at follow up confirms, in almost all patients, the progression of cerebellar manifestations with standing and posture troubles, myoclonus, dystonia, choreoathetosis, and tremor. The age of onset of ataxia is generally coincident with the beginning of children walking, at around 12–13 months, however, signs of head tilting and mild truncal ataxia may be apparent at earlier developmental ages. Age of diagnosis is generally postponed to 3–4 years, pointing out a diagnostic delay of about 2 years (personal observation) for this syndrome. The ongoing loss of coordination and balance, together with the degeneration of anterior horn cells, and peripheral neuropathy lead to a loss of ambulation usually occurring in classic AT between the ages of 12 and 16 years, with some patients becoming wheelchair bound earlier. Joint contractures develop insidiously due to the progressive lack of motor activity and diminished weight gain. Walking capacities can range from normal to abnormal with an irregular, staggering, and wide based gait. Patients can be unable to walk with their feet in a tandem position (the heel to toe position of both feet), walk without support, or walk at all, and be wheelchair bound. Gait speed can also be affected, varying from normal, slightly, or strikingly reduced. Standing capacity is impaired by a significant sway and continuous posture corrections of the body [
3].
Management of AT is entrusted to tailored support and lifelong rehabilitative programs. Difficulties in accessing specialized clinical care prompt the need for advanced and cutting edge techniques, which are, thus, deservedly thought of as essential sources to ameliorate the quality of life of AT patients and their families. However, thanks to the growing body of knowledge, traditional rehabilitative approaches are now more often flanked by fascinating experimental investigations, leading to the more independent management of the disease from the patient’s point of view, while also allowing more frequent and long-lasting patient training. In general, body movement can be monitored using several different technologies, with the optoelectronic ones being considered as the gold standard, which are mainly based on infrared cameras. However, because of drawbacks such as high costs, dedicated rooms, and the necessity of experienced personnel, other technologies have been emerging. Therefore, depending on the particular body movement to be measured, different solutions have been proposed: photoplethysmogram (PPG), ballistocardiogram (BCG), seismocardiogram (SCG) for measuring respiratory rate [
4]; WiFi and radio detection and ranging (RADAR) for activity recognition [
5]; and wearable technology—based on inertial measurement units (IMUs) [
6], flexible sensors [
7], insole pressure sensors, or electromyography sensors—for gait analysis [
8,
9].
Within the frame of clinical or general performance evaluations [
10,
11,
12,
13,
14,
15], temporal gait analyses are nowadays used to complement the classical gait analyses that involve motion analysis, dynamic electromyography, force plate recordings, energy cost measurements, and measurement of the stride characteristics [
16,
17,
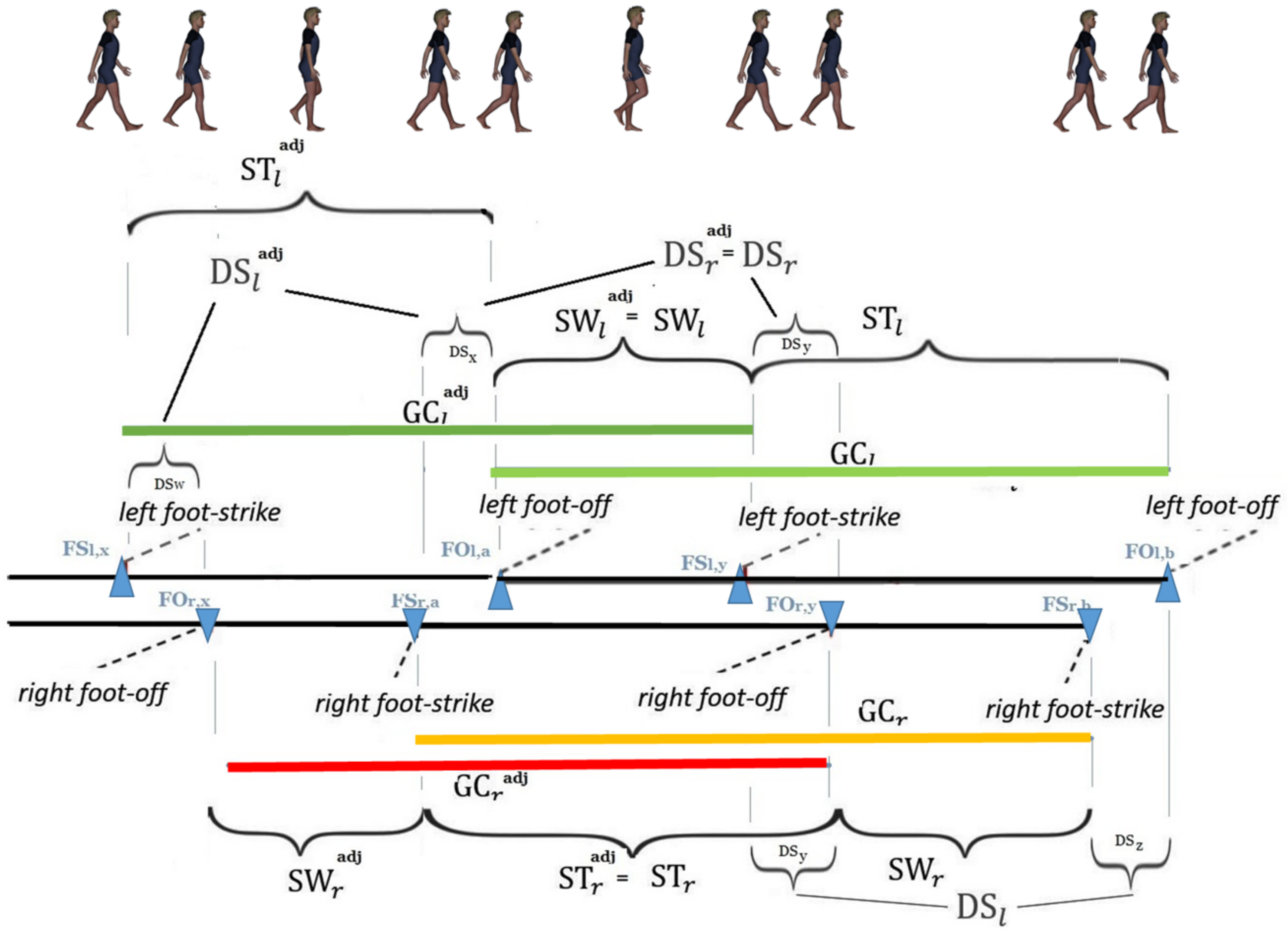
18]. Indeed, four time intervals—namely, the ones associated with the durations of the gait cycle, swing, stance, and double support phases—temporally characterize symmetric and recursive human walking [
16]. An innovative research direction, promoted by [
19], has emerged from most of the literature agreeing that the foot off reliably occurs at 60% to 62% of a physiological gait when the subject is (symmetrically and recursively) walking at a comfortable speed: the analysis of the ratio between the swing and double support phase durations has experimentally recognized it as close—in healthy subjects symmetrically and recursively walking at about 4 km/h [
20], but not in patients affected by neurological disorders—to the golden ratio
, i.e., the positive solution to the equation
(see [
21]). Such an irrational number, which is related to Euclid’s problem of cutting in a self-proportional way a given straight segment, thus captures:
Now, symmetry and harmony are strictly intertwined in walking. Two comprehensive indices in ref. [
24,
25] have been, accordingly, recently suggested to simultaneously characterize these two important features. In particular, ref. [
25] has provided original mathematically founded arguments to a fractal approach to the question (the generic idea that walking can have a fractal structure can be found in [
26], while the existence of significant alterations from such a structure in patients with Parkinson’s Disease has been suggested in [
27]): the larger scale structure resembles the subunit structure through the generation of a self-referential loop (see Refs. [
28,
29] for relevant applications to swimming). Human walking is, then, innovatively described in terms of generalized finite length Fibonacci sequences [
30] and dynamics on graph concepts, with the new mathematical concept of a
composite gait cycle—involving two specific couples of overlapping gait cycles, namely, the left and right gait cycles and the
adjoint right and left gait cycles—to extend the idea of stride to stride intervals [
31] and step-by-step intervals [
32].
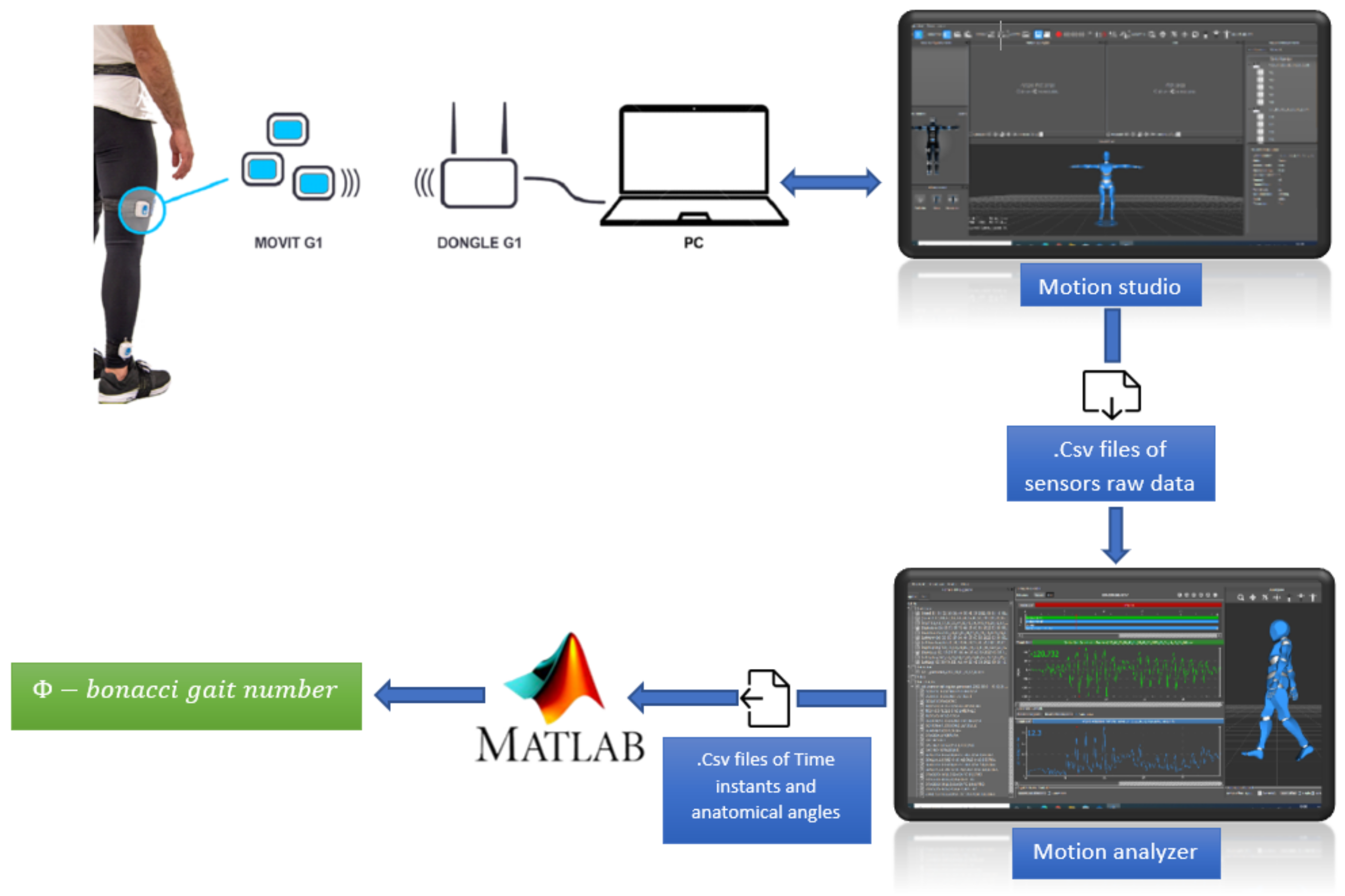
The aim of this paper is to present the reliability of a technologically assisted methodology—performed with an easy to use wearable motion capture system—in assessing motion abilities in AT. Such a methodology relies on the experimental verification of the most recent and comprehensive accurate and objective outcome measures of gait recursivity and harmonicity and symmetry and double support sub phase consistency, as very recently defined in [
25]. Three subjects with different ranges of severity of AT are analyzed and the values of the involved indices are shown to comply with the qualitative evaluations provided by the clinicians.
4. Discussion
Due to the lack of decisive solutions, AT remains a disabling progressive chronic condition, especially in its classic form, requiring huge personal and family commitment in terms of time, money, and lifelong rehabilitative programs. Hopefully, neurorehabilitation has developed, in recent years, new opportunities to minimize and/or compensate for functional alterations and/or neurological disability; this is achieved, rather, by addressing different types of therapy to specific clinical disorders and patients’ age. However, thanks to the growing body of knowledge, traditional rehabilitative approaches are now more often flanked by fascinating experimental investigations leading to the more independent management of the disease from the patient’s point of view, while alsoallowing more frequent and long-lasting patient training. In particular, instrumental gait analysis allows for objectively assessing important parameters related to the locomotor ability of subjects with neurological diseases, although in many neurodegenerative syndromes these analyses have not yet been investigated.
Now, according to the previous section and in particular to
Table 7, the
-bonacci gait number turns out to be larger for the AT patients than the healthy subjects. Furthermore, among the three healthy subjects, the values of this index consistently range from
to
. The largest values of this index—observed in AT patients—reflect the effects of their pathology. Among them, patient A—with the mildest AT phenotype—exhibits the smallest number, despite it being approximately twice as large as the healthy subjects’. Patient G—with an intermediate AT phenotype—exhibits an index that is, in turn, approximately twice as large as patient A.’s. Lastly, a very high value of this index is computed for patient F, who has the most severe AT phenotype. It is worth noticing that the mere analysis of the double support phase durations does not allow us to highlight all these quantitative considerations. In fact, as shown in the related tables, the durations of the double support phases for patient A are similar to those corresponding to the healthy subjects, whereas the same durations for patient G are even lower than those corresponding to healthy subjects. Only for patient F, are these durations are meaningfully large. These results, which comply with the relevant qualitative evaluations provided by the clinicians, support the idea that the
-bonacci gait number can be successfully used in a rare disease such as AT. In more detail, despite a study on a wider sample being needed, these data are sufficient to find statistically significant differences between the patients and the healthy controls (
, Mann–Whitney one tailed U test). The data for the most severe patient (F) exhibit the highest value of the
-bonacci gait number, confirming not only the accuracy of this index in differentiating the patients from the healthy subjects, but also to objectively quantify the deficit among the patients.
Therefore, the use of objective measures of motor abilities in AT patients, such as the ones described in this paper, might facilitate the standardization of rehabilitative treatments and the evaluation of outcomes. These can help, first, in identifying predictors of the progression of motor and movement dysfunctions, and, next, facilitate patient selection and stratification in clinical trials, potentially enabling studies with direct clinical outcomes, which can be hindered, mostly, by inter- and intrasubject variability regarding severity and progression of the disease. Concurrently, in home evaluation through objective measures of motor abilities might minimize difficulties in accessing specialized clinical care for disabled AT people and those living in underserved areas, highlighting the need for the latest strategies involving telemedicine.
5. Further Applications
This section aims at showing that the wearable motion capture system adopted in this paper also allows for evaluating motor imagery (MI), which is an important resource in neurorehabilitation. Defined as a multiprofessional physician led approach to healthcare, it aims at reducing disability and improving functions affected by damaged nervous systems [
37]. MI is a cognitive process in which the representation of a given motor movement is executed in working memory without any motor output [
38]. This process is embedded in a mental imagery construct—a multimodal cognitive simulation process that enables us to represent perceptual information in our minds in the absence of actual sensory input [
39]—and refers specifically to the mental simulation of body movements. The use of MI turns out to be relevant in movement disorders. Indeed, MI has been explored in clinical groups, e.g., patients with movement disorders and specific neurological diseases [
40,
41,
42].
In respect to this, the three AT patients were required to start an additional experiment (see [
43]) by standing over a line marked on the floor. In front of them, another line was taped on the ground at a distance (unknown to the subjects) of 9 m (
m for F). They were first asked to stand still and imagine moving towards the visualized target (referred to as MIs). Then, subjects were requested to imagine the same task by mimicking the physical movements of walking (referred to as MIw) (F did not carried out this activity). To verify the ability to perform such imaginary tasks, the time of MI was calculated by a chronometer (referred to as T) and compared to the time spent to reach the target. The results are reported below.
A (9 m): T = s — MIs = s — MIw = s
F (4.5 m): T = s — MIs = s —MIw = n.a.
G (9 m): T = s — MIs = s — MIw = s
The MI tests provide interesting information about the implicit awareness of pathology severity in patients. Patient A shows a good temporal equivalence between the real execution of the task and the two motor imagery tasks. This equivalence is preserved for the dynamic MI of patient G, whereas the imagined time during the static task is shorter, for patients F and G, than the one corresponding to their real walking, according to the idea that patients may often underestimate their deficits [
43].



 ,
, 




{kind=link}
{kind=link}
{kind=link}