High-Intensity Interval Training Improves Cognitive Flexibility in Older Adults

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
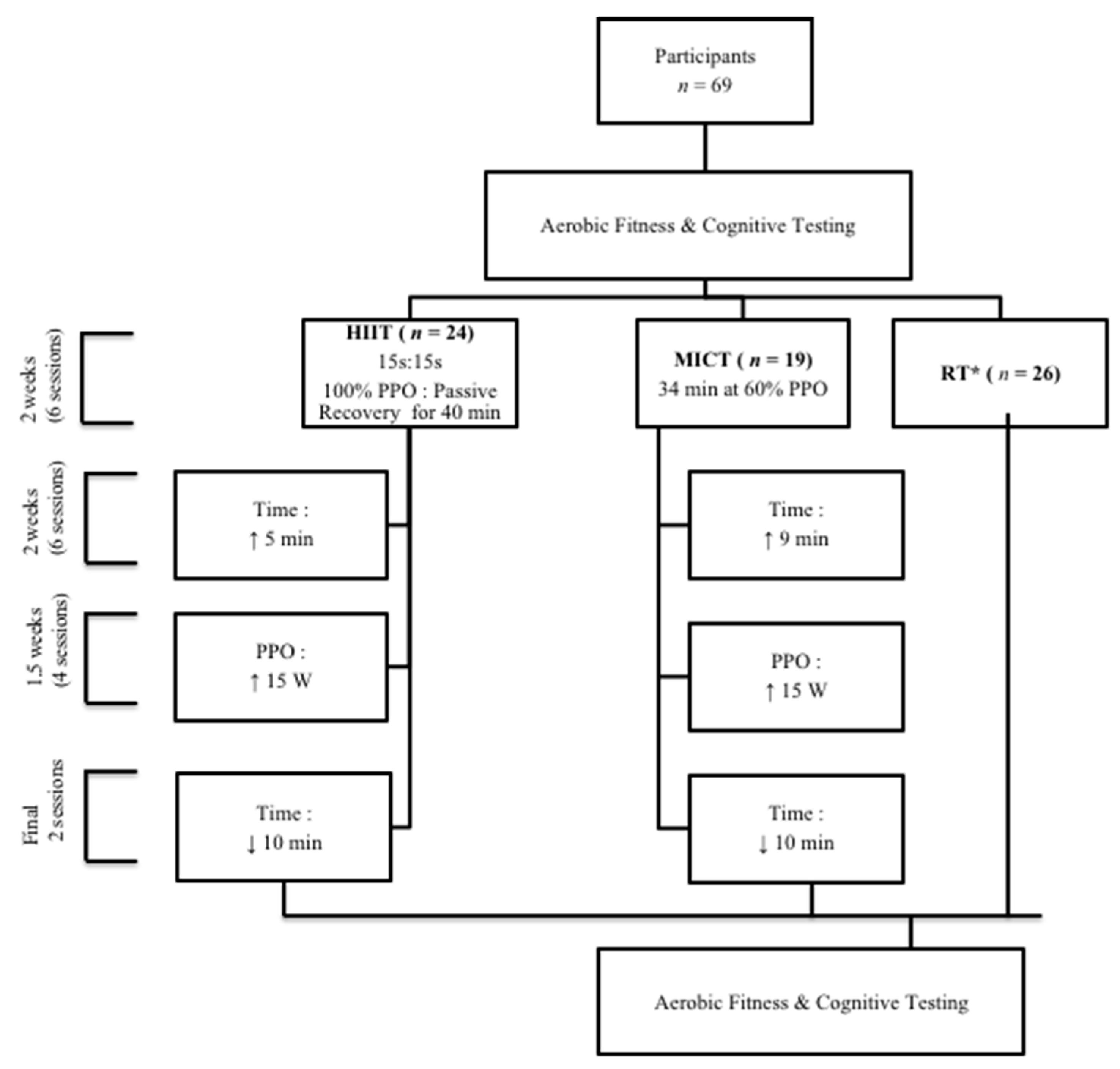
2.2. Experimental Design
2.3. Maximal Continuous Graded Exercise Test
2.4. Exercise Training Protocols
2.5. Cognitive Testing
2.6. Data and Statistical Analyses
3. Results
3.1. Participant Characteristics
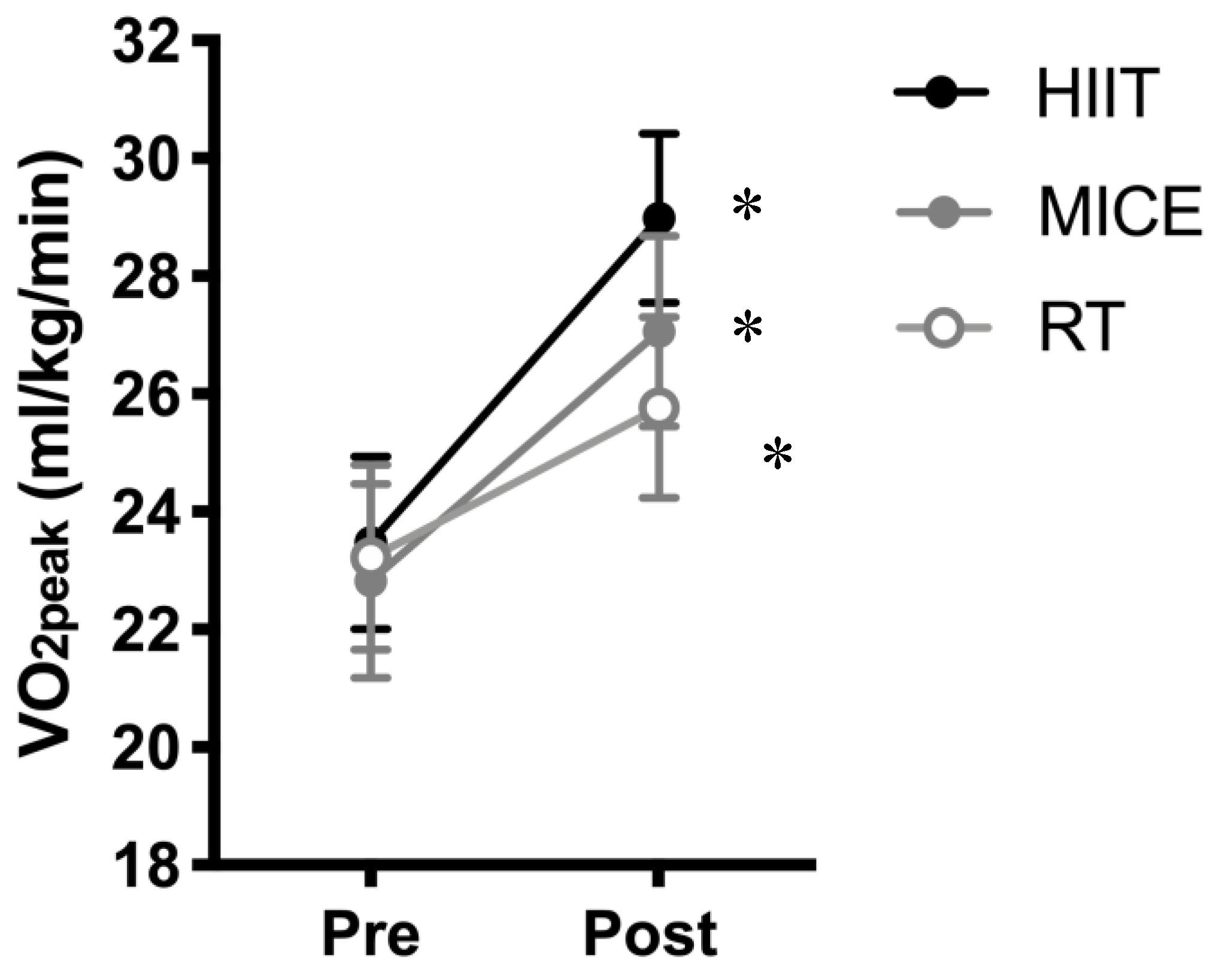
3.2. Cardiorespiratory Fitness
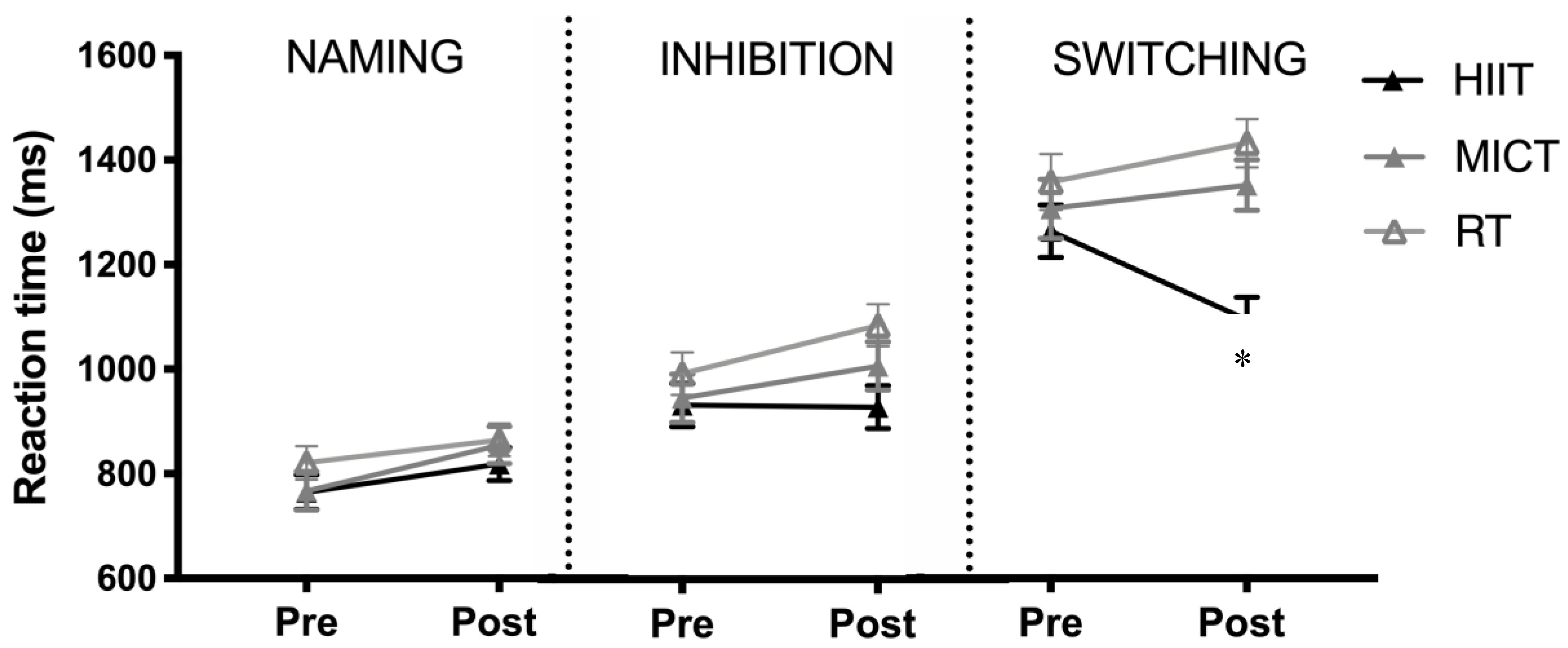
3.3. Cognitive Task
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fjell, A.M.; Sneve, M.H.; Grydeland, H.; Storsve, A.B.; Walhovd, K.B. The Disconnected Brain and Executive Function Decline in Aging. Cereb. Cortex 2017, 27, 2303–2317. [Google Scholar] [CrossRef] [PubMed]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: A latent variable analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, L.R.; Schiehser, D.M.; Weissberger, G.H.; Salmon, D.P.; Delis, D.C.; Bondi, M.W. Specific measures of executive function predict cognitive decline in older adults. J. Int. Neuropsychol. Soc. 2012, 18, 118–127. [Google Scholar] [CrossRef] [Green Version]
- Levy, G.; Jacobs, D.M.; Tang, M.X.; Côté, L.J.; Louis, E.D.; Alfaro, B.; Mejia, H.; Stern, Y.; Marder, K. Memory and executive function impairment predict dementia in Parkinson’s disease. Mov. Disord. 2002, 17, 1221–1226. [Google Scholar] [CrossRef] [PubMed]
- CM, M. The Stroop task: The “gold standard” of attentional measures. J. Exp. Psychol. Gen. 1992, 121, 12–14. [Google Scholar]
- Sinai, M.; Phillips, N.A.; Chertkow, H.; Kabani, N.J. Task switching performance reveals heterogeneity amongst patients with mild cognitive impairment. Neuropsychology 2010, 24, 757–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekari, S.; Earle, M.; Martins, R.; Drisdelle, S.; Killen, M.; Bouffard-Levasseur, V.; Dupuy, O. Effect of High Intensity Interval Training Compared to Continuous Training on Cognitive Performance in Young Healthy Adults: A Pilot Study. Brain Sci. 2020, 10, 81. [Google Scholar] [CrossRef] [Green Version]
- Goenarjo, R.; Bosquet, L.; Berryman, N.; Metier, V.; Perrochon, A.; Fraser, S.A.; Dupuy, O. Cerebral Oxygenation Reserve: The Relationship Between Physical Activity Level and the Cognitive Load During a Stroop Task in Healthy Young Males. Int. J. Environ. Res. Public Health 2020, 17, 1406. [Google Scholar] [CrossRef] [Green Version]
- Dupuy, O.; Gauthier, C.J.; Fraser, S.A.; Desjardins-Crepeau, L.; Desjardins, M.; Mekary, S.; Lesage, F.; Hoge, R.D.; Pouliot, P.; Bherer, L. Higher levels of cardiovascular fitness are associated with better executive function and prefrontal oxygenation in younger and older women. Front. Hum. Neurosci. 2015, 9, 66. [Google Scholar] [CrossRef] [Green Version]
- Shea, T.B.; Remington, R. Cognitive Improvement in Healthy Older Adults Can Parallel That of Younger Adults Following Lifestyle Modification: Support for Cognitive Reserve During Aging. J. Alzheimers Dis. Rep. 2018, 2, 201–205. [Google Scholar] [CrossRef] [Green Version]
- Kawagoe, T.; Onoda, K.; Yamaguchi, S. Associations among executive function, cardiorespiratory fitness, and brain network properties in older adults. Sci. Rep. 2017, 7, 40107. [Google Scholar] [CrossRef] [Green Version]
- Guiney, H.; Machado, L. Benefits of regular aerobic exercise for executive functioning in healthy populations. Psychon Bull. Rev. 2013, 20, 73–86. [Google Scholar] [CrossRef]
- Sáez de Asteasu, M.L.; Martínez-Velilla, N.; Zambom-Ferraresi, F.; Casas-Herrero, Á.; Izquierdo, M. Role of physical exercise on cognitive function in healthy older adults: A systematic review of randomized clinical trials. Ageing Res. Rev. 2017, 37, 117–134. [Google Scholar] [CrossRef] [PubMed]
- Weston, K.S.; Wisløff, U.; Coombes, J.S. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Br. J. Sports Med. 2014, 48, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Ramos, J.S.; Dalleck, L.C.; Tjonna, A.E.; Beetham, K.S.; Coombes, J.S. The impact of high-intensity interval training versus moderate-intensity continuous training on vascular function: A systematic review and meta-analysis. Sports Med. 2015, 45, 679–692. [Google Scholar] [CrossRef]
- Calverley, T.A.; Ogoh, S.; Marley, C.J.; Steggall, M.; Marchi, N.; Brassard, P.; Lucas, S.J.E.; Cotter, J.D.; Roig, M.; Ainslie, P.N.; et al. HIITing the brain with exercise: Mechanisms, consequences and practical recommendations. J. Physiol. 2020, 598, 2513–2530. [Google Scholar] [CrossRef]
- Lucas, S.J.; Cotter, J.D.; Brassard, P.; Bailey, D.M. High-intensity interval exercise and cerebrovascular health: Curiosity, cause, and consequence. J. Cereb. Blood Flow Metab. 2015, 35, 902–911. [Google Scholar] [CrossRef] [PubMed]
- Van Gelder, B.M.; Tijhuis, M.A.; Kalmijn, S.; Giampaoli, S.; Nissinen, A.; Kromhout, D. Physical activity in relation to cognitive decline in elderly men: The FINE Study. Neurology 2004, 63, 2316–2321. [Google Scholar] [CrossRef] [PubMed]
- Angevaren, M.; Vanhees, L.; Wendel-Vos, W.; Verhaar, H.J.; Aufdemkampe, G.; Aleman, A.; Verschuren, W.M. Intensity, but not duration, of physical activities is related to cognitive function. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 825–830. [Google Scholar] [CrossRef]
- Brown, B.M.; Peiffer, J.J.; Sohrabi, H.R.; Mondal, A.; Gupta, V.B.; Rainey-Smith, S.R.; Taddei, K.; Burnham, S.; Ellis, K.A.; Szoeke, C.; et al. Intense physical activity is associated with cognitive performance in the elderly. Transl. Psychiatry 2012, 2, e191. [Google Scholar] [CrossRef] [Green Version]
- Jimenez-Maldonado, A.; Renteria, I.; Garcia-Suarez, P.C.; Moncada-Jimenez, J.; Freire-Royes, L.F. The Impact of High-Intensity Interval Training on Brain Derived Neurotrophic Factor in Brain: A Mini-Review. Front Neurosci. 2018, 12, 839. [Google Scholar] [CrossRef] [PubMed]
- Cotman, C.W.; Berchtold, N.C. Exercise: A behavioral intervention to enhance brain health and plasticity. Trends Neurosci. 2002, 25, 295–301. [Google Scholar] [CrossRef]
- Cotman, C.W.; Berchtold, N.C.; Christie, L.A. Exercise builds brain health: Key roles of growth factor cascades and inflammation. Trends Neurosci. 2007, 30, 464–472. [Google Scholar] [CrossRef]
- Freitas, D.A.; Rocha-Vieira, E.; De Sousa, R.A.L.; Soares, B.A.; Rocha-Gomes, A.; Chaves Garcia, B.C.; Cassilhas, R.C.; Mendonca, V.A.; Camargos, A.C.R.; De Gregorio, J.A.M.; et al. High-intensity interval training improves cerebellar antioxidant capacity without affecting cognitive functions in rats. Behav. Brain Res. 2019, 376, 112181. [Google Scholar] [CrossRef] [PubMed]
- Nicolini, C.; Toepp, S.; Harasym, D.; Michalski, B.; Fahnestock, M.; Gibala, M.J.; Nelson, A.J. No changes in corticospinal excitability, biochemical markers, and working memory after six weeks of high-intensity interval training in sedentary males. Physiol. Rep. 2019, 7, e14140. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.K.; Ha, C.H. The effect of exercise intensity on brain derived neurotrophic factor and memory in adolescents. Environ. Health Prev. Med. 2017, 22, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovacevic, A.; Fenesi, B.; Paolucci, E.; Heisz, J.J. The effects of aerobic exercise intensity on memory in older adults. Appl. Physiol. Nutr. Metab. 2019. [Google Scholar] [CrossRef]
- Moreau, D.; Kirk, I.J.; Waldie, K.E. High-intensity training enhances executive function in children in a randomized, placebo-controlled trial. Elife 2017, 6. [Google Scholar] [CrossRef]
- Pallesen, H.; Bjerk, M.; Pedersen, A.R.; Nielsen, J.F.; Evald, L. The Effects of High-Intensity Aerobic Exercise on Cognitive Performance After Stroke: A Pilot Randomised Controlled Trial. J. Cent. Nerv. Syst. Dis. 2019, 11. [Google Scholar] [CrossRef] [Green Version]
- Venckunas, T.; Snieckus, A.; Trinkunas, E.; Baranauskiene, N.; Solianik, R.; Juodsnukis, A.; Streckis, V.; Kamandulis, S. Interval Running Training Improves Cognitive Flexibility and Aerobic Power of Young Healthy Adults. J. Strength Cond. Res. 2016, 30, 2114–2121. [Google Scholar] [CrossRef]
- Coetsee, C.; Terblanche, E. The effect of three different exercise training modalities on cognitive and physical function in a healthy older population. Eur. Rev. Aging Phys. Act. 2017, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports, M. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Berryman, N.; Bherer, L.; Nadeau, S.; Lauzière, S.; Lehr, L.; Bobeuf, F.; Lussier, M.; Kergoat, M.J.; Vu, T.T.; Bosquet, L. Multiple roads lead to Rome: Combined high-intensity aerobic and strength training vs. gross motor activities leads to equivalent improvement in executive functions in a cohort of healthy older adults. Age 2014, 36, 9710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kernan, W.N.; Viscoli, C.M.; Makuch, R.W.; Brass, L.M.; Horwitz, R.I. Stratified randomization for clinical trials. J. Clin. Epidemiol. 1999, 52, 19–26. [Google Scholar] [CrossRef]
- O’Brien, M.W.; Johns, J.A.; Robinson, S.A.; Bungay, A.; Mekary, S.; Kimmerly, D.S. Impact of High-Intensity Interval Training, Moderate-Intensity Continuous Training, and Resistance Training on Endothelial Function in Older Adults. Med. Sci. Sports Exerc. 2020, 52, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Francois, M.E.; Little, J.P. Effectiveness and safety of high-intensity interval training in patients with type 2 diabetes. Diabetes Spectr. 2015, 28, 39–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guiraud, T.; Nigam, A.; Gremeaux, V.; Meyer, P.; Juneau, M.; Bosquet, L. High-intensity interval training in cardiac rehabilitation. Sports Med. 2012, 42, 587–605. [Google Scholar] [CrossRef]
- Ainslie, P.N.; Cotter, J.D.; George, K.P.; Lucas, S.; Murrell, C.; Shave, R.; Thomas, K.N.; Williams, M.J.; Atkinson, G. Elevation in cerebral blood flow velocity with aerobic fitness throughout healthy human ageing. J. Physiol. 2008, 586, 4005–4010. [Google Scholar] [CrossRef]
- Mekari, S.; Dupuy, O.; Martins, R.; Evans, K.; Kimmerly, D.S.; Fraser, S.; Neyedli, H.F. The effects of cardiorespiratory fitness on executive function and prefrontal oxygenation in older adults. Geroscience 2019, 41, 681–690. [Google Scholar] [CrossRef]
- Predovan, D.; Fraser, S.A.; Renaud, M.; Bherer, L. The effect of three months of aerobic training on stroop performance in older adults. J. Aging Res. 2012, 2012, 269815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angelini, A.; Bendini, C.; Neviani, F.; Bergamini, L.; Manni, B.; Trenti, T.; Rovati, R.; Neri, M. Insulin-like growth factor-1 (IGF-1): Relation with cognitive functioning and neuroimaging marker of brain damage in a sample of hypertensive elderly subjects. Arch. Gerontol. Geriatr. 2009, 49 (Suppl. 1), 5–12. [Google Scholar] [CrossRef]
- Herbert, P.; Hayes, L.D.; Sculthorpe, N.; Grace, F.M. High-intensity interval training (HIIT) increases insulin-like growth factor-I (IGF-I) in sedentary aging men but not masters’ athletes: An observational study. Aging Male 2017, 20, 54–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guadagni, V.; Drogos, L.L.; Tyndall, A.V.; Davenport, M.H.; Anderson, T.J.; Eskes, G.A.; Longman, R.S.; Hill, M.D.; Hogan, D.B.; Poulin, M.J. Aerobic exercise improves cognition and cerebrovascular regulation in older adults. Neurology 2020, 94, e2245–e2257. [Google Scholar] [CrossRef] [PubMed]
- Barha, C.K.; Davis, J.C.; Falck, R.S.; Nagamatsu, L.S.; Liu-Ambrose, T. Sex differences in exercise efficacy to improve cognition: A systematic review and meta-analysis of randomized controlled trials in older humans. Front. Neuroendocr. 2017, 46, 71–85. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| HIIT | MICT | RT | |||||||
|---|---|---|---|---|---|---|---|---|---|
| PRE | POST | ES | PRE | POST | ES | PRE | POST | ES | |
| Sex | 15 F, 9 M | -- | 10 F, 9 M | -- | 17 F, 9 M | -- | |||
| Age | 67 ± 5 | -- | 68 ± 7 | -- | 67 ± 7 | -- | |||
| Height (m) | 1.6 ± 0.1 | -- | 1.7 ± 0.1 | -- | 1.6 ± 0.1 | -- | |||
| Weight (kg) | 73 ± 12 | 73 ± 11 | 0.0 | 75 ± 13 | 75 ± 13 | 0.0 | 74 ± 12 | 75 ± 14 | 0.0 |
| BMI (kg/m2) | 26 ± 4 | 26 ± 4 | 0.0 | 26 ± 4 | 26 ± 4 | 0.0 | 26 ± 7 | 27 ± 4 | 0.0 |
| MMSE | 29 ± 1 | 29 ± 1 | 28 + 1 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mekari, S.; Neyedli, H.F.; Fraser, S.; O’Brien, M.W.; Martins, R.; Evans, K.; Earle, M.; Aucoin, R.; Chiekwe, J.; Hollohan, Q.; et al. High-Intensity Interval Training Improves Cognitive Flexibility in Older Adults. Brain Sci. 2020, 10, 796. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110796
Mekari S, Neyedli HF, Fraser S, O’Brien MW, Martins R, Evans K, Earle M, Aucoin R, Chiekwe J, Hollohan Q, et al. High-Intensity Interval Training Improves Cognitive Flexibility in Older Adults. Brain Sciences. 2020; 10(11):796. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110796
Chicago/Turabian StyleMekari, Said, Heather F. Neyedli, Sarah Fraser, Myles W. O’Brien, Ricardo Martins, Kailey Evans, Meghan Earle, Rachelle Aucoin, Joy Chiekwe, Quinn Hollohan, and et al. 2020. "High-Intensity Interval Training Improves Cognitive Flexibility in Older Adults" Brain Sciences 10, no. 11: 796. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110796