Effect of High Intensity Interval Training Compared to Continuous Training on Cognitive Performance in Young Healthy Adults: A Pilot Study


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Experimental Design
2.3. Maximal Continuous Graded Exercise Test
2.4. Cognitive Testing
2.4.1. Computerized Modified Stroop Task
2.4.2. Trail Making Test
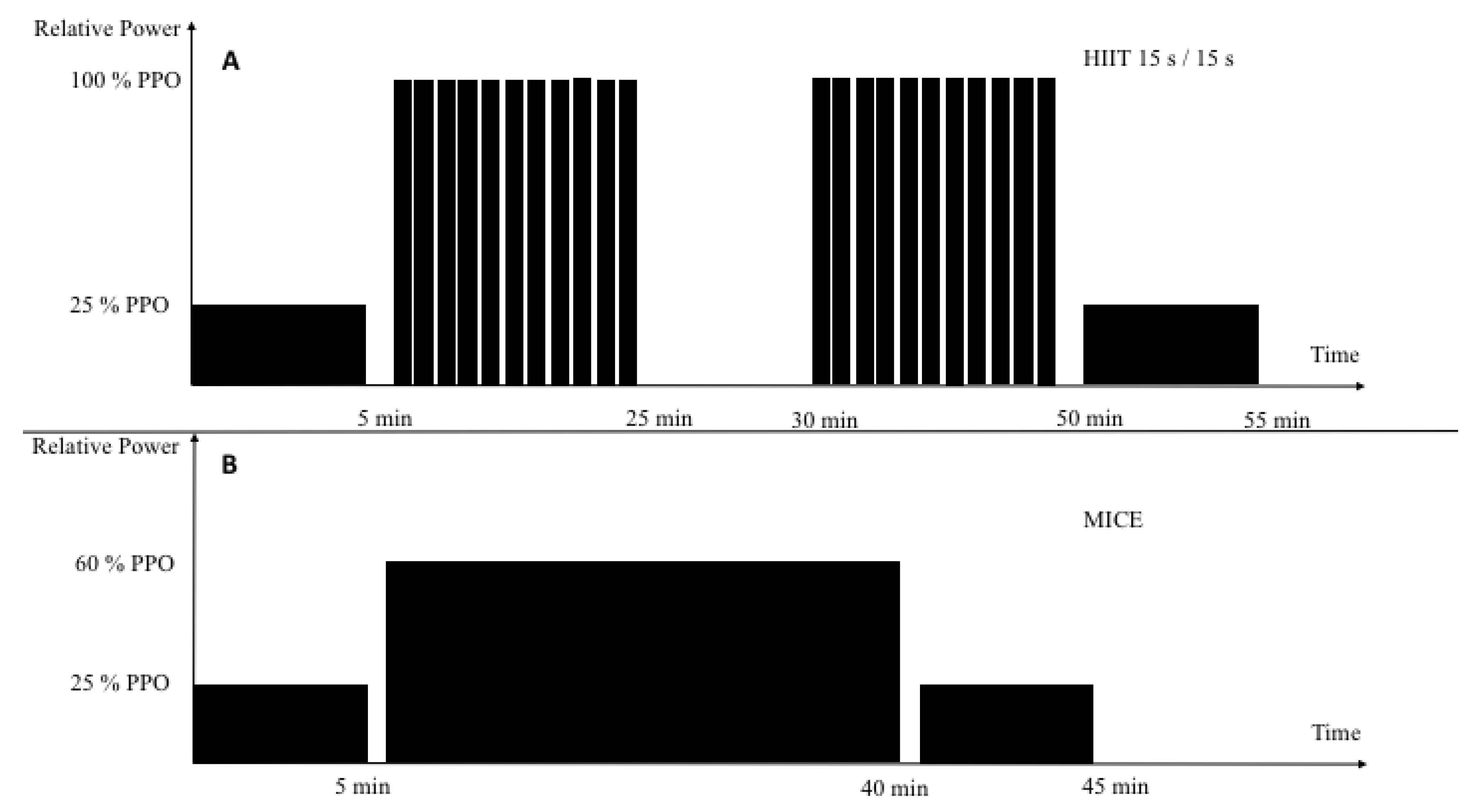
2.5. Training
2.6. Moderate-Intensity Continuous Exercise
2.7. High-Intensity Intermittent Training
3. Statistical Analysis
4. Results
4.1. Maximal Continuous Graded Exercise Test
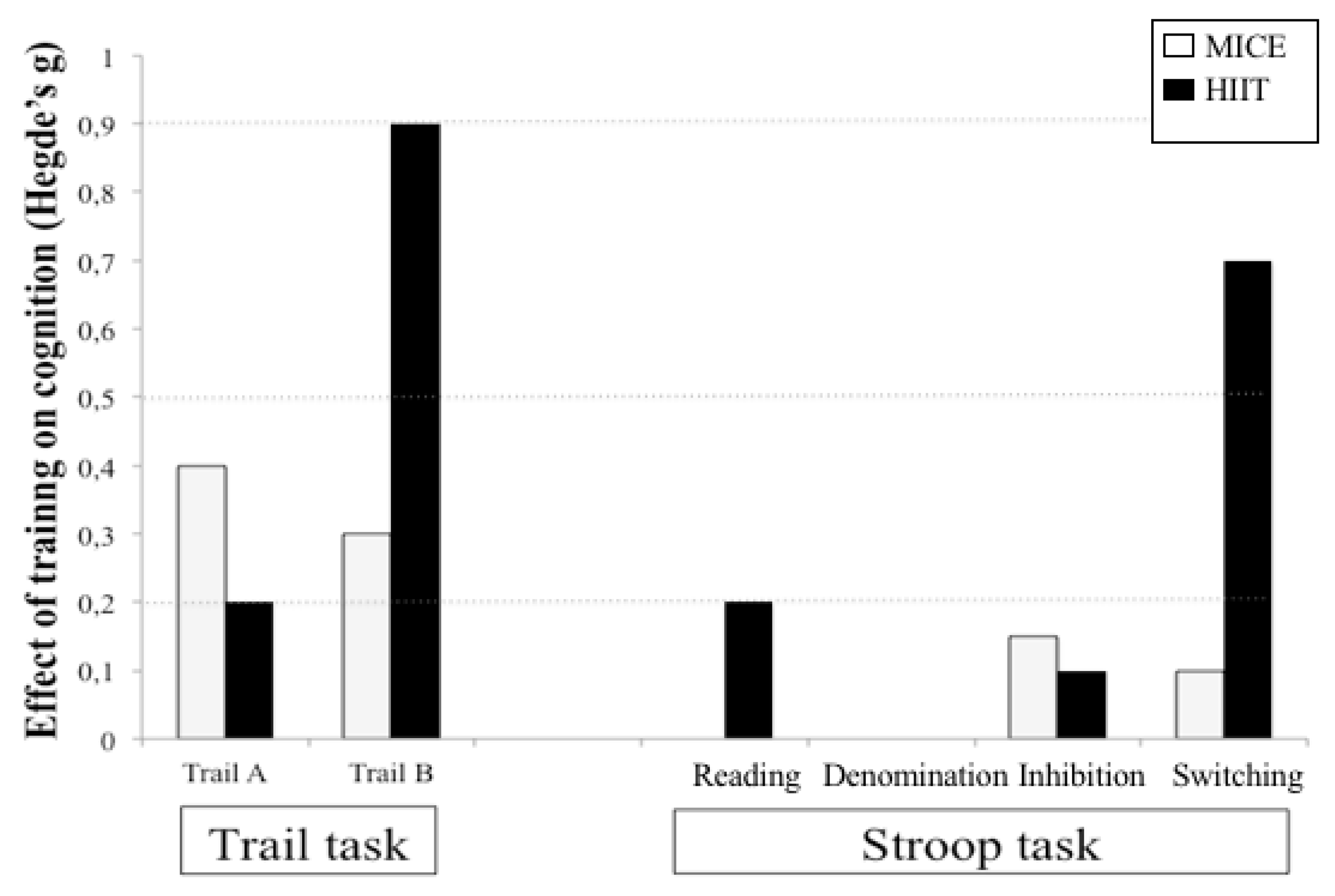
4.2. Cognitive Test
4.2.1. Stroop Task
4.2.2. Trail Making Test
5. Discussion
Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Budde, H.; Schwarz, R.; Velasques, B.; Ribeiro, P.; Holzweg, M.; Machado, S.; Brazaitis, M.; Staack, F. Wegner M8.The need for differentiating between exercise, physical activity, and training. Autoimmun. Rev. 2016, 15, 110–111. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tremblay, M.S.; Warburton, D.E.; Janssen, I.; Paterson, D.H.; Latimer, A.E.; Rhodes, R.E.; Kho, M.E.; Hicks, A.; Leblanc, A.G.; Zehr, L.; et al. New Canadian physical activity guidelines. Appl. Physiol. Nutr. Metab. 2011, 36, 47–58. [Google Scholar] [CrossRef]
- Bherer, L.; Erickson, K.I.; Liu-Ambrose, T. A review of the effects of physical activity and exercise on cognitive and brain functions in older adults. J. Aging Res. 2013, 2013, 657508. [Google Scholar] [CrossRef] [Green Version]
- Kramer, A.F.; Erickson, K.I.; Colcombe, S.J. Exercise, cognition, and the aging brain. J. Appl. Physiol. (1985) 2006, 101, 1237–1242. [Google Scholar] [CrossRef]
- Kramer, A.F.; Hahn, S.; Cohen, N.J.; Banich, M.T.; McAuley, E.; Harrison, C.R.; Chason, J.; Vakil, E.; Bardell, L.; Boileau, R.A.; et al. Ageing, fitness and neurocognitive function. Nature 1999, 400, 418–419. [Google Scholar] [CrossRef]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef]
- Stillman, C.M.; Cohen, J.; Lehman, M.E.; Erickson, K.I. Mediators of Physical Activity on Neurocognitive Function: A Review at Multiple Levels of Analysis. Front. Hum. Neurosci. 2016, 10, 626. [Google Scholar] [CrossRef] [Green Version]
- Cotman, C.W.; Berchtold, N.C. Exercise: A behavioral intervention to enhance brain health and plasticity. Trends Neurosci. 2002, 25, 295–301. [Google Scholar] [CrossRef]
- Cotman, C.W.; Berchtold, N.C.; Christie, L.A. Exercise builds brain health: Key roles of growth factor cascades and inflammation. Trends Neurosci. 2007, 30, 464–472. [Google Scholar] [CrossRef]
- Bullitt, E.; Rahman, F.N.; Smith, J.K.; Kim, E.; Zeng, D.; Katz, L.M.; Marks, B.L. The effect of exercise on the cerebral vasculature of healthy aged subjects as visualized by MR angiography. AJNR Am. J. Neuroradiol. 2009, 30, 1857–1863. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, O.; Gauthier, C.J.; Fraser, S.A.; Desjardins-Crepeau, L.; Desjardins, M.; Mekary, S.; Lesage, F.; Hoge, R.D.; Pouliot, P.; Bherer, L. Higher levels of cardiovascular fitness are associated with better executive function and prefrontal oxygenation in younger and older women. Front. Hum. Neurosci. 2015, 9, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mekari, S.; Dupuy, O.; Martins, R.; Evans, K.; Kimmerly, D.S.; Fraser, S.; Neyedli, H.F. The effects of cardiorespiratory fitness on executive function and prefrontal oxygenation in older adults. Geroscience 2019, 41, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Cao, M.; Quan, M.; Zhuang, J. Effect of High-Intensity Interval Training versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Children and Adolescents: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, S. High-intensity interval training for health benefits and care of cardiac diseases—The key to an efficient exercise protocol. World J. Cardiol. 2019, 11, 171–188. [Google Scholar] [CrossRef] [PubMed]
- Lucas, S.J.; Cotter, J.D.; Brassard, P.; Bailey, D.M. High-intensity interval exercise and cerebrovascular health: Curiosity, cause, and consequence. J. Cereb. Blood Flow Metab. 2015, 35, 902–911. [Google Scholar] [CrossRef]
- Reindell, H.; Roskamm, H. Ein Beitrag zu den physiologischen Grundlagen des Intervall training unter besonderer Berück- sichtigung des Kreilaufes. Schweiz Z Sportmed 1959, 7, 1–8. [Google Scholar]
- Billat, V.L. Interval training for performance: A scientific and empirical practice. Special recommendations for middle and long distance running. Part II: Anaerobic interval training. Sports Med. 2001, 31, 75–90. [Google Scholar] [CrossRef]
- Billat, V.L. Interval training for performance: A scientific and empirical practice. Special recommendations for middle and long distance running. Part I: Aerobic interval training. Sports Med. 2001, 31, 13–31. [Google Scholar] [CrossRef]
- Daniels, J.T.; Scardina, N. Interval training and performance. Sports Med. 1984, 1, 327–334. [Google Scholar] [CrossRef]
- Gaitanos, G.C.; Williams, C.; Boobis, L.H.; Brooks, S. Human muscle metabolism during intermittent maximal exercise. J. Appl. Physiol. 1993, 75, 712–719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laursen, P.B.; Jenkins, D.G. The scientific basis for high intensity interval training: Optimising training programmes and maximising performance in highly trained endurance athletes. Sports Med. 2002, 32, 53–73. [Google Scholar] [CrossRef] [PubMed]
- Daussin, F.N.; Ponsot, E.; Dufour, S.P.; Lonsdorfer-Wolf, E.; Doutreleau, S.; Geny, B.; Piquard, F.; Richard, R. Improvement of VO2max by cardiac output and oxygen extraction adaptation during intermittent versus continuous endurance training. Eur. J. Appl. Physiol. 2007, 101, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Daussin, F.N.; Zoll, J.; Dufour, S.P.; Ponsot, E.; Lonsdorfer-Wolf, E.; Doutreleau, S.; Mettauer, B.; Piquard, F.; Geny, B.; Richard, R. Effect of interval versus continuous training on cardiorespiratory and mitochondrial functions: Relationship to aerobic performance improvements in sedentary. Am. J. Physiol. 2008. [Google Scholar] [CrossRef] [Green Version]
- Helgerud, J.; Hoydal, K.; Wang, E.; Karlsen, T.; Berg, P.; Bjerkaas, M.; Simonsen, T.; Helgesen, C.; Hjorth, N.; Bach, R.; et al. Aerobic high-intensity intervals improve VO2max more than moderate training. Med. Sci. Sports Exerc. 2007, 39, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Juneau, M.; Roy, N.; Nigam, A.; Tardif, J.C.; Larivee, L. Exercise above the ischemic threshold and serum markers of myocardial injury. Can. J. Cardiol. 2009, 25, e338–e341. [Google Scholar] [CrossRef]
- Noël, M.; Jobin, J.; Marcoux, A.; Poirier, P.; Dagenais, G.; Bogaty, P. Can prolonged exercise-induced myocardial ischaemia be innocuous? Eur. Heart J. 2007, 28, 1559–1565. [Google Scholar] [CrossRef] [Green Version]
- van Gelder, B.M.; Tijhuis, M.A.; Kalmijn, S.; Giampaoli, S.; Nissinen, A.; Kromhout, D. Physical activity in relation to cognitive decline in elderly men: The FINE Study. Neurology 2004, 63, 2316–2321. [Google Scholar] [CrossRef]
- Angevaren, M.; Vanhees, L.; Wendel-Vos, W.; Verhaar, H.J.; Aufdemkampe, G.; Aleman, A.; Verschuren, W.M. Intensity, but not duration, of physical activities is related to cognitive function. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 825–830. [Google Scholar] [CrossRef]
- Brown, B.M.; Peiffer, J.J.; Sohrabi, H.R.; Mondal, A.; Gupta, V.B.; Rainey-Smith, S.R.; Taddei, K.; Burnham, S.; Ellis, K.A.; Szoeke, C.; et al. Intense physical activity is associated with cognitive performance in the elderly. Transl. Psychiatry 2012, 2, e191. [Google Scholar] [CrossRef] [Green Version]
- Freitas, D.A.; Rocha-Vieira, E.; De Sousa, R.A.L.; Soares, B.A.; Rocha-Gomes, A.; Chaves Garcia, B.C.; Cassilhas, R.C.; Mendonca, V.A.; Camargos, A.C.R.; De Gregorio, J.A.M.; et al. High-intensity interval training improves cerebellar antioxidant capacity without affecting cognitive functions in rats. Behav. Brain Res. 2019, 376, 112181. [Google Scholar] [CrossRef] [PubMed]
- Nicolini, C.; Toepp, S.; Harasym, D.; Michalski, B.; Fahnestock, M.; Gibala, M.J.; Nelson, A.J. No changes in corticospinal excitability, biochemical markers, and working memory after 6 weeks of high-intensity interval training in sedentary males. Physiol. Rep. 2019, 7, e14140. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.K.; Ha, C.H. The effect of exercise intensity on brain derived neurotrophic factor and memory in adolescents. Environ. Health Prev. Med. 2017, 22, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kovacevic, A.; Fenesi, B.; Paolucci, E.; Heisz, J.J. The effects of aerobic exercise intensity on memory in older adults. Appl. Physiol. Nutr. Metab. 2019. [Google Scholar] [CrossRef]
- Moreau, D.; Kirk, I.J.; Waldie, K.E. High-intensity training enhances executive function in children in a randomized, placebo-controlled trial. Elife 2017, 6. [Google Scholar] [CrossRef]
- Pallesen, H.; Bjerk, M.; Pedersen, A.R.; Nielsen, J.F.; Evald, L. The Effects of High-Intensity Aerobic Exercise on Cognitive Performance After Stroke: A Pilot Randomised Controlled Trial. J. Cent. Nerv. Syst. Dis. 2019, 11. [Google Scholar] [CrossRef] [Green Version]
- Venckunas, T.; Snieckus, A.; Trinkunas, E.; Baranauskiene, N.; Solianik, R.; Juodsnukis, A.; Streckis, V.; Kamandulis, S. Interval Running Training Improves Cognitive Flexibility and Aerobic Power of Young Healthy Adults. J. Strength Cond. Res. 2016, 30, 2114–2121. [Google Scholar] [CrossRef]
- Bowie, C.R.; Harvey, P.D. Administration and interpretation of the Trail Making Test. Nat. Protoc. 2006, 1, 2277–2281. [Google Scholar] [CrossRef]
- O’Brien, M.W.; Johns, J.A.; Robinson, S.A.; Bungay, A.; Mekary, S.; Kimmerly, D.S. Impact of HIIT, MICT, and Resistance Training on Endothelial Function in Older Adults. Med. Sci. Sports Exerc. 2019. [Google Scholar] [CrossRef]
- Guiraud, T.; Juneau, M.; Nigam, A.; Gayda, M.; Meyer, P.; Mekary, S.; Paillard, F.; Bosquet, L. Optimization of high intensity interval exercise in coronary heart disease. Eur. J. Appl. Physiol. 2010, 108, 733–740. [Google Scholar] [CrossRef]
- Dupuy, O.; Lussier, M.; Fraser, S.; Bherer, L.; Audiffren, M.; Bosquet, L. Effect of overreaching on cognitive performance and related cardiac autonomic control. Scand. J. Med. Sci. Sports 2014, 24, 234–242. [Google Scholar] [CrossRef] [PubMed]
- Rognmo, O.; Hetland, E.; Helgerud, J.; Hoff, J.; Slordahl, S.A. High intensity aerobic interval exercise is superior to moderate intensity exercise for increasing aerobic capacity in patients with coronary artery disease. Eur. J. Cardiovasc. Prev. Rehabil. 2004, 11, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Scharf, M.; Lell, M.; Petrasek, C.; von Stengel, S. High versus moderate intensity running exercise to impact cardiometabolic risk factors: The randomized controlled RUSH-study. Biomed. Res. Int. 2014, 2014, 843095. [Google Scholar] [CrossRef] [PubMed]
- Bacon, A.P.; Carter, R.E.; Ogle, E.A.; Joyner, M.J. VO2max trainability and high intensity interval training in humans: A meta-analysis. PLoS ONE 2013, 8, e73182. [Google Scholar] [CrossRef] [PubMed]
- Scribbans, T.D.; Vecsey, S.; Hankinson, P.B.; Foster, W.S.; Gurd, B.J. The Effect of Training Intensity on VO2max in Young Healthy Adults: A Meta-Regression and Meta-Analysis. Int. J. Exerc. Sci. 2016, 9, 230–247. [Google Scholar] [PubMed]
- Colcombe, S.J.; Kramer, A.F.; Erickson, K.I.; Scalf, P.; McAuley, E.; Cohen, N.J.; Webb, A.; Jerome, G.J.; Marquez, D.X.; Elavsky, S. Cardiovascular fitness, cortical plasticity, and aging. Proc. Natl. Acad. Sci. USA 2004, 101, 3316–3321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smiley-Oyen, A.L.; Lowry, K.A.; Francois, S.J.; Kohut, M.L.; Ekkekakis, P. Exercise, fitness, and neurocognitive function in older adults: The “selective improvement” and “cardiovascular fitness” hypotheses. Ann. Behav. Med. 2008, 36, 280–291. [Google Scholar] [CrossRef] [Green Version]
- Madden, D.J.; Blumenthal, J.A.; Allen, P.A.; Emery, C.F. Improving aerobic capacity in healthy older adults does not necessarily lead to improved cognitive performance. Psychol. Aging 1989, 4, 307–320. [Google Scholar] [CrossRef]
- Etnier, J.L.; Nowell, P.M.; Landers, D.M.; Sibley, B.A. A meta-regression to examine the relationship between aerobic fitness and cognitive performance. Brain Res. Rev. 2006, 52, 119–130. [Google Scholar] [CrossRef] [Green Version]
- Best, J.R. Effects of Physical Activity on Children’s Executive Function: Contributions of Experimental Research on Aerobic Exercise. Dev. Rev. 2010, 30, 331–551. [Google Scholar] [CrossRef]
- Piepmeier, A.T.; Etnier, J.L. Brain-derived neurotrophic factor (BDNF) as a potential mechanism of the effects of acute exercise on cognitive performance. J. Sport Health Sci. 2015, 4, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Piepmeier, A.T.; Etnier, J.L.; Wideman, L.; Berry, N.T.; Kincaid, Z.; Weaver, M.A. A preliminary investigation of acute exercise intensity on memory and BDNF isoform concentrations. Eur. J. Sport Sci. 2019. [Google Scholar] [CrossRef] [PubMed]
- Schmolesky, M.T.; Webb, D.L.; Hansen, R.A. The effects of aerobic exercise intensity and duration on levels of brain-derived neurotrophic factor in healthy men. J. Sports Sci. Med. 2013, 12, 502–511. [Google Scholar] [PubMed]
- Winter, B.; Breitenstein, C.; Mooren, F.C.; Voelker, K.; Fobker, M.; Lechtermann, A.; Krueger, K.; Fromme, A.; Korsukewitz, C.; Floel, A.; et al. High impact running improves learning. Neurobiol. Learn. Mem. 2007, 87, 597–609. [Google Scholar] [CrossRef]
- Enette, L.; Vogel, T.; Fanon, J.L.; Lang, P.O. Effect of Interval and Continuous Aerobic Training on Basal Serum and Plasma Brain-Derived Neurotrophic Factor Values in Seniors: A Systematic Review of Intervention Studies. Rejuvenation Res. 2017, 20, 473–483. [Google Scholar] [CrossRef]
- Jimenez-Maldonado, A.; Renteria, I.; Garcia-Suarez, P.C.; Moncada-Jimenez, J.; Freire-Royes, L.F. The Impact of High-Intensity Interval Training on Brain Derived Neurotrophic Factor in Brain: A Mini-Review. Front. Neurosci. 2018, 12, 839. [Google Scholar] [CrossRef]
- Saucedo Marquez, C.M.; Vanaudenaerde, B.; Troosters, T.; Wenderoth, N. High-intensity interval training evokes larger serum BDNF levels compared with intense continuous exercise. J. Appl. Physiol. (1985) 2015, 119, 1363–1373. [Google Scholar] [CrossRef] [Green Version]
- Lou, S.J.; Liu, J.Y.; Chang, H.; Chen, P.J. Hippocampal neurogenesis and gene expression depend on exercise intensity in juvenile rats. Brain Res. 2008, 1210, 48–55. [Google Scholar] [CrossRef]
- Freitas, D.A.; Rocha-Vieira, E.; Soares, B.A.; Nonato, L.F.; Fonseca, S.R.; Martins, J.B.; Mendonca, V.A.; Lacerda, A.C.; Massensini, A.R.; Poortamns, J.R.; et al. High intensity interval training modulates hippocampal oxidative stress, BDNF and inflammatory mediators in rats. Physiol. Behav. 2018, 184, 6–11. [Google Scholar] [CrossRef]
- Ainslie, P.N.; Cotter, J.D.; George, K.P.; Lucas, S.; Murrell, C.; Shave, R.; Thomas, K.N.; Williams, M.J.; Atkinson, G. Elevation in cerebral blood flow velocity with aerobic fitness throughout healthy human ageing. J. Physiol. 2008, 586, 4005–4010. [Google Scholar] [CrossRef]
- Dustman, R.E.; Emmerson, R.Y.; Ruhling, R.O.; Shearer, D.E.; Steinhaus, L.A.; Johnson, S.C.; Bonekat, H.W.; Shigeoka, J.W. Age and fitness effects on EEG, ERPs, visual sensitivity, and cognition. Neurobiol. Aging 1990, 11, 193–200. [Google Scholar] [CrossRef]
- Robinson, M.M.; Lowe, V.J.; Nair, K.S. Increased Brain Glucose Uptake After 12 Weeks of Aerobic High-Intensity Interval Training in Young and Older Adults. J. Clin. Endocrinol. Metab. 2018, 103, 221–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| HIIT | MICE | |||
|---|---|---|---|---|
| PRE | POST | PRE | POST | |
| Age | 29 ± 10.3 | 35 ± 7.4 | ||
| Height (m) | 1.7 ± 0.1 | 1.7 ± 0.1 | ||
| Gender | 9 F, 3 M | 9 F, 4 M | ||
| Weight (kg) | 71.3 ± 13.0 | 70.8 ± 13.4 | 81.3 ± 13.0 | 82.4 ± 23.1 |
| BMI | 24.6 ± 5.0 | 24.4 ± 5.1 | 28.8 ± 8.0 | 29.2 ± 8.2 |
| max (mL/kg/min) | 39.7 ± 8.7 | 41 ± 8.4 | 33.8 ± 8.3 | 35.9 ± 8.6 |
| MAP (W) | 207 ± 44.9 | 217 ± 42.2 a | 180 ± 41.4 | 213 ± 43.0 a |
| HIIT | MICE | |||
|---|---|---|---|---|
| PRE | POST | PRE | POST | |
| Stroop Task (ms) | ||||
| Reading | 598.83 ± 99.40 | 574.15 ±106 | 604.43 ± 89.12 | 602.58 ± 95.66 |
| Denomination | 646.11 ± 93.67 | 616.33 ± 99.30 | 646.11 ± 93.67 | 644.59 ± 92.10 |
| Inhibition | 688.65 ± 95.47 | 680.94 ± 102.20 | 721.67 ± 110.07 | 687.41 ± 86.78 |
| Switching | 980.43 ± 135.27 | 860.04 ± 75.63 a | 1008.45 ± 218.76 | 987.77 ± 188.20 |
| Trail A (sec) | 16.47 ± 4.76 | 15.44 ± 3.09 | 16.64 ± 4.21 | 16.45 ± 3.42 |
| Trail B (sec) | 42.35 ± 14.86 | 30.35 ± 4.13 ab | 33.15 ± 7.06 | 34.13 ± 9.91 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mekari, S.; Earle, M.; Martins, R.; Drisdelle, S.; Killen, M.; Bouffard-Levasseur, V.; Dupuy, O. Effect of High Intensity Interval Training Compared to Continuous Training on Cognitive Performance in Young Healthy Adults: A Pilot Study. Brain Sci. 2020, 10, 81. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10020081
Mekari S, Earle M, Martins R, Drisdelle S, Killen M, Bouffard-Levasseur V, Dupuy O. Effect of High Intensity Interval Training Compared to Continuous Training on Cognitive Performance in Young Healthy Adults: A Pilot Study. Brain Sciences. 2020; 10(2):81. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10020081
Chicago/Turabian StyleMekari, Said, Meghan Earle, Ricardo Martins, Sara Drisdelle, Melanie Killen, Vicky Bouffard-Levasseur, and Olivier Dupuy. 2020. "Effect of High Intensity Interval Training Compared to Continuous Training on Cognitive Performance in Young Healthy Adults: A Pilot Study" Brain Sciences 10, no. 2: 81. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10020081