
Optimal Timing of Cholecystectomy in Secondary Choledocholithiasis Patients Who Underwent Preoperative Endoscopic Retrograde Cholangiopancreatography



Abstract
:1. Introduction
2. Materials and Methods
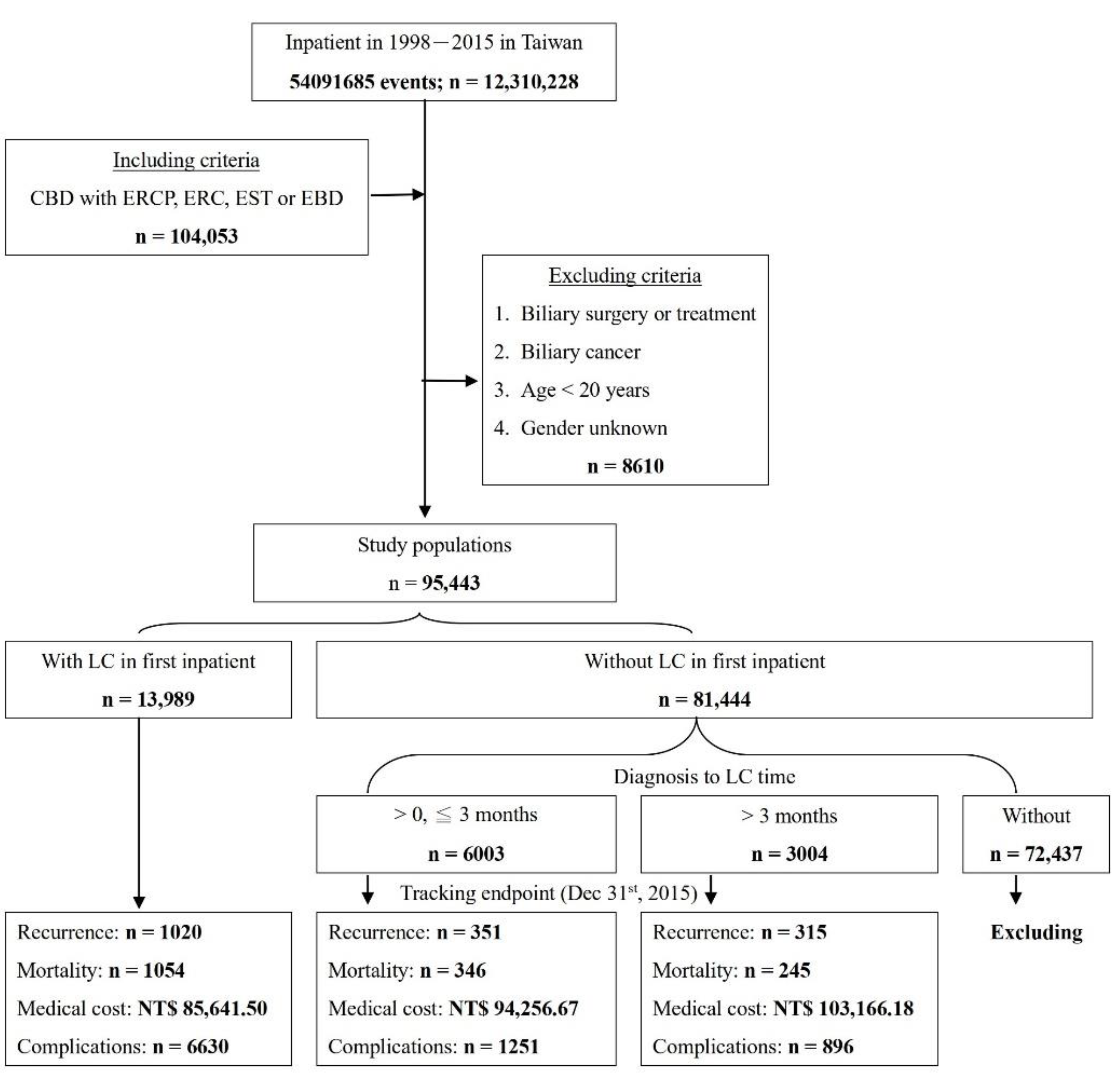
2.1. Study Design
2.2. Data Processing and Statistical Analysis
3. Results
3.1. Comorbidity Profile
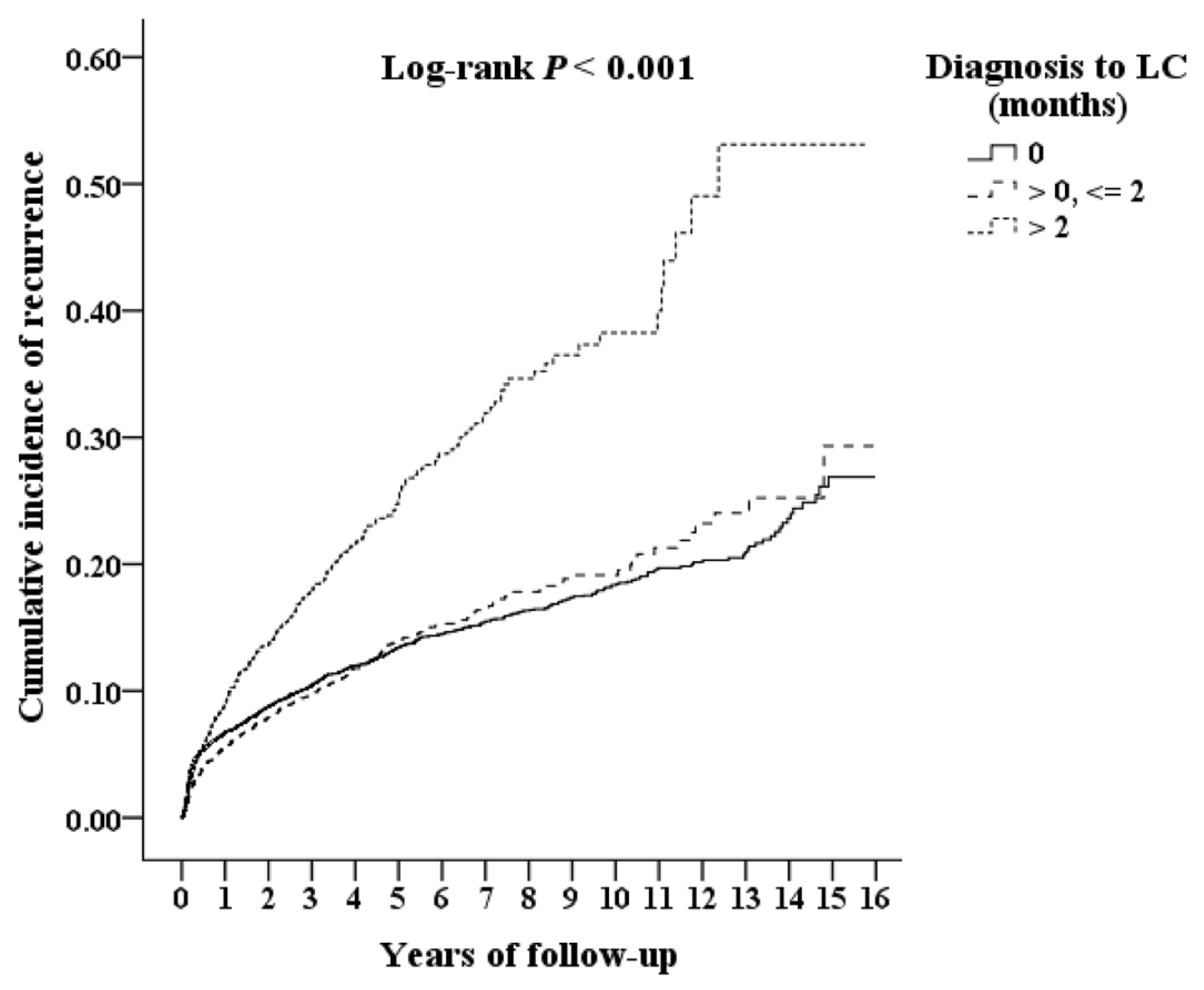
3.2. Recurrence Rates
3.3. Complications
3.4. Mortality
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Molvar, C.; Glaenzer, B. Choledocholithiasis: Evaluation, treatment, and outcomes. Semin. Intervent. Radiol. 2016, 33, 268–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cianci, P.; Restini, E. Management of cholelithiasis with choledocholithiasis: Endoscopic and surgical approaches. World J. Gastroenterol. 2021, 27, 4536–4554. [Google Scholar] [CrossRef] [PubMed]
- Buxbaum, J.L.; Abbas Fehmi, S.M.; Sultan, S.; Fishman, D.S.; Qumseya, B.J.; Cortessis, V.K.; Schilperoort, H.; Kysh, L.; Matsuoka, L.; Yachimski, P.; et al. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis. Gastrointest. Endosc. 2019, 89, 1075–1105.e15. [Google Scholar] [CrossRef] [PubMed]
- Garancini, M.; Redaelli, A.; Dinelli, M.; Leni, D.; Fior, D.; Giardini, V. Updates in the management of cholecystitis, cholangitis, and obstructive jaundice. In Operative Techniques and Recent Advances in Acute Care and Emergency Surgery; Aseni, P., De Carlis, L., Mazzola, A., Grande, A.M., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 455–468. [Google Scholar]
- McNicoll, C.F.; Pastorino, A.; Farooq, U.; St Hill, C.R. Choledocholithiasis; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Boerma, D.; Rauws, E.A.J.; Keulemans, Y.C.A.; Janssen, I.M.C.; Bolwerk, C.J.M.; Timmer, R.; Boerma, E.J.; Obertop, H.; Huibregtse, K.; Gouma, D.J. Wait-and-see policy or laparoscopic cholecystectomy after endoscopic sphincterotomy for bile-duct stones: A randomised trial. Lancet 2002, 360, 761–765. [Google Scholar] [CrossRef]
- Lau, J.Y.; Leow, C.K.; Fung, T.M.; Suen, B.-Y.; Yu, L.-M.; Lai, P.B.; Lam, Y.-H.; Ng, E.K.; Lau, W.Y.; Chung, S.S.; et al. Cholecystectomy or gallbladder in situ after endoscopic sphincterotomy and bile duct stone removal in Chinese patients. Gastroenterology 2006, 130, 96–103. [Google Scholar] [CrossRef]
- Wang, C.C.; Tsai, M.C.; Wang, Y.T.; Yang, T.W.; Chen, H.Y.; Sung, W.W.; Huang, S.M.; Tseng, M.H.; Lin, C.C. Role of cholecystectomy in choledocholithiasis patients underwent endoscopic retrograde cholangiopancreatography. Sci. Rep. 2019, 9, 2168. [Google Scholar] [CrossRef] [Green Version]
- Pisano, M.; Allievi, N.; Gurusamy, K.; Borzellino, G.; Cimbanassi, S.; Boerna, D.; Coccolini, F.; Tufo, A.; Di Martino, M.; Leung, J.; et al. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis. World J. Emerg. Surg. 2020, 15, 61. [Google Scholar] [CrossRef]
- Mann, K.; Belgaumkar, A.P.; Singh, S. Post-endoscopic retrograde cholangiography laparoscopic cholecystectomy: Challenging but safe. JSLS 2013, 17, 371–375. [Google Scholar] [CrossRef] [Green Version]
- Schiphorst, A.H.; Besselink, M.G.; Boerma, D.; Timmer, R.; Wiezer, M.J.; van Erpecum, K.J.; Broeders, I.A.M.J.; van Ramshorst, B. Timing of cholecystectomy after endoscopic sphincterotomy for common bile duct stones. Surg. Endosc. 2008, 22, 2046–2050. [Google Scholar] [CrossRef]
- Miura, F.; Takada, T.; Strasberg, S.M.; Solomkin, J.S.; Pitt, H.A.; Gouma, D.J.; Garden, O.J.; Büchler, M.W.; Yoshida, M.; Mayumi, T.; et al. TG13 flowchart for the management of acute cholangitis and cholecystitis. J. Hepatobiliary Pancreat. Sci. 2013, 20, 47–54. [Google Scholar] [CrossRef]
- Cheng, T.M. Taiwan’s new national health insurance program: Genesis and experience so far. Health Aff. 2003, 22, 61–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.Y.; Kuo, K.N.; Wu, M.S.; Chen, Y.J.; Wang, C.B.; Lin, J.T. Early Helicobacter pylori eradication decreases risk of gastric cancer in patients with peptic ulcer disease. Gastroenterology 2009, 137, 1641–1648.e2. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Chan, F.K.; Wu, M.S.; Kuo, K.N.; Wang, C.B.; Tsao, C.R.; Lin, J.T. Histamine2-receptor antagonists are an alternative to proton pump inhibitor in patients receiving clopidogrel. Gastroenterology 2010, 139, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Strasberg, S.M.; Helton, W.S. An analytical review of vasculobiliary injury in laparoscopic and open cholecystectomy. HPB 2011, 13, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, N.O. Biliary complications postlaparoscopic cholecystectomy: Mechanism, preventive measures, and approach to management: A review. Diagn. Ther. Endosc. 2011, 2011, 967017. [Google Scholar] [CrossRef] [PubMed]
- Romano, L.; Lazzarin, G.; Varrassi, M.; Di Sibio, A.; Vicentini, V.; Schietroma, M.; Carlei, F.; Giuliani, A. Haemobilia secondary to a cystic artery pseudoaneurysm as complication of VLC. Acta Biomed. 2021, 92, e2021125. [Google Scholar] [CrossRef] [PubMed]
- Wilson, E.; Gurusamy, K.; Gluud, C.; Davidson, B.R. Cost-utility and value-of-information analysis of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Br. J. Surg. 2010, 97, 210–219. [Google Scholar] [CrossRef] [PubMed]
- Friis, J.P.C.; Rothman, J.; Burcharth, J. Rosenberg Optimal timing for laparoscopic cholecystectomy after endoscopic retrograde cholangiopancreatography: A systematic review. Scand J. Surg. 2018, 107, 99–106. [Google Scholar] [CrossRef]
- Reinders, J.S.; Goud, A.; Timmer, R.; Kruyt, P.M.; Witteman, B.J.M.; Smakman, N.; Breumelhof, R.; Donkervoort, S.C.; Jansen, J.M.; Heisterkamp, J.; et al. Early laparoscopic cholecystectomy improves outcomes after endoscopic sphincterotomy for choledochocystolithiasis. Gastroenterology. 2010, 138, 2315–2320. [Google Scholar] [CrossRef]
- Gutt, C.N.; Encke, J.; Köninger, J.; Harnoss, J.C.; Weigand, K.; Kipfmüller, K.; Schunter, O.; Götze, T.; Golling, M.T.; Menges, M.; et al. Acute cholecystitis: Early versus delayed cholecystectomy, a multicenter randomized trial (ACDC study, NCT00447304). Ann. Surg. 2013, 258, 385–393. [Google Scholar] [CrossRef]
- Reynolds, B.M.; Dargan, E.L. Acute obstructive cholangitis; a distinct clinical syndrome. Ann. Surg. 1959, 150, 299–303. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Diagnosis to LC (Months) | Total | Group A: 0 (at the Same Time) | Group B: >0, ≤2 | Group C: >2 | p | ||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | n | % | n | % | n | % | n | % | |
| Total | 22,996 | 62.18 | 13,989 | 60.83 | 5970 | 25.96 | 3037 | 13.21 | |
| Gender | <0.001 | ||||||||
| Male | 11,006 | 50.04 | 6484 | 46.35 | 2969 | 49.73 | 1553 | 76.24 | |
| Female | 10,990 | 49.96 | 7505 | 53.65 | 3001 | 50.27 | 484 | 23.76 | |
| Age (years) | 58.85 ± 16.29 | 58.19 ± 16.23 | 58.69 ± 16.59 | 62.22 ± 15.54 | <0.001 | ||||
| IHD | 0.876 | ||||||||
| Without | 22,125 | 96.21 | 13,458 | 96.20 | 5749 | 96.30 | 2918 | 96.08 | |
| With | 871 | 3.79 | 531 | 3.80 | 221 | 3.70 | 119 | 3.92 | |
| HCVD | 0.004 | ||||||||
| Without | 22,620 | 98.36 | 13,790 | 98.58 | 5858 | 98.12 | 2972 | 97.86 | |
| With | 376 | 1.64 | 199 | 1.42 | 112 | 1.88 | 65 | 2.14 | |
| Stroke | 0.032 | ||||||||
| Without | 22,635 | 98.43 | 13,776 | 98.48 | 5886 | 98.59 | 2973 | 97.89 | |
| With | 361 | 1.57 | 213 | 1.52 | 84 | 1.41 | 64 | 2.11 | |
| PUD | <0.001 | ||||||||
| Without | 20,020 | 87.06 | 11,821 | 84.50 | 5432 | 90.99 | 2767 | 91.11 | |
| With | 2976 | 12.94 | 2168 | 15.50 | 538 | 9.01 | 270 | 8.89 | |
| IBD | 0.885 | ||||||||
| Without | 22,991 | 99.98 | 13,986 | 99.98 | 5969 | 99.98 | 3036 | 99.97 | |
| With | 5 | 0.02 | 3 | 0.02 | 1 | 0.02 | 1 | 0.03 | |
| DM | <0.001 | ||||||||
| Without | 19,587 | 85.18 | 12,024 | 85.95 | 5072 | 84.96 | 2491 | 82.02 | |
| With | 3409 | 14.82 | 1965 | 14.05 | 898 | 15.04 | 546 | 17.98 | |
| HF | 0.025 | ||||||||
| Without | 22,813 | 99.20 | 13,875 | 99.19 | 5935 | 99.41 | 3003 | 98.88 | |
| With | 183 | 0.80 | 114 | 0.81 | 35 | 0.59 | 34 | 1.12 | |
| CKD | 0.001 | ||||||||
| Without | 22,844 | 99.34 | 13,907 | 99.41 | 5936 | 99.43 | 3001 | 98.81 | |
| With | 152 | 0.66 | 82 | 0.59 | 34 | 0.57 | 36 | 1.19 | |
| Liver cirrhosis | <0.001 | ||||||||
| Without | 21,640 | 94.10 | 13,048 | 93.27 | 5708 | 95.61 | 2884 | 94.96 | |
| With | 1356 | 5.90 | 941 | 6.73 | 262 | 4.39 | 153 | 5.04 | |
| Pancreatitis | <0.001 | ||||||||
| Without | 20,143 | 87.59 | 11,627 | 83.12 | 5631 | 94.32 | 2885 | 95.00 | |
| With | 2853 | 12.41 | 2362 | 16.88 | 339 | 5.68 | 152 | 5.00 | |
| Recurrence | <0.001 | ||||||||
| Without | 21,310 | 92.67 | 12,969 | 92.71 | 5621 | 94.15 | 2720 | 89.56 | |
| With | 1686 | 7.33 | 1020 | 7.29 | 349 | 5.85 | 317 | 10.44 | |
| Mortality | <0.001 | ||||||||
| Without | 21,351 | 92.85 | 12,935 | 92.47 | 5631 | 94.32 | 2785 | 91.70 | |
| With | 1645 | 7.15 | 1054 | 7.53 | 339 | 5.68 | 252 | 8.30 | |
| Complications | <0.001 | ||||||||
| Without | 14,219 | 61.83 | 7359 | 52.61 | 4749 | 79.55 | 2111 | 69.51 | |
| With | 8777 | 38.17 | 6630 | 47.39 | 1221 | 20.45 | 926 | 30.49 | |
| Variable | Recurrence | Mortality | Complications | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adjusted HR | 95% CI | 95% CI | p | Adjusted HR | 95% CI | 95% CI | p | Adjusted OR | 95% CI | 95% CI | p | |
| Diagnosis to LC (months) | ||||||||||||
| 0 | Reference | Reference | Reference | |||||||||
| >0, ≤2 | 0.967 | 0.855 | 1.094 | 0.596 | 1.116 | 0.985 | 1.265 | 0.085 | 0.296 | 0.275 | 0.318 | <0.001 |
| >2 | 1.704 | 1.498 | 1.939 | <0.001 | 1.511 | 1.313 | 1.739 | <0.001 | 0.487 | 0.446 | 0.513 | <0.001 |
| Gender | ||||||||||||
| Male | 1.153 | 1.047 | 1.269 | 0.004 | 1.500 | 1.359 | 1.654 | <0.001 | 1.079 | 1.021 | 1.142 | <0.001 |
| Female | Reference | Reference | Reference | |||||||||
| Age group (years) | 0.999 | 0.996 | 1.003 | 0.719 | 1.030 | 1.026 | 1.034 | <0.001 | 1.010 | 1.009 | 1.012 | 0.008 |
| HTN | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 1.090 | 0.963 | 1.233 | 0.171 | 1.292 | 1.147 | 1.455 | <0.001 | 0.882 | 0.820 | 0.949 | 0.001 |
| IHD | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 0.975 | 0.778 | 1.222 | 0.824 | 0.810 | 0.651 | 1.007 | 0.057 | 1.200 | 1.039 | 1.387 | 0.013 |
| HCVD | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 0.890 | 0.617 | 1.283 | 0.533 | 1.148 | 0.844 | 1.562 | 0.378 | 0.645 | 0.513 | 0.812 | <0.001 |
| Stroke | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 1.106 | 0.777 | 1.574 | 0.577 | 1.921 | 1.473 | 2.506 | <0.001 | 1.063 | 0.851 | 1.328 | 0.589 |
| PUD | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 0.964 | 0.833 | 1.116 | 0.624 | 1.195 | 1.043 | 1.370 | 0.010 | 1.843 | 1.699 | 1.999 | <0.001 |
| IBD | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 0.000 | - | - | 0.858 | 0.000 | - | - | 0.916 | 0.000 | - | - | 0.999 |
| DM | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 0.825 | 0.716 | 0.951 | 0.008 | 1.303 | 1.153 | 1.472 | <0.001 | 1.216 | 1.121 | 1.319 | <0.001 |
| HF | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 0.861 | 0.498 | 1.489 | 0.593 | 2.739 | 2.023 | 3.710 | <0.001 | 1.861 | 1.364 | 2.540 | <0.001 |
| CKD | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 1.077 | 0.623 | 1.861 | 0.791 | 2.138 | 1.477 | 3.093 | <0.001 | 2.889 | 2.044 | 4.084 | <0.001 |
| Liver cirrhosis | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 0.735 | 0.594 | 0.991 | 0.005 | 1.286 | 1.092 | 1.516 | 0.003 | 1.338 | 1.192 | 1.503 | <0.001 |
| Pancreatitis | ||||||||||||
| Without | Reference | Reference | Reference | |||||||||
| With | 0.848 | 0.725 | 0.991 | 0.038 | 1.044 | 0.903 | 1.207 | 0.562 | 1.240 | 1.141 | 1.347 | <0.001 |
| Variable | Total | 1998–2013 | 2014–2015 | p | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Total | 22,996 | 53.88 | 19,686 | 85.61 | 3310 | 14.39 | |
| Diagnosis to LC (months) | <0.001 | ||||||
| Group A: 0 (at the same time) | 13,989 | 60.83 | 12,427 | 63.13 | 1562 | 47.19 | |
| Group B: >0, ≤2 | 5970 | 25.96 | 4894 | 24.86 | 1076 | 32.51 | |
| Group C: >2 | 3037 | 13.21 | 2365 | 12.01 | 672 | 20.30 | |
| Gender | <0.001 | ||||||
| Male | 11,006 | 47.86 | 9282 | 47.15 | 1724 | 52.08 | |
| Female | 11,990 | 52.14 | 10,404 | 52.85 | 1586 | 47.92 | |
| Age (years) | 58.85 ± 16.29 | 58.29 ± 16.18 | 62.19 ± 16.55 | <0.001 | |||
| Recurrence | 0.012 | ||||||
| Without | 21,310 | 92.67 | 18,208 | 92.49 | 3102 | 93.72 | |
| With | 1686 | 7.33 | 1478 | 7.51 | 208 | 6.28 | |
| Mortality | <0.001 | ||||||
| Without | 21,351 | 92.85 | 18,110 | 91.99 | 3241 | 97.92 | |
| With | 1645 | 7.15 | 1576 | 8.01 | 69 | 2.08 | |
| Complications | 0.562 | ||||||
| Without | 14,219 | 61.83 | 12,157 | 61.75 | 2062 | 62.30 | |
| With | 8777 | 38.17 | 7529 | 38.25 | 1248 | 37.70 | |
| Outcome | Recurrence | Mortality | Complications | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | Variable | Adjusted HR | 95% CI | 95% CI | p | Adjusted HR | 95% CI | 95% CI | p | Adjusted OR | 95% CI | 95% CI | p |
| Overall | Diagnosis to LC (months) | ||||||||||||
| 0 | Reference | Reference | Reference | ||||||||||
| >0, ≤2 | 0.967 | 0.855 | 1.094 | 0.596 | 1.116 | 0.985 | 1.265 | 0.085 | 0.296 | 0.275 | 0.318 | <0.001 | |
| >2 | 1.704 | 1.498 | 1.939 | <0.001 | 1.511 | 1.313 | 1.739 | <0.001 | 0.487 | 0.446 | 0.513 | <0.001 | |
| 1998–2013 | Diagnosis to LC (months) | ||||||||||||
| 0 | Reference | Reference | Reference | ||||||||||
| >0, ≤2 | 0.963 | 0.843 | 1.100 | 0.582 | 1.116 | 0.982 | 1.269 | 0.093 | 0.305 | 0.281 | 0.330 | <0.001 | |
| >2 | 1.769 | 1.540 | 2.031 | <0.001 | 1.508 | 1.304 | 1.743 | <0.001 | 0.504 | 0.457 | 0.555 | <0.001 | |
| 2014–2015 | Diagnosis to LC (months) | ||||||||||||
| 0 | Reference | Reference | Reference | ||||||||||
| >0, ≤2 | 0.813 | 0.579 | 1.143 | 0.234 | 0.983 | 0.546 | 1.770 | 0.955 | 0.243 | 0.202 | 0.293 | <0.001 | |
| >2 | 1.024 | 0.717 | 1.461 | 0.897 | 1.209 | 0.668 | 2.187 | 0.531 | 0.387 | 0.317 | 0.473 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ye, S.-L.; Hsu, S.-D.; Chien, W.-C.; Chung, C.-H. Optimal Timing of Cholecystectomy in Secondary Choledocholithiasis Patients Who Underwent Preoperative Endoscopic Retrograde Cholangiopancreatography. Appl. Sci. 2022, 12, 4574. https://0-doi-org.brum.beds.ac.uk/10.3390/app12094574
Ye S-L, Hsu S-D, Chien W-C, Chung C-H. Optimal Timing of Cholecystectomy in Secondary Choledocholithiasis Patients Who Underwent Preoperative Endoscopic Retrograde Cholangiopancreatography. Applied Sciences. 2022; 12(9):4574. https://0-doi-org.brum.beds.ac.uk/10.3390/app12094574
Chicago/Turabian StyleYe, Shang-Lin, Sheng-Der Hsu, Wu-Chien Chien, and Chi-Hsiang Chung. 2022. "Optimal Timing of Cholecystectomy in Secondary Choledocholithiasis Patients Who Underwent Preoperative Endoscopic Retrograde Cholangiopancreatography" Applied Sciences 12, no. 9: 4574. https://0-doi-org.brum.beds.ac.uk/10.3390/app12094574