Do Adolescents Use Substances to Relieve Uncomfortable Sensations? A Preliminary Examination of Negative Reinforcement among Adolescent Cannabis and Alcohol Users

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Interview
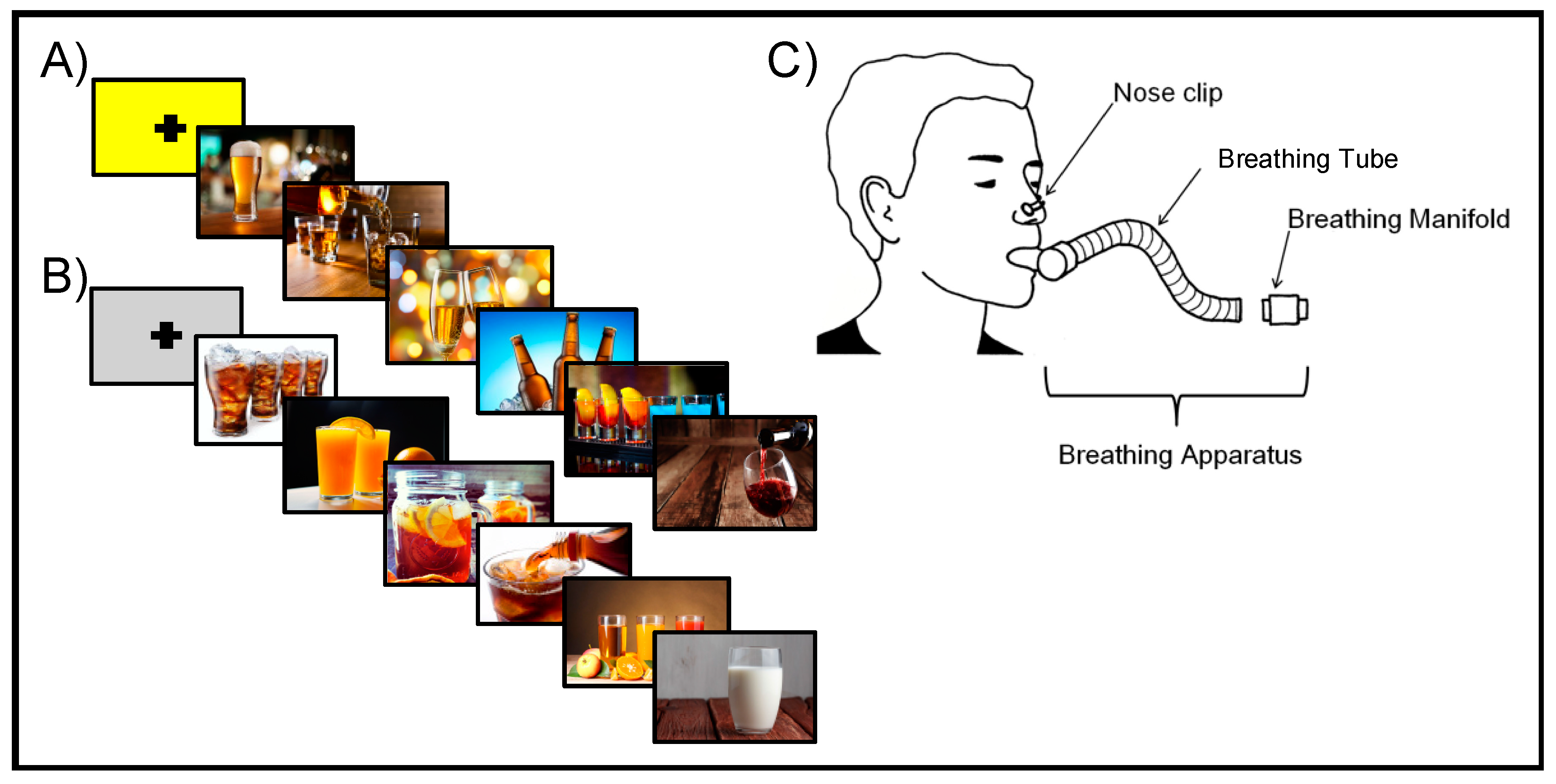
2.3. Neuroimaging Procedures
2.4. Neuroimaging Data Acquisition
2.5. Neuroimaging Data Analysis
2.5.1. Individual-Level Processing
2.5.2. Group-Level Analysis
3. Results
3.1. Subject Characteristics
3.2. Neuroimaging Results
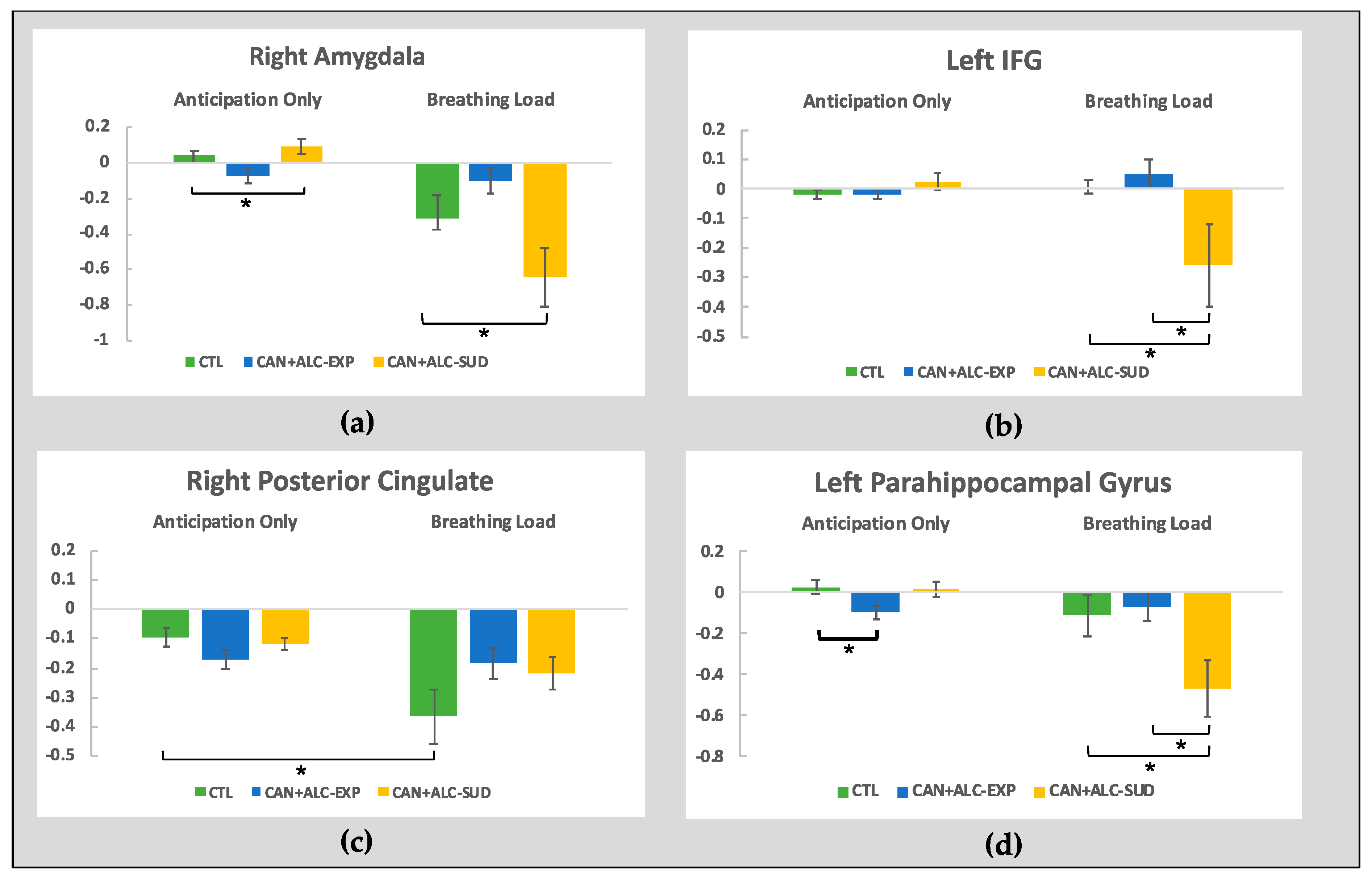
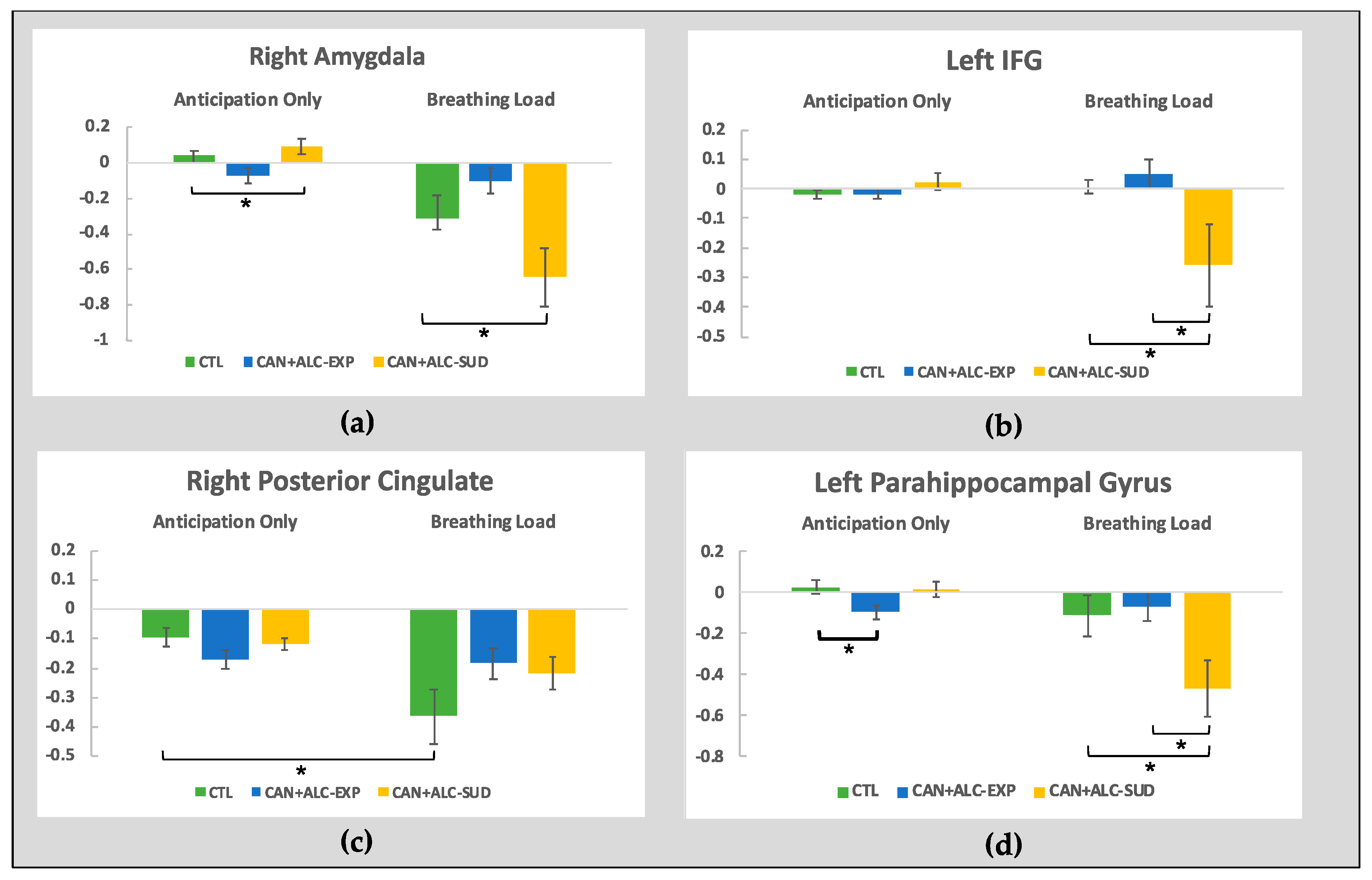
3.2.1. The Group by interoception interaction
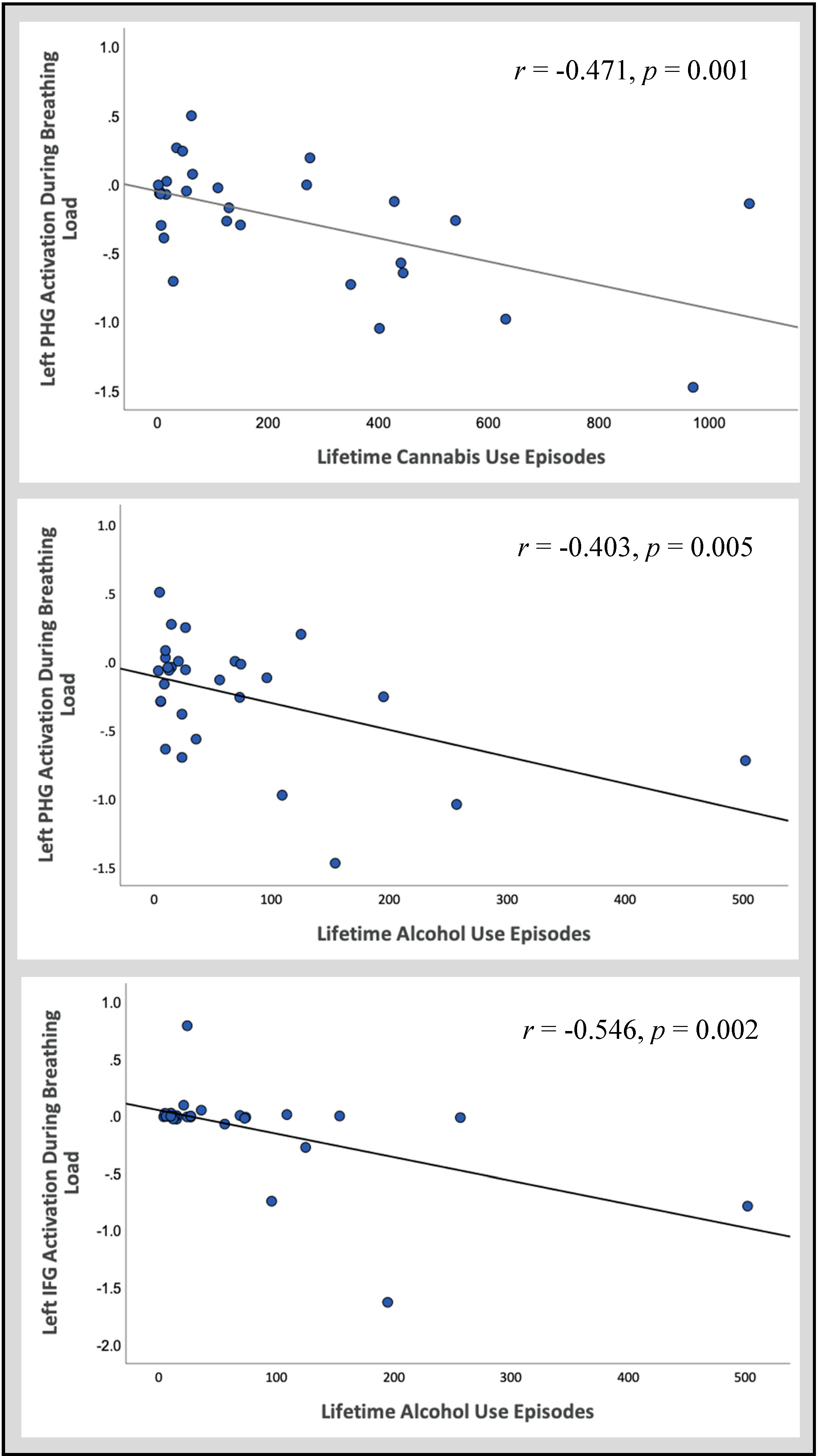
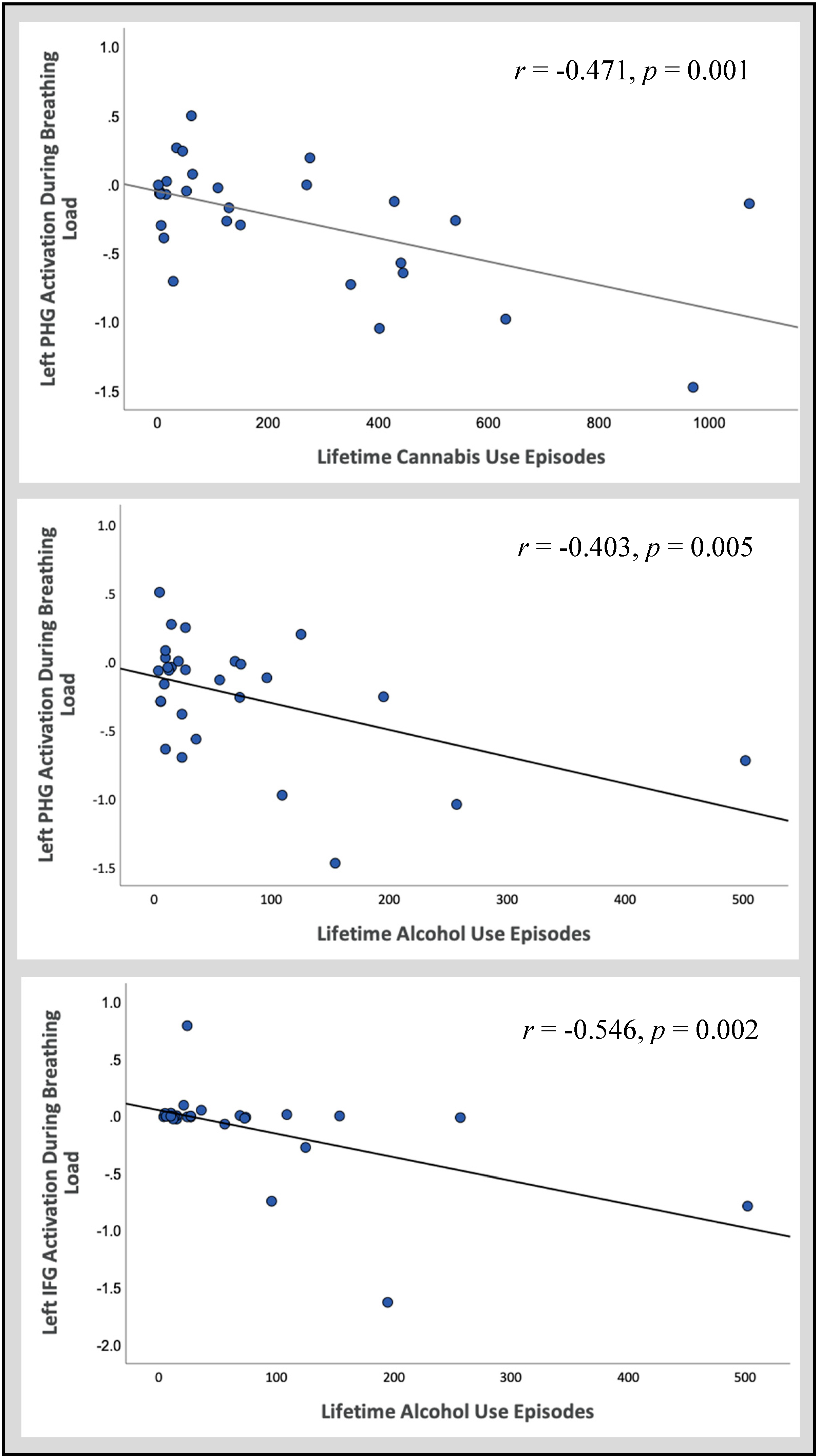
3.2.2. Follow-Up Correlations
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Casey, B.J.; Jones, R.M. Neurobiology of the adolescent brain and behavior: Implications for substance use disorders. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 1189–1201. [Google Scholar] [CrossRef] [PubMed]
- Johnston, L.D.; Miech, R.A.; O’Malley, P.M.; Bachman, J.G.; Schulenberg, J.E.; Patrick, M.E. Monitoring the Future National Survey Results on Drug Use 1975–2019: Overview, Key Findings on Adolescent Drug Use; Education Resources Information Center: Washington, DC, USA, 2020. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2018 National Survey on Drug Use and Health, HHS; HHS Publ. No. PEP19-5068, NSDUH Ser. H-54; Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2019. [CrossRef] [Green Version]
- Hasin, D.S. US Epidemiology of Cannabis Use and Associated Problems. Neuropsychopharmacology 2018, 43, 195–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, B.F.; Dawson, D.A. Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: Results from the national longitudinal alcohol epidemiologic survey. J. Subst. Abuse 1997, 9, 103–110. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings; NSDUH Series H-48; HHS Publication No. (SMA) 14-4863; Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2014.
- London, E.D.; Ernst, M.; Grant, S.; Bonson, K.; Weinstein, A. Orbitofrontal cortex and human drug abuse: Functional imaging. Cereb. Cortex 2000, 10, 334–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, J.L.; Juavinett, A.L.; May, A.C.; Davenport, P.W.; Paulus, M.P. Do you feel alright? Attenuated neural processing of aversive interoceptive stimuli in current stimulant users. Psychophysiology 2015, 52, 249–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bechara, A.; Tranel, D.; Damasio, H. Characterization of the decision-making deficit of patients with ventromedial prefrontal cortex lesions. Brain 2000, 123. [Google Scholar] [CrossRef] [Green Version]
- Nestor, L.J.; Ghahremani, D.G.; Monterosso, J.; London, E.D. Prefrontal hypoactivation during cognitive control in early abstinent methamphetamine-dependent subjects. Psychiatry Res. Neuroimaging 2011, 194. [Google Scholar] [CrossRef] [Green Version]
- Paulus, M.P.; Feinstein, J.S.; Tapert, S.F.; Liu, T.T. Trend detection via temporal difference model predicts inferior prefrontal cortex activation during acquisition of advantageous action selection. Neuroimage 2004. [Google Scholar] [CrossRef]
- Verdejo-Garcia, A.; Chong, T.T.J.; Stout, J.C.; Yücel, M.; London, E.D. Stages of dysfunctional decision-making in addiction. Pharmacol. Biochem. Behav. 2018. [Google Scholar] [CrossRef]
- Sönmez, M.B.; Kahyacı Kılıç, E.; Ateş Çöl, I.; Görgülü, Y.; Köse Çınar, R. Decreased interoceptive awareness in patients with substance use disorders. J. Subst. Use 2017, 22. [Google Scholar] [CrossRef]
- May, A.C.; Stewart, J.L.; Migliorini, R.; Tapert, S.F.; Paulus, M.P. Methamphetamine Dependent Individuals Show Attenuated Brain Response to Pleasant Interoceptive Stimuli. Drug Alcohol Depend. 2013, 131, 238–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, S.H.; Zvolensky, M.J.; Eifert, G.H. Negative-reinforcement drinking motives mediate the relation between anxiety sensitivity and increased drinking behavior. Pers. Individ. Differ. 2001. [Google Scholar] [CrossRef]
- Craig, A.D. How do you feel? Interoception: The sense of the physiological condition of the body. Nat. Rev. Neurosci. 2002. [Google Scholar] [CrossRef] [PubMed]
- Pollatos, O.; Gramann, K.; Schandry, R. Neural systems connecting interoceptive awareness and feelings. Hum. Brain Mapp. 2007. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.D. Interoception: The sense of the physiological condition of the body. Curr. Opin. Neurobiol. 2003, 13, 500–505. [Google Scholar] [CrossRef]
- Barrett, L.F.; Simmons, W.K. Interoceptive predictions in the brain. Nat. Rev. Neurosci. 2015. [Google Scholar] [CrossRef] [Green Version]
- Paulus, M.P.; Tapert, S.F.; Schulteis, G. The role of interoception and alliesthesia in addiction. Pharmacol. Biochem. Behav. 2009. [Google Scholar] [CrossRef] [Green Version]
- Verdejo-Garcia, A.; Clark, L.; Dunn, B.D. The role of interoception in addiction: A critical review. Neurosci. Biobehav. Rev. 2012. [Google Scholar] [CrossRef]
- Naqvi, N.H.; Bechara, A. The Insula: A Critical Neural Substrate for Drug Seeking under Conflict and Risk. Wiley Handb. Cogn. 2015. [Google Scholar] [CrossRef]
- Paulus, M.P.; Stewart, J.L. Interoception and drug addiction. Neuropharmacology 2014, 76, 342–350. [Google Scholar] [CrossRef]
- Critchley, H.D.; Wiens, S.; Rotshtein, P.; Öhman, A.; Dolan, R.J. Neural systems supporting interoceptive awareness. Nat. Neurosci. 2004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etkin, A.; Buechel, C.; Gross, J.J. The neural bases of emotion regulation. Nat. Rev. Neurosci. 2015. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.L.; Flagan, T.M.; May, A.C.; Reske, M.; Simmons, A.N.; Paulus, M.P. Young adults at risk for stimulant dependence show reward dysfunction during reinforcement-based decision making. Biol. Psychiatry 2013, 73, 235–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berk, L.; Stewart, J.L.; May, A.C.; Wiers, R.W.; Davenport, P.W.; Paulus, M.P.; Tapert, S.F. Under pressure: Adolescent substance users show exaggerated neural processing of aversive interoceptive stimuli. Addiction 2015, 110, 2025–2036. [Google Scholar] [CrossRef] [Green Version]
- Stewart, J.L.; Butt, M.; May, A.C.; Tapert, S.F.; Paulus, M.P. Insular and cingulate attenuation during decision making is associated with future transition to stimulant use disorder. Addiction 2017, 112, 1567–1577. [Google Scholar] [CrossRef] [PubMed]
- Verdejo-García, A.; Bechara, A. A somatic marker theory of addiction. Neuropharmacology 2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wills, T.A.; Pokhrel, P.; Morehouse, E.; Fenster, B. Behavioral and Emotional Regulation and Adolescent Substance Use Problems: A Test of Moderation Effects in a Dual-Process Model. Psychol. Addict. Behav. 2011, 25, 279–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payer, D.; Lieberman, M.; London, E. Neural correlates of affect processing and aggression in methamphetamine dependence. Arch. Gen. Psychiatry 2011, 68, 271–282. [Google Scholar] [CrossRef] [Green Version]
- Veinante, P.; Yalcin, I.; Barrot, M. The amygdala between sensation and affect: A role in pain. J. Mol. Psychiatry 2013. [Google Scholar] [CrossRef] [Green Version]
- Morawetz, C.; Bode, S.; Derntl, B.; Heekeren, H.R. The effect of strategies, goals and stimulus material on the neural mechanisms of emotion regulation: A meta-analysis of fMRI studies. Neurosci. Biobehav. Rev. 2017. [Google Scholar] [CrossRef]
- Conrod, P.; Nikolaou, K. Annual Research Review: On the developmental neuropsychology of substance use disorders. J. Child Psychol. Psychiatry Allied Discip. 2016. [Google Scholar] [CrossRef] [PubMed]
- Wolitzky-Taylor, K.; McBeth, J.; Guillot, C.R.; Stone, M.D.; Kirkpatrick, M.G.; Zvolensky, M.J.; Buckner, J.D.; Leventhal, A.M. Transdiagnostic processes linking anxiety symptoms and substance use problems among adolescents. J. Addict. Dis. 2016. [Google Scholar] [CrossRef] [PubMed]
- Karoly, H.C.; Schacht, J.P.; Meredith, L.R.; Jacobus, J.; Tapert, S.F.; Gray, K.M.; Squeglia, L.M. Investigating a novel fMRI cannabis cue reactivity task in youth. Addict. Behav. 2019, 89, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Tapert, S.F.; Cheung, E.H.; Brown, G.G.; Frank, L.R.; Paulus, M.P.; Schweinsburg, A.D.; Meloy, M.J.; Brown, S.A. Neural Response to Alcohol Stimuli in Adolescents with Alcohol Use Disorder. Arch. Gen. Psychiatry 2003, 60, 727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopata, M.; La Fata, J.; Evanich, M.J.; Lourenço, R.V. Effects of flow-resistive loading on mouth occlusion pressure during CO2 rebreathing. Am. Rev. Respir. Dis. 1977. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.L.; Parnass, J.M.; May, A.C.; Davenport, P.W.; Paulus, M.P. Altered frontocingulate activation during aversive interoceptive processing in young adults transitioning to problem stimulant use. Front. Syst. Neurosci. 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, J.L.; May, A.C.; Poppa, T.; Davenport, P.W.; Tapert, S.F.; Paulus, M.P. You are the danger: Attenuated insula response in methamphetamine users during aversive interoceptive decision-making. Drug Alcohol Depend. 2014, 142, 110–119. [Google Scholar] [CrossRef] [Green Version]
- Schacht, J.P.; Anton, R.F.; Myrick, H. Functional neuroimaging studies of alcohol cue reactivity: A quantitative meta-analysis and systematic review. Addict. Biol. 2013. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Zimmermann, K.; Xin, F.; Zhao, W.; Derckx, R.T.; Sassmannshausen, A.; Scheele, D.; Hurlemann, R.; Weber, B.; Kendrick, K.M.; et al. Cue Reactivity in the Ventral Striatum Characterizes Heavy Cannabis Use, Whereas Reactivity in the Dorsal Striatum Mediates Dependent Use. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019. [Google Scholar] [CrossRef]
- Pierucci-Lagha, A.; Gelernter, J.; Feinn, R.; Cubells, J.F.; Pearson, D.; Pollastri, A.; Farrer, L.; Kranzler, H.R. Diagnostic reliability of the semi-structured assessment for drug dependence and alcoholism (SSADDA). Drug Alcohol Depend. 2005. [Google Scholar] [CrossRef]
- Brown, S.A.; Myers, M.G.; Lippke, L.; Tapert, S.F.; Stewart, D.G.; Vik, P.W. Psychometric evaluation of the Customary Drinking and Drug Use Record (CDDR): A measure of adolescent alcohol and drug involvement. J. Stud. Alcohol 1998, 59, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Whiteside, S.P.; Lynam, D.R. The Five Factor Model and impulsivity: Using a structural model of personality to understand impulsivity. Pers. Individ. Differ. 2001, 30, 669–689. [Google Scholar] [CrossRef]
- Mehling, W.E.; Price, C.; Daubenmier, J.J.; Acree, M.; Bartmess, E.; Stewart, A. The Multidimensional Assessment of Interoceptive Awareness (MAIA). PLoS ONE 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pomerleau, O.F.; Fagerström, K.O.; Marks, J.L.; Tate, J.C.; Pomerleau, C.S. Development and validation of a self-rating scale for positive- and negative-reinforcement smoking: The Michigan nicotine reinforcement questionnaire. Nicotine Tob. Res. 2003. [Google Scholar] [CrossRef] [PubMed]
- Paulus, M.P.; Flagan, T.; Simmons, A.N.; Gillis, K.; Kotturi, S.; Thom, N.; Johnson, D.C.; Van Orden, K.F.; Davenport, P.W.; Swain, J.L. Subjecting elite athletes to inspiratory breathing load reveals behavioral and neural signatures of optimal performers in extreme environments. PLoS ONE 2012, 7, e29394. [Google Scholar] [CrossRef]
- Davenport, P.W.; Vovk, A. Cortical and subcortical central neural pathways in respiratory sensations. Respir. Physiol. Neurobiol. 2009. [Google Scholar] [CrossRef]
- Cox, R.W. AFNI: Software for analysis and visualization of functional magnetic resonance neuroimages. Comput. Biomed. Res. 1996. [Google Scholar] [CrossRef]
- Eklund, A.; Nichols, T.E.; Knutsson, H. Cluster failure: Why fMRI inferences for spatial extent have inflated false-positive rates. Proc. Natl. Acad. Sci. USA 2016. [Google Scholar] [CrossRef] [Green Version]
- Luijten, M.; Schellekens, A.F.; Kühn, S.; Machielse, M.W.J.; Sescousse, G. Disruption of Reward Processing in Addiction. JAMA Psychiatry 2017. [Google Scholar] [CrossRef]
- Dager, A.D.; Anderson, B.M.; Rosen, R.; Khadka, S.; Sawyer, B.; Jiantonio-Kelly, R.E.; Austad, C.S.; Raskin, S.A.; Tennen, H.; Wood, R.M.; et al. Functional magnetic resonance imaging (fMRI) response to alcohol pictures predicts subsequent transition to heavy drinking in college students. Addiction 2014. [Google Scholar] [CrossRef]
- Somerville, L.H.; Jones, R.M.; Casey, B.J. A time of change: Behavioral and neural correlates of adolescent sensitivity to appetitive and aversive environmental cues. Brain Cogn. 2010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado, M.R.; Locke, H.M.; Stenger, V.A.; Fiez, J.A. Dorsal striatum responses to reward and punishment: Effects of valence and magnitude manipulations. Cogn. Affect. Behav. Neurosci. 2003, 3, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Ernst, M.; Nelson, E.E.; Jazbec, S.; McClure, E.B.; Monk, C.S.; Leibenluft, E.; Blair, J.; Pine, D.S. Amygdala and nucleus accumbens in responses to receipt and omission of gains in adults and adolescents. Neuroimage 2005, 25, 1279–1291. [Google Scholar] [CrossRef] [PubMed]
- Elliott, R.; Newman, J.L.; Longe, O.A.; Deakin, J.F.W. Differential response patterns in the striatum and orbitofrontal cortex to financial reward in humans: A parametric functional magnetic resonance imaging study. J. Neurosci. 2003, 23, 303–307. [Google Scholar] [CrossRef]
- Seymour, B.; Daw, N.; Dayan, P.; Singer, T.; Dolan, R. Differential Encoding of Losses and Gains in the Human Striatum. J. Neurosci. 2007, 27, 4826–4831. [Google Scholar] [CrossRef] [Green Version]
- Hardin, M.G.; Ernst, M. Functional brain imaging of development-related risk and vulnerability for substance use in adolescents. Annu. Rev. Clin. Psychol. 2016, 11, 361–377. [Google Scholar] [CrossRef]
- May, A.C.; Stewart, J.L.; Tapert, S.F.; Paulus, M.P. The effect of age on neural processing of pleasant soft touch stimuli. Front. Behav. Neurosci. 2014, 8, 52. [Google Scholar] [CrossRef] [Green Version]
- Aguinaldo, L.D.; Squeglia, L.M.; Gray, K.M.; Coronado, C.; Lees, B.; Tomko, R.L.; Jacobus, J. Behavioral Treatments for Adolescent Cannabis Use Disorder: A Rationale for Cognitive Retraining. Curr. Addict. Rep. 2019. [Google Scholar] [CrossRef]
- Fatseas, M.; Serre, F.; Alexandre, J.M.; Debrabant, R.; Auriacombe, M.; Swendsen, J. Craving and substance use among patients with alcohol, tobacco, cannabis or heroin addiction: A comparison of substance- and person-specific cues. Addiction 2015. [Google Scholar] [CrossRef]
- Karoly, H.C.; Schacht, J.P.; Jacobus, J.; Meredith, L.R.; Taylor, C.T.; Tapert, S.F.; Gray, K.M.; Squeglia, L.M. Preliminary evidence that computerized approach avoidance training is not associated with changes in fMRI cannabis cue reactivity in non-treatment-seeking adolescent cannabis users. Drug Alcohol Depend. 2019. [Google Scholar] [CrossRef]
- Filbey, F.M.; Claus, E.; Audette, A.R.; Niculescu, M.; Banich, M.T.; Tanabe, J.; Du, Y.P.; Hutchison, K.E. Exposure to the taste of alcohol elicits activation of the mesocorticolimbic neurocircuitry. Neuropsychopharmacology 2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strang, N.M.; Claus, E.D.; Ramchandani, V.A.; Graff-Guerrero, A.; Boileau, I.; Hendershot, C.S. Dose-dependent effects of intravenous alcohol administration on cerebral blood flow in young adults. Psychopharmacology 2015. [Google Scholar] [CrossRef] [PubMed]
- Bjork, J.M.; Smith, A.R.; Hommer, D.W. Striatal sensitivity to reward deliveries and omissions in substance dependent patients. Neuroimage 2008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gowin, J.L.; Stewart, J.L.; May, A.C.; Ball, T.M.; Wittmann, M.; Tapert, S.F.; Paulus, M.P. Altered cingulate and insular cortex activation during risk-taking in methamphetamine dependence: Losses lose impact. Addiction 2014, 109, 237–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, W.A.; Chmelka, M.B.; Howard, B.K.; Thompson, R.W. Comorbid alcohol and cannabis use disorders among high-risk youth at intake into residential care. J. Adolesc. Health 2013. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| CAN+ALC-SUDGroup Description | % Meeting Diagnostic Criteria | Diagnostic Criteria Endorsed | |||||
| M(SD) | Min | Max | |||||
| THC Use Disorder | 92.31 | 3.42 (1.38) | 2 | 6 | |||
| Alcohol Use Disorder | 61.54 | 2.63 (.74) | 2 | 4 | |||
| Substance Use | CAN+ALC-SUD Cannabis/Alcohol Substance Use Disorder | CAN+ALC-EXP Cannabis/Alcohol Experimenter | CTL Little to No Substance Use | df | t | p | |
| Lifetime Cannabis Use | 467.85 (288.05) | 39.38 (45.15) | 0.17 (0.514) | 12.48 | −5.31 | <0.001 | |
| Days Since Last THC Use | 18.69 (33.34) | 71.69 (82.25) | 46.11 (160.19) | 20.63 | 2.35 | 0.029 | |
| Lifetime Alcohol Use | 131.92 (131.55) | 17.44 (15.87) | 0.22 (0.73) | 12.28 | −3.12 | 0.009 | |
| Days Since Last Alcohol | 16.46 (11.67) | 45.38 (98.99) | 22.22 (66.12) | 27 | 1.04 | 0.306 | |
| Lifetime Alcohol Binge Episode | 92.83 (71.90) | 7.87 (7.97) | 0.11 (0.47) | 11.22 | −4.07 | 0.002 | |
| Days Since Last Binge | 24.70 (24.83) | 90.93 (135. 77) | 240 (--) | 15.38 | 1.84 | 0.085 | |
| Lifetime Hallucinogen Use | 2.69 (3.88) | 0.13 (0.50) | -- | 12.32 | −2.37 | 0.035 | |
| Days Since Last Hallucinogen | 82.31 (93.58) | 9.81 (39.25) | -- | 15.42 | −2.61 | 0.019 | |
| Lifetime Sedative Use | 0.77 (1.36) | -- | -- | 12.00 | −2.03 | 0.065 | |
| Days Since Last Sedative Use | 179.15 (330.97) | -- | -- | 12.00 | −1.95 | 0.075 | |
| Lifetime Amphetamine Use | 0.31 (1.11) | -- | -- | 12.00 | −1.00 | 0.337 | |
| Days Since Last Amphetamine Use | 14.46 (52.14) | -- | -- | 12 | −1.00 | 0.337 | |
| Lifetime Rx Stimulant Use | 1.92 (5.48) | 0.06 (0.25) | -- | 12.04 | −1.22 | 0.245 | |
| Days Since Last Rx Stimulant Use | 148.23 (297.47) | 17.94 (71.75) | -- | 13.14 | −1.54 | 0.147 | |
| Lifetime Cocaine Use | 0.92 (1.50) | -- | -- | 12.00 | −2.22 | 0.046 | |
| Days Since Last Cocaine Use | 55.00 (91.33) | -- | -- | 12.00 | −2.17 | 0.051 | |
| Lifetime Ecstasy Use | 14.85 (27.65) | -- | -- | 12.00 | −1.94 | 0.077 | |
| Days Since Last Ecstasy Use | 293.62 (333.72) | -- | -- | 12.00 | −3.17 | 0.008 | |
| Lifetime Opiate Use | 0.92 (2.75) | 1.94 (7.49) | -- | 27 | 0.462 | 0.647 | |
| Days Since Last Opiate Use | 139.31 (277.92) | 26.56 (73.13) | -- | 13.35 | −1.42 | 0.178 | |
| Lifetime Inhalant Use | 2.38 (8.30) | -- | -- | 12.00 | −1.04 | 0.321 | |
| Days Since Last Inhalant Use | 106.00 (259.42) | -- | -- | 12.00 | −1.47 | 0.166 | |
| Lifetime Nicotine Use | 232.00 (409.19) | 4.19 (6.73) | 0.56 (2.36) | 12.00 | −2.01 | 0.068 | |
| Days Since Last Nicotine Use | 92.69 (108.66) | 130.69 (157.63) | 21.94 (93.10) | 26.39 | 0.766 | 0.451 | |
| CAN+ALC-SUD Cannabis/Alcohol Substance Use Disorder | CAN+ALC-EXP Cannabis/Alcohol Experimenter | CTL Little to No Substance Use | ||||
|---|---|---|---|---|---|---|
| Demographics | M(SD) | M(SD) | M(SD) | df | F | p |
| Age (in years) | 16.62 (0.51) | 16.69 (0.70) | 16.33 (0.77) | 2,44 | 1.27 | 0.290 |
| Education (in years) | 10.46 (0.78) | 10.47 (0.83) | 10.11 (0.90) | 2,43 | 0.956 | 0.392 |
| WRAT 4 Verbal IQ | 107.31 (14.29) | 106.75 (12.37) | 112.00 (13.82) | 2,44 | 0.770 | 0.469 |
| VAS Ratings | M(SD) | M(SD) | M(SD) | df | F | p |
| Unpleasant | 5.69 (3.29) | 4.63 (2.64) | 5.34 (3.49) | 2,44 | 0.432 | 0.652 |
| Intensity | 4.08 (3.47) | 2.13 (2.77) | 4.41 (2.89) | 2,44 | 2.68 | 0.08 |
| Questionnaires | M(SD) | M(SD) | M(SD) | df | F/t | p |
| MAIA | ||||||
| Noticing | 2.83 (1.52) | 2.75 (1.03) | 2.78 (1.19) | 2,43 | 0.016 | 0.984 |
| Not Distracting | 2.14 (0.50) | 2.37 (1.12) | 2.52 (1.30) | 2,43 | 0.443 | 0.645 |
| Not Worrying | 2.89 (1.43) | 2.81 (1.42) | 2.70 (1.05) | 2,43 | 0.079 | 0.925 |
| Attention Regulation | 3.17 (.95) | 3.45 (0.74) | 3.14 (1.15) | 2,43 | 0.494 | 0.613 |
| Emotional Awareness | 3.18 (1.43) | 3.04 (1.31) | 3.07 (.93) | 2,43 | 0.054 | 0.948 |
| Self-Regulation | 3.10 (1.05) | 3.23 (0.90) | 3.01 (1.05) | 2,43 | 0.207 | 0.814 |
| Body Listening | 1.36 (1.16) | 1.96 (1.44) | 1.79 (1.05) | 2,43 | 0.844 | 0.437 |
| Trusting | 3.47 (1.40) | 3.73 (1.08) | 3.72 (0.92) | 2,43 | 0.231 | 0.795 |
| UPPS | ||||||
| Lack of Premeditation | 2.08 (0.39) | 2.18 (0.49) | 1.89 (0.42) | 2,44 | 1.92 | 0.159 |
| Urgency | 2.30 (0.66) | 2.17 (0.59) | 2.06 (0.51) | 2,44 | 0.672 | 0.516 |
| Sensation Seeking | 3.18 (0.29) | 3.09 (0.48) | 3.03 (0.44) | 2,44 | 0.528 | 0.594 |
| Lack of Perseverance | 2.03 (0.59) | 2.13 (0.58) | 1.83 (0.34) | 2,44 | 1.53 | 0.229 |
| MNRQ | ||||||
| Negative Reinforcement | 2.85 (2.38) | 0.875 (1.63) | -- | 20.52 | 2.55 | 0.019 |
| Positive Reinforcement | 11.38 (2.53) | 7.25 (3.45) | -- | 27 | 3.59 | 0.001 |
| GROUP BY INTEROCEPTIVE CONDITION INTERACTION | |||||||||
| R/L | Voxels | Volume | X | Y | Z | BA | Anticipation | Load | |
| Amygdala | R | 33 | 2112 | 28 | −9 | −30 | 28 | SUD > EXP | EXP > SUD |
| Inferior Frontal Gyrus | L | 28 | 1792 | −13 | 24 | −20 | 11 | -- | EXP = CTL > SUD |
| Posterior Cingulate | R | 25 | 1600 | 13 | −65 | 16 | 31 | -- | EXP = SUD > CTL |
| Parahippocampal Gyrus | L | 21 | 1344 | −24 | −7 | −19 | 35 | CTL > EXP | CTL = EXP > SUD |
| MAIN EFFECT OF INTEROCEPTIVE CONDITION | |||||||||
| R/L | Voxels | Volume | X | Y | Z | BA | Condition Effect | ||
| Cingulate Gyrus | R | 3141 | 201024 | 8 | −6 | 23 | 24 | Load > Anticipation | |
| Fusiform Gyrus | R | 663 | 42432 | 40 | −12 | −24 | 20 | Anticipation > Load | |
| Superior Frontal Gyrus | R | 334 | 21376 | 1 | 4 | 57 | 6 | Load > Anticipation | |
| Cingulate Gyrus | L | 131 | 8384 | −2 | −25 | 37 | 31 | Load > Anticipation | |
| Cuneus | R | 112 | 7168 | 18 | −85 | 28 | 18 | Load > Anticipation | |
| Thalamus | R | 64 | 4096 | 6 | −18 | 4 | Load > Anticipation | ||
| Declive | L | 61 | 3904 | −15 | −63 | −20 | Load > Anticipation | ||
| Middle Frontal Gyrus | L | 48 | 3072 | −36 | 37 | 28 | 9 | Anticipation > Load | |
| Middle Occipital Gyrus | R | 43 | 2752 | 34 | −83 | 9 | 19 | Load > Anticipation | |
| Anterior Cingulate | L | 39 | 2496 | −6 | 31 | 15 | 24 | Load > Anticipation | |
| Precuneus | R | 36 | 2304 | 5 | −43 | 43 | 7 | Load > Anticipation | |
| Precentral Gyrus | R | 29 | 1856 | 18 | −26 | 64 | 4 | Load > Anticipation | |
| Precentral Gyrus | L | 24 | 1536 | −18 | −29 | 63 | 4 | Anticipation > Load | |
| MAIN EFFECT OF CUE STIMULUS TYPE | |||||||||
| R/L | Voxels | Volume | X | Y | Z | BA | Stimulus Effect | ||
| Medial Frontal Gyrus | R | 43 | 2752 | 1 | 44 | 30 | 9 | Substance > Comparison | |
| Anterior Cingulate | L | 23 | 1472 | −1 | 46 | 8 | 32 | Substance > Comparison | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
May, A.C.; Jacobus, J.; Stewart, J.L.; Simmons, A.N.; Paulus, M.P.; Tapert, S.F. Do Adolescents Use Substances to Relieve Uncomfortable Sensations? A Preliminary Examination of Negative Reinforcement among Adolescent Cannabis and Alcohol Users. Brain Sci. 2020, 10, 214. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10040214
May AC, Jacobus J, Stewart JL, Simmons AN, Paulus MP, Tapert SF. Do Adolescents Use Substances to Relieve Uncomfortable Sensations? A Preliminary Examination of Negative Reinforcement among Adolescent Cannabis and Alcohol Users. Brain Sciences. 2020; 10(4):214. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10040214
Chicago/Turabian StyleMay, April C., Joanna Jacobus, Jennifer L. Stewart, Alan N. Simmons, Martin P. Paulus, and Susan F. Tapert. 2020. "Do Adolescents Use Substances to Relieve Uncomfortable Sensations? A Preliminary Examination of Negative Reinforcement among Adolescent Cannabis and Alcohol Users" Brain Sciences 10, no. 4: 214. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10040214