Histological and Bone Morphometric Evaluation of Osseointegration Aspects by Alkali Hydrothermally-Treated Implants

Abstract
:1. Introduction
2. Materials and Methods
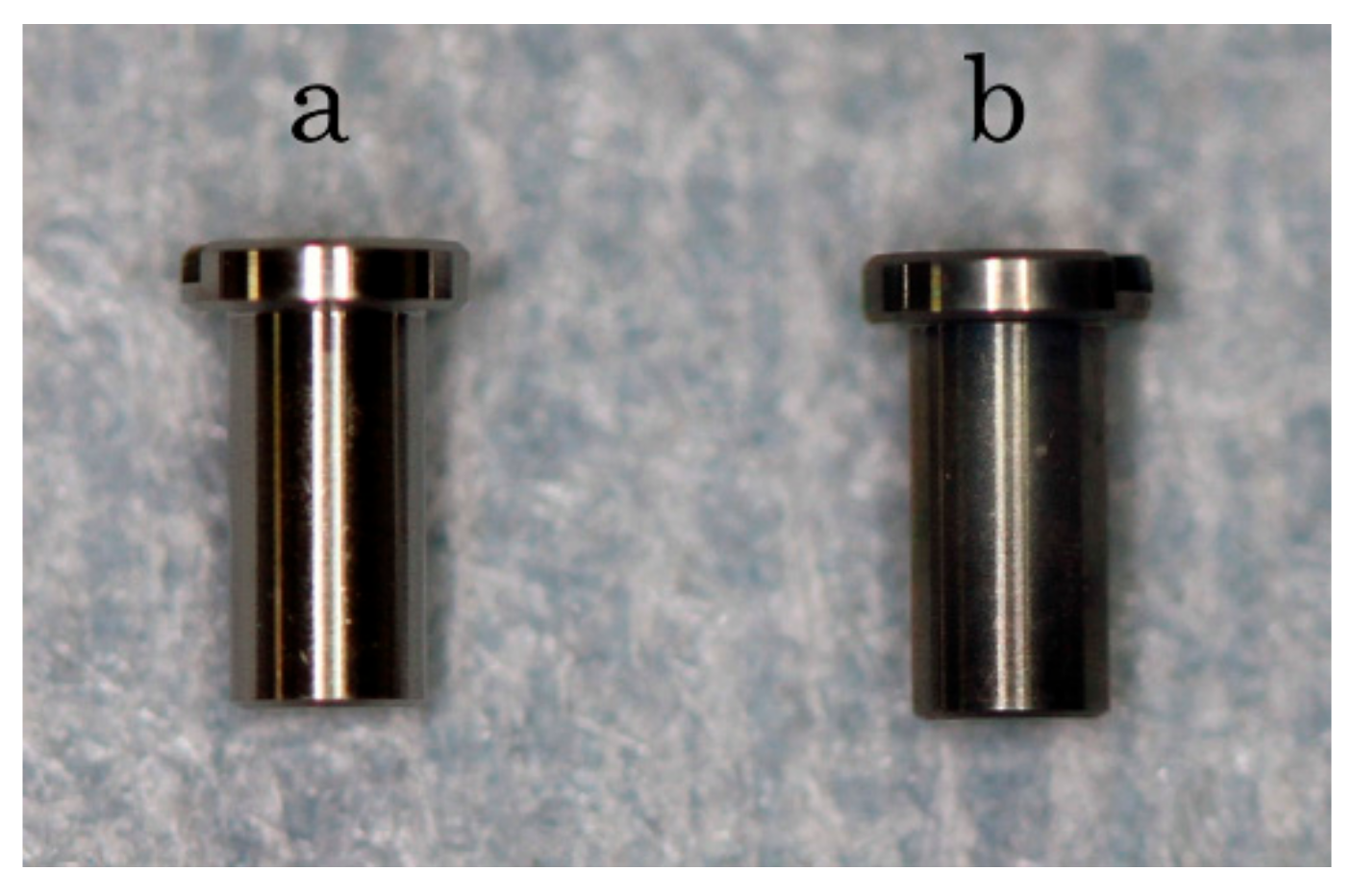
2.1. Sample Preparation
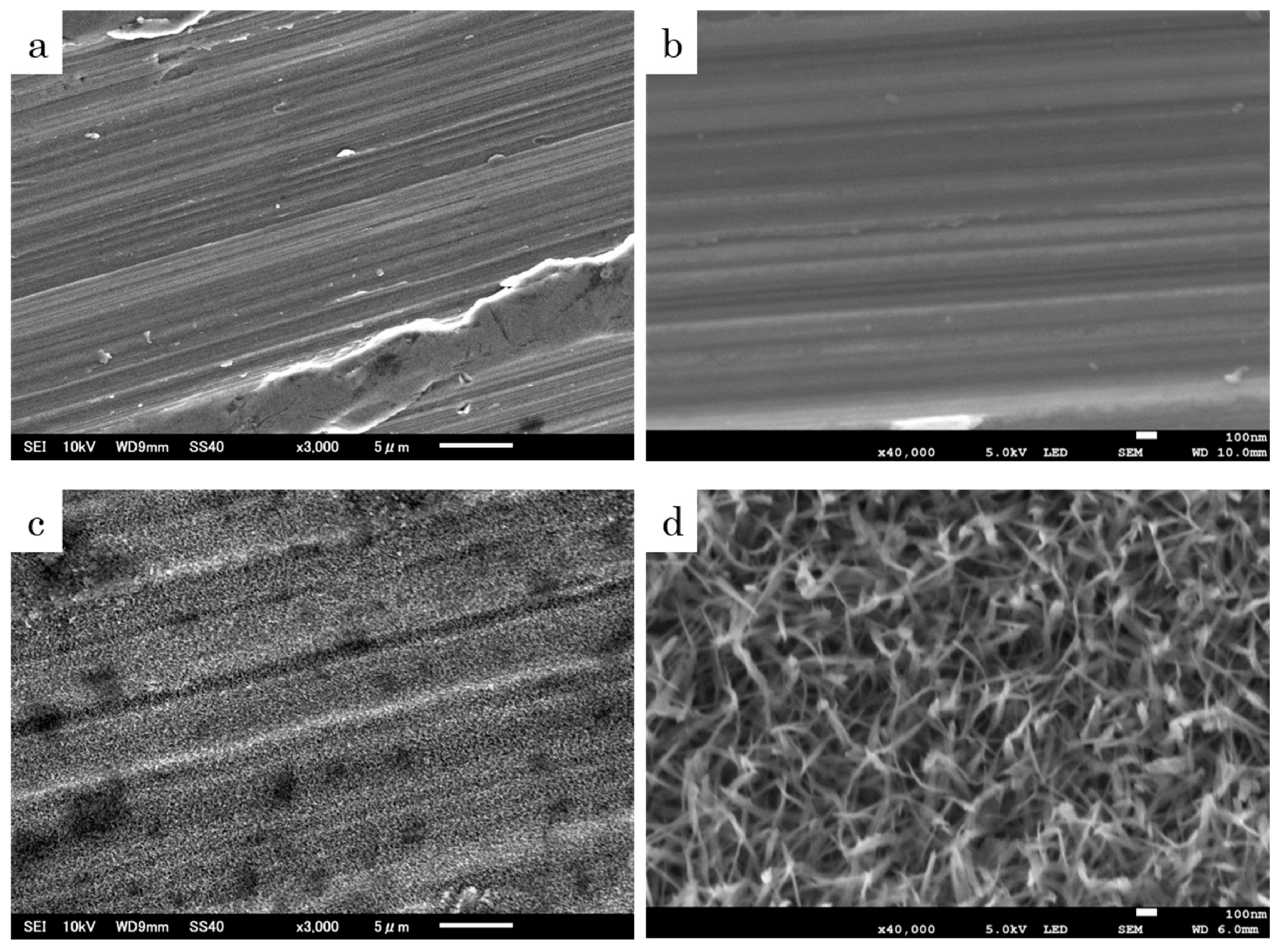
2.2. Analysis of Surface Structure
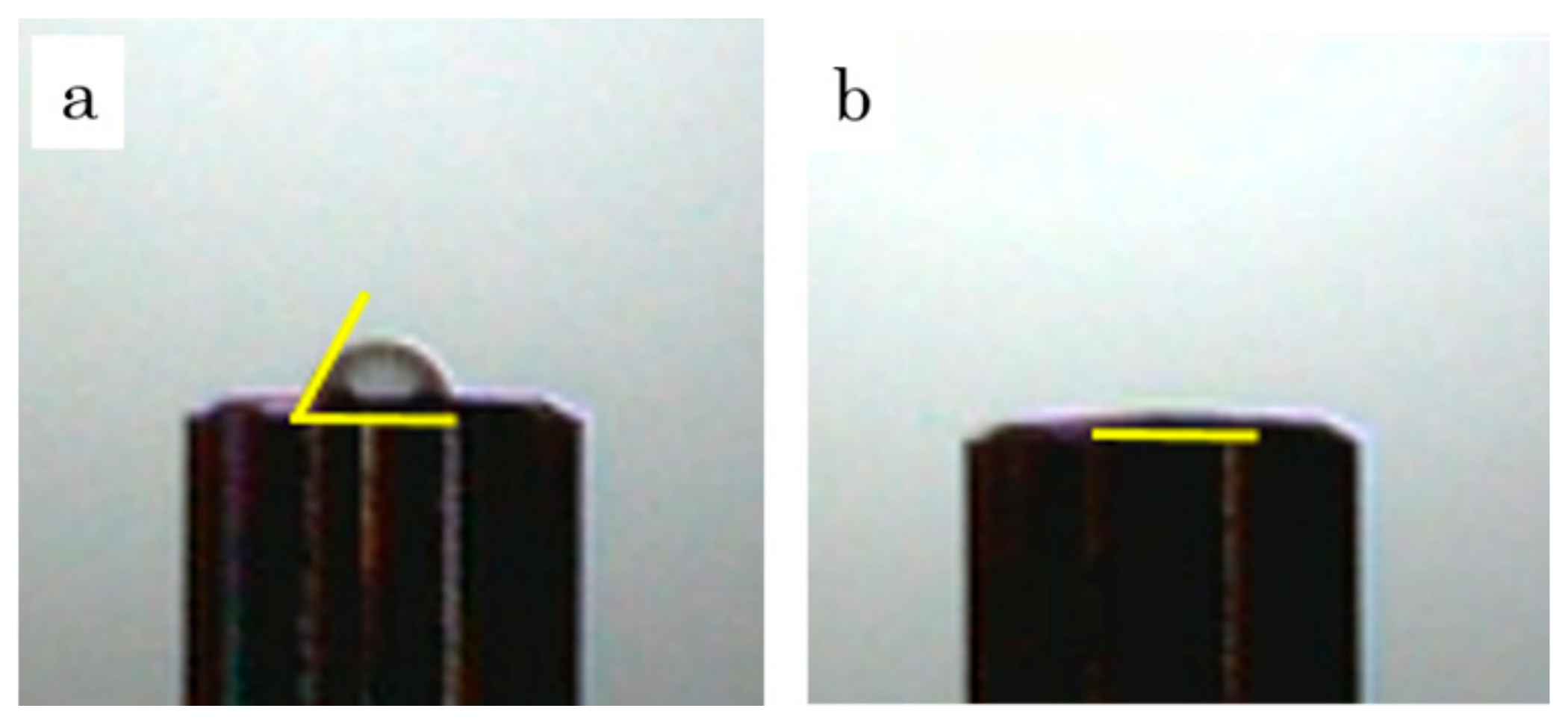
2.3. Wettability Test
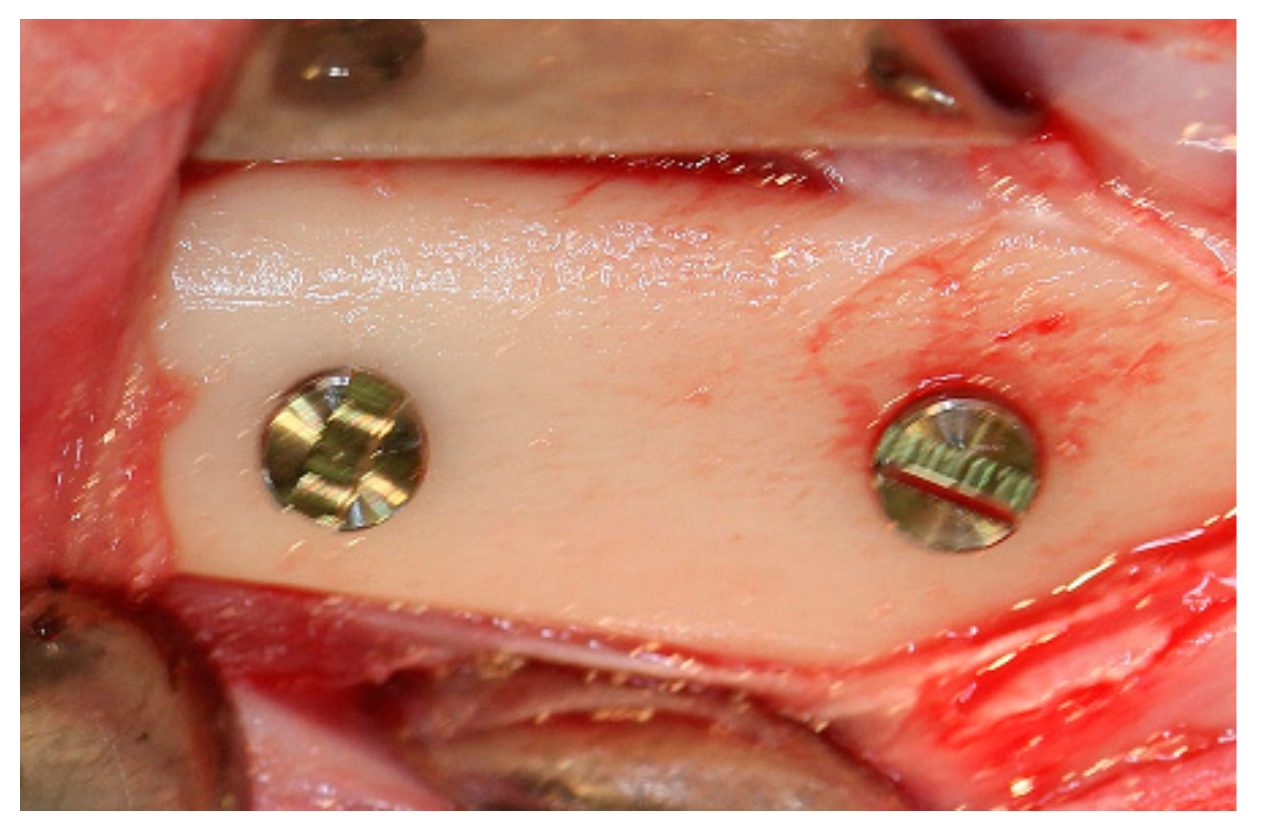
2.4. Animal Experiment
2.5. Removal Torque
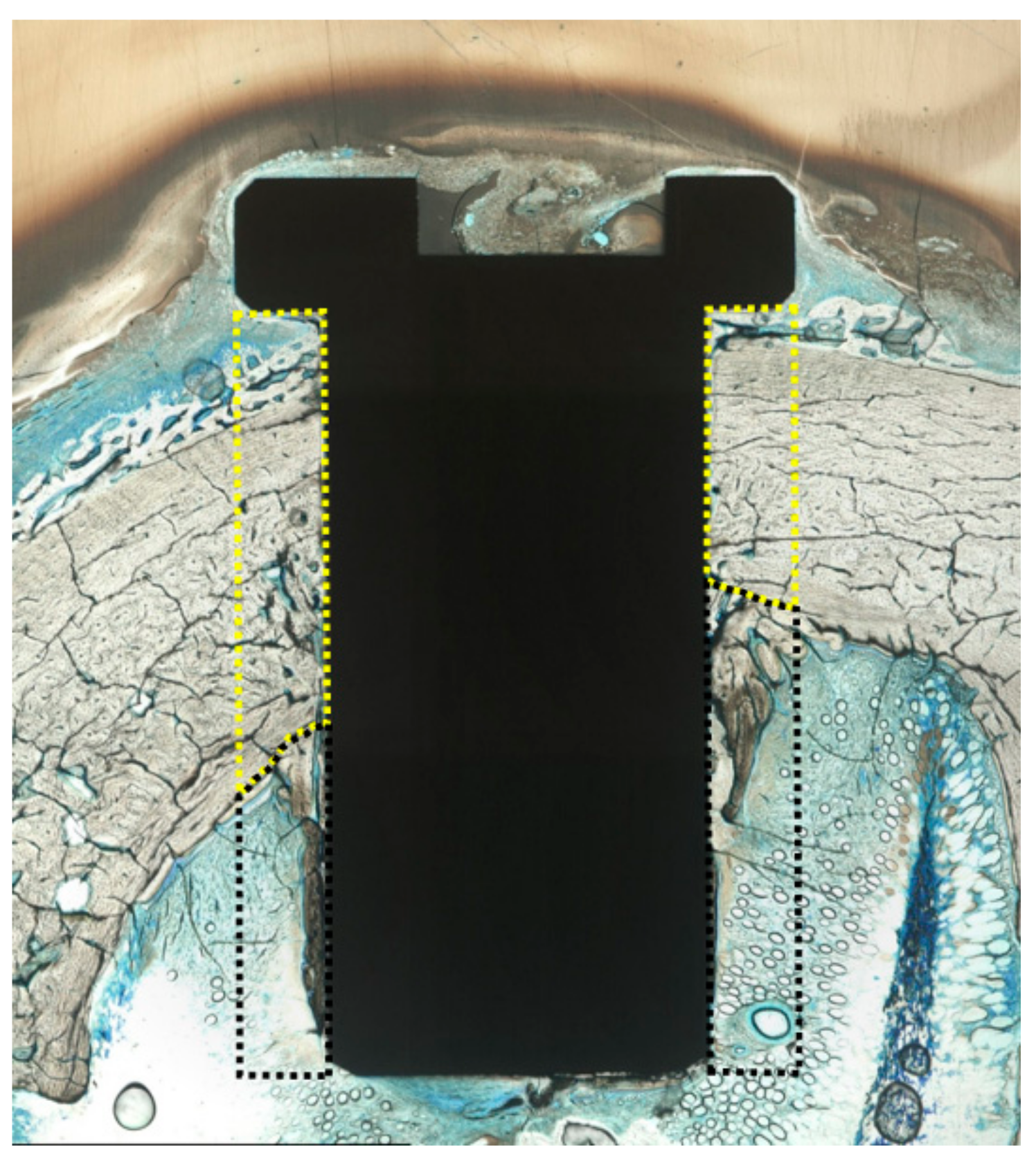
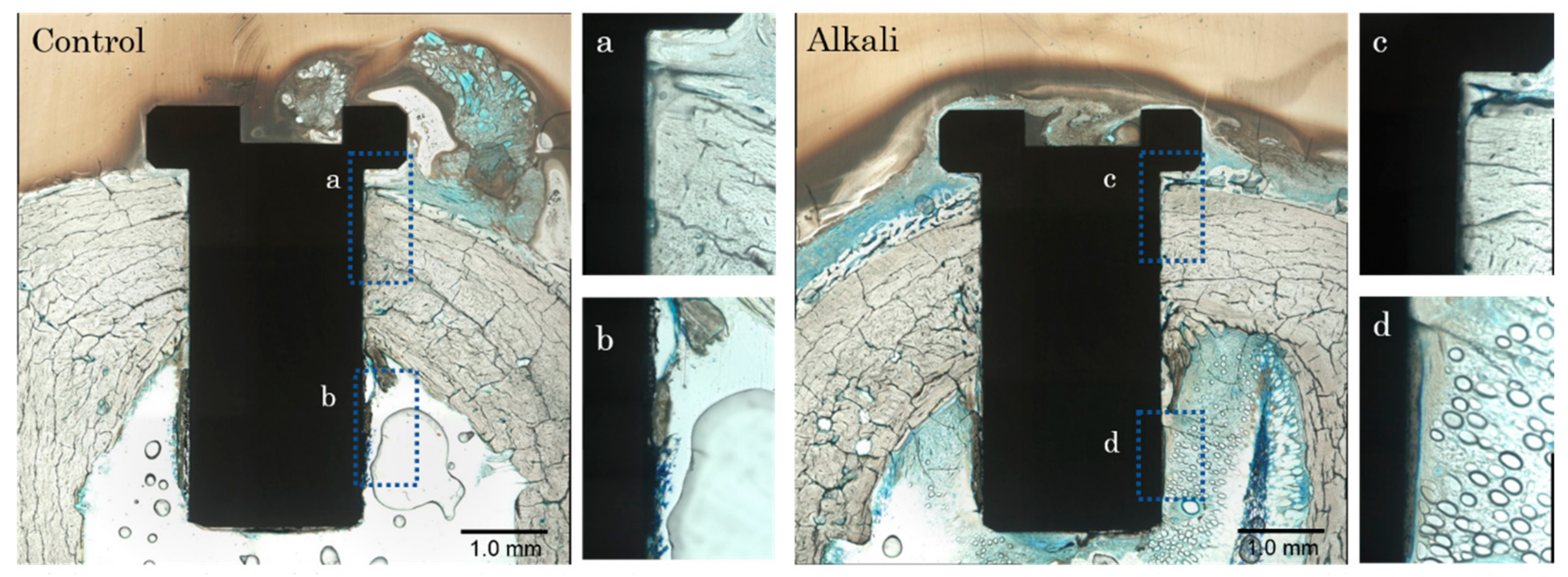
2.6. Histological Examination
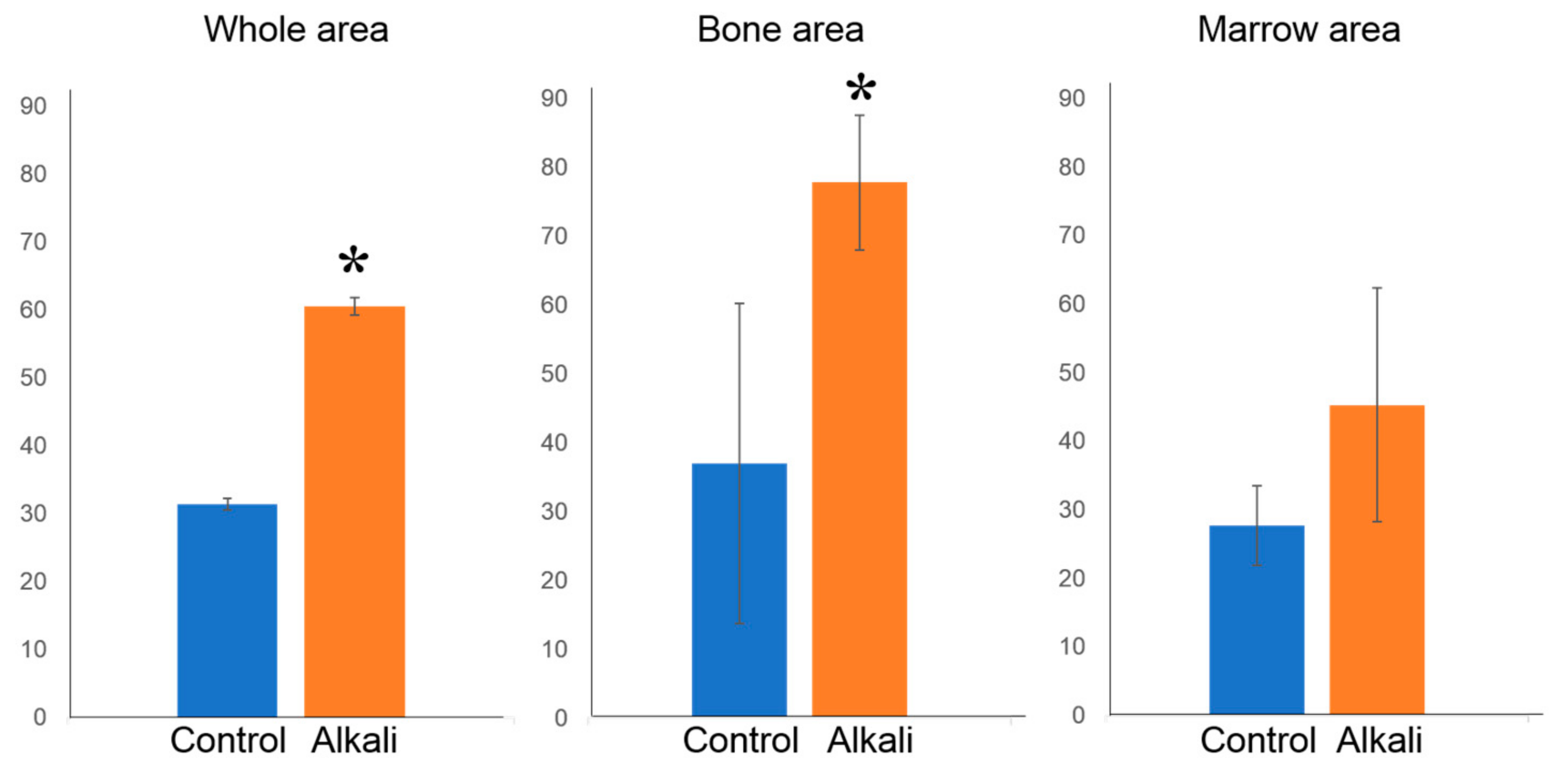
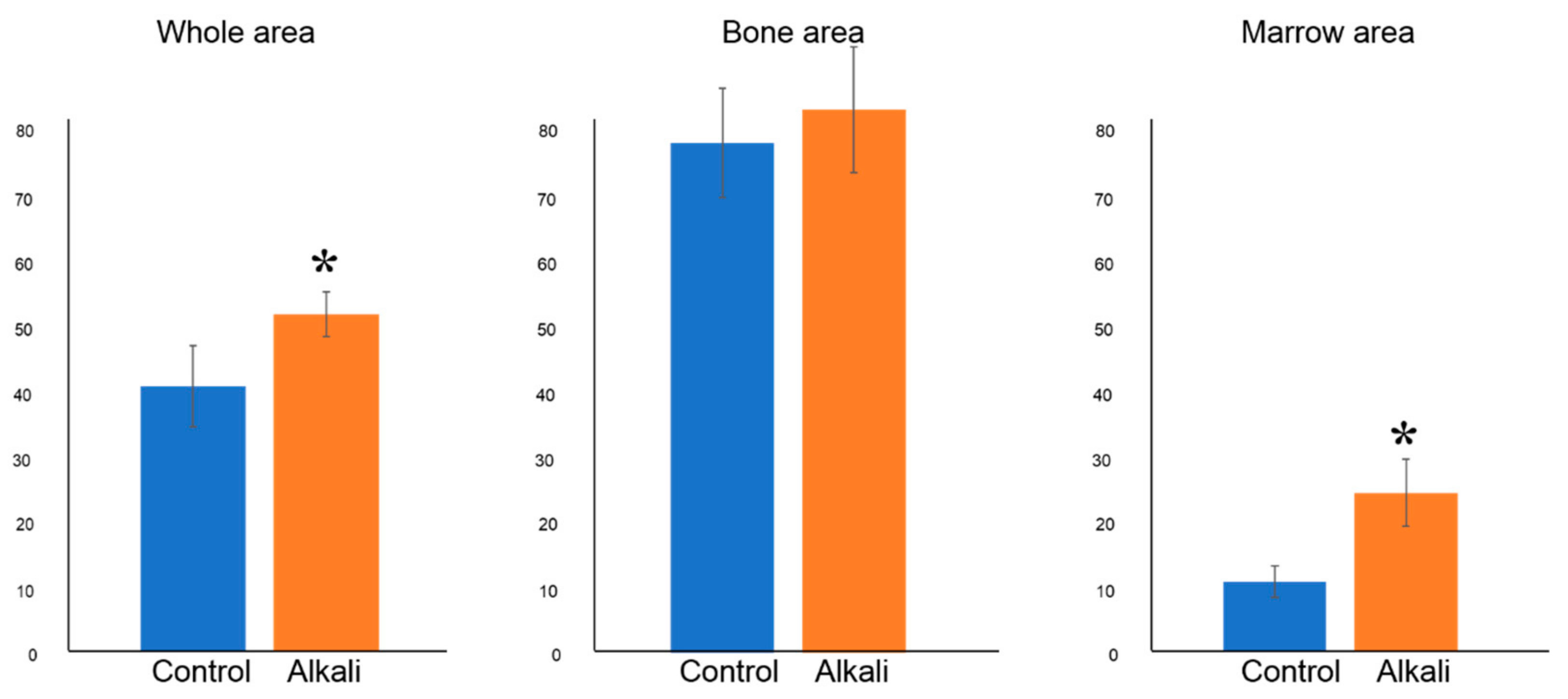
2.7. Histomorphometric Examination
2.8. Statistical Analysis
3. Results
3.1. Comparison of Surface Morphologies
3.2. Wettability Test
3.3. Removal Torque
3.4. Histological and Histomorphometric Examination
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Brånemark, P.; Zarb, G.; Albrektsson, T. Tissue-Integrated Prostheses; Quintessence Publishing: Hanover Park, IL, USA, 1985; pp. 11–43. [Google Scholar]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 Years of progress, current trends and open questions. Periodontol 2000 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Chappuis, V.; Buser, R.; Brägger, U.; Bornstein, M.M.; Salvi, G.E.; Buser, D. Long-term outcomes of dental implants with a titanium plasma-sprayed surface: A 20-year prospective case series study in partially edentulous patients. Clin. Implant Dent. Relat. Res. 2013, 15, 780–790. [Google Scholar] [CrossRef] [PubMed]
- Niinomi, M. Recent research and development in titanium alloys for biomedical applications and healthcare goods. Sci. Technol. Adv. Mater. 2003, 4, 445–454. [Google Scholar] [CrossRef]
- Le Guéhennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Iwaya, Y.; Machigashira, M.; Kanbara, K.; Miyamoto, M.; Noguchi, K.; Izumi, Y.; Ban, S. Surface properties and biocompatibility of acid-etched titanium. Dent. Mater. J. 2008, 27, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Hamouda, I.M.; Enan, E.T.; Al-Wakeel, E.E.; Yousef, M.K. Alkali and heat treatment of titanium implant material for bioactivity. Int. J. Oral Maxillofac. Implants 2012, 27, 776–784. [Google Scholar] [PubMed]
- Shi, X.; Nakagawa, M.; Kawachi, G.; Xu, L.; Ishikawa, K. Surface modification of titanium by hydrothermal treatment in Mg-containing solution and early osteoblast responses. J. Mater. Sci. Mater. Med. 2012, 23, 1281–1290. [Google Scholar] [CrossRef] [PubMed]
- Jemat, A.; Ghazali, M.J.; Razali, M.; Otsuka, Y. Surface Modifications and their effects on titanium dental implants. BioMed Res. Int. 2015, 791725. [Google Scholar] [CrossRef] [PubMed]
- Offermanns, V.; Andersen, O.Z.; Riede, G.; Sillassen, M.; Jeppesen, C.S.; Almtoft, K.P.; Talasz, H.; Öhman-Mägi, C.; Lethaus, B.; Tolba, R.; et al. Effect of strontium surface-functionalized implants on early and late osseointegration: A histological, spectrometric and tomographic evaluation. Acta Biomater. 2018, 15, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, Z.; Lohmann, C.H.; Oefinger, J.; Bonewald, L.F.; Dean, D.D.; Boyan, B.D. Implant surface characteristics modulate differentiation behavior of cells in the osteobl astic lineage. Adv. Dent. Res. 1999, 13, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 1—Review focusing on topographic and chemical properties of different surfaces and in vivo responses to them. Int. J. Prosthodont. 2004, 17, 536–543. [Google Scholar]
- Oliveira, P.T.; Zalzal, S.F.; Beloti, M.M.; Rosa, A.L.; Nanci, A. Enhancement of in vitro osteogenesis on titanium by chemically produced nanotopography. J. Biomed. Mater. Res. A. 2007, 80, 554–564. [Google Scholar] [CrossRef]
- Yao, C.; Slamovich, E.B.; Webster, T.J. Enhanced osteoblast functions on anodized titanium with nanotube-like structures. J. Biomed. Mater. Res. A. 2008, 85, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Goldman, M.; Juodzbalys, G.; Vilkinis, V. Titanium surfaces with nanostructures influence on osteoblasts proliferation: A systematic review. J. Oral Maxillofac. Res. 2014, 5, e1. [Google Scholar] [CrossRef]
- Karazisis, D.; Petronis, S.; Agheli, H.; Emanuelsson, L.; Norlindh, B.; Johansson, A.; Rasmusson, L.; Thomsen, P.; Omar, O. The influence of controlled surface nanotopography on the early biological events of osseointegration. Acta Biomater. 2017, 15, 559–571. [Google Scholar] [CrossRef] [PubMed]
- Kokubo, T.; Miyaji, F.; Kim, H.M. Spontaneous formation of bone like apatite layer on chemically treated titanium metals. J. Am. Ceram. Soc. 1996, 79, 1127–1129. [Google Scholar] [CrossRef]
- Ban, S.; Iwaya, Y.; Kono, H.; Sato, H. Surface modification of titanium by etching in concentrated sulfuric acid. Dent. Mater. 2006, 22, 1115–1120. [Google Scholar] [CrossRef] [PubMed]
- Kono, H.; Miyamoto, M.; Ban, S. Bioactive Apatite coating on titanium using an alternate soaking process. Dent. Mater. J. 2007, 26, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Kobatake, R.; Doi, K.; Oki, Y.; Umehara, H.; Kawano, H.; Kubo, T.; Tsuga, K. Investigation of effective modification treatments for titanium membranes. Appl. Sci. 2017, 7, 1022. [Google Scholar] [CrossRef]
- Zhuang, X.M.; Zhou, B.; Ouyang, J.L.; Sun, H.P.; Wu, Y.L.; Liu, Q.; Deng, F.L. Enhanced MC3T3-E1 preosteoblast response and bone formation on the addition of nano-needle and nano-porous features to microtopographical titanium surfaces. Biomed. Mater. 2014, 9, 045001. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Yang, F.; Zheng, X.; Ding, C.; Dai, K.; Huang, L. Nano-structured titanium coating for improving biological performance. Nanosci. Nanotechnol. 2011, 11, 10770–10773. [Google Scholar] [CrossRef]
- Mendonça, G.; Mendonça, D.B.; Aragão, F.J.; Cooper, L.F. Advancing dental implant surface technology—From micron- to nanotopography. Biomaterials 2008, 29, 3822–3835. [Google Scholar] [CrossRef] [PubMed]
- Camargo, W.A.; Takemoto, S.; Hoekstra, J.W.; Leeuwenburgh, S.C.G.; Jansen, J.A.; van den Beucken, J.J.J.P.; Alghamdi, H.S. Effect of surface alkali-based treatment of titanium implants on ability to promote in vitro mineralization and in vivo bone formation. Acta Biomater. 2017, 57, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Takemoto, M.; Fujibayashi, S.; Akiyama, H.; Tanaka, M.; Yamaguchi, S.; Deepak, K.P.; Kenji, D.; Tomiharu, M.; Takashi, N.; et al. Osteoinduction on acid and heat treated porous Ti metal samples in canine muscle. PLoS ONE 2014, 9, e88366. [Google Scholar] [CrossRef] [PubMed]
- Dalby, M.J.; McCloy, D.; Robertson, M.; Wilkinson, C.D.; Oreffo, R.O. Osteoprogenitor response to defined topographies with nanoscale depths. Biomaterials 2006, 27, 1306–1315. [Google Scholar] [CrossRef]
- Kim, H.M.; Miyaji, F.; Kokubo, T.; Nakamura, T. Preparation of bioactive Ti and its alloys via simple chemical surface treatment. J. Biomed. Mater. Res. 1996, 32, 409–417. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Kato, H.; Neo, M.; Oka, M.; Kim, H.M.; Kokubo, T.; Nakamura, T. Alkali-and heat-treated porous titanium for orthopedic implants. J. Biomed. Mater. Res. 2001, 54, 198–208. [Google Scholar] [CrossRef]
- Nishiguchi, S.; Fujibayashi, S.; Kim, H.M.; Kokubo, T.; Nakamura, T. Biology of alkali-and heat-treated titanium implants. J. Biomed. Mater. 2003, 67, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.S.; Lee, T.M.; Chang, C.H.; Liu, J.K. The effect of microrough surface treatment on miniscrews used as orthodontic anchors. Clin. Oral Implants Res. 2009, 20, 1178–1184. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, L.; Röstlund, T.; Albrektsson, B.; Albrektsson, T. Removal torques for polished and rough titanium implants. Int. J. Oral Maxillofac. Implants 1988, 3, 21–24. [Google Scholar] [PubMed]
- Oki, Y.; Doi, K.; Makihara, Y.; Kobatake, R.; Kubo, T.; Tsuga, K. Effects of continual intermittent administration of parathyroid hormone on implant stability in the presence of osteoporosis: An in vivo study using resonance frequency analysis in a rabbit model. J. Appl. Oral Sci. 2017, 25, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, Y.; Doi, K.; Oki, Y.; Kobatake, R.; Abe, Y.; Tsuga, K. Enhanced osseointegration of a modified titanium implant with bound phospho-threonine: A preliminary in vivo study. J. Funct. Biomater. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, I.; Huang, Y.; Butz, F.; Ogawa, T.; Lin, A.; Wang, C.J. Discrete deposition of hydroxyapatite nanoparticles on a titanium implant with predisposing substrate microtopography accelerated osseointegration. Nanotechnology 2007, 18, 245101. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | °(±SD) |
|---|---|
| Control | 79.0 ± 2.3 * |
| Alkali | almost 0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Umehara, H.; Kobatake, R.; Doi, K.; Oki, Y.; Makihara, Y.; Kubo, T.; Tsuga, K. Histological and Bone Morphometric Evaluation of Osseointegration Aspects by Alkali Hydrothermally-Treated Implants. Appl. Sci. 2018, 8, 635. https://0-doi-org.brum.beds.ac.uk/10.3390/app8040635
Umehara H, Kobatake R, Doi K, Oki Y, Makihara Y, Kubo T, Tsuga K. Histological and Bone Morphometric Evaluation of Osseointegration Aspects by Alkali Hydrothermally-Treated Implants. Applied Sciences. 2018; 8(4):635. https://0-doi-org.brum.beds.ac.uk/10.3390/app8040635
Chicago/Turabian StyleUmehara, Hanako, Reiko Kobatake, Kazuya Doi, Yoshifumi Oki, Yusuke Makihara, Takayasu Kubo, and Kazuhiro Tsuga. 2018. "Histological and Bone Morphometric Evaluation of Osseointegration Aspects by Alkali Hydrothermally-Treated Implants" Applied Sciences 8, no. 4: 635. https://0-doi-org.brum.beds.ac.uk/10.3390/app8040635