The Clinical Application of EEG-Signals Recurrence Analysis as a Measure of Functional Connectivity: Comparative Case Study of Patients with Various Neuropsychiatric Disorders



Abstract
:1. Introduction
2. Materials and Methods
2.1. Cases
2.2. EEG Data Recording
2.3. EEG Recurrence Analysis
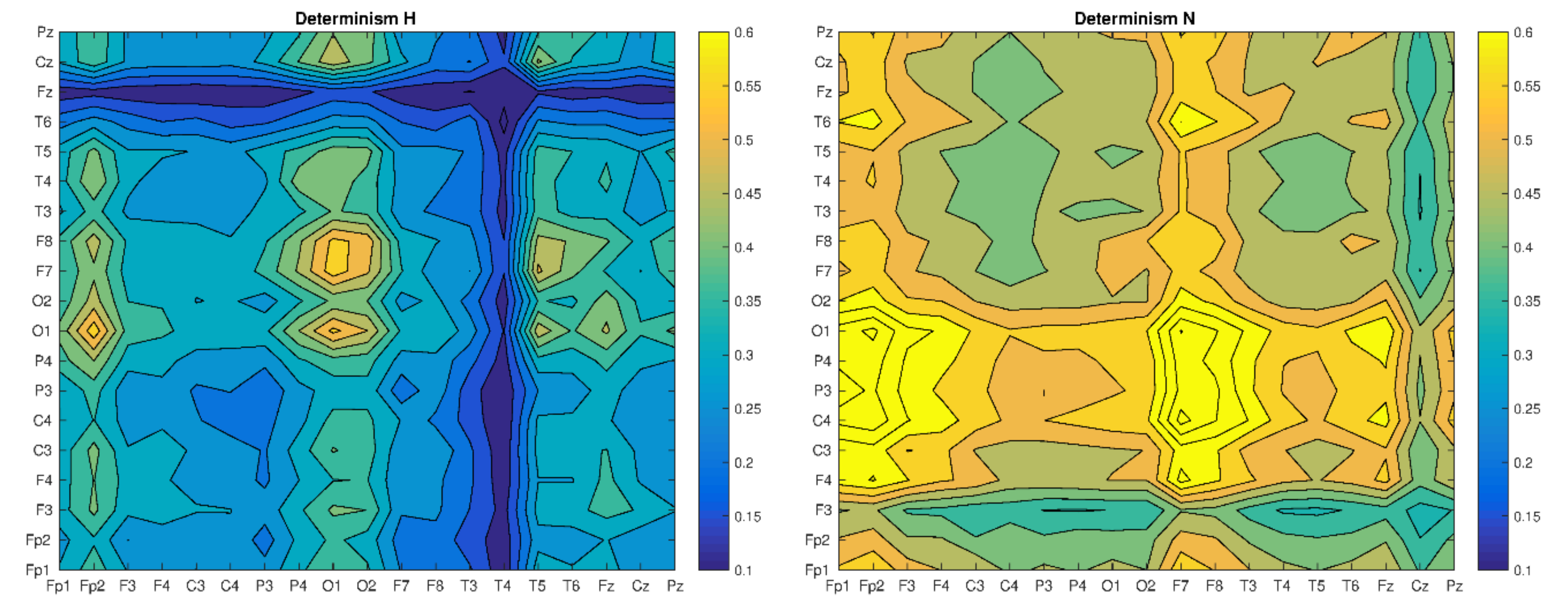
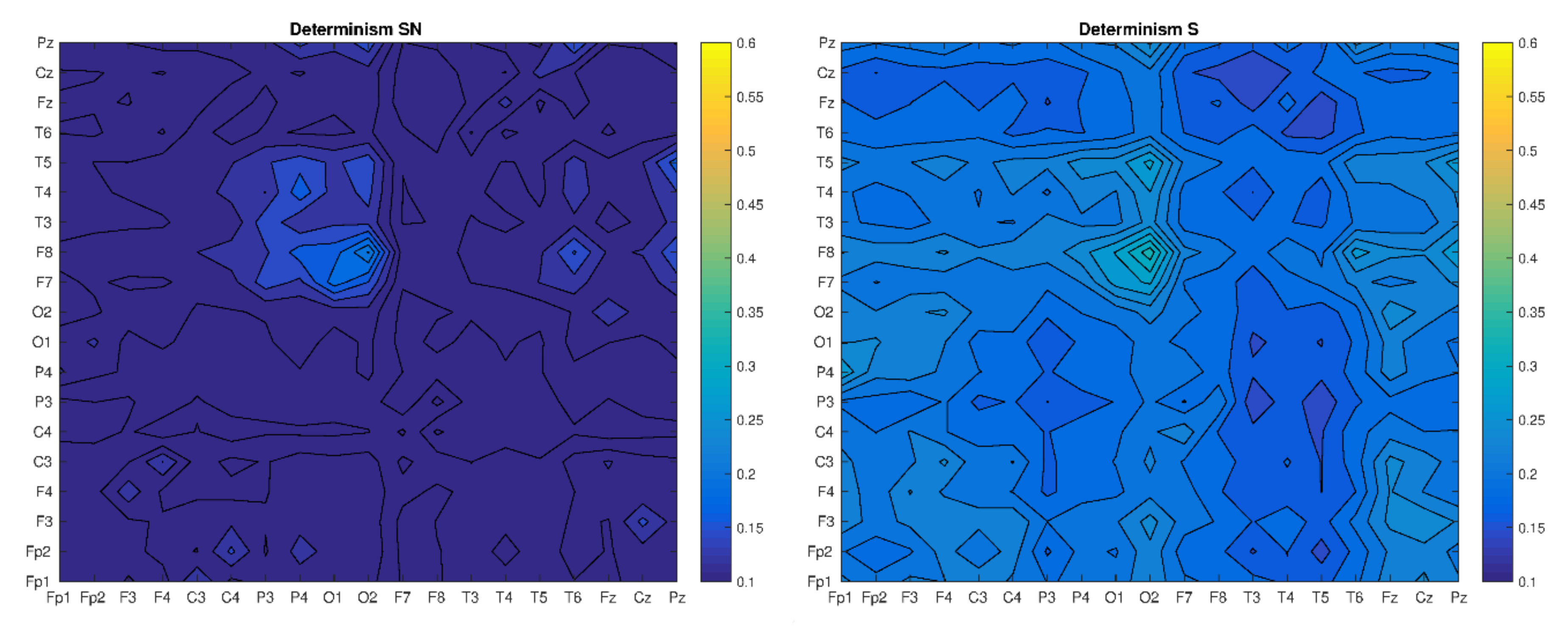
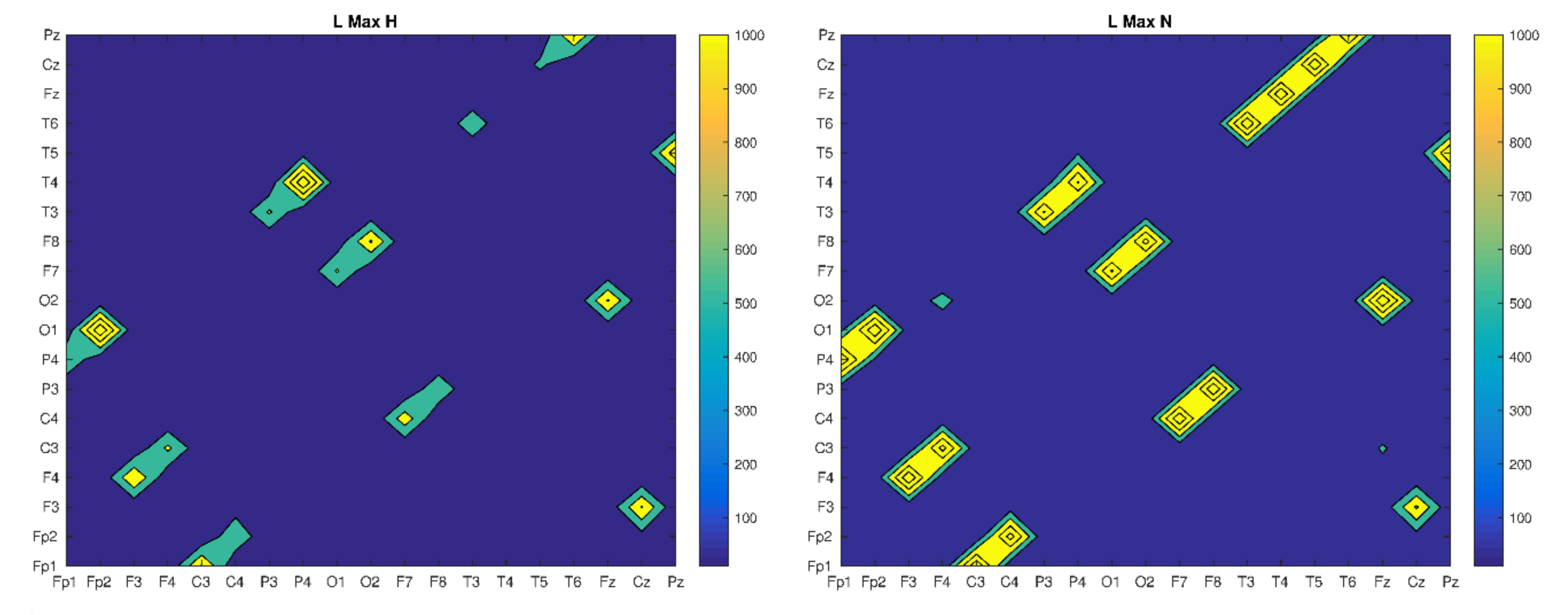
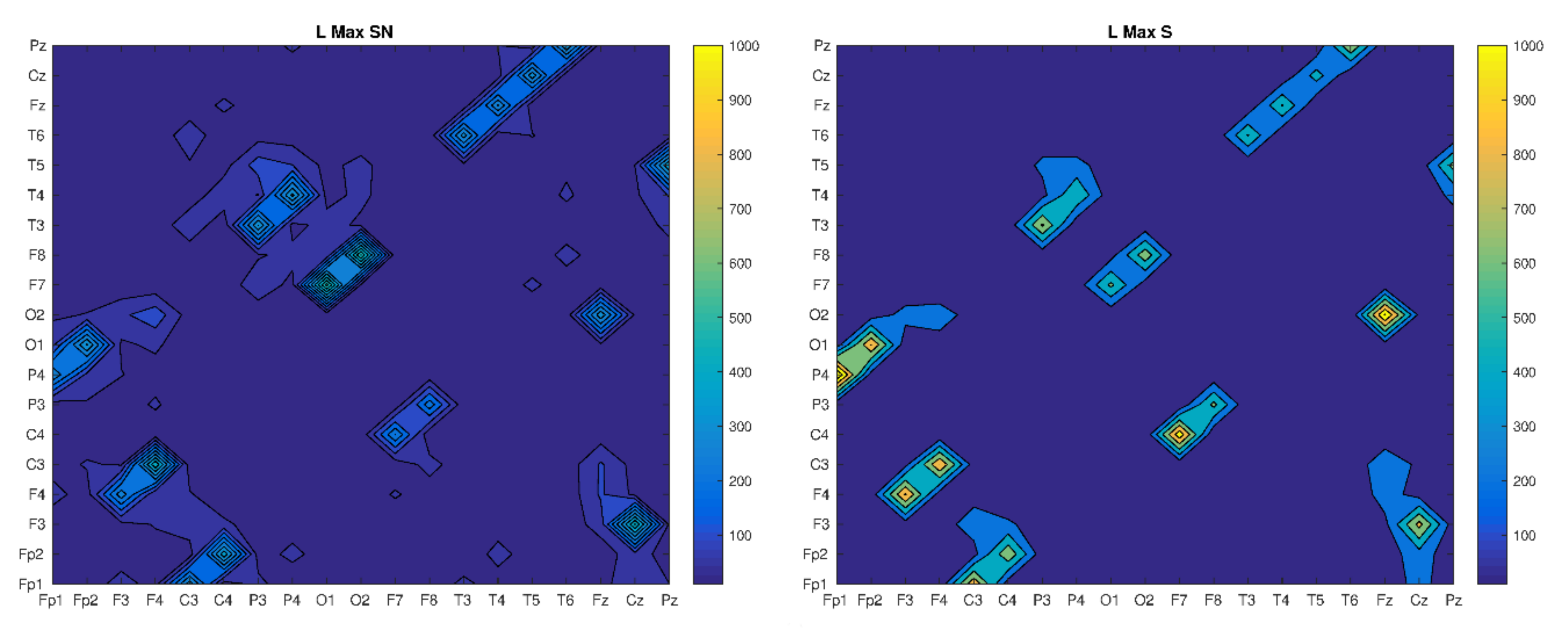
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Andreasen, N.C.; Nopoulos, P.; O’Leary, D.S.; Miller, D.D.; Wassink, T.; Flaum, M. Defining the phenotype of schizophrenia: Cognitive dysmetria and its neural mechanisms. Biol. Psychiatry 1999, 46, 908–920. [Google Scholar] [CrossRef]
- Friston, K.J. The disconnection hypothesis. Schizophr. Res. 1998, 30, 115–125. [Google Scholar] [CrossRef]
- Krukow, P.; Jonak, K.; Karakuła-Juchnowicz, H.; Podkowiński, A.; Jonak, K.; Borys, M.; Harciarek, M. Disrupted functional connectivity within the left prefrontal cortex and sensorimotor areas predicts impaired cognitive speed in patients with first-episode schizophrenia. Psychiatry Res. Neuroimaging 2018, 17, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Kubicki, M.; McCarley, R.; Westin, C.-F.; Park, H.-J.; Maier, S.; Kikinis, R. A review of diffusion tensor imaging studies in schizophrenia. Schizophr. Res. 2007, 41, 15–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubl, D.; Koenig, T.; Strik, W.; Federspiel, A.; Kreis, R.; Boesch, C. Pathways that make voices: White matter changes in auditory hallucinations. Arch. Gen. Psychiatry 2004, 61, 658–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krukow, P.; Jonak, K.; Morylowska-Topolska, J.; Karakuła-Juchnowicz, H. Specific neuropsychological and neurophysiological dysfunctions of a patients with first-episode schizophrenia and comorbid white matter damage. Acta Neuropsychol. 2007, 15, 201–219. [Google Scholar]
- Baleja-Stawicka, I.; Kwiecińska, E.; Kłoszewska, I.A.Ł. Metachromatic leucodystrophy as a cause of dementia and organic delusional syndrome in young adults -a case report. Adv. Psychiatry Neurol. 2008, 17, 237–241. [Google Scholar]
- Lai, C.-Y.; Scarr, S.; Udawela, M.; Everall, I.; Chen, W.J.; Dean, B. Biomarkers in schizophrenia: A focus on blood based diagnostics and theranostics. Word J. Psychiatry 2016, 6, 102–117. [Google Scholar] [CrossRef]
- Singer, W. Neuronal synchrony: A versatile code for the definition of relations? Neuron 1999, 24, 49–65. [Google Scholar] [CrossRef] [Green Version]
- Uhlhass, P.J.; Singer, W. Abnormal neural oscillations and synchrony in schizophrenia. Nat. Rev. Neurosci. 2010, 11, 100–113. [Google Scholar] [CrossRef]
- Jonak, K.; Krukow, P.; Karakuła-Juchnowicz, H. Hypercoherence and increased energy of gamma oscillations in patient with first onset of schizophrenia and cerebral white matter damage. Curr. Probl. Psychiatry 2016, 17, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Sakkalis, V. Review of advanced techniques for the estimation of brain connectivity measured with EEG/MEG. Comput. Biol. Med. 2011, 41, 1110–1117. [Google Scholar] [CrossRef] [PubMed]
- Litak, G.; Syta, A.; Gajewski, J.; Jonak, J. Detecting and identifying non-stationary courses in the ripping head power consumption by recurrence plots. Meccanica 2010, 45, 603–608. [Google Scholar] [CrossRef]
- Syta, A.; Jonak, J.; Jedliski, U.; Litak, G. Failure diagnosis of a gear box by recurrences. J. Vib. Acoust. Trans. ASME 2012, 134, 041006. [Google Scholar] [CrossRef]
- Acharya, U.R.; Faust, O.; Kannathal, N.; Chua, T.; Laxminarayan, S. Non-linear analysis of EEG signals at various sleep stages. Comput. Methods Programs Biomed. 2005, 80, 37–45. [Google Scholar] [CrossRef]
- Rangaprakash, D.; Pradhan, N. Study of phase synchronization in multichannel seizure EEG using nonlinear recurrence measure. Biomed. Signal Process. Control 2014, 11, 114–122. [Google Scholar] [CrossRef]
- Acharya, U.R.; Vinitha Sree, S.; Swapna, G.; Martis, R.J.; Suri, J.S. Automated EEG analysis of epilepsy: A review. Knowl. Based Syst. 2013, 45, 147–165. [Google Scholar] [CrossRef]
- Ngamga, E.J.; Bialonski, S.; Marwan, N.; Kurths, J.; Geier, C.; Lehnertz, K. Evaluation of selected recurrence measures in discriminating pre-ictal and inter-ictal periods from epileptic EEG data. Phys. Lett. Sect. A Gen. At. Solid State Phys. 2016, 380, 1419–1425. [Google Scholar] [CrossRef] [Green Version]
- Stam, C.J. Nonlinear dynamical analysis of EEG and MEG: Review of an emerging field. Clin. Neurophysiol. 2005, 116, 2266–2301. [Google Scholar] [CrossRef]
- Lombardi, A.; Guccione, P.; Mascolo, L.; Taurisano, P.; Fazio, L.; Nico, G. Combining Graph Analysis and Recurrence Plot on fMRI data. In Proceedings of the 2015 IEEE International Symposium on Medical Measurements and Applications (MeMeA) Proceedings, Turin, Italy, 7–9 May 2015. [Google Scholar]
- Millan, M.J.; Fone, K.; Steckler, T.; Horan, W.P. Negative symptoms of schizophrenia: Clinical characteristics, pathophysiological substrates, experimental models and prospects of improved treatment. Eur. Neuropsychopharmacol. 2014, 24, 645–692. [Google Scholar] [CrossRef] [Green Version]
- Eckmann, J.-P.; Kamphorst, S.O.; Ruelle, D. Recurrence Plots of Dynamical Systems. Europhys. Lett. 1987, 4, 973–977. [Google Scholar] [CrossRef] [Green Version]
- Takens, F. Detecting Strange Attractors in Turbulence. Lecture Notes in Mathematics Dynamical Systems and Turbulence, Warwick; Springer: Berlin/Heidelberg, Germany, 1980; pp. 366–381. [Google Scholar]
- Fraser, A.M.; Swinney, H.L. Independent coordinates for strange attractors from mutual information. Phys. Rev. A 1986, 33, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Kennel, M.B.; Abarbanel, H.D.I. False neighbors and false strands: A reliable minimum embedding dimension algorithm. Phys. Rev. E 2002, 66, 026209. [Google Scholar] [CrossRef] [PubMed]
- Webber, C.L.; Marwan, N. Recurrence Quantification Analysis–Theory and Best Practices; Springer: Cham/Heidelberg, Germany; New York, NY, USA; Dordrecht, The Netherlands; London, UK, 2005. [Google Scholar]
- Marwan, N.; Carmenromano, M.; Thiel, M.; Kurths, J. Recurrence plots for the analysis of complex systems. Phys. Rep. 2007, 438, 237–329. [Google Scholar] [CrossRef]
- Marwan, N.; Donges, J.F.; Zou, Y.; Donner, R.V.; Kurths, J. Complex network approach for recurrence analysis of time series. Phys. Lett. Sect. A Gen. At. Solid State Phys. 2009, 373, 4246–4254. [Google Scholar] [CrossRef] [Green Version]
- Webber, C.L.; Zbilut, J.P. Assessing Deterministic Structures in Physiological Systems Using Recurrence Plot Strategies. Bioeng. Approaches Pulm. Physiol. Med. 1994, 137–148. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
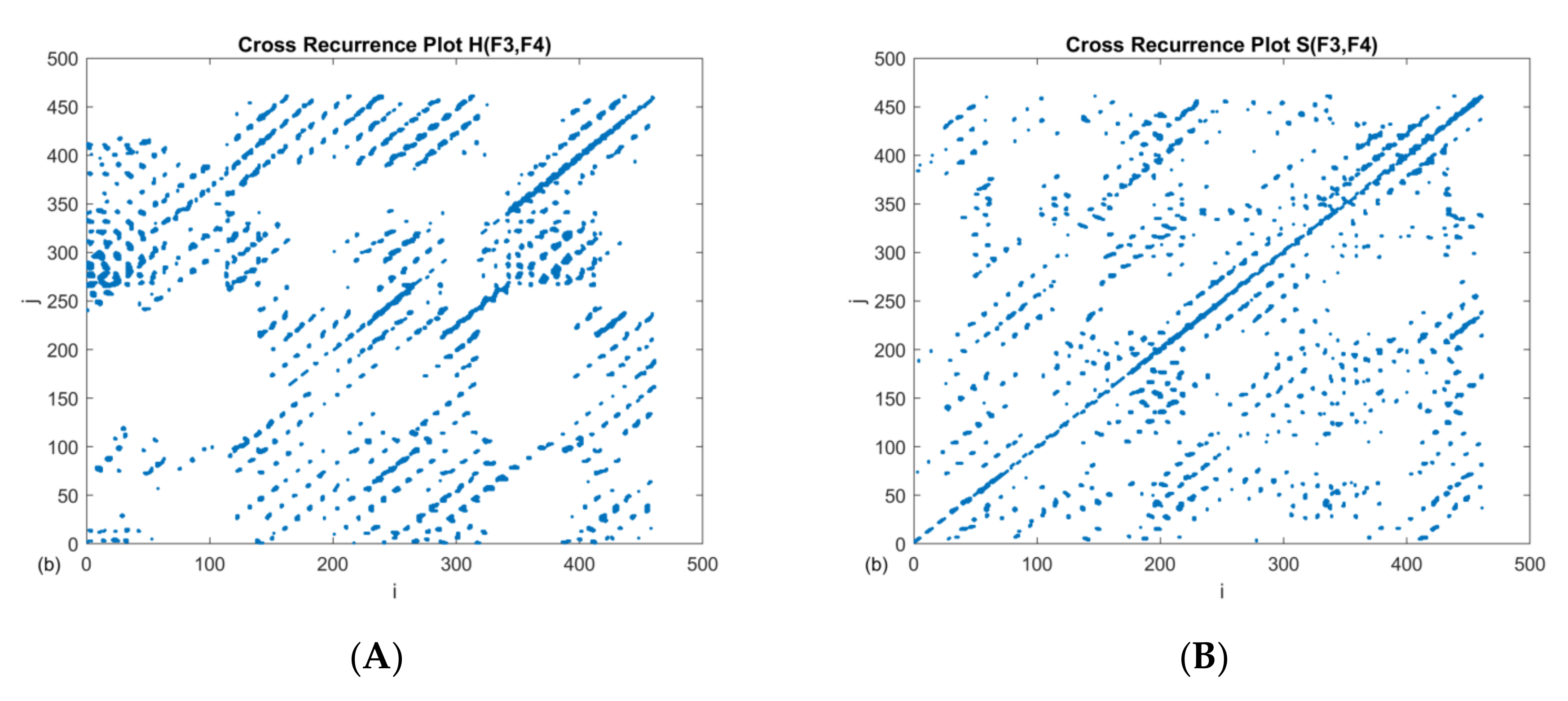
| RR | DET | L | LMAX | |
|---|---|---|---|---|
| H(F3–F4) | 0.035 | 0.44 | 6.5 | 111 |
| S(F3–F4) | 0.025 | 0.25 | 6.2 | 47 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jonak, K.; Syta, A.; Karakuła-Juchnowicz, H.; Krukow, P. The Clinical Application of EEG-Signals Recurrence Analysis as a Measure of Functional Connectivity: Comparative Case Study of Patients with Various Neuropsychiatric Disorders. Brain Sci. 2020, 10, 380. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10060380
Jonak K, Syta A, Karakuła-Juchnowicz H, Krukow P. The Clinical Application of EEG-Signals Recurrence Analysis as a Measure of Functional Connectivity: Comparative Case Study of Patients with Various Neuropsychiatric Disorders. Brain Sciences. 2020; 10(6):380. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10060380
Chicago/Turabian StyleJonak, Kamil, Arkadiusz Syta, Hanna Karakuła-Juchnowicz, and Paweł Krukow. 2020. "The Clinical Application of EEG-Signals Recurrence Analysis as a Measure of Functional Connectivity: Comparative Case Study of Patients with Various Neuropsychiatric Disorders" Brain Sciences 10, no. 6: 380. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10060380