The Role of the T2–FLAIR Mismatch Sign as an Imaging Marker of IDH Status in a Mixed Population of Low- and High-Grade Gliomas

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Histological Diagnosis and Molecular Typing
2.4. Imaging Protocol
2.5. Statistical Analysis
3. Results
3.1. Study Sample Description
- Kappa = 0.647 (95% CI: 0.337–0.957).
- Kappa interpretation:
- Kappa < 0: no agreement.
- Kappa between 0.00 and 0.20: slight agreement.
- Kappa between 0.21 and 0.40: fair agreement.
- Kappa between 0.41 and 0.60: moderate agreement.
- Kappa between 0.61 and 0.80: substantial agreement.
- Kappa between 0.81 and 1.00: almost perfect agreement.
3.2. Agreement between the Two Reviewers
3.3. Logistic Regression
3.4. Probabilities
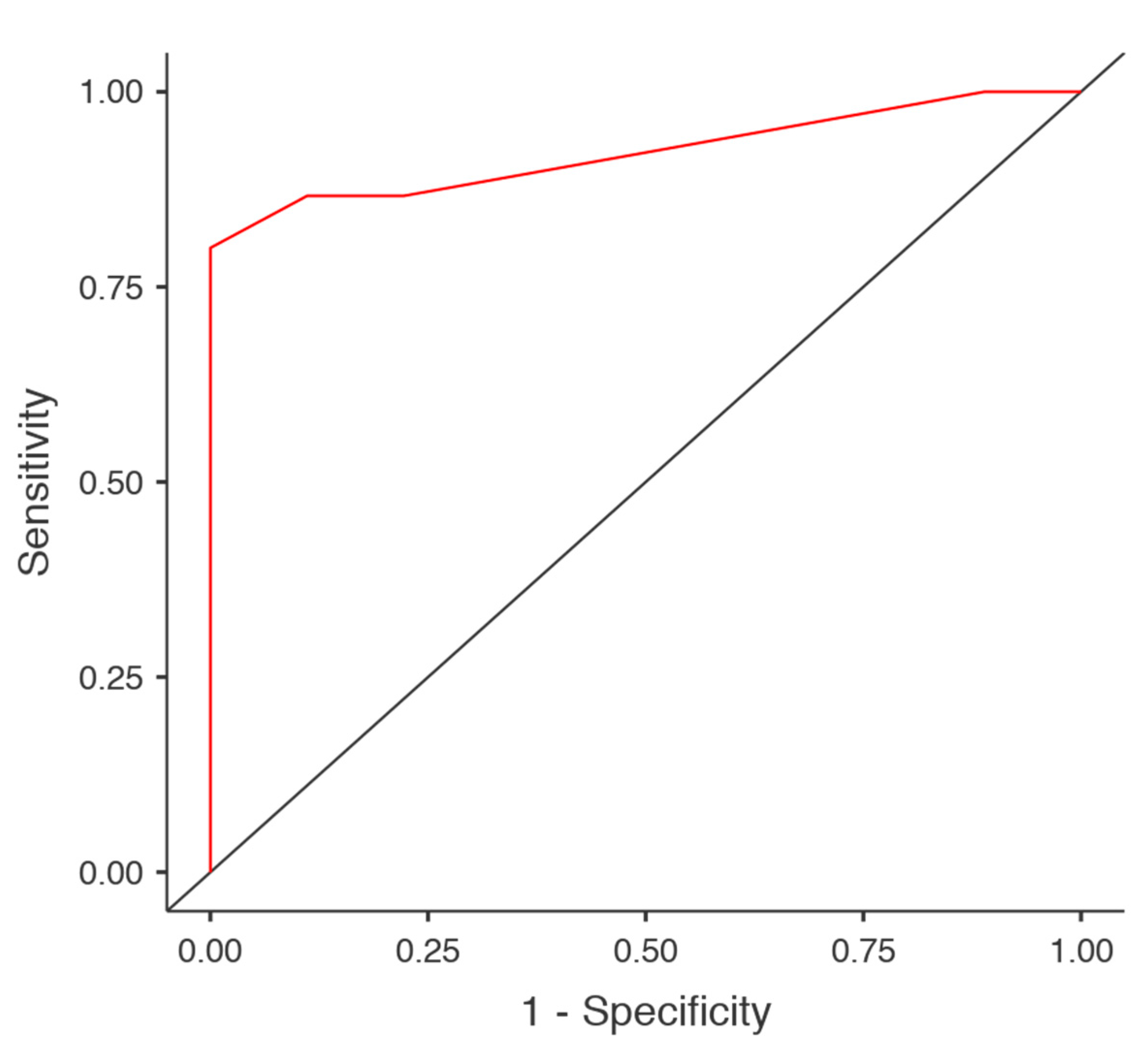
3.5. Diagnostic Accuracy
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wesseling, P.; Capper, D. WHO 2016 Classification of gliomas. Neuropathol. Appl. Neurobiol. 2018, 44, 139–150. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella, D.; Webster, B.; Hiroko, K.C.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.; Burger, P.C.; Jouvet, A.; Scheithauer, B.W.; Kleihues, P. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007, 114, 97–109. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, R.B.; Blair, H.; Ballman, K.V.; Giannini, C.; Arusell, R.M.; Law, M.; Flynn, H.; Passe, S.; Felten, S.; Brown, P.D.; et al. A t (1; 19 )(q10; p10 ) Mediates the Combined Deletions of 1p and 19q and Predicts a Better Prognosis of Patients with Oligodendroglioma. Cancer Res. 2006, 66, 9852–9861. [Google Scholar] [CrossRef] [Green Version]
- Juratli, T.A.; Kirsch, M.; Geiger, K.; Klink, B.; Leipnitz, E.; Pinzer, T.; Soucek, S.; Schrok, E.; Schackert, G.; Krex, D. The prognostic value of IDH mutations and MGMT promoter status in secondary high-grade gliomas. J. Neurooncol. 2012, 110, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Christians, A.; Adel-Horowski, A.; Banan, R.; Lehmann, U.; Bartels, S.; Behling, F.; Barrantes-Freer, A.; Stadelmann, C.; Rohde, V.; Stockhammer, F.; et al. The prognostic role of IDH mutations in homogeneously treated patients with anaplastic astrocytomas and glioblastomas. Acta Neuropathol. Commun. 2019, 7, 156. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.M.; Brat, D.J. Genomic profiling of lower—Grade gliomas uncovers cohesive disease groups: Implications for diagnosis and treatment. Chin. J. Cancer 2016, 35, 10–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Louis, D.N.; Wesseling, P.; Aldape, K.; Brat, D.J.; Capper, D.; Cree, I.A. cIMPACT-NOW update 6: New entity and diagnostic principle recommendations of the cIMPACT-Utrecht meeting on future CNS tumor classification and grading. Brain Pathol. 2020, 1–13. [Google Scholar] [CrossRef]
- Vigneswaran, K.; Neill, S.; Hadjipanayis, C.G. Beyond the World Health Organization grading of infiltrating gliomas: Advances in the molecular genetics of glioma classification. Ann. Transl. Med. 2015, 3, 95. [Google Scholar] [CrossRef]
- Bohman, L.-E.; Swanson, K.R.; Moore, J.L.; Russ, R.; Mandigo, C.; Hankinson, T.; Assanah, M.; Canoll, P.; Bruce, J. Magnetic Resonance Imaging Characteristics of Glioblastoma Multiforme: Implications for Understanding Glioma Ontogeny. Neurosurgery 2010, 67, 1319–1328. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.H.; Poisson, L.M.; Brat, D.J.; Zhou, Y.; Cooper, L.; Snuderl, M.; Thomas, C.; Franceschi, A.M.; Grif, B.; Flanders, A.E.; et al. T2—FLAIR Mismatch, an Imaging Biomarker for IDH and 1p/19q Status in Lower-grade Gliomas: A TCGA/TCIA Project. Clin. Cancer Res. 2017, 23, 6078–6086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemeyer, B.; Muniz, B.; Marchiori, E. T2-FLAIR Mismatch Sign as an Imaging Biomarker in Lower-Grade Gliomas. Eur. Neurol. 2018, 79, 317–318. [Google Scholar] [CrossRef]
- Price, S.J. Advances in imaging low-grade gliomas. Adv. Tech. Stand. Neurosurg. 2010, 35, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Broen, M.P.G.; Smits, M.; Wijnenga, M.M.J.; Dubbink, H.J.; Anten, M.H.M.E.; Schijns, O.E.M.G.; Beckervordersandforth, J.; Postma, A.A.; van den Bent, M.J. The T2-FLAIR mismatch sign as an imaging marker for non-enhancing IDH-mutant, 1p/19q-intact lower-grade glioma: A validation study. Neuro. Oncol. 2018, 20, 1393–1399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lasocki, A.; Gaillard, F.; Gorelik, A.; Gonzales, M. MRI Features Can Predict 1p/19q Status in Intracranial Gliomas. Am. J. Neuroradiol. 2018, 39, 687–692. [Google Scholar] [CrossRef]
- Jain, R.; Johnson, D.R.; Patel, S.H.; Castillo, M.; Smits, M.; van den Bent, M.J.; Chi, A.S.; Daniel, P. Real world” use of a highly reliable imaging sign: Astrocytomas. Neuro. Oncol. 2020, 22, 936–943. [Google Scholar] [CrossRef]
- Kinoshita, M.; Uchikoshi, M.; Sakai, M.; Kanemura, Y. T2 -FLAIR Mismatch Sign Is Caused by Long T 1 and T 2 of IDH- mutant, 1p19q Non-codeleted Astrocytoma. Magn. Reson. Med. Sci. 2020, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Deguchi, S.; Oishi, T.; Mitsuya, K.; Kakuda, Y.; Endo, M.; Sugino, T.; Hayashi, N. Clinicopathological analysis of T2-FLAIR mismatch sign in lower- grade gliomas. Sci. Rep. 2020, 10, 10113. [Google Scholar] [CrossRef]
- Foltyn, M.; Natalia, K.; Taborda, N.; Neuberger, U.; Brugnara, G.; Reinhardt, A.; Stichel, D.; Heiland, S.; Herold-mende, C.; Unterberg, A.; et al. T2/FLAIR-mismatch sign for noninvasive detection of IDH-mutant 1p/19q non-codeleted gliomas: Validity and pathophysiology. Neuro-Oncol. Adv. 2020, 2, 1–9. [Google Scholar] [CrossRef]
- Horbinski, C.; Kelly, L.; Nikiforov, Y.E.; Durso, M.B.; Nikiforova, M.N. Detection of IDH1 and IDH2 mutations by fluorescence melting curve analysis as a diagnostic tool for brain biopsies. J. Mol. Diagn. 2010, 12, 487–492. [Google Scholar] [CrossRef]
- Natté, R.; van Eijk, R.; Eilers, P.; Cleton-Jansen, A.-M.; Oosting, J.; Kouwenhove, M.; Kros, J.M.; van Duinen, S. Multiplex ligation-dependent probe amplification for the detection of 1p and 19q chromosomal loss in oligodendroglial tumors. Brain Pathol. 2005, 15, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Batchala, P.P.; Muttikkal, T.J.E.; Donahue, J.H.; Patrie, J.T.; Schiff, D.; Fadul, C.E.; Mrachek, E.K.; Lopes, M.-B.; Jain, R.; Patel, S.H. Neuroimaging-Based Classification Algorithm for Predicting 1p/19q-Codeletion Status in IDH -Mutant Lower Grade Gliomas. AJNR Am. J. Neuroradiol. 2019, 40, 426–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juratli, T.A.; Tummala, S.S.; Riedl, A.; Daubner, D.; Hennig, S.; Penson, T. Radiographic assessment of contrast enhancement and T2/FLAIR mismatch sign in lower grade gliomas: Correlation with molecular groups. J. Neurooncol. 2019, 141, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Yolcu, Y.U.; Goyal, A.; Kerezoudis, P.; Burns, T.C.; Parney, I.F. The T2-FLAIR–mismatch sign as an imaging biomarker for. Neurosurg. Focus 2020, 47, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Jain, R. The T2-FLAIR–mismatch sign. Neurosurg. Focus 2020, 48, 9–10. [Google Scholar] [CrossRef]
- Throckmorton, P.; Graber, J.J. T2-FLAIR mismatch in isocitrate dehydrogenase mutant astrocytomas: Variability and evolution. Neurology 2020, 95, e1582–e1589. [Google Scholar] [CrossRef]
- Corell, A.; Ferreyra Vega, S.; Hoefling, N.; Carstam, L.; Smits, A.; Olsson Bontell, T.; Björkman-Burtscher, I.M.; Carén, H.; Jakola, A.S. The clinical significance of the T2-FLAIR mismatch sign in grade II and III gliomas: A population-based study. BMC Cancer 2020, 20, 450. [Google Scholar] [CrossRef]
- Johnson, D.R.; Kaufmann, T.J.; Patel, S.H.; Chi, A.S.; Snuderl, M.; Jain, R. There is an exception to every rule—T2-FLAIR mismatch sign in gliomas. Neuroradiology 2019, 61, 225–227. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mean | SD | ||
|---|---|---|---|
| Age (years) | 53 | 12.8 | |
| Subgroup | Counts | % | |
| Gender | Female | 11 | 45.8 |
| Male | 13 | 54.2 | |
| Laterality | Left | 7 | 29.2 |
| Right | 17 | 70.8 | |
| Location | Frontal | 15 | 62.5 |
| Temporal | 5 | 20.8 | |
| Insular | 2 | 8.4 | |
| Paracentral | 1 | 4.2 | |
| Parietal | 1 | 4.2 | |
| Midline shift | No | 18 | 75 |
| Yes | 6 | 25 | |
| Homogeneous | No | 10 | 41.7 |
| Yes | 14 | 58.3 | |
| Edema | No | 10 | 41.7 |
| Minimal | 4 | 16.7 | |
| Yes | 8 | 33.3 | |
| Significant | 2 | 8.3 | |
| Contrast enhancement | No | 13 | 54.2 |
| Yes | 11 | 45.8 | |
| IDH status | Mutant type | 15 | 62.5 |
| Wild-type | 9 | 37.5 | |
| WHO classification of the CNS tumors | Diffuse astrocytoma, IDH mutant | 12 | 50 |
| Anaplastic astrocytoma, IDH wild-type | 1 | 4.2 | |
| Glioblastoma, IDH wild-type | 8 | 33.3 | |
| Oligodendroglioma, IDH mutant and 1p/19q codeleted | 2 | 8.4 | |
| Oligodendroglioma, NOS | 1 | 4.2 |
| Observer 2 | ||||
|---|---|---|---|---|
| Yes | No | Total | ||
| Observer 1 | Yes | 13 | 1 | 14 |
| No | 3 | 7 | 10 | |
| Total | 16 | 8 | 24 |
| Univariate Logistic Regression | ||||
|---|---|---|---|---|
| Reference | OR (95% CI) | p | ||
| Laterality | Right | Left | 1.37 (0.228–8.30) | 0.728 |
| Location | Insular | Frontal | 1.14 × 108 (0–Inf) | 0.998 |
| Paracentral | Frontal | 1.14 × 108 (0–Inf) | 0.999 | |
| Parietal | Frontal | 1.14 × 108 (0–Inf) | 0.999 | |
| Temporal | Frontal | 1.16 × 10−9 (0–Inf) | 0.997 | |
| Midline shift | Yes | No | 6.36 × 10−10 (0–Inf) | 0.996 |
| Homogeneous | Yes | No | 14.0 (1.86–106.27) | 0.01 |
| Edema | Minimal | No | 9.54 × 10−9 (0–Inf) | 0.996 |
| Significant | No | 1.01 × 10−17 (0–Inf) | 0.996 | |
| Yes | No | 1.06 × 10−9 (0–Inf) | 0.995 | |
| CE | Yes | No | 0.0313 (0.03–0.356) | 0.005 |
| T2–FLAIR mismatch sign | Yes | No | 52.0 (4.03–670.6) | 0.002 |
| Multivariate Model 1 | Multivariate Model 2 | Multivariate Model 3 | Multivariate Model 4 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Reference | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | ||
| Homogeneous | Yes | No | 5.48 × 10−8 (0–Inf) | 0.997 | 2.802 (0.177–44.29) | 0.464 | - | - | 0.07 × 10−7 (0–Inf) | 0.997 |
| CE | Yes | No | 1.96 × 10−9 (0–Inf) | 0.996 | - | - | 0.161 (0.007–3.37) | 0.239 | 1.85 × 10−8 (0–Inf) | 0.996 |
| T2–FLAIR mismatch sign | Yes | No | - | - | 29.642 (1.73–509.15) | 0.019 | 17.585 (0.919–336.55) | 0.057 | 16.1 (0.824–315) | 0.067 |
| 95% Confidence Interval | ||||||
|---|---|---|---|---|---|---|
| Contrast Enhancement | Homogeneous | T2–FLAIR Mismatch Sign | Probability | SE | Lower | Upper |
| Univariate Model 1 | ||||||
| No | 0.3 | 0.1449 | 0.0998 | 0.624 | ||
| Yes | 0.857 | 0.0935 | 0.5732 | 0.964 | ||
| Univariate Model 2 | ||||||
| No | 0.2 | 0.1265 | 0.0504 | 0.541 | ||
| Yes | 0.929 | 0.0688 | 0.6297 | 0.99 | ||
| Univariate Model 3 | ||||||
| No | 0.923 | 0.0739 | 0.6094 | 0.989 | ||
| Yes | 0.273 | 0.1343 | 0.0905 | 0.586 | ||
| Multivariate Model 1 | ||||||
| No | No | 0.545 | 0.3795 | 0.0562 | 0.96 | |
| Yes | 0.955 | 0.0537 | 0.649 | 0.996 | ||
| Yes | No | 0.162 | 0.1174 | 0.0341 | 0.513 | |
| Yes | 0.772 | 0.2489 | 0.1748 | 0.982 | ||
| Multivariate Model 2 | ||||||
| No | No | 0.162 | 0.1231 | 0.0317 | 0.533 | |
| Yes | 0.852 | 0.1846 | 0.2469 | 0.99 | ||
| Yes | No | 0.352 | 0.2913 | 0.0424 | 0.869 | |
| Yes | 0.941 | 0.0615 | 0.6434 | 0.993 | ||
| Multivariate Model 3 | ||||||
| No | No | 1 | 1.81 × 10−5 | 2.22 × 10−16 | 1 | |
| Yes | No | 0.3 | 0.1449 | 0.0998 | 0.624 | |
| No | Yes | 0.923 | 0.0739 | 0.6094 | 0.989 | |
| Yes | Yes | 2.35 × 10−8 | 9.30 × 10−5 | 2.22 × 10−16 | 1 | |
| Multivariate Model 4 | ||||||
| No | No | No | 1 | 3.34 × 10−4 | 2.22 × 10−16 | 1 |
| Yes | 1 | 2.07 × 10−5 | 2.22 × 10−16 | 1 | ||
| Yes | No | 0.559 | 0.37852 | 0.0589 | 0.963 | |
| Yes | 0.953 | 0.05465 | 0.6475 | 0.996 | ||
| Yes | No | No | 0.18 | 0.12978 | 0.0377 | 0.552 |
| Yes | 0.78 | 0.24513 | 0.1775 | 0.983 | ||
| Yes | No | 2.35 × 10−8 | 9.30 × 10−5 | 2.22 × 10−16 | 1 | |
| Yes | 3.79 × 10−7 | 0.0015 | 2.22 × 10−16 | 1 | ||
| Parameters | Accuracy | Specificity (95% CI) | Sensitivity (95% CI) | AUC | |
|---|---|---|---|---|---|
| Univariate | T2–FLAIR mismatch sign | 0.875 | 0.867 (0.584–0.976) | 0.889 (0.507–0.994) | 0.878 |
| CE | 0.833 | 0.800 (0.513–0.947) | 0.889 (0.507–0.994) | 0.844 | |
| Homogeneity | 0.792 | 0.800 (0.513–0.947) | 0.778 (0.402–0.960) | 0.789 | |
| Multivariate | CE, Homogeneity | 0.833 | 0.800 (0.513–0.947) | 0.889 (0.507–0.994) | 0.856 |
| T2–FLAIR mismatch sign, CE | 0.833 | 0.867 (0.584–0.976) | 0.778 (0.402–0.960) | 0.915 | |
| T2–FLAIR mismatch sign, Homogeneity | 0.875 | 0.867 (0.584–0.976) | 0.889 (0.507–0.994) | 0.907 | |
| T2–FLAIR mismatch sign, CE, Homogeneity | 0.833 | 0.867 (0.584–0.976) | 0.778 (0.402–0.960) | 0.922 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapsalaki, E.Z.; Brotis, A.G.; Tsikrika, A.; Tzerefos, C.; Paschalis, T.; Dardiotis, E.; Fountas, K.N. The Role of the T2–FLAIR Mismatch Sign as an Imaging Marker of IDH Status in a Mixed Population of Low- and High-Grade Gliomas. Brain Sci. 2020, 10, 874. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110874
Kapsalaki EZ, Brotis AG, Tsikrika A, Tzerefos C, Paschalis T, Dardiotis E, Fountas KN. The Role of the T2–FLAIR Mismatch Sign as an Imaging Marker of IDH Status in a Mixed Population of Low- and High-Grade Gliomas. Brain Sciences. 2020; 10(11):874. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110874
Chicago/Turabian StyleKapsalaki, Eftychia Z., Alexandros G. Brotis, Alexandra Tsikrika, Christos Tzerefos, Thanos Paschalis, Efthymios Dardiotis, and Konstantinos N. Fountas. 2020. "The Role of the T2–FLAIR Mismatch Sign as an Imaging Marker of IDH Status in a Mixed Population of Low- and High-Grade Gliomas" Brain Sciences 10, no. 11: 874. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110874