Effortful Control and Prefrontal Cortex Functioning in Children with Autism Spectrum Disorder: An fNIRS Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Short Form of the Early Adolescent Temperament Questionnaire—Revised (EATQ-R)
2.3.2. d2 Test of Attention
2.3.3. Cambridge Neuropsychological Test Automated Battery (CANTAB)
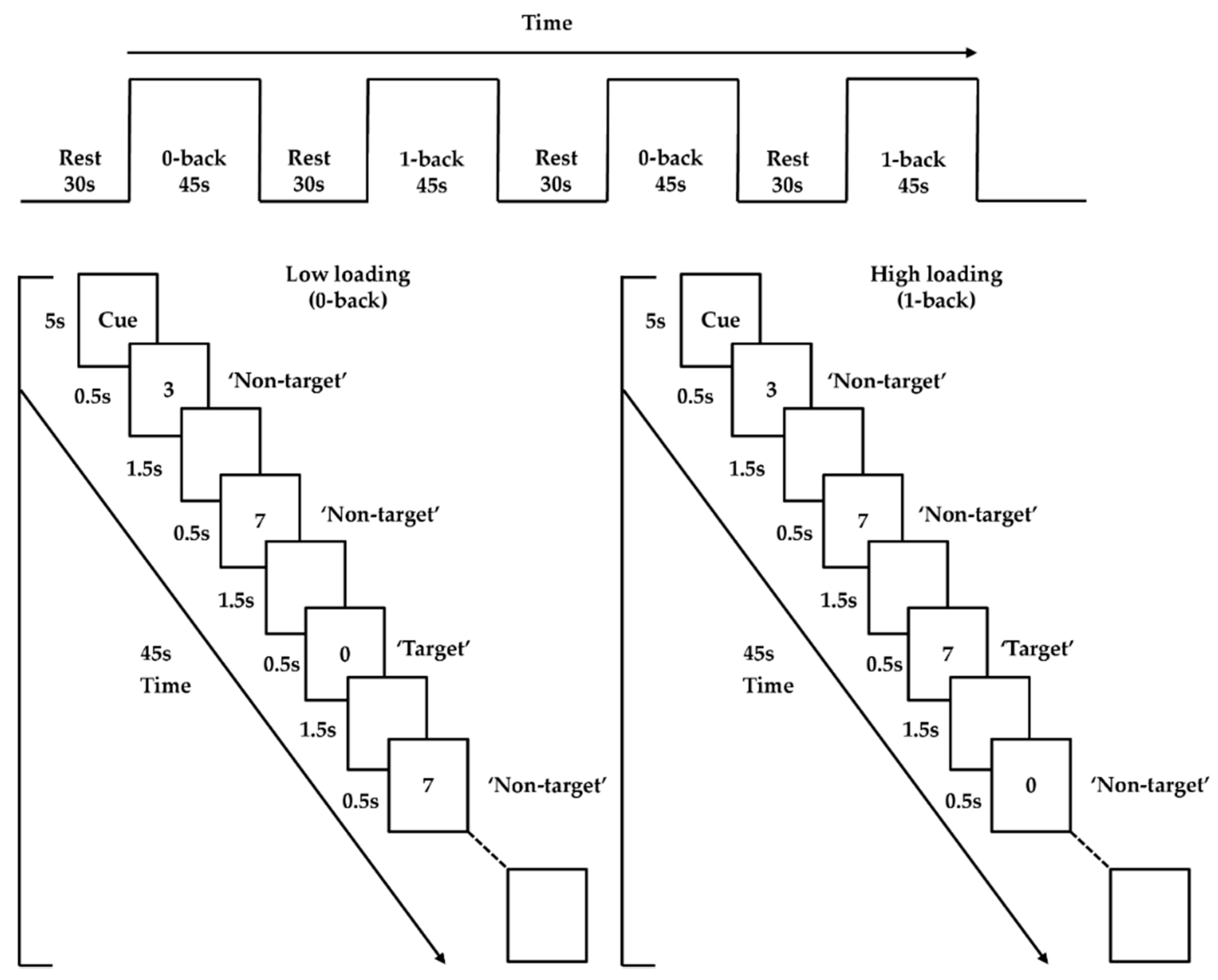
2.3.4. n-back Task
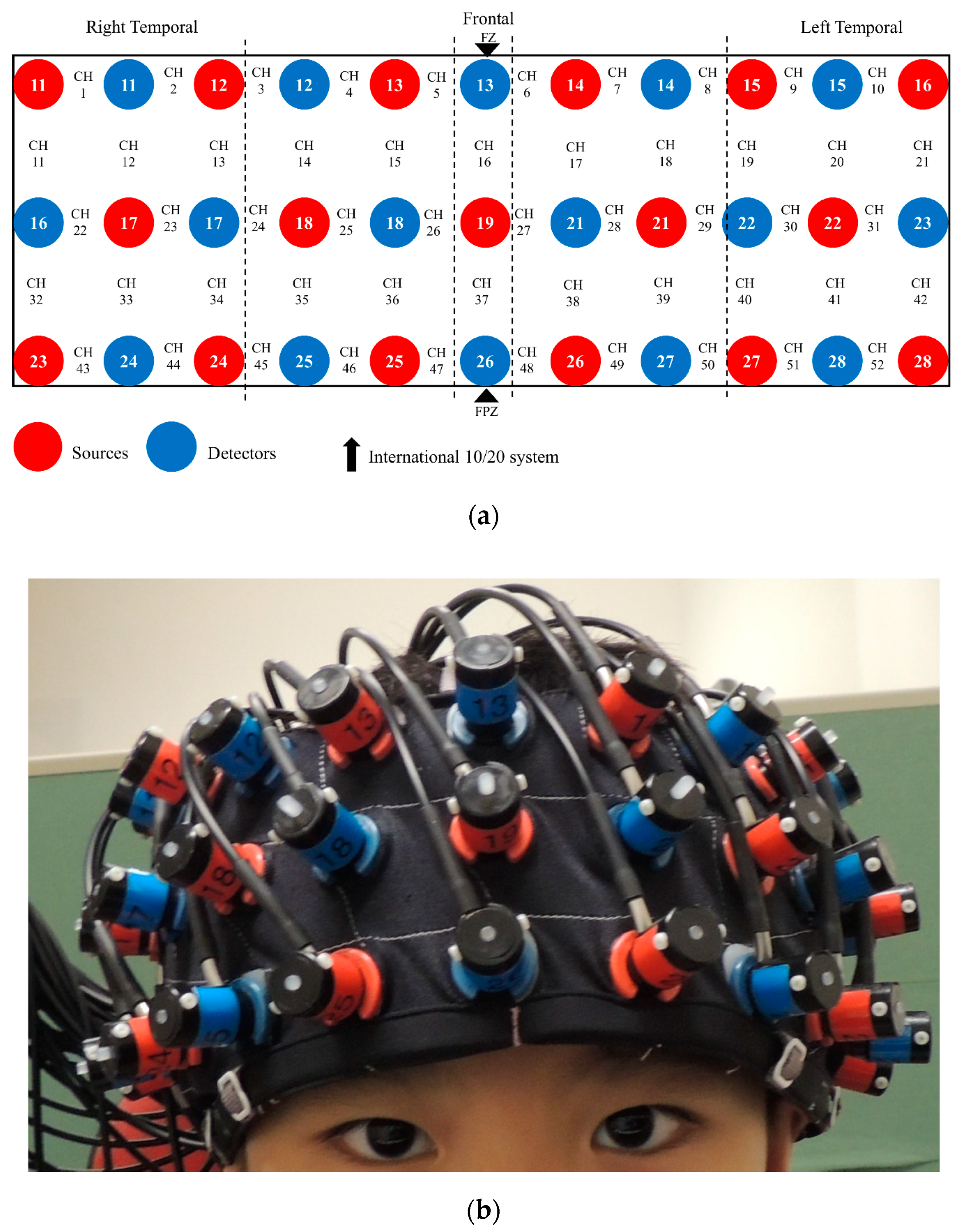
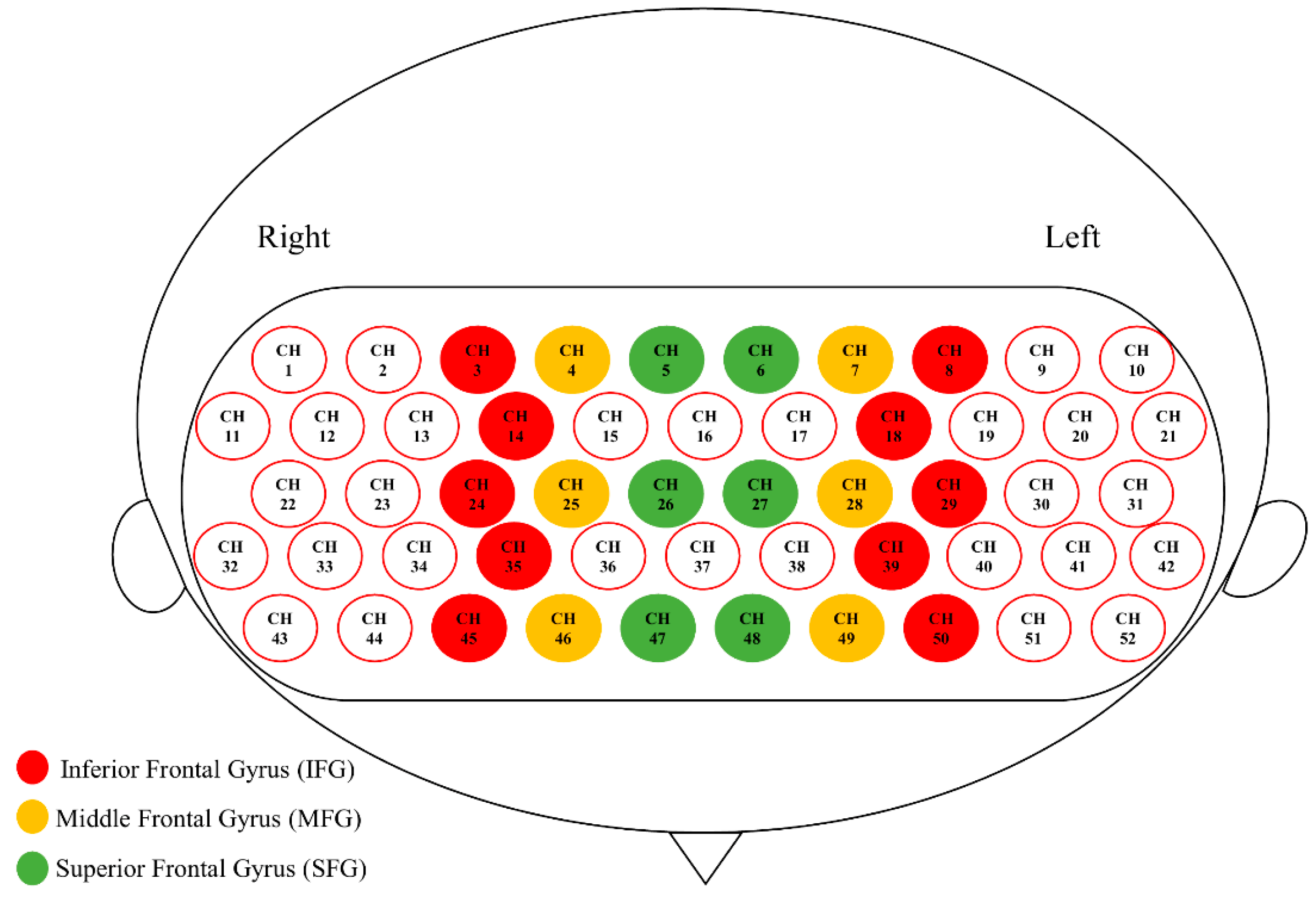
2.4. fNIRS Recording
2.5. Data Analysis
2.5.1. Questionnaires and Neuropsychological Measures
2.5.2. Preprocessing for fNIRS Data
2.5.3. fNIRS Data Analysis
2.5.4. Brain–Behavior Relationship
3. Results
3.1. Demographic, Intellectual, and Clinical Characteristics
3.2. EC, Executive, and Socioemotional Measures
3.3. PFC Activation during the N-Back Task
3.4. PFC Connectivity during the n-Back Task
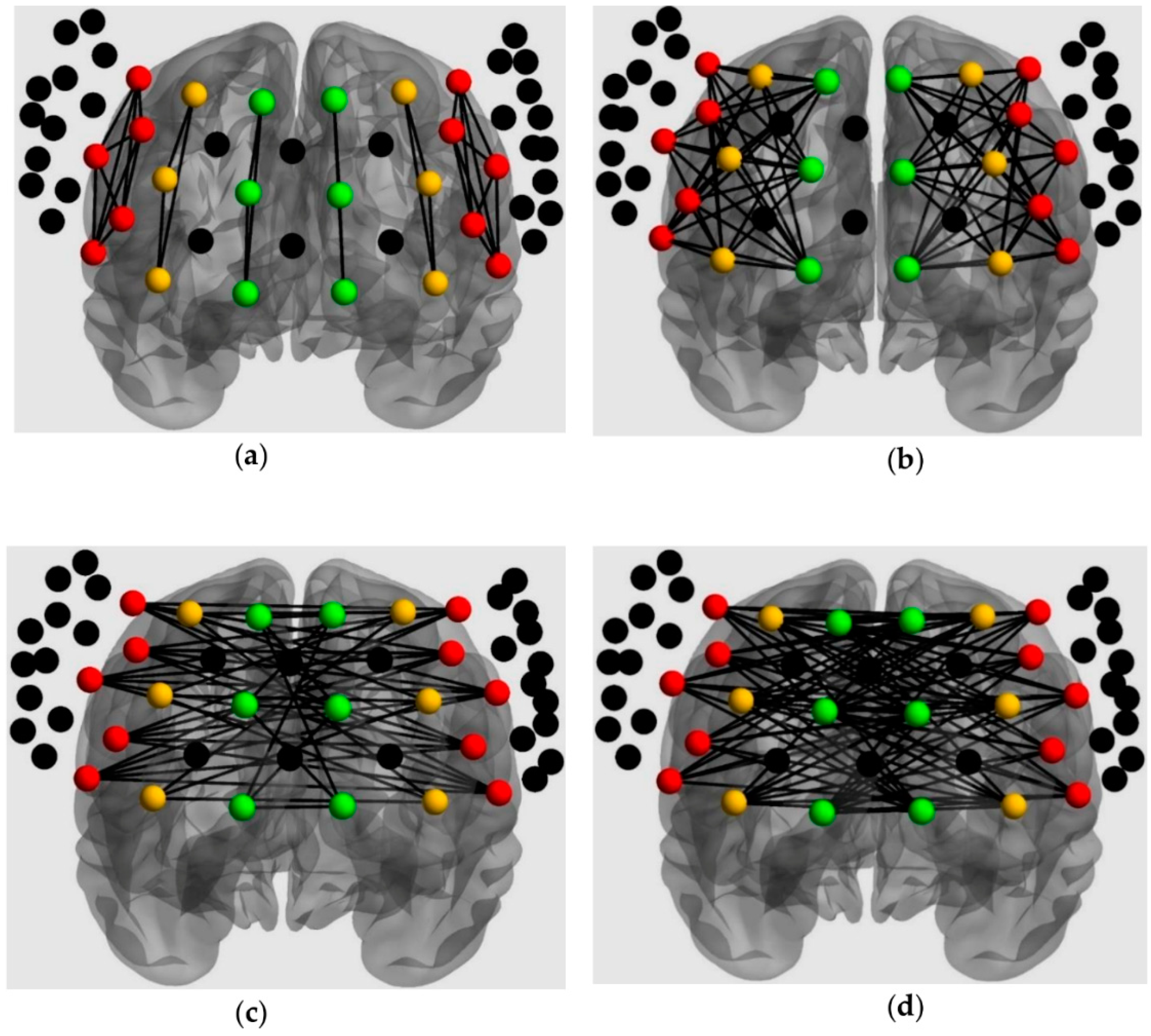
3.4.1. Intrahemispheric Connectivity
3.4.2. Interhemispheric Connectivity
3.5. Individual Differences of EC in the ASD Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. The Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Eisenberg, N.; Smith, L.C.; Sadovsky, A.; Spinarad, L.T. Effortful control: Relations with emotion regulation, adjustment, and socialization in childhood. In Handbook of Self-Regulation: Research, Theory, and Applications; Baumeister, R.F., Kathleen, D.V., Eds.; The Guilford Press: New York, NY, USA, 2004; pp. 259–282. [Google Scholar]
- Konstantareas, M.M.; Stewart, K. Affect Regulation and Temperament in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2006, 36, 143–154. [Google Scholar] [CrossRef]
- Schwartz, C.B.; Henderson, H.A.; Inge, A.P.; Zahka, N.E.; Coman, D.C.; Kojkowski, N.M.; Hileman, C.M.; Mundy, P.C. Temperament as a Predictor of Symptomotology and Adaptive Functioning in Adolescents with High-Functioning Autism. J. Autism Dev. Disord. 2009, 39, 842–855. [Google Scholar] [CrossRef] [Green Version]
- Rothbart, M.; Bates, J.E. Temperament. In Handbook of Child Psychology: Social, Emotional, and Personality Development, 6th ed.; Eisenberg, W.D., Lerner, R.M., Eds.; John Wiley & Sons, Inc: New York, NY, USA, 2006; Volume 3, pp. 99–166. [Google Scholar]
- Goldstein, M.A.; Brendel, G.; Tuescher, O.; Pan, H.; Epstein, J.; Beutel, M.; Yang, Y.; Thomas, K.; Levy, K.; Silverman, M.E.; et al. Neural substrates of the interaction of emotional stimulus processing and motor inhibitory control: An emotional linguistic go/no-go fMRI study. NeuroImage 2007, 36, 1026–1040. [Google Scholar] [CrossRef]
- Claes, L.; Vertommen, S.; Smits, D.; Bijttebier, P. Emotional reactivity and self-regulation in relation to personality disorders. Pers. Individ. Differ. 2009, 47, 948–953. [Google Scholar] [CrossRef]
- Eisenberg, N.; Spinrad, T.L.; Eggum, N.D. Emotion-Related Self-Regulation and Its Relation to Children’s Maladjustment. Annu. Rev. Clin. Psychol. 2010, 6, 495–525. [Google Scholar] [CrossRef] [Green Version]
- Lengua, L.J.; Bush, N.R.; Long, A.C.; Kovacs, E.A.; Trancik, A.M. Effortful control as a moderator of the relation between contextual risk factors and growth in adjustment problems. Dev. Psychopathol. 2008, 20, 509–528. [Google Scholar] [CrossRef] [Green Version]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Q.; Chen, S.H.; Main, A. Commonalities and Differences in the Research on Children’s Effortful Control and Executive Function: A Call for an Integrated Model of Self-Regulation. Child Dev. Perspect. 2011, 6, 112–121. [Google Scholar] [CrossRef]
- Miller, E.K.; Cohen, J.D. An Integrative Theory of Prefrontal Cortex Function. Annu. Rev. Neurosci. 2001, 24, 167–202. [Google Scholar] [CrossRef] [Green Version]
- Kelley, W.M.; Wagner, D.D.; Heatherton, T.F. In Search of a Human Self-Regulation System. Annu. Rev. Neurosci. 2015, 38, 389–411. [Google Scholar] [CrossRef] [Green Version]
- Quiñones-Camacho, L.E.; Fishburn, F.A.; Camacho, M.C.; Wakschlag, L.S.; Perlman, S.B. Cognitive flexibility-related prefrontal activation in preschoolers: A biological approach to temperamental effortful control. Dev. Cogn. Neurosci. 2019, 38, 100651. [Google Scholar] [CrossRef] [PubMed]
- Seeley, W.W.; Menon, V.; Schatzberg, A.F.; Keller, J.; Glover, G.H.; Kenna, H.; Reiss, A.L.; Greicius, M.D. Dissociable Intrinsic Connectivity Networks for Salience Processing and Executive Control. J. Neurosci. 2007, 27, 2349–2356. [Google Scholar] [CrossRef] [PubMed]
- Dosenbach, N.U.; Fair, D.A.; Miezin, F.M.; Cohen, A.L.; Wenger, K.K.; Dosenbach, R.A.T.; Fox, M.D.; Snyder, A.Z.; Vincent, J.L.; Raichle, M.E.; et al. Distinct brain networks for adaptive and stable task control in humans. Proc. Natl. Acad. Sci. USA 2007, 104, 11073–11078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fekete, T.; Beacher, F.D.; Cha, J.; Rubin, D.; Mujica-Parodi, L.R. Small-world network properties in prefrontal cortex correlate with predictors of psychopathology risk in young children: A NIRS study. NeuroImage 2014, 85, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Courchesne, E.; Pierce, K. Why the frontal cortex in autism might be talking only to itself: Local over-connectivity but long-distance disconnection. Curr. Opin. Neurobiol. 2005, 15, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Ecker, C.; Bookheimer, S.Y.; Murphy, D.G.M. Neuroimaging in autism spectrum disorder: Brain structure and function across the lifespan. Lancet Neurol. 2015, 14, 1121–1134. [Google Scholar] [CrossRef] [Green Version]
- Philip, R.C.; Dauvermann, M.R.; Whalley, H.C.; Baynham, K.; Lawrie, S.M.; Stanfield, A.C. A systematic review and meta-analysis of the fMRI investigation of autism spectrum disorders. Neurosci. Biobehav. Rev. 2012, 36, 901–942. [Google Scholar] [CrossRef]
- Zhang, Z.; Peng, P.; Zhang, D. Executive Function in High-Functioning Autism Spectrum Disorder: A Meta-analysis of fMRI Studies. J. Autism Dev. Disord. 2020, 1–17. [Google Scholar] [CrossRef]
- Kana, R.K.; Keller, T.A.; Minshew, N.J.; Just, M.A. Inhibitory Control in High-Functioning Autism: Decreased Activation and Underconnectivity in Inhibition Networks. Biol. Psychiatry 2007, 62, 198–206. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, J.; Johnson, K.A.; Kehoe, E.; Bokde, A.L.; Garavan, H.; Gallagher, L.; McGrath, J. Disrupted Functional Connectivity in Dorsal and Ventral Attention Networks During Attention Orienting in Autism Spectrum Disorders. Autism Res. 2014, 8, 136–152. [Google Scholar] [CrossRef]
- Solomon, M.; Ozonoff, S.J.; Ursu, S.; Ravizza, S.; Cummings, N.; Ly, S.; Carter, C.S. The neural substrates of cognitive control deficits in autism spectrum disorders. Neuropsychologia 2009, 47, 2515–2526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Reilly, C.; Lewis, J.D.; Elsabbagh, M. Is functional brain connectivity atypical in autism? A systematic review of EEG and MEG studies. PLoS ONE 2017, 12, e0175870. [Google Scholar] [CrossRef] [PubMed]
- Owen, A.M.; McMillan, K.M.; Laird, A.R.; Bullmore, E. N-back working memory paradigm: A meta-analysis of normative functional neuroimaging studies. Hum. Brain Mapp. 2005, 25, 46–59. [Google Scholar] [CrossRef] [Green Version]
- Yeung, M.K.; Sze, S.L.; Woo, J.; Kwok, T.C.Y.; Shum, D.H.K.; Yu, R.; Chan, A.S. Reduced Frontal Activations at High Working Memory Load in Mild Cognitive Impairment: Near-Infrared Spectroscopy. Dement. Geriatr. Cogn. Disord. 2016, 42, 278–296. [Google Scholar] [CrossRef]
- Tsuchida, A.; Fellows, L.K. Lesion Evidence That Two Distinct Regions within Prefrontal Cortex are Critical for n-Back Performance in Humans. J. Cogn. Neurosci. 2009, 21, 2263–2275. [Google Scholar] [CrossRef]
- Gajewski, P.D.; Hanisch, E.; Falkenstein, M.; Thönes, S.; Wascher, E. What Does the n-Back Task Measure as We Get Older? Relations between Working-Memory Measures and Other Cognitive Functions Across the Lifespan. Front. Psychol. 2018, 9, 2208. [Google Scholar] [CrossRef] [Green Version]
- Di Martino, A.; Kelly, C.; Grzadzinski, R.; Zuo, X.-N.; Mennes, M.; Mairena, M.A.; Lord, C.; Castellanos, F.X.; Milham, M.P. Aberrant Striatal Functional Connectivity in Children with Autism. Biol. Psychiatry 2011, 69, 847–856. [Google Scholar] [CrossRef] [Green Version]
- Barendse, E.M.; Schreuder, L.J.; Thoonen, G.; Hendriks, M.P.H.; Kessels, R.P.C.; Backes, W.H.; Aldenkamp, A.P.; Jansen, J.F. Working memory network alterations in high-functioning adolescents with an autism spectrum disorder. Psychiatry Clin. Neurosci. 2017, 72, 73–83. [Google Scholar] [CrossRef]
- Lever, A.G.; Werkle-Bergner, M.; Brandmaier, A.M.; Ridderinkhof, K.R.; Geurts, H.M. Atypical working memory decline across the adult lifespan in autism spectrum disorder? J. Abnorm. Psychol. 2015, 124, 1014–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, D.L.; Goldstein, G.; Carpenter, P.A.; Minshew, N.J. Verbal and Spatial Working Memory in Autism. J. Autism Dev. Disord. 2005, 35, 747–756. [Google Scholar] [CrossRef]
- Koshino, H.; Carpenter, P.A.; Minshew, N.J.; Cherkassky, V.L.; Keller, T.A.; Just, M.A. Functional connectivity in an fMRI working memory task in high-functioning autism. NeuroImage 2005, 24, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Yeung, M.K.; Lee, T.L.; Chan, A.S. Right-lateralized frontal activation underlies successful updating of verbal working memory in adolescents with high-functioning autism spectrum disorder. Biol. Psychol. 2019, 148, 107743. [Google Scholar] [CrossRef] [PubMed]
- Boas, D.A.; Elwell, C.E.; Ferrari, M.; Taga, G. Twenty years of functional near-infrared spectroscopy: Introduction for the special issue. NeuroImage 2014, 85, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Quaresima, V. A brief review on the history of human functional near-infrared spectroscopy (fNIRS) development and fields of application. NeuroImage 2012, 63, 921–935. [Google Scholar] [CrossRef]
- Cui, X.; Bray, S.; Bryant, D.M.; Glover, G.H.; Reiss, A.L. A quantitative comparison of NIRS and fMRI across multiple cognitive tasks. NeuroImage 2011, 54, 2808–2821. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Roeyers, H. Exploring brain functions in autism spectrum disorder: A systematic review on functional near-infrared spectroscopy (fNIRS) studies. Int. J. Psychophysiol. 2019, 137, 41–53. [Google Scholar] [CrossRef] [Green Version]
- Muris, P.; Meesters, C. Reactive and Regulative Temperament in Youths: Psychometric Evaluation of the Early Adolescent Temperament Questionnaire-Revised. J. Psychopathol. Behav. Assess. 2008, 31, 7–19. [Google Scholar] [CrossRef] [Green Version]
- Bates, M.E.; Lemay, E.P. The d2 Test of Attention: Construct validity and extensions in scoring techniques. J. Int. Neuropsychol. Soc. 2004, 10, 392–400. [Google Scholar] [CrossRef]
- José, H.L.; Elena, C.; María, P.F. Convergent validity of measures of attention and impulsivity from the trees simple visual discrimination test (divisa-uam). An. Psicol. Ann. Psychol. 2014, 31, 74–83. [Google Scholar]
- Syväoja, H.J.; Tammelin, T.H.; Ahonen, T.; Räsänen, P.; Tolvanen, A.; Kankaanpää, A.; Kantomaa, M.T. Internal consistency and stability of the CANTAB neuropsychological test battery in children. Psychol. Assess. 2015, 27, 698–709. [Google Scholar] [CrossRef] [Green Version]
- Wild, K.; Musser, E.D. The cambridge neuropsychological test automated battery in the assessment of executive functioning. In Handbook of Executive Functioning; Goldstein, S., Naglieri, J.A., Eds.; Springer: New York, NY, USA, 2014; pp. 171–190. [Google Scholar]
- Ehlis, A.-C.; Bähne, C.G.; Jacob, C.; Herrmann, M.J.; Fallgatter, A.J. Reduced lateral prefrontal activation in adult patients with attention-deficit/hyperactivity disorder (ADHD) during a working memory task: A functional near-infrared spectroscopy (fNIRS) study. J. Psychiatr. Res. 2008, 42, 1060–1067. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Okamoto, M.; Dan, H.; Jurcak, V.; Dan, I. Spatial registration of multichannel multi-subject fNIRS data to MNI space without MRI. NeuroImage 2005, 27, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, C.E.; Richards, J.E.; Almli, C.R. Age-specific MRI templates for pediatric neuroimaging. Dev. Neuropsychol. 2012, 37, 379–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, W.; Richards, J.E.; Lei, D.; Zhu, H.; Lee, K.; Gong, Q. The construction of MRI brain/head templates for Chinese children from 7 to 16 years of age. Dev. Cogn. Neurosci. 2015, 15, 94–105. [Google Scholar] [CrossRef] [Green Version]
- Santosa, H.; Zhai, X.; Fishburn, F.; Huppert, T. The NIRS Brain AnalyzIR Toolbox. Algorithms 2018, 11, 73. [Google Scholar] [CrossRef] [Green Version]
- Delpy, D.T.; Cope, M.; Van Der Zee, P.; Arridge, S.; Wray, S.; Wyatt, J. Estimation of optical pathlength through tissue from direct time of flight measurement. Phys. Med. Biol. 1988, 33, 1433–1442. [Google Scholar] [CrossRef] [Green Version]
- Barker, J.W.; Aarabi, A.; Huppert, T.J. Autoregressive model based algorithm for correcting motion and serially correlated errors in fNIRS. Biomed. Opt. Express 2013, 4, 1366–1379. [Google Scholar] [CrossRef] [Green Version]
- Ye, J.C.; Tak, S.; Jang, K.E.; Jung, J.; Jang, J. NIRS-SPM: Statistical parametric mapping for near-infrared spectroscopy. NeuroImage 2009, 44, 428–447. [Google Scholar] [CrossRef]
- Xia, M.; Wang, J.; He, Y. BrainNet Viewer: A Network Visualization Tool for Human Brain Connectomics. PLoS ONE 2013, 8, e68910. [Google Scholar] [CrossRef] [Green Version]
- Zhu, H.; Xu, J.; Li, J.; Peng, H.; Cai, T.; Li, X.; Wu, S.; Cao, W.; He, S. Decreased functional connectivity and disrupted neural network in the prefrontal cortex of affective disorders: A resting-state fNIRS study. J. Affect. Disord. 2017, 221, 132–144. [Google Scholar] [CrossRef]
- Townsend, J.; Ashby, F. Methods of modeling capacity in simple processing systems. Cog. Theory 1978, 3, 199–239. [Google Scholar]
- Townsend, J.; Ashby, F. The Stochastic Modeling of Elementary Psychological Processes (Part 2), 1st ed.; Cambridge University Press: New York, NY, USA, 1983. [Google Scholar]
- Samyn, V.; Eroeyers, H.; Bijttebier, P. Effortful control in typically developing boys and in boys with ADHD or autism spectrum disorder. Res. Dev. Disabil. 2011, 32, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Adamek, L.; Nichols, S.; Tetenbaum, S.P.; Bregman, J.; Ponzio, C.A.; Carr, E.G. Individual Temperament and Problem Behavior in Children with Autism Spectrum Disorders. Focus Autism Other Dev. Disabil. 2011, 26, 173–183. [Google Scholar] [CrossRef]
- Geschwind, D.H.; Levitt, P. Autism spectrum disorders: Developmental disconnection syndromes. Curr. Opin. Neurobiol. 2007, 17, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Zeestraten, E.A.; Gudbrandsen, M.; Daly, E.; De Schotten, M.T.; Catani, M.; Acqua, F.D.; Lai, M.-C.; Ruigrok, A.N.V.; Lombardo, M.V.; Chakrabarti, B.; et al. Sex differences in frontal lobe connectivity in adults with autism spectrum conditions. Transl. Psychiatry 2017, 7, e1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Just, M.A.; Keller, T.A.; Malave, V.L.; Kana, R.K.; Varma, S. Autism as a neural systems disorder: A theory of frontal-posterior underconnectivity. Neurosci. Biobehav. Rev. 2012, 36, 1292–1313. [Google Scholar] [CrossRef] [Green Version]
- Frith, C. Is autism a disconnection disorder? Lancet Neurol. 2004, 3, 577. [Google Scholar] [CrossRef]
- Minshew, N.J.; Goldstein, G.; Siegel, D.J. Neuropsychologic functioning in autism: Profile of a complex information processing disorder. J. Int. Neuropsychol. Soc. 1997, 3, 303–316. [Google Scholar] [CrossRef]
- Stuss, D.T.; Alexander, M.P. Is there a dysexecutive syndrome? Philos. Trans. R. Soc. B Biol. Sci. 2007, 362, 901–915. [Google Scholar] [CrossRef] [Green Version]
- Faja, S.; Dawson, G. Reduced delay of gratification and effortful control among young children with autism spectrum disorders. Autism 2013, 19, 91–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedge, C.; Powell, G.; Sumner, P. The reliability paradox: Why robust cognitive tasks do not produce reliable individual differences. Behav. Res. Methods 2017, 50, 1166–1186. [Google Scholar] [CrossRef] [PubMed]
- Dang, J.; King, K.M.; Inzlicht, M. Why Are Self-Report and Behavioral Measures Weakly Correlated? Trends Cogn. Sci. 2020, 24, 267–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brickenkamp, R.; Rump, G. Die Stabilität des Aufmerksamkeits-Belastungs—Tests (Test d2) über längere Zeitabschnitte. [Long-term, test-retest stability of the d2 Test of Attention.]. Diagnostica 1966, 12, 17–24. [Google Scholar]
- Zhang, J.; Shen, L.; Gao, N.; Yan, C. The Revision and Application of the Revision of the Early Adolescent Temperament Questionnaire. Chin. Ment. Heal. J. 2008, 22, 439–443. [Google Scholar]
- Bölte, S.; Poustka, F.; Constantino, J.N. Assessing autistic traits: Cross-cultural validation of the social responsiveness scale (SRS). Autism Res. 2008, 1, 354–363. [Google Scholar] [CrossRef]
- Etkin, A.; Egner, T.; Kalisch, R. Emotional processing in anterior cingulate and medial prefrontal cortex. Trends Cogn. Sci. 2011, 15, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Phelps, E.A.; LeDoux, J.E. Contributions of the Amygdala to Emotion Processing: From Animal Models to Human Behavior. Neuron 2005, 48, 175–187. [Google Scholar] [CrossRef] [Green Version]
- Baron-Cohen, S.; Ring, H.; Bullmore, E.; Wheelwright, S.; Ashwin, C.; Williams, S. The amygdala theory of autism. Neurosci. Biobehav. Rev. 2000, 24, 355–364. [Google Scholar] [CrossRef]
- Szmalec, A.; Verbruggen, F.; Vandierendonck, A.; Kemps, E. Control of interference during working memory updating. J. Exp. Psychol. Hum. Percept. Perform. 2011, 37, 137–151. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TD (n = 19) | ASD (n = 20) | t/χ2/r | p | |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| Age (years) | 10.28 (0.67) | 10.16 (1.04) | 0.42 | 0.68 |
| IQ | 108.79 (9.47) | 101.65 (16.96) | 1.63 | 0.11 |
| Gender (Males:Females) # | 12:07 | 20:00 | 6.65 | 0.010 ** |
| ADI-R Social Interaction ## | - | 14.20 (7.41) | 0.052 | 0.83 |
| ADI-R Communication ## | - | 10.75 (5.70) | −0.32 | 0.18 |
| ADI-R Restricted and Stereotyped Behavior ## | - | 5.35 (2.70) | −0.30 | 0.21 |
| Variables | TD (n = 19) | ASD (n = 20) | t | p | d |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | ||||
| EATQ-R # | |||||
| Total | 3.18 (0.50) | 2.67 (0.61) | 2.83 | 0.007 ** | 0.91 |
| Attention | 3.16 (0.68) | 2.54 (0.67) | 2.79 | 0.008 ** | 0.92 |
| Inhibitory control | 3.42 (0.48) | 2.79 (0.76) | 3.05 | 0.005 ** | 0.99 |
| Activation control | 2.97 (0.57) | 2.68 (0.69) | 1.39 | 0.17 | 0.46 |
| D2 Test of Attention | |||||
| Concentration performance index | 141.2 (20.2) | 121.5 (25.0) | 2.69 | 0.011 * | 0.86 |
| CANTAB Reaction Time Task # | |||||
| Mean reaction time (ms) | 421.8 (51.2) | 468.0 (117.3) | 2.67 | 0.011 * | 0.51 |
| CANTAB Multitasking Test # | |||||
| Switch block error | 7.28 (4.39) | 12.45 (7.86) | 2.46 | 0.019 * | 0.81 |
| CANTAB Emotion Recognition Task # | |||||
| Total hit rate | 23.72 (3.89) | 19.00 (4.33) | 3.48 | 0.001 ** | 1.15 |
| SRS-2 # | |||||
| Total T-score | 40.3 (17.4) | 87.4 (26.8) | 6.22 | <0.001 *** | 2.09 |
| Variables | TD (n = 19) | ASD (n = 20) | Z | p | r |
|---|---|---|---|---|---|
| Median (95% CI) | Median (95% CI) | ||||
| Mean reaction time (ms) | |||||
| Low load | 445.1 (423.8–538.7) | 502.1 (517.1–687.1) | 3.15 | 0.001 ** | 0.50 |
| High load | 536.0 (505.0–644.4) | 636.3 (603.9–811.6) | 1.80 | 0.074 | 0.29 |
| Accuracy | |||||
| Low load | 0.97 (0.93–0.97) | 0.95 (0.92–0.97) | 0.27 | 0.79 | 0.043 |
| High load | 0.94 (0.87–0.95) | 0.89 (0.83–0.93) | 0.64 | 0.53 | 0.10 |
| Inverse efficiency score | |||||
| Low load | 496.1 (494.7–518.4) | 633.8 (621.2–653.9) | 5.36 | <0.001 *** | 0.86 |
| High load | 611.3 (608.8–664.8) | 794.8 (761.2–875.0) | 4.72 | <0.001 *** | 0.76 |
| Main/Interaction Effects | Mean (SE) | F(1,35) | p | ηp2 |
|---|---|---|---|---|
| Connectivity pattern (within and between ROI) | Within: 0.18 (0.011) | 48.28 | <0.001 *** | 0.58 |
| Between: 0.22 (0.012) | ||||
| Loading (low and high) | Low: 0.21 (0.013) | 4.50 | 0.041 * | 0.11 |
| High: 0.19 (0.010) | ||||
| Frontal side (left and right) | Right: 0.18 (0.014) | 4.68 | 0.037 * | 0.12 |
| Left: 0.22 (0.013) | ||||
| Group (TD and ASD) | TD: 0.21 (0.015) | 1.29 | 0.26 | 0.036 |
| ASD: 0.19 (0.015) | ||||
| Two-way interaction | ||||
| Connectivity pattern × loading | 3.09 | 0.088 | 0.081 | |
| Connectivity pattern × frontal side | 0.037 | 0.85 | 0.001 | |
| Loading × frontal side | 2.42 | 0.13 | 0.065 | |
| Loading × group | 0.61 | 0.44 | 0.017 | |
| Connectivity pattern × group | 0.23 | 0.63 | 0.007 | |
| Frontal side × group | 8.98 | 0.005 ** | 0.20 | |
| Three-way interaction | ||||
| Connectivity pattern × loading × frontal side | 5.71 | 0.022 * | 0.14 | |
| Connectivity pattern × loading × group | 5.61 | 0.024 * | 0.14 | |
| Connectivity pattern × frontal side × group | 0.010 | 0.92 | 0.000 | |
| Loading × frontal side × group | 2.99 | 0.092 | 0.079 | |
| Four-way interaction | ||||
| Connectivity pattern × frontal side × loading × group | 0.006 | 0.94 | 0.000 |
| Main/Interaction Effects | Mean (SE) | F(1,34) | p | ηp2 |
|---|---|---|---|---|
| Connectivity pattern (within and between ROI) | Within ROI: 0.19 (0.014) | 10.06 | 0.003 ** | 0.23 |
| Between ROI: 0.20 (0.013) | ||||
| Loading (low and high) | Low: 0.21 (0.015) | 5.43 | 0.026 * | 0.14 |
| High: 0.18 (0.014) | ||||
| Group (TD and ASD) | TD: 0.21 (0.019) | 2.14 | 0.15 | 0.059 |
| ASD: 0.17 (0.018) | ||||
| Two-way interaction | ||||
| Connectivity pattern × loading | 0.75 | 0.39 | 0.021 | |
| Loading × group | 1.44 | 0.24 | 0.041 | |
| Connectivity pattern × group | 4.41 | 0.043 * | 0.12 | |
| Three-way interaction | ||||
| Connectivity pattern × loading × group | 0.14 | 0.71 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krishnamurthy, K.; Yeung, M.K.; Chan, A.S.; Han, Y.M.Y. Effortful Control and Prefrontal Cortex Functioning in Children with Autism Spectrum Disorder: An fNIRS Study. Brain Sci. 2020, 10, 880. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110880
Krishnamurthy K, Yeung MK, Chan AS, Han YMY. Effortful Control and Prefrontal Cortex Functioning in Children with Autism Spectrum Disorder: An fNIRS Study. Brain Sciences. 2020; 10(11):880. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110880
Chicago/Turabian StyleKrishnamurthy, Karthikeyan, Michael K. Yeung, Agnes S. Chan, and Yvonne M. Y. Han. 2020. "Effortful Control and Prefrontal Cortex Functioning in Children with Autism Spectrum Disorder: An fNIRS Study" Brain Sciences 10, no. 11: 880. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110880