Pathological Findings in Chronic Inflammatory Demyelinating Polyradiculoneuropathy: A Single-Center Experience

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Nerve Biopsy
2.3. Statistical Analysis
2.4. Ethics
3. Results
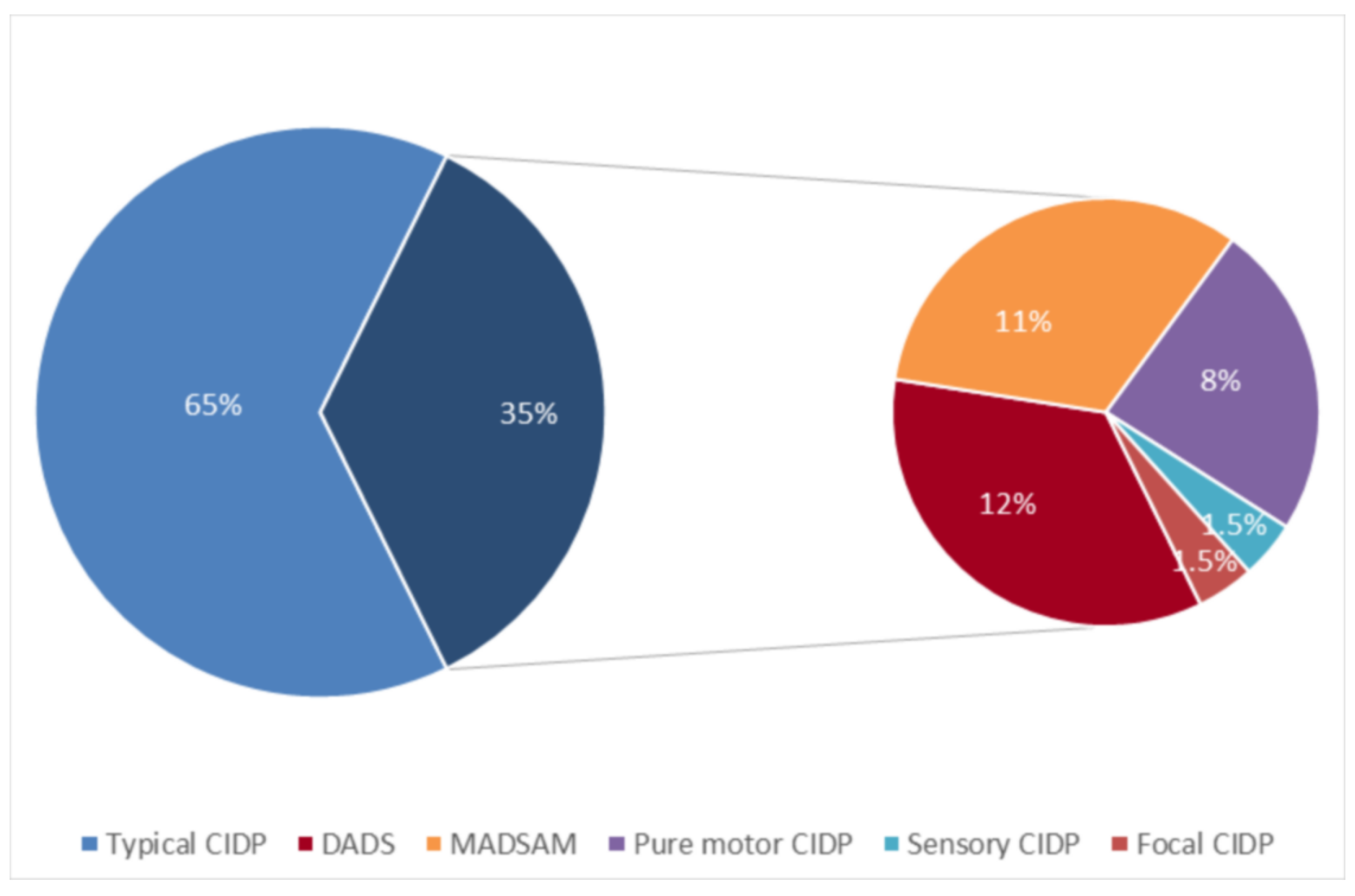
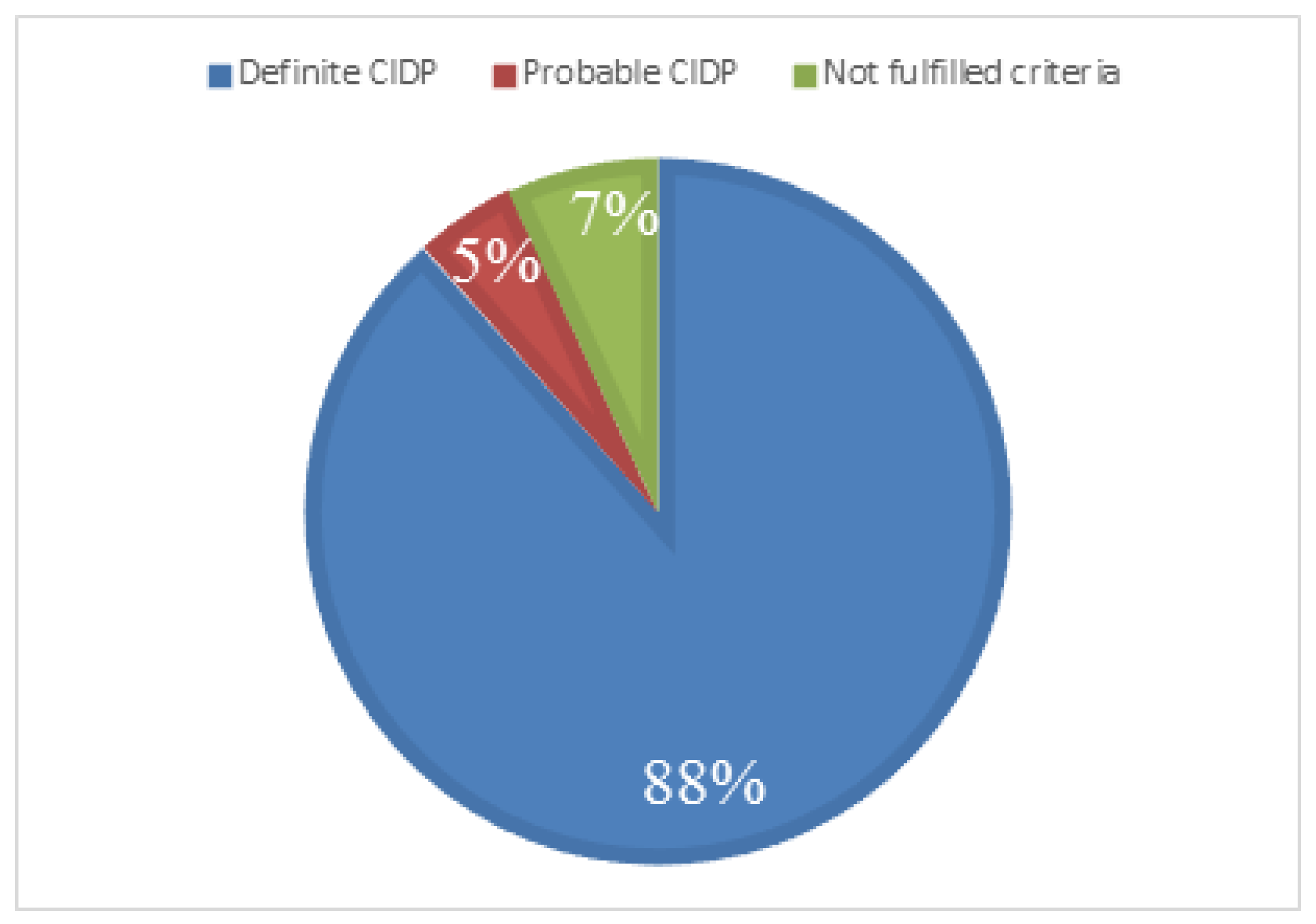
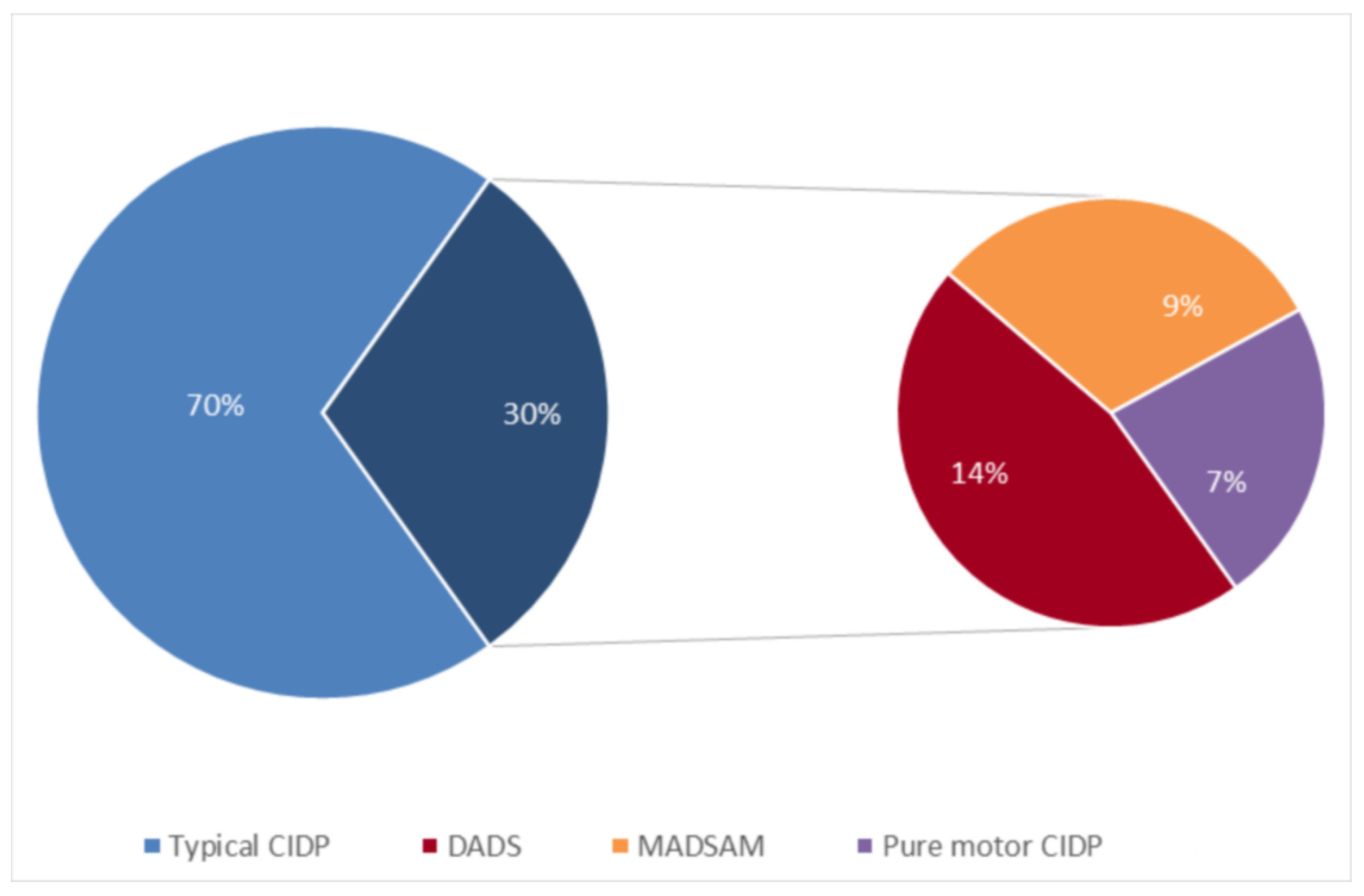
3.1. Clinical Results
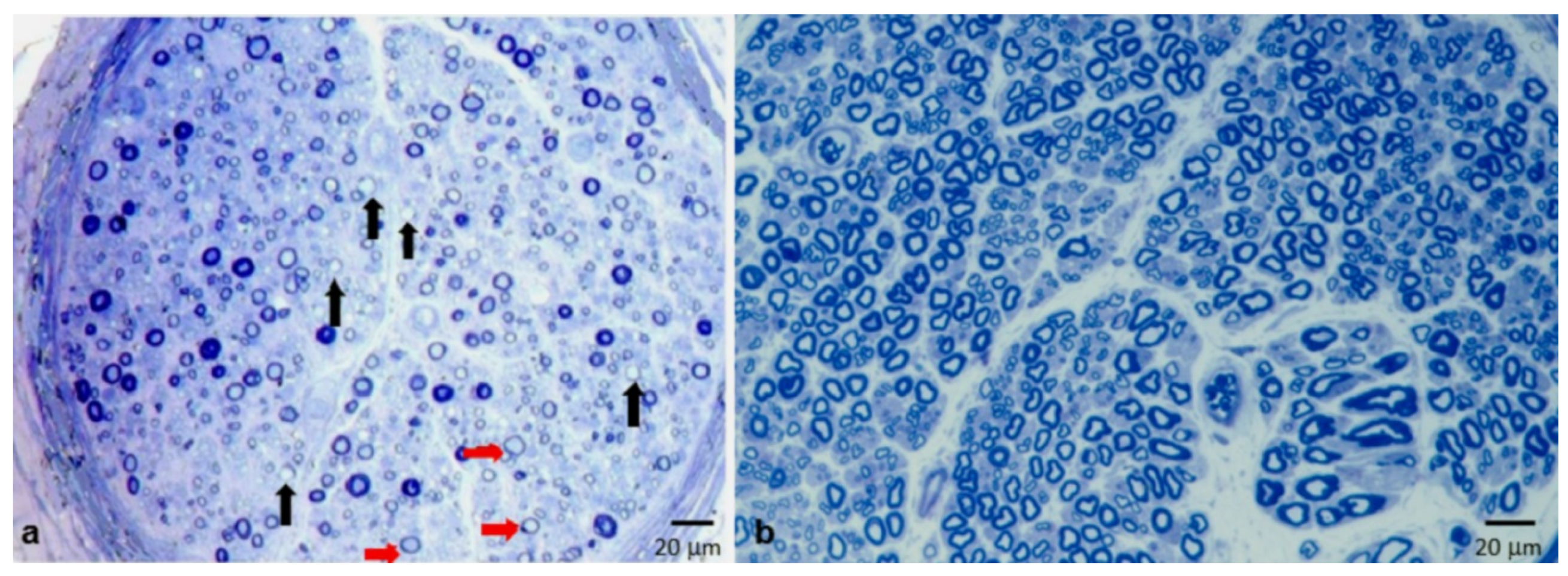
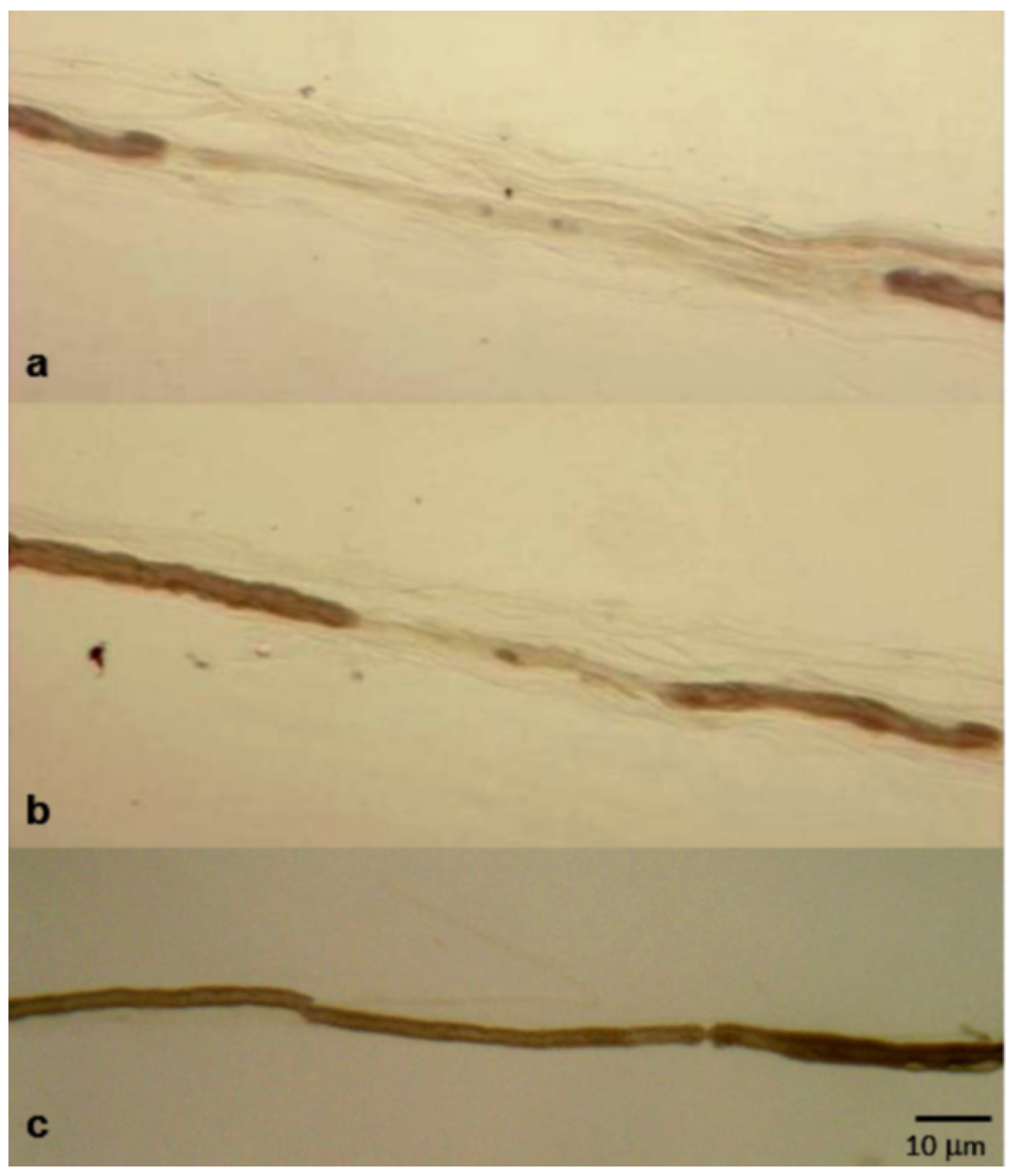
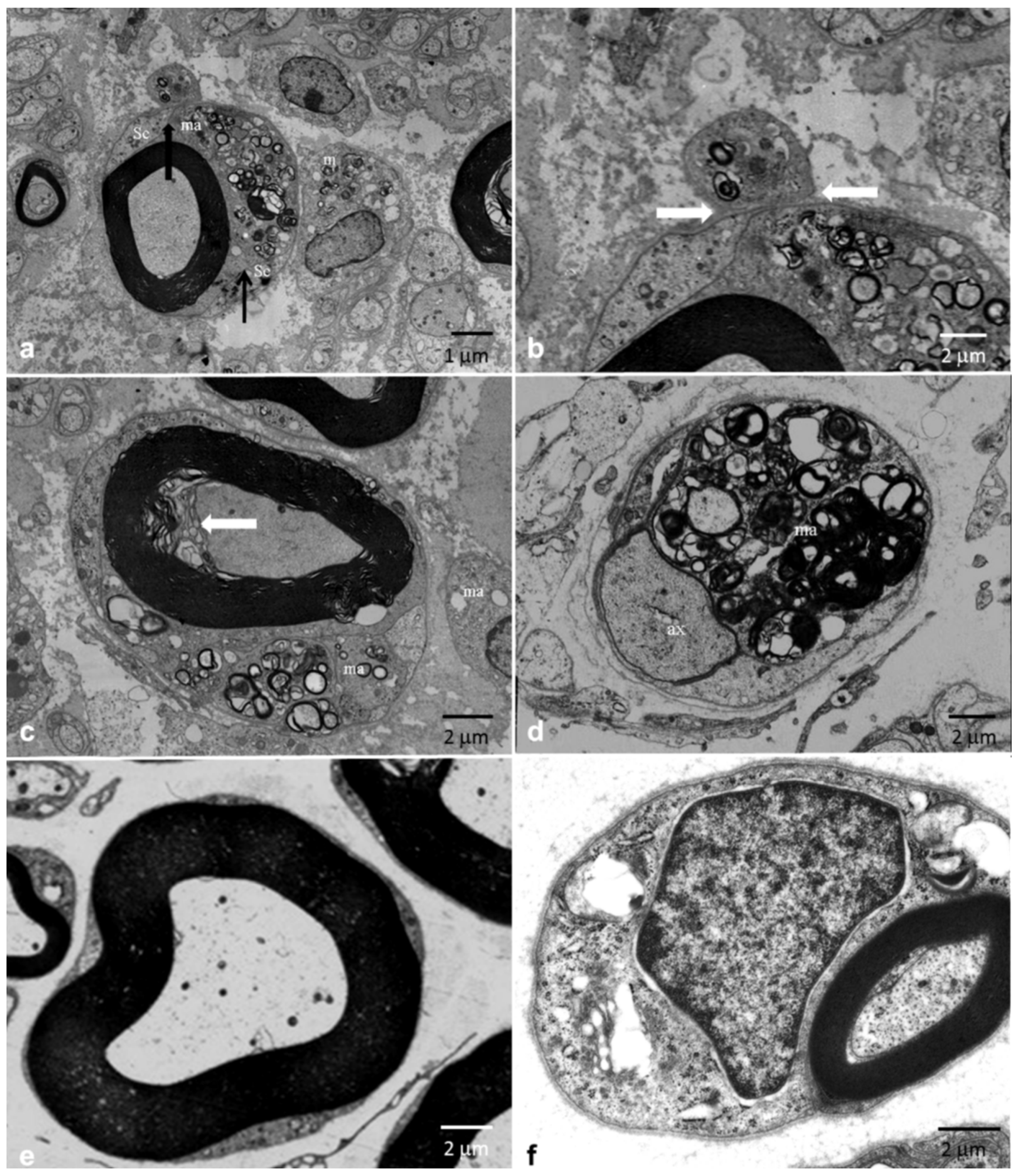
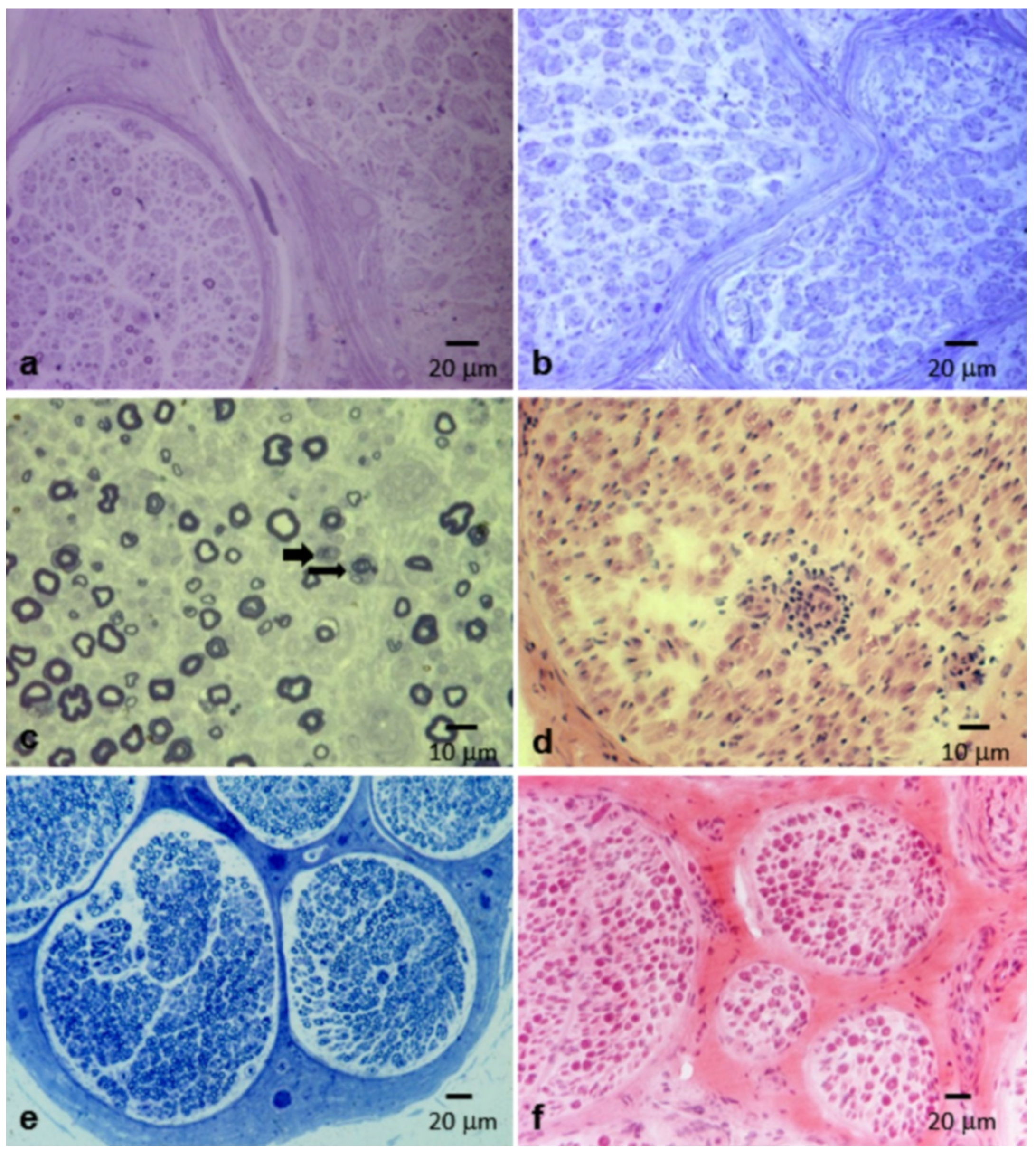
3.2. Pathological Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vallat, J.M.; Sommer, C.; Magy, L. Chronic inflammatory demyelinating polyradiculoneuropathy: Diagnostic and therapeutic challenges for a treatable condition. Lancet Neurol. 2010, 9, 402–412. [Google Scholar] [CrossRef]
- Hughes, R.A.; Allen, D.; Makowska, A.; Gregson, N.A. Pathogenesis of chronic inflammatory demyelinating polyradiculoneuropathy. J. Peripher. Nerv. Syst. 2006, 11, 30–46. [Google Scholar] [CrossRef]
- Saperstein, D.S.; Katz, J.S.; Amato, A.A.; Barohn, R.J. Clinical spectrum of chronic acquired demyelinating polyneuropathies. Muscle Nerve 2001, 24, 311–324. [Google Scholar] [CrossRef]
- Dyck, P.J.; Lais, A.C.; Ohta, M.; Bastron, J.A.; Okazaki, H.; Groover, R.V. Chronic inflammatory polyradiculoneuropathy. Mayo Clin. Proc. 1975, 50, 621–637. [Google Scholar]
- Doneddu, P.E.; Cocito, D.; Manganelli, F.; Fazio, R.; Briani, C.; Filosto, M.; Benedetti, L.; Mazzeo, A.; Marfia, G.A.; Cortese, A.; et al. Atypical CIDP: Diagnostic criteria, progression and treatment response. Data from the Italian CIDP Database. J. Neurol. Neurosurg. Psychiatry 2019, 90, 125–132. [Google Scholar] [CrossRef]
- Prineas, J.W.; McLeod, J.G. Chronic relapsing polyneuritis. J. Neurol. Sci. 1976, 27, 427–458. [Google Scholar] [CrossRef]
- Barohn, R.J.; Kissel, J.T.; Warmolts, J.R.; Mendell, J.R. Chronic inflammatory demyelinating polyradiculoneuropathy. Clinical characteristics, course, and recommendations for diagnostic criteria. Arch. Neurol. 1989, 46, 878–884. [Google Scholar] [CrossRef]
- Krendel, D.A.; Parks, H.P.; Anthony, D.C.; St Clair, M.B.; Graham, D.G. Sural nerve biopsy in chronic inflammatory demyelinating polyradiculoneuropathy. Muscle Nerve 1989, 12, 257–264. [Google Scholar] [CrossRef]
- Azulay, J.P.; Pouget, J.; Pellissier, J.F.; Blin, O.; Serratrice, G. [Chronic polyradiculoneuritis. 25 cases]. Rev. Neurol. (Paris) 1992, 148, 752–761. [Google Scholar]
- Matsumuro, K.; Izumo, S.; Umehara, F.; Osame, M. Chronic inflammatory demyelinating polyneuropathy: Histological and immunopathological studies on biopsied sural nerves. J. Neurol. Sci. 1994, 127, 170–178. [Google Scholar] [CrossRef]
- Gorson, K.C.; Allam, G.; Ropper, A.H. Chronic inflammatory demyelinating polyneuropathy: Clinical features and response to treatment in 67 consecutive patients with and without a monoclonal gammopathy. Neurology 1997, 48, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Rizzuto, N.; Morbin, M.; Cavallaro, T.; Ferrari, S.; Fallahi, M.; Galiazzo Rizzuto, S. Focal lesions area feature of chronic inflammatory demyelinating polyneuropathy (CIDP). Acta Neuropathol. 1998, 96, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, C.; Lacroix, C.; Planté, V.; Adams, D.; Chedru, F.; Guglielmi, J.M.; Said, G. Clinicopathologic findings and prognosis of chronic inflammatory demyelinating polyneuropathy. Neurology 1999, 52, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Vallat, J.M.; Tabaraud, F.; Magy, L.; Torny, F.; Bernet-Bernady, P.; Macian, F.; Couratier, P. Diagnostic value of nerve biopsy for atypical chronic inflammatory demyelinating polyneuropathy: Evaluation of eight cases. Muscle Nerve 2003, 27, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, G.B.; Mahadevan, A.; Taly, A.B.; Nalini, A.; Shankar, S.K. Sural nerve biopsy in chronic inflammatory demyelinating polyneuropathy: Are supportive pathologic criteria useful in diagnosis? Neurol. India 2010, 58, 542–548. [Google Scholar] [CrossRef]
- Piccione, E.A.; Engelstad, J.; Dyck, P.J.; Mauermann, M.L.; Dispenzieri, A.; Dyck, P.J.B. Nerve pathologic features differentiate POEMS syndrome from CIDP. Acta Neuropathol. Commun. 2016, 4, 116. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, S.; Koike, H.; Nishi, R.; Kawagashira, Y.; Iijima, M.; Katsuno, M.; Sobue, G. Clinicopathological characteristics of subtypes of chronic inflammatory demyelinating polyradiculoneuropathy. J. Neurol. Neurosurg. Psychiatry 2019, 90, 988–996. [Google Scholar] [CrossRef]
- Tatum, A.H. Experimental paraprotein neuropathy, demyelination by passive transfer of human IgM anti-myelin-associated glycoprotein. Ann. Neurol. 1993, 33, 502–506. [Google Scholar] [CrossRef]
- Querol, L.; Illa, I. Paranodal and other autoantibodies in chronic inflammatory neuropathies. Curr. Opin. Neurol. 2015, 28, 474–479. [Google Scholar] [CrossRef]
- Joint Task Force of the EFNS and the PNS. European Federation of Neurological Societies/Peripheral Nerve Society Guideline on management of chronic inflammatory demyelinating polyradiculoneuropathy: Report of a joint task force of the European Federation of Neurological Societies and the Peripheral Nerve Society—First Revision. Peripher. Nerv. Syst. 2010, 15, 1–9. [Google Scholar] [CrossRef]
- Luigetti, M.; Di Paolantonio, A.; Bisogni, G.; Romano, A.; Conte, A.; Barbato, F.; Del Grande, A.; Madia, F.; Rossini, P.M.; Lauretti, L.; et al. Sural nerve biopsy in peripheral neuropathies: 30-year experience from a single center. Neurol. Sci. 2020, 41, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Dyck, P.J.; Prineas, J.; Pollard, J. Chronic inflammatory demyelinating polyradiculopathy. In Peripheral Neuropathy; Dyck, P.J., Thomas, P.K., Griffin, J.W., Low, P.A., Poduslo, J.F., Eds.; WB Saunders: Philadelphia, PA, USA, 1993; pp. 1498–1517. [Google Scholar]
- Prada, V.; Massucco, S.; Venturi, C.; Geroldi, A.; Bellone, E.; Mandich, P.; Minuto, M.; Varaldo, E.; Mancardi, G.; Grandis, M.; et al. Diagnostic Value of Sural Nerve Biopsy: Retrospective Analysis of Clinical Cases From 1981 to 2017. Front. Neurol. 2019, 22, 1218. [Google Scholar] [CrossRef] [PubMed]
- Vallat, J.M.; Mathis, S.; Vegezzi, E.; Richard, L.; Duchesne, M.; Gallouedec, G.; Corcia, P.; Magy, L.; Uncini, A.; Devaux, J. Antibody- and macrophage-mediated segmental demyelination in chronic inflammatory demyelinating polyneuropathy: Clinical, electrophysiological, immunological and pathological correlates. Eur. J. Neurol. 2020, 27, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Uncini, A.; Notturno, F.; Capasso, M. Natura non facit saltus in anti-ganglioside antibody-mediated neuropathies. Muscle Nerve 2013, 48, 484–487. [Google Scholar] [CrossRef]
- Uncini, A.; Sabatelli, M.; Mignogna, T.; Lugaresi, A.; Liguori, R.; Montagna, P. Chronic progressive steroid responsive axonal polyneuropathy: A CIDP vaariant or a primary axonal disorder? Muscle Nerve 1996, 19, 365–371. [Google Scholar] [CrossRef]
- Shang, P.; Zhu, M.; Wang, Y.; Zheng, X.; Wu, X.; Zhu, J.; Feng, J.; Zhang., H.L. Axonal variants of Guillain-Barré syndrome: An update. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Tang, L.; Huang, Q.; Qin, Z.; Tang, X. Distinguish CIDP with autoantibody from that without autoantibody: Pathogenesis, histopathology, and clinical features. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Vallat, J.M.; Magy, L.; Corcia, P.; Boulesteix, J.M.; Uncini, A.; Mathis, S. Ultrastructural Lesions of Nodo-Paranodopathies in Peripheral Neuropathies. J. Neuropathol. Exp. Neurol. 2020, 79, 247–255. [Google Scholar] [CrossRef]
- Cortese, A.; Lombardi, R.; Briani, C.; Callegari, I.; Benedetti, L.; Manganelli, F.; Luigetti, M.; Ferrari, S.; Clerici, A.M.; Marfia, G.A.; et al. Antibodies to neurofascin, contactin-1, and contactin-associated protein 1 in CIDP: Clinical relevance of IgG isotype. Neurol. Neuroimmunol. Neuroinflamm. 2019, 7, e639. [Google Scholar] [CrossRef] [Green Version]
- Koike, H.; Kadoya, M.; Kaida, K.I.; Ikeda, S.; Kawagashira, Y.; Iijima, M.; Kato, D.; Ogata, H.; Yamasaki, R.; Matsukawa, N.; et al. Paranodal dissection in chronic inflammatory demyelinating polyneuropathy with anti-neurofascin-155 and anti-contactin-1 antibodies. J. Neurol. Neurosurg. Psychiatry 2017, 88, 465–473. [Google Scholar] [CrossRef]
- Padua, L.; Granata, G.; Sabatelli, M.; Inghilleri, M.; Lucchetta, M.; Luigetti, M.; Coraci, D.; Martinoli, C.; Briani, C. Heterogeneity of root and nerve ultrasound pattern in CIDP patients. Clin. Neurophysiol. 2014, 125, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Wang, W.; Zhao, Y.; Liu, B.; Wang, Y.; Yang, Y.; Ren, Y.; Liu, H. MR neurography of lumbosacral nerve roots: Diagnostic value in chronic inflammatory demyelinating polyradiculoneuropathy and correlation with electrophysiological parameters. Eur. J. Radiol. 2020, 124, 108816. [Google Scholar] [CrossRef] [PubMed]
- Sabatelli, M.; Madia, F.; Mignogna, T.; Lippi, G.; Quaranta, L.; Tonali, P. Pure motor chronic inflammatory demyelinating polyneuropathy. J. Neurol. 2001, 248, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Pollard, J.D. Chronic inflammatory demyelinating polyradiculoneuropathy. Curr. Opin. Neurol. 2002, 3, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Sabatelli, M.; Mignogna, T.; Lippi, G.; Porcu, C.; Tonali, P. Intramyelinic edema in chronic inflammatory demyelinating polyneuropathy. Clin. Neuropathol. 1996, 15, 17–21. [Google Scholar]
- Ochoa, J.; Fowler, T.J.; Gilliatt, R.W. Anatomical changes in peripheral nerves compressed by a pneumatic tourniquet. J. Anat. 1972, 113, 433–455. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Count (%) | |
|---|---|
| Final histopathological findings | |
| Demyelinating | 2 (4.7%) |
| Mixed | 29 (67.4%) |
| Axonal | 9 (20.9%) |
| Normal | 3 (7.0%) |
| Evidence of demyelination | |
| Absent | 11 (25.6%) |
| Only by teased fiber analysis | 6 (13.9%) |
| Only by semithin sections analysis | 7 (16.3%) |
| Both by semithin sections and teased fiber analysis | 16 (37.2%) |
| Not evaluable | 3 (7.0%) |
| Evidence of remyelination by teased fiber analysis | 9 (20.9%) |
| Onion bulbs | 8 (18.6%) |
| Loss of fibers | |
| Absent | 7 (16.3%) |
| Mild | 10 (23.2%) |
| Moderate | 11 (25.6%) |
| Severe | 15 (34.9%) |
| Axonal degeneration | 22 (51.2%) |
| Regeneration clusters | 26 (60.5%) |
| Inflammatory infiltrates | 2 (4.7%) |
| Vasa nervorum abnormalities | 0 (0%) |
| Intramyelinic edema | 3 (7.0%) |
| Endoneural or subepineural edema | 5 (11.6%) |
| Reference | No. of Biopsies | Demyelination | Axonal Loss/Degeneration | Onion Bulbs | Inflammatory Infiltrates | Normal Pathology |
|---|---|---|---|---|---|---|
| Dyck et al., 1975 [4] | 26 | 23.4 | 100 | 15 | 19 | 0 |
| Prineas et al., 1976 [6] | 26 * | 80 | 30 | 39 | NR | 20 |
| Barohn et al., 1989 [7] | 56 | 60.7 | 33.9 | NR | 10.7 | 17.9 |
| Krendel et al., 1989 [8] | 14 | 50 | NR | 36 | 29 | NR |
| Azulay et al., 1992 [9] | 20 | 90 | 55 | 35 | 15 | 10 |
| Matsumuro et al., 1994 [10] | 9 | 100 | 88.9 | 22 | 22.2 | 0 |
| Gorson et al., 1997 [11] | 18 | 39 | 61 | 5 | 17 | 17 |
| Rizzuto et al., 1998 [12] | 105 | 100 | 85 | 48 | 25 | 0 |
| Bouchard et al., 1999 [13] | 95 # | 72 | 47 | 18 | 4 | 2 |
| Vallat et al., 2003 [14] | 8 ** | 100 | 100 | NR | 75 | 0 |
| Kulkarmi et al., 2010 [15] | 46 | 82.8 | 56.6 | 28.3 | 58.7 | 0 |
| Piccione et al., 2016 [16] | 26 # | 46.0 | 69.2 | 38.5 | 61.5 | 0 |
| Ikeda et al., 2019 [17] | 106 | 22.8 | 8.1 | NR | 29.7 | NR |
| Luigetti et al. (this paper) | 43 | 67.4 | 83.8 | 18.6 | 4.7 | 7.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luigetti, M.; Romano, A.; Di Paolantonio, A.; Bisogni, G.; Rossi, S.; Conte, A.; Madia, F.; Sabatelli, M. Pathological Findings in Chronic Inflammatory Demyelinating Polyradiculoneuropathy: A Single-Center Experience. Brain Sci. 2020, 10, 383. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10060383
Luigetti M, Romano A, Di Paolantonio A, Bisogni G, Rossi S, Conte A, Madia F, Sabatelli M. Pathological Findings in Chronic Inflammatory Demyelinating Polyradiculoneuropathy: A Single-Center Experience. Brain Sciences. 2020; 10(6):383. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10060383
Chicago/Turabian StyleLuigetti, Marco, Angela Romano, Andrea Di Paolantonio, Giulia Bisogni, Salvatore Rossi, Amelia Conte, Francesca Madia, and Mario Sabatelli. 2020. "Pathological Findings in Chronic Inflammatory Demyelinating Polyradiculoneuropathy: A Single-Center Experience" Brain Sciences 10, no. 6: 383. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10060383