Does the Occurrence of Particular Symptoms and Outcomes of Arterial Ischemic Stroke Depend on Sex in Pediatric Patients?—A Pilot Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Neurological Examinations
2.3. Criteria for Dividing Participants into Subgroups
2.4. Consequences of Ischemic Stroke
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
3.2. Analysis of the Prevalence of AIS Symptoms
3.3. Analysis of the Prevalence of Post-Stroke Consequences
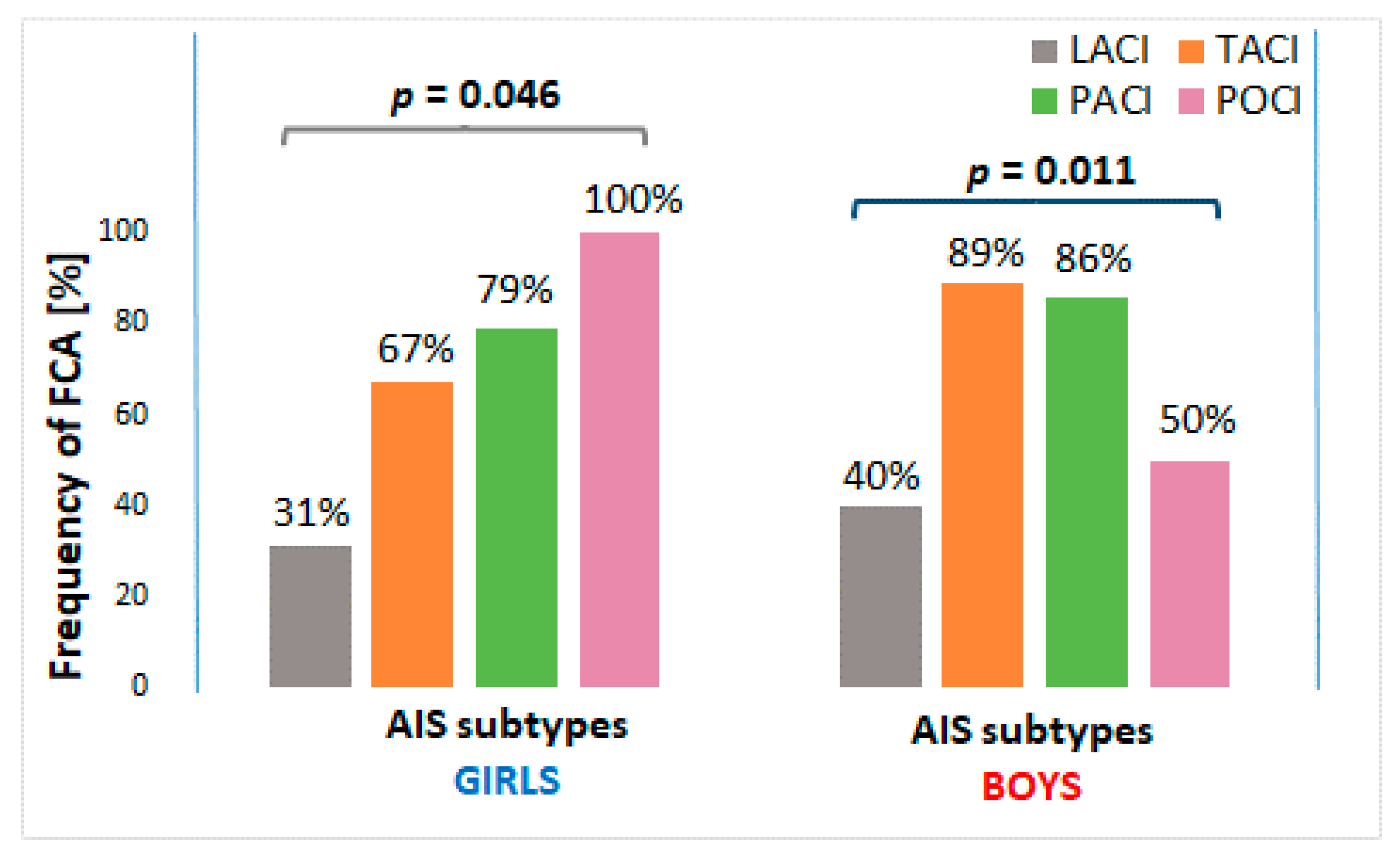
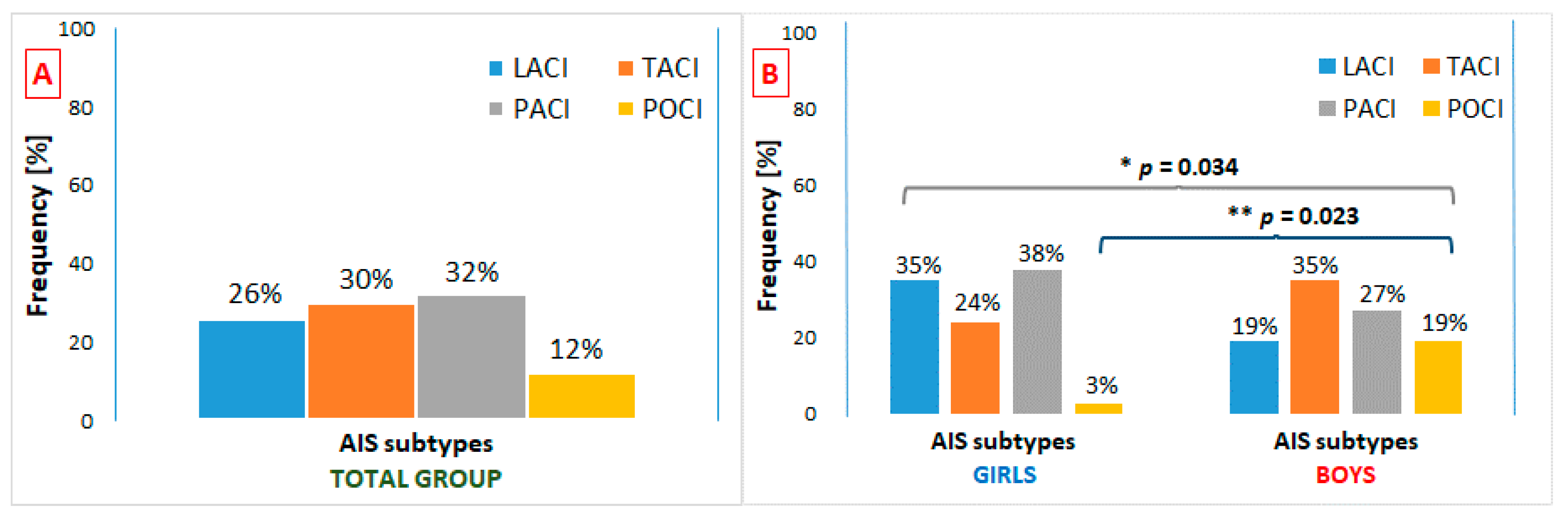
3.4. Neurological Symptoms and Consequences of AIS in Subgroups Due to AIS Location
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Amlie-Lefond, C.; Bernard, T.J.; Sébire, G.; Friedman, N.R.; Heyer, G.L.; Lerner, N.B.; de Veber, G.; Fullerton, H.J. Predictors of Cerebral Arteriopathy in Children With Arterial Ischemic Stroke: Results of the International Pediatric Stroke Study. Circulation 2009, 119, 1417–1423. [Google Scholar] [CrossRef] [Green Version]
- Sébire, G.; Fullerton, H.; Riou, E.; de Veber, G. Toward the definition of cerebral arteriopathies of childhood. Curr. Opin. Pediatr. 2004, 16, 617–622. [Google Scholar] [CrossRef]
- Fullerton, H.J.; Wu, Y.W.; Zhao, S.; Johnston, S.C. Risk of stroke in children: Ethnic and gender disparities. Neurology 2003, 61, 189–194. [Google Scholar] [CrossRef]
- Agrawal, N.; Johnston, S.C.; Wu, Y.W.; Sidney, S.; Fullerton, H.J. Imaging Data Reveal a Higher Pediatric Stroke Incidence Than Prior US Estimates. Stroke 2009, 40, 3415–3421. [Google Scholar] [CrossRef] [Green Version]
- Mallick, A.A.; Ganesan, V.; Kirkham, F.J.; Fallon, P.; Hedderly, T.; McShane, T.; Parker, A.P.; Wassmer, E.; Wraige, E.; Amin, S.; et al. Childhood arterial ischaemic stroke incidence, presenting features, and risk factors: A prospective population-based study. Lancet Neurol. 2014, 13, 35–43. [Google Scholar] [CrossRef]
- National Center for Injury Prevention and Control, CDC. 10 Leading Causes of Death by Age Group. 2018. Available online: https://www.cdc.gov/injury/wisqars/pdf/leading_causes_of_death_by_age_group_2018-508.pdf (accessed on 2 July 2020).
- Krishnamurthi, R.V.; de Veber, G.; Feigin, V.L.; Barker-Collo, S.; Fullerton, H.; Mackay, M.T.; O’Callahan, F.; Lindsay, M.P.; Kolk, A.; Lo, W.; et al. GBD 2013 Stroke Panel Experts Group. Stroke Prevalence, Mortality and Disability-Adjusted Life Years in Children and Youth Aged 0–19 Years: Data from the Global and Regional Burden of Stroke 2013. Neuroepidemiology 2015, 45, 177–189. [Google Scholar] [CrossRef] [Green Version]
- Beslow, L.A.; Dowling, M.M.; Hassanein, S.M.A.; Lynch, J.K.; Zafeiriou, D.; Sun, L.R.; Kopyta, I.; Titomanlio, L.; Kolk, A.; Chan, A.; et al. Mortality after Pediatric Arterial Ischemic Stroke. Pediatrics 2018, 141, e20174146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fullerton, H.J.; Stence, N.; Hills, N.K.; Jiang, B.; Amlie-Lefond, C.; Bernard, T.J.; Friedman, N.R.; Ichord, R.; Mackay, M.T.; Rafay, M.F.; et al. Focal Cerebral Arteriopathy of Childhood: Novel Severity Score and Natural History. Stroke 2018, 49, 2590–2596. [Google Scholar] [CrossRef]
- Lopez-Vicente, M.; Ortega-Gutierrez, S.; Amlie-Lefond, C.; Torbey, M.T. Diagnosis and Management of Pediatric Arterial Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2010, 19, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Kopyta, I.; Sarecka-Hujar, B.; Skrzypek, M. Post-stroke epilepsy in Polish paediatric patients. Dev. Med. Child Neurol. 2015, 57, 821–828. [Google Scholar] [CrossRef] [Green Version]
- Ahnstedt, H.; McCullough, L.D.; Cipolla, M.J. The Importance of Considering Sex Differences in Translational Stroke Research. Transl. Stroke Res. 2016, 7, 261–273. [Google Scholar] [CrossRef] [Green Version]
- Gibson, C.L. Cerebral Ischemic Stroke: Is Gender Important? J. Cereb. Blood Flow Metab. 2013, 33, 1355–1361. [Google Scholar] [CrossRef]
- Manwani, B.; McCullough, L.D. Sexual Dimorphism in Ischemic Stroke: Lessons from the Laboratory. Womens Health 2011, 7, 319–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritzel, R.M.; Capozzi, L.A.; McCullough, L.D. Sex, stroke, and inflammation: The potential for estrogen-mediated immunoprotection in stroke. Horm. Behav. 2013, 63, 238–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, F.; McCullough, L.D. Interactions between age, sex, and hormones in experimental ischemic stroke. Neurochem. Int. 2012, 61, 1255–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szczepanek, D.; Grochowski, C.; Litak, J.; Janusz, W.; Maciejewski, R.; Trojanowski, T. Moyamoya disease among Polish population: Single clinic experience and literature review. Postępy Nauk Med. 2017, 10, 549–553. [Google Scholar] [CrossRef]
- Pittock, S.J.; Meldrum, D.; Hardiman, O.; Thornton, J.; Brennan, P.; Moroney, J.T. The Oxfordshire Community Stroke Project classification: Correlation with imaging, associated complications, and prediction of outcome in acute ischemic stroke. J. Stroke Cerebrovasc. Dis. 2003, 12, 1–7. [Google Scholar] [CrossRef]
- Beslow, L.A.; Abend, N.S.; Gindville, M.C.; Bastian, R.A.; Licht, D.J.; Smith, S.E.; Hillis, A.E.; Ichord, R.N.; Jordan, L.C. Pediatric intracerebral hemorrhage: Acute symptomatic seizures and epilepsy. JAMA Neurol. 2013, 70, 448–454. [Google Scholar] [CrossRef] [Green Version]
- De Veber, G.A.; Kirton, A.; Booth, F.A.; Yager, J.Y.; Wirrell, E.C.; Wood, E.; Shevell, M.; Surmava, A.-M.; McCusker, P.; Massicotte, M.P.; et al. Epidemiology and Outcomes of Arterial Ischemic Stroke in Children: The Canadian Pediatric Ischemic Stroke Registry. Pediatr. Neurol. 2017, 69, 58–70. [Google Scholar] [CrossRef]
- Goeggel Simonetti, B.; Ritter, B.; Gautschi, M.; Wehrli, E.; Boltshauser, E.; Schmitt-Mechelke, T.; Weber, P.; Weissert, M.; El-Koussy, M.; Steinlin, M. Basilar artery stroke in childhood: Basilar Artery Stroke in Childhood. Dev. Med. Child Neurol. 2013, 55, 65–70. [Google Scholar] [CrossRef]
- Golomb, M.R.; Fullerton, H.J.; Nowak-Gottl, U.; de Veber, G.; for the International Pediatric Stroke Study Group. Male Predominance in Childhood Ischemic Stroke: Findings from the International Pediatric Stroke Study. Stroke 2009, 40, 52–57. [Google Scholar] [CrossRef] [Green Version]
- Chung, B.; Wong, V. Pediatric Stroke among Hong Kong Chinese Subjects. Pediatrics 2004, 114, e206–e212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Per, H.; Unal, E.; Poyrazoglu, H.G.; Ozdemir, M.A.; Donmez, H.; Gumus, H.; Uzum, K.; Canpolat, M.; Akyildiz, B.N.; Coskun, A.; et al. Childhood Stroke: Results of 130 Children From a Reference Center in Central Anatolia, Turkey. Pediatr. Neurol. 2014, 50, 595–600. [Google Scholar] [CrossRef]
- Vázquez López, M.; de Castro de Castro, P.; Barredo Valderrama, E.; Miranda Herrero, M.C.; Gil Villanueva, N.; Alcaraz Romero, A.J.; Pascual, S.I. Outcome of arterial ischemic stroke in children with heart disease. Eur. J. Paediatr. Neurol. 2017, 21, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Carey, S.; Wrogemann, J.; Booth, F.A.; Rafay, M.F. Epidemiology, Clinical Presentation, and Prognosis of Posterior Circulation Ischemic Stroke in Children. Pediatr. Neurol. 2017, 74, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Balcerzyk, A.; Nowak, M.; Kopyta, I.; Emich-Widera, E.; Pilarska, E.; Pienczk-Ręcławowicz, K.; Kaciński, M.; Wendorff, J.; Zak, I. Impact of the -174G/C interleukin-6 (IL-6) gene polymorphism on the risk of paediatric ischemic stroke, its symptoms and outcome. Folia Neuropathol. 2012, 50, 147–151. [Google Scholar] [PubMed]
- Muwakkit, S.A.; Majdalani, M.; Hourani, R.; Mahfouz, R.A.; Otrock, Z.K.; Bilalian, C.; Chan, A.K.; Abboud, M.; Mikati, M.A. Inherited thrombophilia in childhood arterial stroke: Data from Lebanon. Pediatr. Neurol. 2011, 45, 155–158. [Google Scholar] [CrossRef] [PubMed]
- López-Espejo, M.; Hernández-Chávez, M. Prevalence and Predictors of Long-Term Functional Impairment, Epilepsy, Mortality, and Stroke Recurrence after Childhood Stroke: A Prospective Study of a Chilean Cohort. J. Stroke Cerebrovasc. Dis. 2017, 26, 1646–1652. [Google Scholar] [CrossRef]
- Felling, R.J.; Sun, L.R.; Maxwell, E.C.; Goldenberg, N.; Bernard, T. Pediatric arterial ischemic stroke: Epidemiology, risk factors, and management. Blood Cells Mol. Dis. 2017, 67, 23–33. [Google Scholar] [CrossRef]
- Denti, L.; Artoni, A.; Scoditti, U.; Caminiti, C.; Giambanco, F.; Casella, M.; Ceda, G.P. Impact of gender–age interaction on the outcome of ischemic stroke in an Italian cohort of patients treated according to a standardized clinical pathway. Eur. J. Intern. Med. 2013, 24, 807–812. [Google Scholar] [CrossRef]
- Geng, C.; Lin, Y.; Tang, Q.; Tang, Y.; Wang, X.; Zhou, J.S.; Yang, J.; Zheng, D.; Zhang, Y.D.; Nanjing First Hospital Stroke Registry Investigators. Sex differences in clinical characteristics and 1-year outcomes of young ischemic stroke patients in East China. Ther. Clin. Risk Manag. 2018, 15, 33–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- İncecik, F.; Hergüner, Ö.M.; Besen, Ş. Risk factors for epilepsy after ischemic stroke in children. İzmir Dr. Behçet Uz Çocuk Hastan. Dergisi 2017, 7, 178–182. [Google Scholar] [CrossRef] [Green Version]
- Laugesaar, R.; Vaher, U.; Lõo, S.; Kolk, A.; Männamaa, M.; Talvik, I.; Õiglane-Shlik, E.; Loorits, D.; Talvik, T.; Ilves, P. Epilepsy after perinatal stroke with different vascular subtypes. Epilepsia Open 2018, 3, 193–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirton, A.; deVeber, G.; Pontigon, A.M.; Macgregor, D.; Shroff, M. Presumed perinatal ischemic stroke: Vascular classification predicts outcomes. Ann. Neurol. 2008, 63, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Ilves, P.; Tomberg, T.; Kepler, J.; Laugesaar, R.; Kaldoja, M.L.; Kepler, K.; Kolk, A. Different plasticity patterns of language function in children with perinatal and childhood stroke. J. Child Neurol. 2014, 29, 756–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westmacott, R.; MacGregor, D.; Askalan, R.; de Veber, G. Late emergence of cognitive deficits after unilateral neonatal stroke. Stroke 2009, 40, 2012–2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chelse, A.B.; Kurz, J.E.; Gorman, K.M.; Epstein, L.G.; Balmert, L.C.; Ciolino, J.D.; Wainwright, M.S. Remote poststroke headache in children: Characteristics and association with stroke recurrence. Neurol. Clin. Pract. 2019, 9, 194–200. [Google Scholar] [CrossRef]
- Abdullahi, S.U.; De Baun, M.R.; Jordan, L.C.; Rodeghier, M.; Galadanci, N.A. Stroke Recurrence in Nigerian Children With Sickle Cell Disease: Evidence for a Secondary Stroke Prevention Trial. Pediatr. Neurol. 2019, 95, 73–78. [Google Scholar] [CrossRef]
- Vaartjes, I.; Reitsma, J.B.; Berger-van Sijl, M.; Bots, M.L. Gender Differences in Mortality after Hospital Admission for Stroke. Cerebrovasc. Dis. 2009, 28, 564–571. [Google Scholar] [CrossRef]
- Ganesan, V.; Chong, W.K.; Cox, T.C.; Chawda, S.J.; Prengler, M.; Kirkham, F.J. Posterior circulation stroke in childhood: Risk factors and recurrence. Neurology 2002, 59, 1552–1556. [Google Scholar] [CrossRef]
- Mackay, M.T.; Prabhu, S.P.; Coleman, L. Childhood posterior circulation arterial ischemic stroke. Stroke 2010, 41, 2201–2209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Öztürk, Ş.; Ege, F.; Ekmekçi, H. Language Disorders due to Posterior System Strokes—An Ignored Dysfunction. Noro Psikiyatr. Arşivi. 2014, 51, 313–317. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group/Subgroup of AIS Patients | Number of Male Subjects | Male:Female Ratio | Proportion of Male Subjects | Lower and Upper Limits of 95%CI for Proportion of Male Subjects |
|---|---|---|---|---|
| Total (N = 89) | 52 | 1.41:1 | 0.584 | (0.475–0.686) |
| Infant–Toddlers (N = 17) | 11 | 1.83:1 | 0.647 | (0.386–0.847) |
| Children (N = 41) | 22 | 1.16:1 | 0.537 | (0.376–0.690) |
| Adolescents (N = 31) | 19 | 1.58:1 | 0.613 | (0.438–0.763) |
| LACI (N = 23) | 10 | 0.78:1 | 0.435 | (0.239–0.651) |
| TACI (N = 27) | 18 | 2:1 | 0.667 | (0.460–0.828) |
| PACI (N = 28) | 14 | 1:1 | 0.500 | (0.311–0.689) |
| POCI (N = 11) | 10 | 10:1 | 0.909 | (0.571–0.995) |
| Total Group N = 89 | Girls with AIS N = 37 (42%) | Boys with AIS N = 52 (58%) | p | |
|---|---|---|---|---|
| Age at stroke onset (years), M ± SD | 8.40 ± 5.56 | 8.40 ± 5.16 | 8.39 ± 5.89 | 0.997 |
| Median, (Min.–Max.) | 8 (0.11–18) | 8 (1–17) | 7 (0.11–18) | |
| Interquartile range (IQR) | 11 (3–14) | 9.25 (3–12.5) | 11 (4–15) | |
| Birth weight (g), M ± SD | 3093.39 ± 532 | 2956 ± 514 | 3186 ± 531 | 0.094 |
| FCA, n (%) | 59 (66) | 22 (60) | 37 (71) | 0.265 |
| Heart disease, n (%) | 14 (16) | 6 (16) | 8 (15) | 1.000 |
| Number of infarct foci, n (%) | 1.000 | |||
| One | 62 (70) | 26 (70) | 36 (69) | |
| Two or more | 13 (14) | 6 (16) | 7 (14) |
| GIRLS | Total N= 37 | LACI N= 13 | TACI N= 9 | PACI N= 14 | POCI N= 1 | p* |
| SYMPTOMS OF AIS | ||||||
| Hemiplegia, n (%) | 3 (8) | 0 (0) | 2 (22) | 1 (7) | 0 (0) | 0.301 |
| Hemiparesis, n (%) | 33 (89) | 12 (92) | 7 (78) | 13 (93) | 1 (100) | 0.582 |
| Central type facial nerve palsy, n (%) | 20 (54) | 7 (54) | 4 (44) | 8 (57) | 1 (100) | 0.953 |
| Consciousness disturbances, n (%) | 26 (70) | 9 (69) | 8 (89) | 8 (57) | 1 (100) | 0.389 |
| Headache, vertigo, n (%) | 10 (27) | 3 (23) | 1 (11) | 5 (36) | 1 (100) | 0.232 |
| Aphasia, n (%) | 14 (38) | 6 (46) | 4 (33) | 4 (29) | 1 (100) | 0.499 |
| Convulsions, n (%) | 6 (16) | 1 (8) | 2 (22) | 2 (14) | 1 (100) | 0.239 |
| Other symptoms, n (%) | 6 (16) | 3 (23) | 1 (11) | 1 (7) | 1 (100) | 0.185 |
| BOYS | Total N = 52 | LACI N = 10 | TACI N = 18 | PACI N = 14 | POCI N = 10 | p * |
| SYMPTOMS OF AIS | ||||||
| Hemiplegia, n (%) | 6 (12) | 1 (10) | 3 (17) | 2 (14) | 0 (0) | 0.781 |
| Hemiparesis, n (%) | 41 (79) | 9 (90) | 15 (83) | 10 (71) | 7 (70) | 0.652 |
| Central type facial nerve palsy, n (%) | 29 (56) | 5 (50) | 13 (72) | 9 (64) | 2 (20) | 0.050 |
| Consciousness disturbances, n (%) | 35 (67) | 6 (60) | 14 (78) | 9 (64) | 6 (60) | 0.680 |
| Headache, vertigo, n (%) | 18 (35) | 4 (40) | 8 (44) | 2 (14) | 4 (40) | 0.322 |
| Aphasia, n (%) | 22 (42) | 3 (30) | 9 (50) | 6 (43) | 4 (40) | 0.794 |
| Convulsions, n (%) | 9 (17) | 1 (10) | 3 (17) | 3 (17) | 2 (20) | 0.959 |
| Other symptoms, n (%) | 17 (33) | 1 (10) | 3 (17) | 4 (29) | 9 (90) | <0.001 |
| GIRLS | Total N= 37 | LACI N= 13 | TACI N= 9 | PACI N= 14 | POCI N= 1 | p* |
| POST-STROKE OUTCOMES | ||||||
| Hemiparesis, n (%) | 27 (73) | 7 (54%) | 9 (100) | 10 (71) | 1 (100) | 0.089 |
| Seizures, n (%) | 10 (27) | 1 (8) | 5 (56) | 3 (23) | 1 (100) | 0.022 |
| Aphasia, n (%) | 2 (5) | 0 (0) | 2 (22) | 0 (0) | 0 (0) | 0.108 |
| Other motor disturbances, n (%) | 4 (11) | 1 (8) | 1 (11) | 1 (7) | 1 (100) | 0.170 |
| Number of post-stroke outcomes, n (%) | 0.160 | |||||
| None | 8 (22) | 5 (38) | 0 (0) | 3 (21) | 0 (0) | |
| One or more | 29 (78) | 8 (62) | 9 (100) | 11 (79) | 1 (100) | |
| BOYS | Total N = 52 | LACI N = 10 | TACI N = 18 | PACI N = 14 | POCI N = 10 | p * |
| POST-STROKE OUTCOMES | ||||||
| Hemiparesis, n (%) | 33 (64) | 4 (40) | 16 (89) | 9 (64) | 4 (40) | 0.026 |
| Seizures, n (%) | 10 (19) | 1 (10) | 5 (28) | 2 (14) | 2 (20) | 0.721 |
| Aphasia, n (%) | 7 (14) | 0 (0) | 3 (17) | 2 (14) | 2 (20) | 0.668 |
| Other motor disturbances, n (%) | 5 (10) | 0 (0) | 2 (11) | 2 (14) | 1 (10) | 0.855 |
| Number of post-stroke outcomes, n (%) | 0.074 | |||||
| None | 13 (25) | 5 (50) | 2 (11) | 2 (14) | 4 (40) | |
| One or more | 39 (75) | 5 (50) | 16 (89) | 12 (86) | 6 (60) |
| SYMPTOMS OF AIS | Children with PS N = 11 | Children with AS N = 78 | p * | Girls with AS N = 36 | Boys with AS N = 42 | p ** |
|---|---|---|---|---|---|---|
| Hemiplegia, n (%) | 0 (0) | 9 (12) | 0.594 | 3 (8) | 6 (14) | 0.494 |
| Hemiparesis, n (%) | 8 (73) | 66 (85) | 0.387 | 32 (89) | 34 (81) | 0.367 |
| Central type facial nerve palsy, n (%) | 3 (27) | 46 (59) | 0.059 | 19 (53) | 27 (64) | 0.360 |
| Consciousness disturbances, n (%) | 7 (64) | 54 (69) | 0.736 | 25 (69) | 29 (69) | 1.000 |
| Headache, vertigo, n (%) | 5 (45) | 23 (29) | 0.284 | 9 (25) | 14 (33) | 0.464 |
| Aphasia, n (%) | 5 (45) | 31 (40) | 0.522 | 13 (36) | 18 (43) | 0.644 |
| Convulsions, n (%) | 3 (27) | 12 (15) | 0.387 | 5 (14) | 7 (17) | 0.765 |
| Other symptoms, n (%) | 10 (91) | 13 (17) | <0.001 | 5 (14) | 8 (19) | 0.762 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kopyta, I.; Dobrucka-Głowacka, A.; Cebula, A.; Sarecka-Hujar, B. Does the Occurrence of Particular Symptoms and Outcomes of Arterial Ischemic Stroke Depend on Sex in Pediatric Patients?—A Pilot Study. Brain Sci. 2020, 10, 881. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110881
Kopyta I, Dobrucka-Głowacka A, Cebula A, Sarecka-Hujar B. Does the Occurrence of Particular Symptoms and Outcomes of Arterial Ischemic Stroke Depend on Sex in Pediatric Patients?—A Pilot Study. Brain Sciences. 2020; 10(11):881. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110881
Chicago/Turabian StyleKopyta, Ilona, Anna Dobrucka-Głowacka, Agnieszka Cebula, and Beata Sarecka-Hujar. 2020. "Does the Occurrence of Particular Symptoms and Outcomes of Arterial Ischemic Stroke Depend on Sex in Pediatric Patients?—A Pilot Study" Brain Sciences 10, no. 11: 881. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10110881